Driving Outcomes among Older Adults: A Systematic Review on Racial and Ethnic Differences over 20 Years

Abstract
:1. Introduction
2. Materials and Methods
2.1. PICOS Framework
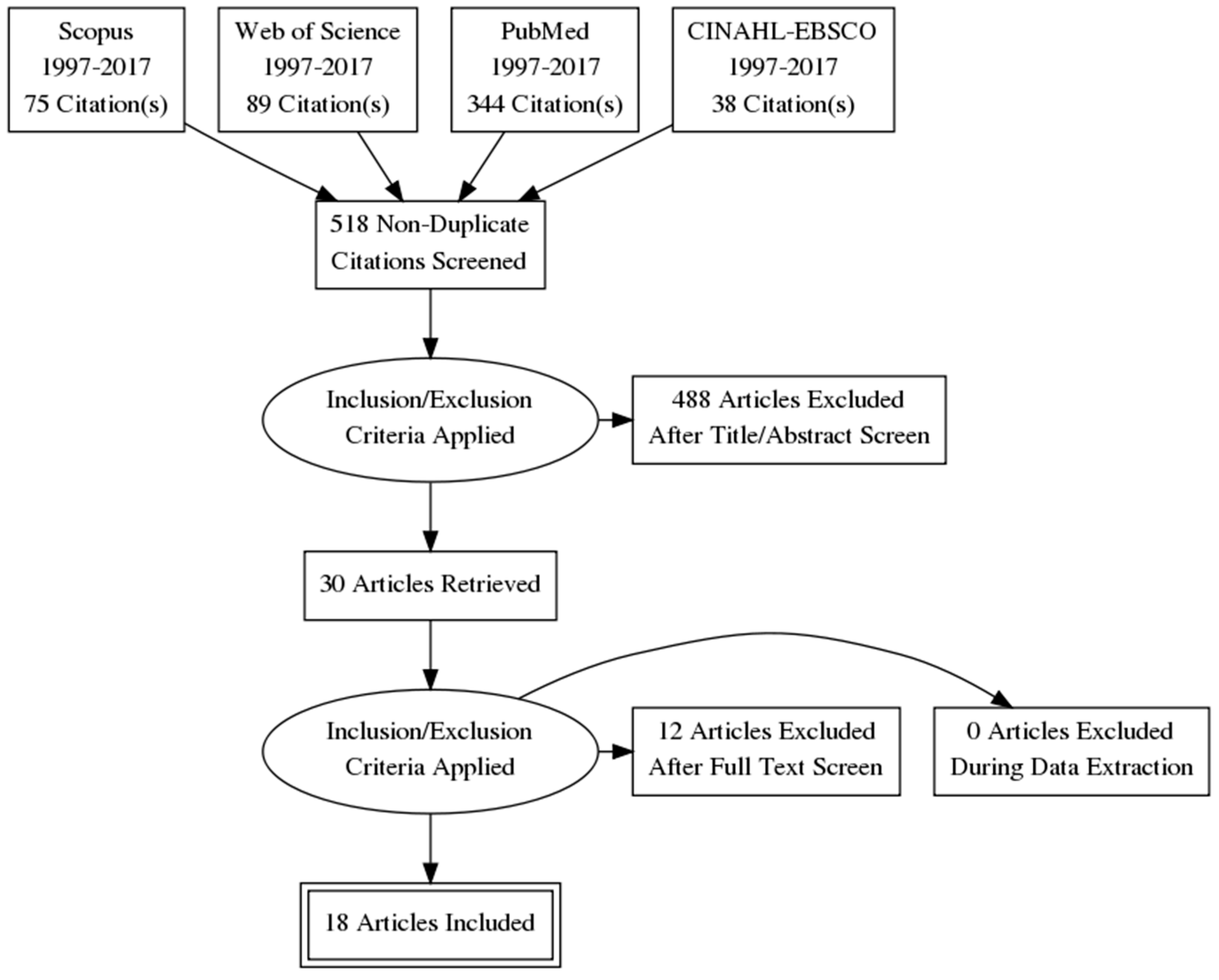
2.2. Literature Search
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction, Assessment, and Qualitative Synthesis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interests
References
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J. Dementia prevention, intervention, and care. The Lancet 2017, 390, 2673–2734. Available online: http://www.thelancet.com/commissions/dementia2017 (accessed on 12 November 2017).
- Alzheimer’s Association. Alzheimer’s Disease Facts and Figures. 2016. Available online: http://www.alz.org/documents_custom/2016-facts-and-figures.pdf (accessed on 12 November 2017).
- Dickerson, A.E.; Molnar, L.J.; Bédard, M.; Eby, D.W.; Berg-Weger, M.; Choi, M.; Grigg, J.; Horowitz, A.; Meuser, T.; Myers, A. Transportation and aging: An updated research agenda to advance safe mobility among older adults transitioning from driving to non-driving. Gerontologist 2017. [Google Scholar] [CrossRef] [PubMed]
- Chihuri, S.; Mielenz, T.J.; DiMaggio, C.J.; Betz, M.E.; DiGuiseppi, C.; Jones, V.C.; Li, G. Driving cessation and health outcomes in older adults. J. Am. Geriatr. Soc. 2016, 64, 332–341. [Google Scholar] [CrossRef] [PubMed]
- Casutt, G.; Martin, M.; Keller, M.; Jäncke, L. The relation between performance in on-road driving, cognitive screening and driving simulator in older healthy drivers. Transp. Res. Part F 2014, 22, 232–244. [Google Scholar] [CrossRef]
- Hird, M.A.; Egeto, P.; Fischer, C.E.; Naglie, G.; Schweizer, T.A. A Systematic Review and Meta-Analysis of On-Road Simulator and Cognitive Driving Assessment in Alzheimer’s Disease and Mild Cognitive Impairment. J. Alzheimer's Dis. 2016, 53, 1–17. [Google Scholar] [CrossRef] [PubMed]
- The Federal Interagency Forum on Aging-Related Statistics. Older Americans 2016: Key Indicators of Well-Being. Available online: https://agingstats.gov/docs/LatestReport/Older-Americans-2016-Key-Indicators-of-WellBeing.pdf (accessed on 25 October 2017).
- National Research Council Panel on Race, Ethnicity, and Health in Later Life; Committee on Population of the National Research Council (NRC). Understanding Racial and Ethnic Differences in Health in Late Life: A Research Agenda; National Academies Press: Washington, DC, USA, 2004. [Google Scholar]
- Burchard, E.G.; Ziv, E.; Coyle, N.; Gomez, S.L.; Tang, H.; Karter, A.J.; Mountain, J.L.; Pérez-stable, E.J.; Sheppard, D.; Risch, N. The importance of race and ethnic background in biomedical research and clinical practice. N. Eng. J. Med. 2003, 348, 1170–1175. [Google Scholar] [CrossRef] [PubMed]
- Fuller-Thomson, E.; Nuru-Jeter, A.; Minkler, M.; Guralnik, J.M. Black-White disparities in disability among older Americans: Further untangling the role of race and socioeconomic status. J. Aging Health 2009, 21, 677–698. [Google Scholar] [CrossRef] [PubMed]
- Ighodaro, E.T.; Nelson, P.T.; Kukull, W.A.; Schmitt, F.A.; Abner, E.L.; Caban-Holt, A.; Bardach, S.H.; Hord, D.C.; Glover, C.M.; Jicha, G.A. Challenges and Considerations Related to Studying Dementia in Blacks/African Americans. J. Alzheimer's Dis. 2017, 60, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ball, K.; Edwards, J.D.; Ross, L.A.; McGwin, G., Jr. Cognitive training decreases motor vehicle collision involvement of older drivers. J. Am. Geriatr. Soc. 2010, 58, 2107–2113. [Google Scholar] [CrossRef] [PubMed]
- Carr, D.B.; Barco, P.P.; Babulal, G.M.; Stout, S.H.; Johnson, A.M.; Xiong, C.; Morris, J.C.; Roe, C.M. Association of functional impairments and co-morbid conditions with driving performance among cognitively normal older adults. PLoS ONE 2016, 11, e0167751. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.; Lohman, M.C.; Mezuk, B. Trajectories of cognitive decline by driving mobility: Evidence from the Health and Retirement Study. Int. J. Geriatr. Psychiatry 2014, 29, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.; Mezuk, B. Aging without driving: Evidence from the Health and Retirement Study, 1993 to 2008. J. Appl. Gerontol. 2013, 32, 902–912. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.; Mezuk, B.; Lohman, M.C.; Edwards, J.D.; Rebok, G.W. Gender and racial disparities in driving cessation among older adults. J. Aging Health 2012, 25, 147S–162S. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.; O’Connor, M.L.; Mingo, C.A.; Mezuk, B. Gender and racial disparities in life-space constriction among older adults. Gerontologist 2015, 56, 1153–1160. [Google Scholar] [CrossRef] [PubMed]
- Dugan, E.; Lee, C.M. Biopsychosocial risk factors for driving cessation: Findings from the Health and Retirement Study. J. Aging Health 2013, 25, 1313–1328. [Google Scholar] [CrossRef] [PubMed]
- Edwards, J.; Lister, J.; Lin, F.; Andel, R.; Brown, L.; Wood, J.M. Association of hearing impairment and subsequent driving mobility in older adults. Gerontologist 2017, 55, 137–138. [Google Scholar] [CrossRef] [PubMed]
- Edwards, J.D.; Perkins, M.; Ross, L.A.; Reynolds, S.L. Driving status and three-year mortality among community-dwelling older adults. J. Gerontol. Ser. A 2009, 64, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Green, K.A.; McGwin, G.; Owsley, C. Associations between visual, hearing, and dual sensory impairments and history of motor vehicle collision involvement of older drivers. J. Am. Geriatr. Soc. 2013, 61, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Lunsman, M.; Edwards, J.D.; Andel, R.; Small, B.J.; Ball, K.K.; Roenker, D.L. What predicts changes in useful field of view test performance? Psychol. Aging 2008, 23, 917. [Google Scholar] [CrossRef] [PubMed]
- MacGregor, J.M.; Freeman, D.H.; Zhang, D. A traffic sign recognition test can discriminate between older drivers who have and have not had a motor vehicle crash. J. Am. Geriatr. Soc. 2001, 49, 466–469. [Google Scholar] [CrossRef] [PubMed]
- Munro, C.A.; Jefferys, J.; Gower, E.W.; Muñoz, B.E.; Lyketsos, C.G.; Keay, L.; Turano, K.A.; Bandeen-Roche, K.; West, S.K. Predictors of Lane-Change Errors in Older Drivers. J. Am. Geriatr. Soc. 2010, 58, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Okonkwo, O.C.; Crowe, M.; Wadley, V.G.; Ball, K. Visual attention and self-regulation of driving among older adults. Int. Psychogeriatr. 2008, 20, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Owsley, C.; Ball, K.; McGwin, G., Jr.; Sloane, M.E.; Roenker, D.L.; White, M.F.; Overley, E.T. Visual Processing Impairment and Risk of Motor Vehicle Crash Among Older Adults. JAMA 1998, 279, 1083–1088. [Google Scholar] [CrossRef] [PubMed]
- Owsley, C.; McGwin, G., Jr.; Sloane, M.; Wells, J.; Stalvey, B.T.; Gauthreaux, S. Impact of cataract surgery on motor vehicle crash involvement by older adults. JAMA 2002, 288, 841–849. [Google Scholar] [CrossRef] [PubMed]
- Sims, R.V.; McGwin, G., Jr.; Allman, R.M.; Ball, K.; Owsley, C. Exploratory study of incident vehicle crashes among older drivers. J. Gerontol. Ser. A 2000, 55, M22–M27. [Google Scholar]
- Sims, R.V.; Owsley, C.; Allman, R.M.; Ball, K.; Smoot, T.M. A preliminary assessment of the medical and functional factors associated with vehicle crashes by older adults. J. Am. Geriatr. Soc. 1998, 46, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Foley, D.J.; Heimovitz, H.K.; Guralnik, J.M.; Brock, D.B. Driving life expectancy of persons aged 70 years and older in the United States. Am. J. Publ. Health 2002, 92, 1284–1289. [Google Scholar] [CrossRef]
- Chin, A.L.; Negash, S.; Hamilton, R. Diversity and disparity in dementia: The impact of ethnoracial differences in Alzheimer’s disease. Alzheimer Dis. Assoc. Disord. 2011, 25, 187. [Google Scholar] [CrossRef] [PubMed]
- Tsvetkova, D.Z.; Bergquist, S.H.; Parker, M.W.; Jarrett, T.L.; Howell, J.C.; Watts, K.D.; Kollhoff, A.; Roberts, D.L.; Hu, W.T. Fear and uncertainty do not influence reported willingness to undergo lumbar punctures in a US multi-cultural cohort. Front. Aging Neurosci. 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Saelens, B.E. Assessment of physical activity by self-report: Status, limitations, and future directions. Res. Q. Exerc. Sport 2000, 71, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Rabbitt, P.; Abson, V. ‘Lost and Found’: Some logical and methodological limitations of self-report uestionnaires as tools to study cognitive ageing. Br. J. Psychol. 1990, 81, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Eby, D.W.; Molnar, L.J.; Zhang, L.; St Louis, R.M.; Zanier, N.; Kostyniuk, L.P. Keeping Older Adults Driving Safely: A Research Synthesis of Advanced In-Vehicle Technologies, A LongROAD Study; American Automobile Association: Washington, DC, USA, 2015. [Google Scholar]
- Eby, D.W.; Silverstein, N.M.; Molnar, L.J.; LeBlanc, D.; Adler, G. Driving behaviors in early stage dementia: A study using in-vehicle technology. Accid. Anal. Prev. 2012, 49, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Babulal, G.M.; Stout, S.H.; Benzinger, T.L.S.; Ott, B.R.; Carr, D.B.; Webb, M.; Traub, C.M.; Addison, A.; Morris, J.C.; Warren, D.K.; et al. A Naturalistic Study of Driving Behavior in Older Adults and Preclinical Alzheimer Disease. J. Appl. Gerontol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Babulal, G.M.; Traub, C.M.; Webb, M.; Stout, S.H.; Addison, A.; Carr, D.B.; Ott, B.R.; Morris, J.C.; Roe, C.M. Creating a driving profile for older adults using GPS devices and naturalistic driving methodology. F1000Research 2016. [Google Scholar] [CrossRef]
- Zhou, Y.; Elashoff, D.; Kremen, S.; Teng, E.; Karlawish, J.; Grill, J.D. African Americans are less likely to enroll in preclinical Alzheimer’s disease clinical trials. Alzheimer's Dement. Trans. Res. Clin. Interv. 2017, 3, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.M.; Scharff, D.P.; Mathews, K.J.; Hoffsuemmer, J.S.; Jackson, P.; Morris, J.C.; Edwards, D.F. Barriers and facilitators of African American participation in Alzheimer’s disease biomarker research. Alzheimer Dis. Assoc. Disord. 2010, 24, S24. [Google Scholar] [PubMed]
- Williams, M.M.; Meisel, M.M.; Williams, J.; Morris, J.C. An interdisciplinary outreach model of African American recruitment for Alzheimer’s disease research. Gerontologist 2011, 51, S134–S141. [Google Scholar] [CrossRef] [PubMed]
- Dilworth-Anderson, P. Introduction to the science of recruitment and retention among ethnically diverse populations. Gerontologist 2011, 51, S1–S4. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| First Author (Year) | Study Design | Purpose | Age Range or Mean (SD) of n (in Years) | Sample Size | Racial/Ethnic Group n (% of Total Sample) | Explicit Focus on Race or Ethnicity | Group Difference Found in Driving Outcome | |
|---|---|---|---|---|---|---|---|---|
| 1 | Edwards (2017) [18] | Retrospective Longitudinal | Impact of hearing impairment on driving mobility | 63–90 | 500 | African American 57 (11.4%) | No—Race/Ethnicity treated as covariate | Minority race associated with baseline-restricted mobility |
| 2 | Carr (2016) [12] | Prospective Longitudinal | Examine functional impairments and comorbidities on driving performance | 64.9–88.2 | 129 | African American 12 (9.3%) | No—Race/Ethnicity treated as covariate | No |
| 3 | Choi (2015) [16] | Randomized Controlled Trial | Examine gender and racial disparities in life-space constriction in later life | 73.6 (5.9) | 2765 | African American 726 (26.2%) | Yes | African Americans have more life-space constriction at baseline but are stable over time |
| 4 | Choi (2014) [13] | Retrospective Longitudinal | Association between driving status and cognitive functioning in later life | 71.9 (4.4) | 9135 | Mixed 1251 (13.6%) | No—Race/Ethnicity treated as covariate | No |
| 5 | Choi (2013) [14] | Retrospective Longitudinal | Characterize former vs. never drivers over 15 years | 77.4 (4.44) and 77.4 (4.77) | 3098 | African Americans 539 (17.3%), Hispanics 327 (10.5%), Other 77 (2.4%) | Yes | Minority race was significant predicted to have never driven |
| 6 | Dugan (2013) [17] | Retrospective Longitudinal | Biopsychosocial risk factors associated with driving cessation | 75.10 (7.16) | 17,349 | Mixed 3643 (20.9%) | Yes | Minority race a risk factor for current and future driving cessation |
| 7 | Green (2013) [20] | Retrospective Longitudinal | Examine sensory impairment as risk factor for crashes among older drives | 70–99 | 1998 | African American 350 (17.5%), Other 9 (<1%) | No—Race/Ethnicity treated as covariate | No |
| 8 | Choi (2012) [15] | Randomized Controlled Trial | Examine gender and racial disparities in driving cessation | 73.54 (5.88) | 2645 | African American 394 (14.9%), Other 17 (0.06%) | Yes | Minority race more likely to stop driving faster in later life |
| 9 | Ball (2010) [11] | Randomized Controlled Trial | Examine the effect of cognitive training on subsequent crashes among older adults | 65–91 | 908 | African American 164 (18.0%) | No—Race/Ethnicity treated as covariate | No |
| 10 | Munro (2010) [23] | Cross-sectional | Examine risk factors that predict lane-changing errors in older adults | 67–87 | 1080 | African American 129 (11.9%) | No—Race/Ethnicity treated as covariate | No |
| 11 | Edwards (2009) [19] | Prospective Longitudinal | Examine driving status as a predictor of mortality among older adults | 73.16 (2.77) | 660 | African American 94 (14.2%) | No—Race/Ethnicity treated as covariate | No |
| 12 | Lunsman (2008) [21] | Randomized Controlled Trial | Examine what factors predict change in visual processing | 65–94 | 690 | African American 185 (26.8%), Other 9 (1.3%) | No—Race/Ethnicity treated as covariate | No |
| 13 | Okonkwo (2008) [24] | Prospective Longitudinal | Examine self-regulation of older adults via driving habits and visual attention | 75–100.44 | 1543 | Other 41 (2.6%) | No—Race/Ethnicity treated as covariate | No |
| 14 | Owsley (2002) [26] | Prospective Longitudinal | Examine cataract surgery as a risk factor for crashes among older adults | 71.2 (6.6) and 71.5 (5.4) | 277 | Other 37 (13.3%) | No—Race/Ethnicity treated as covariate | No |
| 15 | MacGregor (2001) [22] | Prospective Longitudinal | Examine if traffic sign test can distinguish older adult driver who crashed | 65–91 | 120 | Other 21 (17.5%) | No—Race/Ethnicity treated as covariate | No |
| 16 | Sims (2000) [27] | Prospective Longitudinal | Identify medical and functional risk factors for at-fault crashes | 57–91 | 174 | African American 26 (14.9%) | No—Race/Ethnicity treated as covariate | No |
| 17 | Sims (1998) [28] | Cross-sectional Case-control | Identify medical and functional risk factors for at-fault crashes | 57–91 | 174 | African American 26 (14.9%) | No—Race/Ethnicity treated as covariate | African American race was associated with more at-fault crashes |
| 18 | Owsley (1998) [25] | Prospective Longitudinal | Examine visual processing impairment as a risk factor for crashes | 55–87 | 294 | African American 56 (19%) | No—Race/Ethnicity treated as covariate | No |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Babulal, G.M.; Williams, M.M.; Stout, S.H.; Roe, C.M. Driving Outcomes among Older Adults: A Systematic Review on Racial and Ethnic Differences over 20 Years. Geriatrics 2018, 3, 12. https://doi.org/10.3390/geriatrics3010012
Babulal GM, Williams MM, Stout SH, Roe CM. Driving Outcomes among Older Adults: A Systematic Review on Racial and Ethnic Differences over 20 Years. Geriatrics. 2018; 3(1):12. https://doi.org/10.3390/geriatrics3010012
Chicago/Turabian StyleBabulal, Ganesh M., Monique M. Williams, Sarah H. Stout, and Catherine M. Roe. 2018. "Driving Outcomes among Older Adults: A Systematic Review on Racial and Ethnic Differences over 20 Years" Geriatrics 3, no. 1: 12. https://doi.org/10.3390/geriatrics3010012
APA StyleBabulal, G. M., Williams, M. M., Stout, S. H., & Roe, C. M. (2018). Driving Outcomes among Older Adults: A Systematic Review on Racial and Ethnic Differences over 20 Years. Geriatrics, 3(1), 12. https://doi.org/10.3390/geriatrics3010012