Evaluation of Drug-Disease Interactions and Their Association with Unplanned Hospital Readmission Utilizing STOPP Version 2 Criteria

Abstract
:1. Introduction
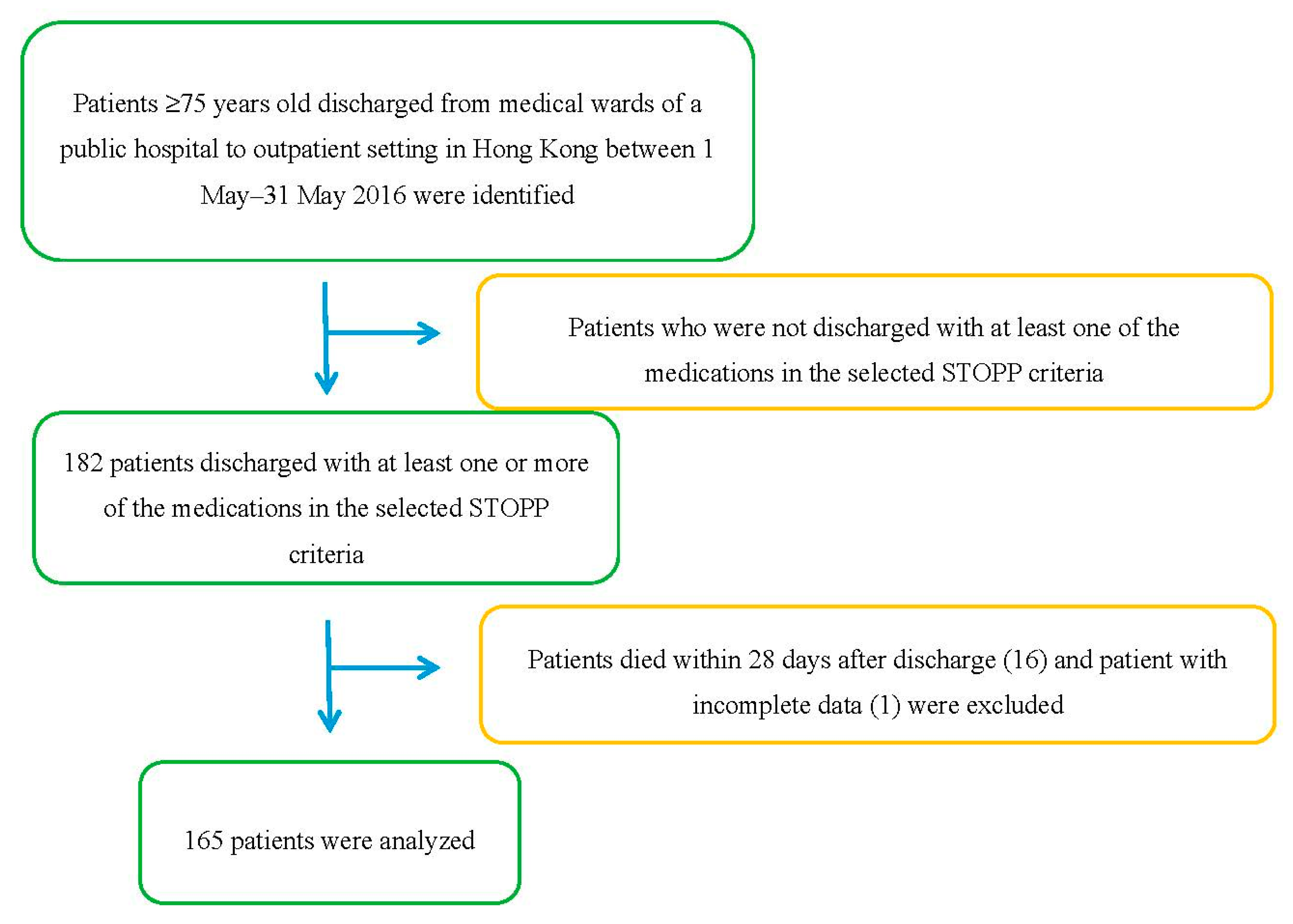
2. Materials and Methods
3. Results
3.1. Variables Associated with Unplanned Early Readmission
3.1.1. Bivariate Analysis
3.1.2. Multivariate Analysis
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A

{kind=link}
| Characteristic | Total (n = 165) (%) | Not Readmitted within 28 Days (n = 123) (%) | Readmitted within 28 Days (n = 42) (%) | p Value | |
|---|---|---|---|---|---|
| Age | 83.35 ± 5.49 | 83.03 ± 5.33 | 84.29 ± 5.84 | 0.383 | |
| Gender | Male | 65 (39.4) | 46 (37.4) | 19 (45.2) | 0.369 |
| Female | 100 (60.6) | 77 (62.6) | 23 (54.8) | ||
| Number of chronic medication | <6 | 45 (27.3) | 36 (29.5) | 9 (21.4) | 0.575 |
| 6–10 | 104 (63) | 76 (62.3) | 28 (6.7) | ||
| >10 | 16 (9.7) | 11 (9) | 5 (11.9) | ||
| Number of comorbidities | <5 | 98 (59.4) | 73 (59.8) | 25 (59.5) | 0.984 |
| ≥5 | 67 (40.6) | 50 (41) | 17 (40.5) | ||
| Patients with PIM(s) identified | 45 (27.3) | 21 (17.1) | 24 (57.1) | <0.001 | |
| Arrhythmia | 47 (28.5) | 39 (32) | 8 (19) | 0.117 | |
| Asthma | 5 (3) | 3 (2.5) | 2 (4.8) | 0.602 | |
| Cancer | 20 (12.1) | 14 (11.5) | 6 (14.3) | 0.619 | |
| COPD | 19 (11.5) | 15 (12.3) | 4 (9.5) | 0.784 | |
| Delirium | 15 (9.1) | 11 (9) | 4 (9.5) | 1.000 | |
| Dementia | 6 (3.6) | 5 (4) | 1 (2.4) | 1.000 | |
| Diabetes | 73 (44.2) | 57 (46.7) | 16 (38.1) | 0.353 | |
| Gastrointestinal disorder | 8 (4.8) | 3 (2.5) | 5 (11.9) | 0.026 | |
| Glaucoma | 10 (6.1) | 6 (4.9) | 4 (9.5) | 0.278 | |
| Gout | 27 (16.4) | 14 (11.5) | 13 (31) | 0.003 | |
| Heart failure | 38 (23) | 26 (21.3) | 12 (28.6) | 0.323 | |
| Hyperlipidemia | 61 (37) | 47 (38.5) | 14 (33.3) | 0.572 | |
| Hypertension | 112 (67.9) | 85 (69.7) | 27 (64.3) | 0.564 | |
| Ischemic heart disease | 58 (35.2) | 45 (36.9) | 13 (31) | 0.509 | |
| Liver disease | 15 (9.1) | 12 (9.8) | 3 (7.1) | 0.762 | |
| Myocardial infarction | 15 (9.1) | 10 (8.2) | 5 (11.9) | 0.535 | |
| Parkinsonism | 6 (3.6) | 5 (4.1) | 1 (2.4) | 1.000 | |
| Prostatism | 23 (13.9) | 19 (15.6) | 4 (9.5) | 0.339 | |
| Psychiatric disorder | 73 (44.2) | 57 (46.7) | 16 (38.1) | 0.353 | |
| Renal disease | 34 (20.6) | 22 (18) | 12 (28.6) | 0.139 | |
| Stroke | 26 (15.8) | 19 (15.6) | 7 (16.7) | 0.851 | |
| Urine retention | 23 (13.9) | 16 (13.1) | 7 (16.7) | 0.554 | |
| Drug-disease interaction with | |||||
| Selective COX-2 NSAIDs/Diltiazem/VerapamilNon-selective beta blockers/Oestrogens/Thiazolidinediones | 0 (0) | 0 (0) | 0 (0) | - | |
| TCAs | 3 (1.8) | 2 (1.6) | 1 (2.4) | 1 | |
| Antipsychotics | 1 (0.6) | 1 (0.8) | 0 (0) | 1 | |
| Anticholinergics/antimuscarinics | 37 (22.4) | 15 (12.2) | 22 (52.4) | <0.001 | |
| Antimuscarinic bronchodilators | 9 (5.5) | 5 (4.1) | 4 (9.5) | 0.234 | |
| Prochlorperazine/Metoclopramide | 1 (0.6) | 0 (0) | 1 (2.4) | 0.255 | |
| Oral bisphosphonate | 3 (1.8) | 0 (0) | 3 (7.1) | 0.016 | |
References
- Wong, L.Y.; Cheung, W.L.; Leung, C.M.; Yam, H.K.; Chan, W.K.; Wong, Y.Y.; Yeoh, E.K. Unplanned readmission rates, length of hospital stay, mortality, and medical costs of ten common medical conditions: A retrospective analysis of Hong Kong hospital data. BMC Health Serv. Res. 2011, 11, 149. [Google Scholar] [CrossRef] [PubMed]
- Ko, C.F.; Yu, T.K.K.; Ko, T.P.S. A survey of hospital readmission in elderly patients. Hong Kong Med. J. 1996, 2, 258–262. [Google Scholar]
- Yam, H.K.; Wong, L.Y.; Chan, W.K.; Leung, M.C.; Wong, F.Y.; Cheung, A.W.; Yeoh, E.K. Avoidable readmission in Hong Kong—System, clinician, patient or social factor? BMC Health Serv. Res. 2010, 10, 311. [Google Scholar] [CrossRef] [PubMed]
- Bero, L.A.; Lipton, H.L.; Bird, J.A. Characterization of geriatric drug-related hospital readmissions. Med. Care 1991, 29, 989–1003. [Google Scholar] [CrossRef] [PubMed]
- Fialova, D.; Topinkova, E.; Gambassi, G.; Finne-Soveri, H.; Jonsson, P.V.; Carpenter, I.; Schroll, M.; Onder, G.; Sorbye, L.W.; Wagner, C.; et al. Potentially inappropriate medication use among elderly home care patients in Europe. JAMA 2005, 293, 1348–1358. [Google Scholar] [CrossRef] [PubMed]
- Tamura, B.K.; Bell, C.L.; Inaba, M.; Masaki, K.H. Ouctomes of polypharmacy in nursing home residents. Clin. Geriatr. Med. 2012, 28, 217–236. [Google Scholar] [CrossRef] [PubMed]
- Gnjidic, D.; Le Couteur, D.G.; Pearson, S.A.; McLachlan, A.J.; Viney, R.; Hilmer, S.N.; Blyth, F.M.; Joshy, G.; Banks, E. High risk prescribing in older adults: Prevalence, clinical and economic implications and potential for intervention at the population level. BMC Public Health 2013, 13, 115. [Google Scholar] [CrossRef] [PubMed]
- Bongue, B.; Naudin, F.; Laroche, M.; Galteau, M.M.; Guy, C.; Gueguen, R.; Convers, J.P.; Colvez, A.; Maarouf, N. Trends of the potentially inappropriate medication consumption over 10 years in older adults in the East of France. Pharmacoepidemiol. Drug Saf. 2009, 18, 1125–1133. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, C.; Aquila, G.D.; Gasperini, B.; Onder, G.; Lattanzio, F.; Volpato, S.; Corsonello, A.; Maraldi, C.; Baernabei, R.; Cherubini, A.; et al. Potentially inappropriate drug prescriptions and risk of hospitalization among older, Italian, nursing home residents. Drugs Aging 2010, 27, 747–758. [Google Scholar] [CrossRef] [PubMed]
- Leger, D.Y.; Moreau, S.; Signol, N.; Fargeas, J.B.; Picat, M.A.; Penot, A.; Abraham, J.; Laroche, M.L.; Bordessoule, D. Polypharmacy, potentially inappropriate medications and drug-drug interactions in geriatric patients with hematologic malignancy: Observational single-center study of 122 patients. J. Geriatr. Oncol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Rougé Bugat, M.E.; Bourgouin, M.; Gérard, S.; Lozano, S.; Brechemier, D.; Cestac, P.; Cool, C.; Balardy, L. Drug prescription including interactions with anticancer treatments in the elderly: A global approach. J. Nutr. Health Aging 2017, 21, 849. [Google Scholar] [CrossRef] [PubMed]
- Hill-Taylor, B.; Walsh, K.A.; Stewart, S.; Hayden, J.; Byrne, S.; Sketris, I.S. Effectiveness of the STOPP/START (Screening Tool of Older Persons’ potentially inappropriate Prescriptions/Screening Tool to Alert doctors to the Right Treatment) criteria: Systematic review and meta-analysis of randomized controlled studies. J. Clin. Pharm. Ther. 2016, 41, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Lindblad, C.I.; Hanlon, J.T.; Gross, C.R.; Sloane, R.J.; Pieper, C.F.; Hajjar, E.R.; Ruby, C.M.; Schmader, K.E. Clinically important drug-disease interactions and their prevalence in older adults. Clin. Ther. 2006, 28, 1133–1143. [Google Scholar] [CrossRef] [PubMed]
- Hanlon, J.T.; Sloane, R.J.; Pieper, C.F.; Schmader, K.E. Association of adverse drug reactions with drug-drug and drug-disease interactions in frail older outpatients. Age Ageing 2011, 40, 274–277. [Google Scholar] [CrossRef] [PubMed]
- Simon, S.R.; Gurwitz, J.H. Drug therapy in the elderly: Improving quality and access. Clin. Pharmacol. Ther. 2003, 73, 387–393. [Google Scholar] [CrossRef]
- Hamilton, H.; Gallagher, P.; Ryan, C.; Byrne, S.; O’Mahony, D. Potentially inappropriate medications defined by STOPP Criteria and the risk of adverse drug events in older hospitalized patients. Am. Med. Assoc. 2011, 171, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Sylvie, D.; D’Arcy, C.; Sanfilippo, F.M.; Emery, J.D. Association between potentially inappropriate medications from Beers criteria and the risk of unplanned hospitalization in elderly patients. Ann. Pharmacother. 2014, 48, 6–16. [Google Scholar]
- Gallagher, P.F.; O’connor, M.O.; O’Mahony, D. Prevention of potentially inappropriate prescribing for elderly patients: A randomized controlled trial using STOPP/START Criteria. Clin. Pharmacol. Ther. 2011, 89, 845–854. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, M.D.; Qin, H.; Mercer, S.Q.; Fong, J.; Haydar, Z. Risk factors for 30-day hospital readmission in patients ≥65 years of age. Proc. (Bayl. Univ. Med. Cent.) 2008, 21, 363–372. [Google Scholar] [PubMed]
- Green, S.B. How many subjects does it take to do a regression analysis? Multivar. Behav. Res. 1991, 26, 499–510. [Google Scholar] [CrossRef] [PubMed]
- The American Geriatrics Society 2012 Beers Criteria Update Expert Panel. AGS Updated Beers Criteria for potentially inappropriate medication use in older adults. J. Am. Geriatr. Soc. 2012, 60, 616–631. [Google Scholar]
- O’Sullivan, D.P.; O’Mahony, D.; Parsons, C.; Hughes, C.; Murphy, K.; Patterson, S.; Byrne, S. A prevalence study of potentially inappropriate prescribing in Irish long-term care residents. Drugs Aging 2013, 30, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Ubeda, A.; Ferrandiz, M.L.; Maicas, N.; Gomez, C.; Bonet, M.; Peris, J.E. Potentially inappropriate prescribing in institutionalised older patients in Spain: The STOPP-START criteria compared with the Beers criteria. Pharm. Pract. 2012, 10, 83–91. [Google Scholar] [CrossRef]
- Aspinall, S.L.; Zhao, X.; Semla, T.P.; Cunningham, F.E.; Paquin, A.M.; Pugh, M.J. Epidemiology of Drug-Disease Interactions in Older Veteran Nursing Home Residents. J. Am. Geriatr. Soc. 2015, 63, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.S.; Misiaszek, B.C.; Brymer, C. Improving prescribing in the elderly: A study in the long-term care setting. Can. J. Clin. Pharmacol. 2001, 8, 78–83. [Google Scholar] [PubMed]
- Nightingale, G.; Hajjar, E.; Swartz, K.; Andrel-Sendecki, J.; Chapman, A. Evaluation of a pharmacist-led medication assessment used to identify prevalence of and associations with polypharmacy and potentially inappropriate medication use among ambulatory senior adults with cancer. J. Clin. Oncol. 2015, 33, 1453–1459. [Google Scholar] [CrossRef] [PubMed]
- Suehs, B.T.; Davis, C.; Franks, B.; Yuran, T.E.; Ng, D.; Bradt, J.; Knispel, J.; Vassilakis, M.; Berner, T. Effect of Potentially Inappropriate Use of Antimuscarinic Medications on Healthcare Use and Cost in Individuals with Overactive Bladder. J. Am. Geriatr. Soc. 2016, 64, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Duffield, C.; Diers, D.; O’Brien-Pallas, L.; Aisbett, C.; Roche, M.; King, M.; Aisbett, K. Nursing Staffing, Nursing Workload, the Work Environment and Patient Outcomes. Appl. Nurs. Res. 2011, 24, 244–255. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, P.; Barry, P.; O’Mahony, D. Inappropriate prescribing in the elderly. J. Clin. Pharm. Ther. 2007, 32, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, H.J.; Gallagher, P.F.; O’Mahony, D. Inappropriate prescribing and adverse drug events in older people. BMC Geriatr. 2009, 9, 5. [Google Scholar] [CrossRef] [PubMed]
- Anrys, P.; Boland, B.; Degryse, J.; Lepeleire, J.; Petrovic, M.; Marien, S.; Dalleur, O.; Strauven, G.; Foulon, V.; Spinewine, A. STOPP/START version 2—Development of software applications: Easier said than done? Age Ageing 2016, 45, 589–592. [Google Scholar] [CrossRef] [PubMed]
- Walsh, K.A.; O’Riodan, D.; Kearney, P.M.; Timmons, S.; Byrne, S. Improving the appropriateness of prescribing in older patients: A systematic review and meta-analysis of pharmacists’ interventions in secondary care. Age Ageing 2016, 45, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Soiza, R.L.; Subbarayan, S.; Antonio, C.; Cruz-Jentoft, A.J.; Petrovic, M.; Gudmundsson, A.; O’Mahony, D. The SENATOR project: Developing and trialling a novel software engine to optimize medications and nonpharmacological therapy in older people with multimorbidity and polypharmacy. Ther. Adv. Drug Saf. 2017, 8, 81–85. [Google Scholar] [CrossRef] [PubMed]
| Inclusion Criteria | |
| |
| |
|
|
| |
| Exclusion Criteria | |
| |
| |
| Type of Data | Data Collected |
|---|---|
| Demographic data | Age, gender |
| Medications | Number of chronic medications, identified PIM(s) related to drug-disease interactions under selected STOPP version 2 criteria as shown in Table 3 |
| Comorbidities | Type of comorbidities, number of comorbidities |
| Readmission | Records of emergency readmission within 28 days of discharge |
| Drugs | Interacting Disease State |
|---|---|
| Diltiazem or verapamil | NYHA class III or IV heart failure |
| Tricyclic antidepressants (TCAs) | dementia, narrow angle glaucoma, cardiac conduction abnormalities, prostatism, prior history of urinary retention |
| Chlorpromazine, Clozapine, flupenthixol, zuclopenthixol * | History of prostatism or previous urinary retention |
| Antipsychotics (i.e., other than quetiapine or clozapine) | Parkinsonism, Lewy Body disease |
| Anticholinergics/antimuscarinics | Dementia, delirium, chronic cognitive impairment narrow angle glaucoma, chronic prostatism |
| Prochlorperazine or metoclopramide | Parkinsonism |
| Antimuscarinic bronchodilators | History of narrow angle glaucoma or bladder outflow obstruction |
| Non-selective beta blocker | History of asthma requiring treatment |
| COX-2 NSAID (celecoxib, etoricoxib, parecoxib) | Cardiovascular disease |
| Oral bisphosphonate | Gastrointestinal disease |
| Oestrogens | History of breast cancer or venous thromboembolism (VTE) |
| Thiazolidenediones (Pioglitazone, Rosiglitazone) | Heart Failure |
| Possible Factors Influencing Readmission | Raw OR (95% CI) | p | |
|---|---|---|---|
| Age | <83 years old | 1.447 (0.711, 2.944) | 0.308 |
| ≥83 years old | |||
| Gender | Male | 0.723 (0.356, 1.469) | 0.370 |
| Female | |||
| Number of chronic medications | <6 | 1.517 (0.660, 3.490) | 0.327 |
| ≥6 | |||
| Number of comorbidities | <5 | 0.993 (0.486, 2.026) | 0.984 |
| ≥5 | |||
| PIM(s) identified | Yes | 6.476 (2.996, 13.988) | <0.001 |
| No | |||
| PIM(s) associated with the use of | |||
| TCAs | 1.476 (0.130, 16.702) | 0.753 | |
| Anticholinergics/antimuscarinics | 7.920 (3.518, 17.828) | <0.001 | |
| Antimuscarinic bronchodilators | 2.484 (0.635, 9.724) | 0.191 | |
| Arrhythmia | 0.507 (0.215, 1.196) | 0.121 | |
| Asthma | 2 (0.323, 12.401) | 0.457 | |
| Cancer | 1.298 (0.464, 3.627) | 0.619 | |
| COPD | 0.758 (0.237, 2.425) | 0.640 | |
| Delirium | 1.072 (0.322, 3.566) | 0.910 | |
| Dementia | 0.576 (0.065, 5.073) | 0.619 | |
| Diabetes | 0.713 (0.348, 1.459) | 0.354 | |
| Gastrointestinal disorder | 5.405 (1.233, 23.699) | 0.025 | |
| Glaucoma | 2.053 (0.550, 7.661) | 0.285 | |
| Gout | 3.490 (1.479, 8.238) | 0.004 | |
| Heart failure | 1.492 (0.672, 3.312) | 0.325 | |
| Hyperlipidemia | 0.809 (0.387, 1.690) | 0.572 | |
| Hypertension | 0.805 (0.385, 1.683) | 0.564 | |
| Ischemic heart disease | 0.777 (0.367, 1.645) | 0.510 | |
| Liver disease | 0.712 (0.191, 2.655) | 0.612 | |
| Myocardial infarction | 1.527 (0.492, 4.755) | 0.465 | |
| Parkinsonism | 0.576 (0.065, 5.073) | 0.619 | |
| Prostatism | 0.576 (0.184, 1.802) | 0.343 | |
| Psychiatric disorder | 0.713 (0.348, 1.459) | 0.354 | |
| Renal disease | 1.836 (0.815, 4.140) | 0.143 | |
| Stroke | 1.095 (0.424, 2.823) | 0.851 | |
| Urine retention | 1.338 (0.509, 3.517) | 0.555 | |
| Readmission Factors | Adjusted OR (95%CI) | p Value |
|---|---|---|
| PIM(s) identified | 6.557 (2.889, 14.971) | <0.000 |
| Gastrointestinal disorder | 3.718 (0.742, 18.622) | 0.110 |
| Gout | 4.344 (1.666, 11.323) | 0.003 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lau, M.H.M.; Tenney, J.W. Evaluation of Drug-Disease Interactions and Their Association with Unplanned Hospital Readmission Utilizing STOPP Version 2 Criteria. Geriatrics 2017, 2, 33. https://doi.org/10.3390/geriatrics2040033
Lau MHM, Tenney JW. Evaluation of Drug-Disease Interactions and Their Association with Unplanned Hospital Readmission Utilizing STOPP Version 2 Criteria. Geriatrics. 2017; 2(4):33. https://doi.org/10.3390/geriatrics2040033
Chicago/Turabian StyleLau, Mandy Hau Man, and Justin W. Tenney. 2017. "Evaluation of Drug-Disease Interactions and Their Association with Unplanned Hospital Readmission Utilizing STOPP Version 2 Criteria" Geriatrics 2, no. 4: 33. https://doi.org/10.3390/geriatrics2040033
APA StyleLau, M. H. M., & Tenney, J. W. (2017). Evaluation of Drug-Disease Interactions and Their Association with Unplanned Hospital Readmission Utilizing STOPP Version 2 Criteria. Geriatrics, 2(4), 33. https://doi.org/10.3390/geriatrics2040033