
Healthcare and End-of-Life Needs of Lesbian, Gay, Bisexual, and Transgender (LGBT) Older Adults: A Scoping Review


Abstract
:1. Introduction
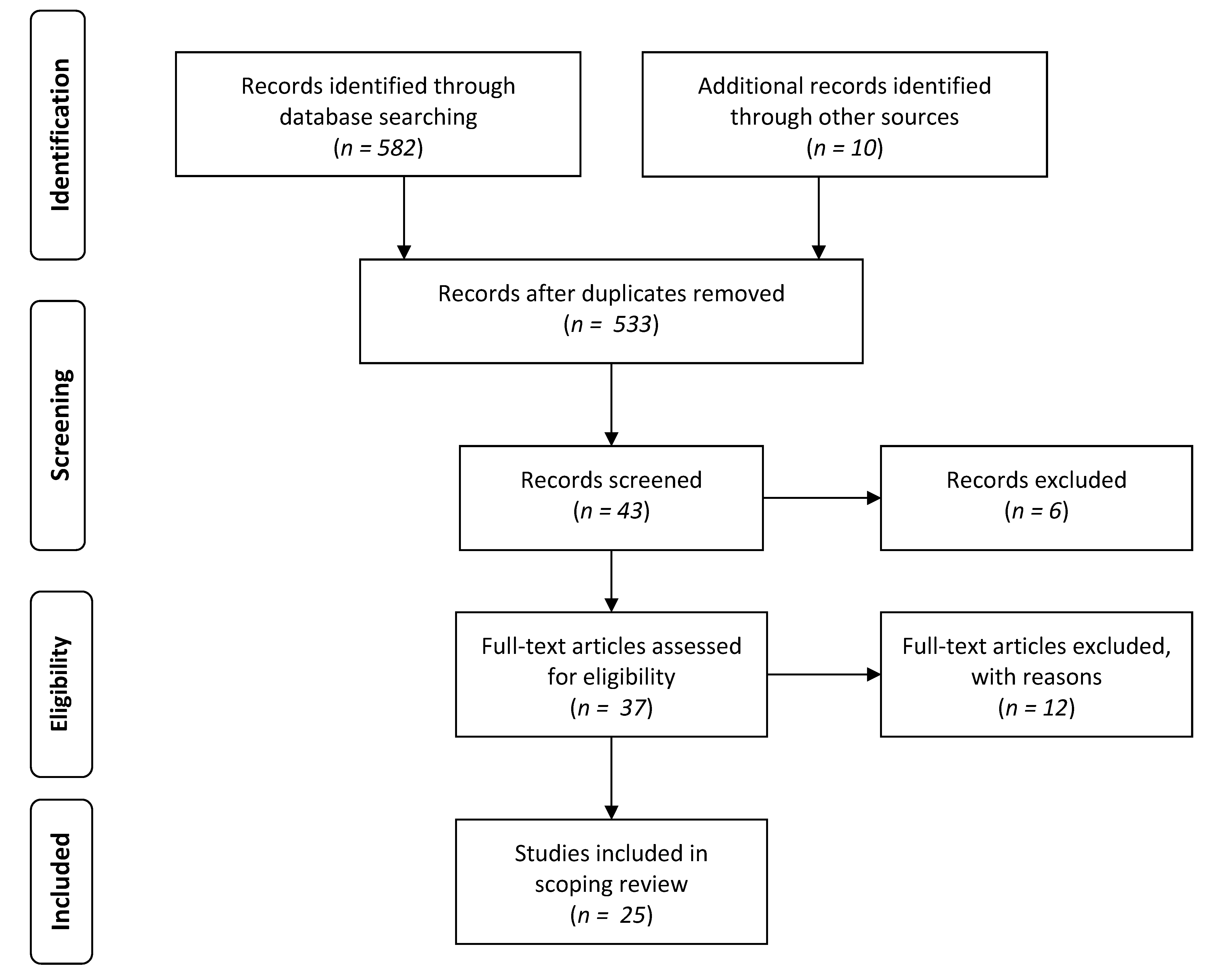
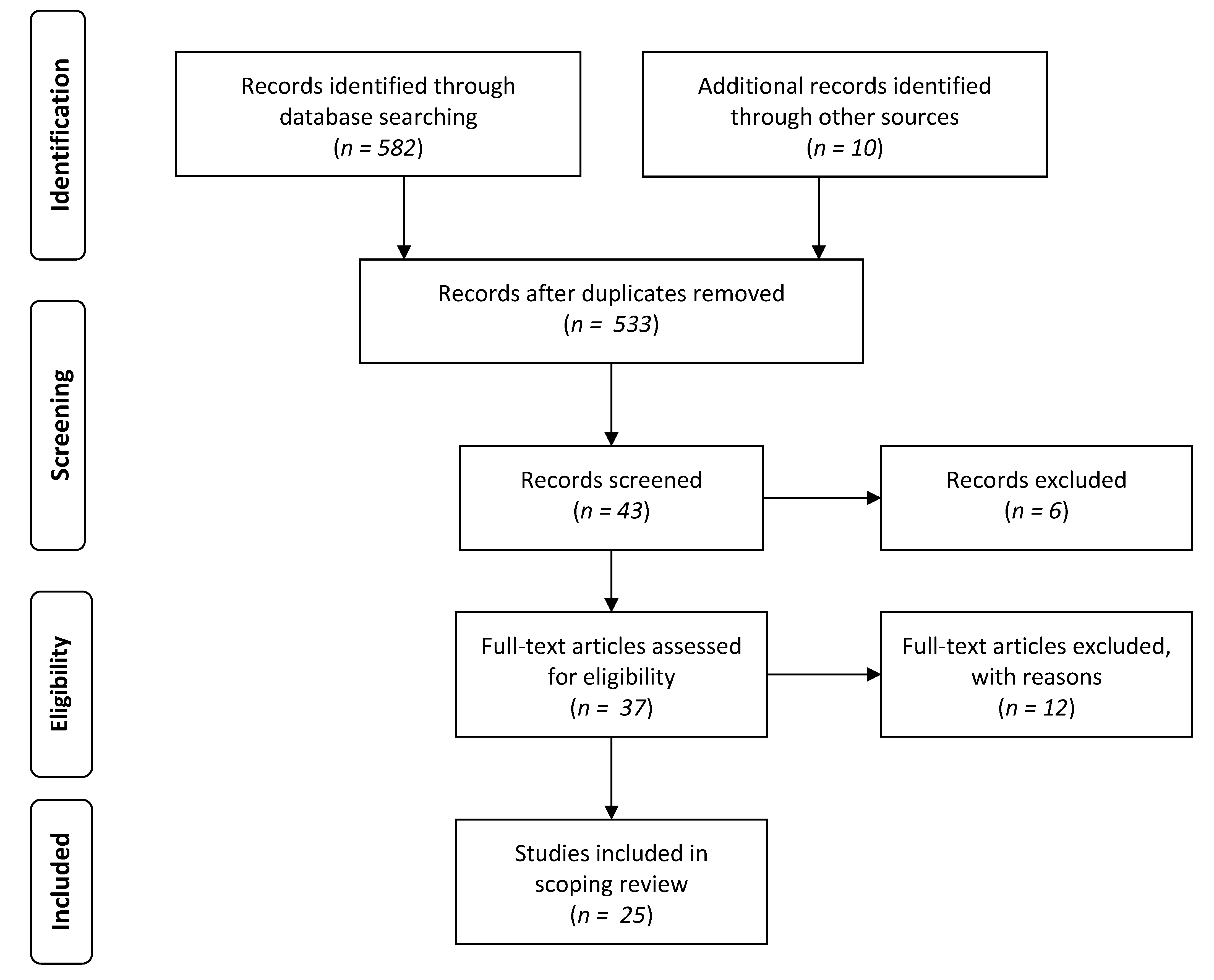
2. Method
3. Results
- social support and chosen family;
- intimacy;
- health status;
- fear of discrimination and lack of trust;
- lack of knowledge and preparedness; and
- cultural competence in the healthcare system.
3.1. Social Support and Chosen Family
3.2. Intimacy
3.3. Health Status
3.4. Fear of Discrimination and Lack of Trust
3.5. Lack of Knowledge and Preparedness
3.6. Cultural Competence in the Healthcare System
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A.

{kind=link}
| No. | Author Information | Sample Information | Research Design | Relevant Themes |
|---|---|---|---|---|
| 1 | Brotman et al. 2007 [8] | Age: Range = 33–72; mean/median = n/a 1a Gender: M and F Sample Size: 17 Location: Quebec, British Columbia, Halifax | Method: QualitativeDesign: Cross-sectional Collection: Interviews Analysis: Qualitative analysis | Social support and chosen family, fear of discrimination and lack of trust, |
| 2 | Griebling 2016 [9] | n/a | Design: Synthesis paper | Social support and chosen family, intimacy, health status, cultural competence in the healthcare system |
| 3 | Metlife Mature Market Institute et al. 2010 [10] | Age: Range = 40–61; mean/median = n/a Gender: M and F including ftm and mtf transgender individuals Sample Size: 1000 Location: United States, Canada, Thailand, Australia, Sweden, Mexico | Method: Mixed-method Design: Cross-sectional Collection: Interviews and Questionnaires Analysis: descriptive statistics, confidence intervals, | Social support and chosen family, lack of knowledge and preparedness |
| 4 | Almack et al. 2010 [11] | Age: Range = 55–84; mean/median = n/a 2a Gender: M and F Sample Size: 15 Location: United Kingdom | Method: Qualitative Design: Cross-sectional Collection: Focus groups Analysis: Qualitative analysis | Social support and chosen family |
| 5 | Harding et al. 2012 [24] | n/a | Design: Synthesis paper | Lack of knowledge and preparedness, cultural competence in the healthcare system |
| 6 | Corbett 2007 [26] | Age: Range = 23–65; mean/median = n/a Gender: M and F Sample Size: 27 Location: Uppsala, Sweden | Method: Qualitative Design: Cross-sectional Collection: Interviews Analysis: Qualitative analysis | Cultural competence in the healthcare system |
| 7 | Rawlings 2012 [7] | n/a | Design: Synthesis paper | Social support and chosen family, fear of discrimination and lack of trust, Cultural competence in the healthcare system |
| 8 | Aldredge et al. 2012 [27] | Age: Range = n/a 3a; mean/median = n/a 3a Gender: M and F Sample Size: 6 Location: United States | Method: Qualitative Design: Cross-sectional Collection: Reflective works Analysis: Qualitative analysis | Cultural competence in the healthcare system |
| 9 | Lawton et al. 2014 [28] | n/a | Design: Synthesis paper | Cultural competence in the healthcare system |
| 10 | Arthur 2015 [16] | n/a | Design: Synthesis paper | Cultural competence in the healthcare system, fear of discrimination and lack of trust |
| 11 | Duffy et al. 2014 [29] | Age: Range = early 60s–78; mean/median = n/a Gender: M and F Sample Size: 4 Location: Sydney, Australia | Method: Qualitative Design: Case-study Collection: Interview Analysis: Qualitative analysis | Cultural competence in the healthcare system |
| 12 | Kimmel 2014 [12] | n/a | Design: Synthesis paper | Health status, fear of discrimination and lack of trust, cultural competence in the healthcare system |
| 13 | Porter et al. 2014 [30] | Age: Range = n/a 4a; mean/median = n/a 4a Gender: M and F Sample Size: 76 Location: United States | Method: Quantitative Design: Case series Collection: Questionnaires Analysis: Descriptive statistics, t-tests, chi-square analyses, ANOVAs, | Cultural competence in the healthcare system |
| 14 | Price 2005 [1] | n/a | Design: Synthesis paper | Cultural competence in the healthcare system, fear of discrimination and lack of trust |
| 15 | Hughes et al. 2014 [20] | Age: Range = <40 to 70+; mean/median = n/a Gender: M, F, Transgender, Intersex Sample Size: 305 Location: New South Wales, Australia | Method: Mixed-method Design: Cross-sectional Collection: Questionnaires Analysis: Qualitative analysis, descriptive statistics, chi-square | Lack of knowledge and preparedness |
| 16 | Hughes et al. 2015 [21] | Age: Range = <40 to 70+; mean/median = n/a Gender: M, F, Transgender, Intersex Sample Size: 305 Location: New South Wales, Australia | Method: Mixed-method Design: Cross-sectional Collection: Qualitative analysis, descriptive statistics, chi-square analysis, bivariate analysis | Lack of knowledge and preparedness |
| 17 | Cartwright et al. 2012 [23] | Age: Range = n/a; mean/median = n/a 4a Gender: M and F Sample Size: 25 Location: New South Wales, Australia | Method: Qualitative Design: Cross-sectional Collection: Interviews Analysis: Qualitative analysis | Lack of knowledge and preparedness, |
| 18 | Powell et al. 2012 [25] | n/a | Design: Synthesis paper | Lack of knowledge and preparedness |
| 19 | Witten et al. 2014 [15] | Age: Range = 18 to 51 and over ; mean/median = n/a Gender: mtf and ftm transgender Sample Size: 1,963 Location: United States, Canada, Thailand, Australia, Sweden, Mexico | Method: Mixed Method Design: Cross-sectional Collection: Questionnaires, Interviews Analysis: Means, descriptive statistics, confidence intervals, chi-square analysis, t-tests, qualitative analysis, | Fear of discrimination and lack of trust, lack of knowledge and preparedness |
| 20 | Witten et al. 2015 [22] | Age: Range = 18 to 51 and over; mean/median = n/a Gender: transgender 5a Sample Size: 276 Location: United States, Canada, Thailand, Australia, Sweden, Mexico | Method: Mixed Method Design: Cross-sectional Collection: Questionnaires, Interviews Analysis: Means, descriptive statistics, confidence intervals, chi-square, t-test, qualitative analysis, | Lack of knowledge and preparedness, Fear of discrimination and lack of trust |
| 21 | Hash et al. 2007 [17] | Age: Range = 50–77; mean = 60 Gender: M and F Sample Size: 19 Location: United States | Method: Qualitative Design: Cross-sectional Collection: Interviews Analysis: Qualitative analysis, descriptive statistics | Fear of discrimination and lack of trust |
| 22 | June et al. 2012 [18] | Age: Range = 60–81; mean = 64.8 Gender: F Sample Size: 30 Location: Colorado, United States | Method: Quantitative Design: Cross-sectional Collection: Questionnaire Analysis: t-tests, chi-square, analysis of covariance (ANCOVA), | Fear of discrimination and lack of trust |
| 23 | Averett et al. 2011 [19] | Age: Range= 51–86; median = 62 Gender: F Sample Size: 456 Location: United States | Method: Mixed-method Design: Cross-sectional Collection: Questionnaire Analysis: Descriptive statistics, means | Fear of discrimination and lack of trust |
| 24 | Masini et al. 2008 [13] | Age: Range = 50–79; mean = 57 Gender: M and F Sample Size: 220 Location: United States | Method: Quantitative Design: Cross-sectional Collection: Questionnaire Analysis: Descriptive statistics, multiple regression, chi-square analysis, frequencies | Health status |
| 25 | McGovern 2014 [14] | n/a | Design: Synthesis paper | Health status |
References
- Price, E. All but invisible: Older gay men and lesbians: the sexuality of older people, and gay and lesbian sexuality in particular, is an issue that has largely been ignored in the nursing literature. But, says Elizabeth Price, older gay men and lesbians are becoming more vociferous about the health and social care services they have a right to expect. Nursing Older People 2005, 17, 16–18. [Google Scholar] [PubMed]
- Ottawa Senior Pride Network & Ipsos Reid. Housing Survey; Ipsos Reid: Ottawa, ON, Canada, October 2015. [Google Scholar]
- Hatzenbuehler, M.L.; Bellatorre, A.; Lee, Y.; Finch, B.K.; Muennig, P.; Fiscella, K. Structural stigma and all-cause mortality in sexual minority populations. Soc. Sci. Med. 2014, 103, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Brotman, S.; Ferrer, I.; Sussman, T.; Ryan, B.; Richard, B. Access and equity in the design and delivery of health and social care to LGBTQ older adults: A Canadian perspective. In The Lives of LGBT Older Adults: Understanding Challenges and Resilience; Orel, N., Fruhauf, C., Eds.; American Psychological Association: Washington, DC, USA, 2014. [Google Scholar]
- Arksey, H.; O’Malley, L. Scoping studies: towards a methodological framework. Int. J. Soc. Res. Meth. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed]
- Rawlings, D. End-of-life care considerations for gay, lesbian, bisexual, and transgender individuals. Int. J. Palliat. Nurs. 2012, 18, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Brotman, S.; Ryan, B.; Collins, S.; Chamberland, L.; Cormier, R.; Julien, D.; Meyer, E.; Peterkin, A.; Richard, B. Coming out to care: Caregivers of gay and lesbian seniors in Canada. Gerontologist. 2007, 47, 490–503. [Google Scholar] [CrossRef] [PubMed]
- Griebling, T.L. Sexuality and aging: A focus on lesbian, gay, bisexual, and transgender (LGBT) needs in palliative and end of life care. Curr. Opin. Support. Palliat. Care 2016, 10, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Metlife Mature Market Institute®2; The Lesbian And Gay Aging Issues Network of The American Society On Aging. Out and Aging: The MetLife Study of Lesbian and Gay Baby Boomers 1. J. GLBT Fam. Stud. 2010, 6, 40–57. [Google Scholar]
- Almack, K.; Seymour, J.; Bellamy, G. Exploring the Impact of Sexual Orientation on Experiences and Concerns about End of Life Care and on Bereavement for Lesbian, Gay and Bisexual Older People. Sociology 2010, 44, 908–924. [Google Scholar] [CrossRef]
- Kimmel, D. Lesbian, Gay, Bisexual, and Transgender Aging Concerns. Clin. Gerontol. 2014, 37, 49–63. [Google Scholar] [CrossRef]
- Masini, B.E.; Barrett, H.A. Social Support as a Predictor of Psychological and Physical Well-Being and Lifestyle in Lesbian, Gay, and Bisexual Adults Aged 50 and Over. J. Gay Lesbian Soc. Services 2008, 20, 91–110. [Google Scholar] [CrossRef]
- McGovern, J. The Forgotten: Dementia and the Aging LGBT Community. J. Gerontol. Soc. Work 2014, 57, 845–857. [Google Scholar] [CrossRef] [PubMed]
- Witten, T.M. End of life, chronic illness, and trans-identities. J. Soc. Work End Life Palliat. Care 2014, 10, 34–58. [Google Scholar] [CrossRef] [PubMed]
- Arthur, D.P. Social Work Practice with LGBT Elders at End of Life: Developing Practice Evaluation and Clinical Skills Through a Cultural Perspective. J. Soc. Work End Life Palliat. Care 2015, 11, 178–201. [Google Scholar] [CrossRef] [PubMed]
- Hash, K.M.; Netting, F.E. Long-term planning and decision-making among midlife and older gay men and lesbians. J. Soc. Work End Life Palliat. Care 2007, 3, 59–77. [Google Scholar] [CrossRef] [PubMed]
- June, A.; Segal, D.L.; Klebe, K.; Klebe, L.K. Views of Hospice and Palliative Care Among Younger and Older Sexually Diverse Women. Am. J. Hosp. Palliat. Med. 2012, 29, 455–461. [Google Scholar]
- Averett, P.; Yoon, I.; Jenkins, C.L. Older Lesbians: Experiences of Aging, Discrimination and Resilience. J. Women Aging 2011, 23, 216–232. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.; Cartwright, C. LGBT people’s knowledge of and preparedness to discuss end-of-life care planning options. Health Soc. Care Community 2014, 22, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.; Cartwright, C. Lesbian, gay, bisexual and transgender people’s attitudes to end-of-life decision-making and advance care planning: LGBT people and advance care planning. Australas. J. Ageing 2015, 34, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Witten, T.M. Elder Transgender Lesbians: Exploring the Intersection of Age, Lesbian Sexual Identity, and Transgender Identity. J. Lesbian Stud. 2015, 19, 73–89. [Google Scholar] [CrossRef] [PubMed]
- Cartwright, C.; Hughes, M.; Lienert, T. End-of-life care for gay, lesbian, bisexual and transgender people. Cult. Health Sex. 2012, 14, 537–548. [Google Scholar] [CrossRef] [PubMed]
- Harding, R.; Epiphaniou, E.; Chidgey-Clark, J. Needs, Experiences, and Preferences of Sexual Minorities for End-of-Life Care and Palliative Care: A Systematic Review. J. Palliat. Med. 2012, 15, 602–611. [Google Scholar] [CrossRef] [PubMed]
- Powell, L.A.; Neustifter, R. An Updated Social Context for Therapy with Elder Lesbian Couples. J. Fem. Fam. Ther. 2012, 24, 213–229. [Google Scholar] [CrossRef]
- Corbett, K. Lesbian women and gay men found that nurses often assumed they were heterosexual, which led to feelings of discomfort and insecurity. Evidence-Based Nursing 2007, 10, 94. [Google Scholar] [CrossRef] [PubMed]
- Aldredge, P.A.; Conlon, A. Reflections: Gay Men and Lesbians at End-of-Life. J. Soc. Work End-Of-Life Palliat. Care 2012, 8, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Lawton, A.; White, J.; Fromme, E.K. End-of-Life and Advance Care Planning Considerations for Lesbian, Gay, Bisexual, and Transgender Patients #275. J. Palliat. Med. 2014, 17, 106–108. [Google Scholar] [PubMed]
- Duffy, F. , Healy, J.P. A Social Work Practice Reflection on Issues Arising for LGBTI Older People Interfacing With Health and Residential Care: Rights, Decision Making and End-of-Life Care. Soc. Work Health Care 2014, 53, 568–583. [Google Scholar] [CrossRef] [PubMed]
- Porter, K.E.; Krinsky, L. Do LGBT Aging Trainings Effectuate Positive Change in Mainstream Elder Service Providers? J. Homosex. 2014, 61, 197–216. [Google Scholar] [CrossRef] [PubMed]
- Marie, Curie. “Hiding who I am” The reality of end of life care for LGBT people [Internet]. Available online: https://www.mariecurie.org.uk/globalassets/media/documents/policy/policy-publications/june-2016/reality-end-of-life-care-lgbt-people.pdf (accessed on 14 February 2017).
- Dementia, Transgender & Intersex People: Do service providers really know what their needs are? Alzheimer’s Australia: Canberra, Australia, 2014.
- Bengston, V.L.; Elder, G.H.; Putney, N.M. The Lifecourse Perspective on Ageing: Linked Lives, Timing and History. In The Cambridge Handbook of Age and Ageing; Johnson, M.L., Ed.; Cambridge University Press: Cambridge, UK, 2005; pp. 493–501. [Google Scholar]
- Egale Canada. FAQ – About C–279. Gender Identity Bill. [Internet]. Available online: http://trans.egale.ca/faq-about-c-279/ (accessed on 8 June 2016).
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stinchcombe, A.; Smallbone, J.; Wilson, K.; Kortes-Miller, K. Healthcare and End-of-Life Needs of Lesbian, Gay, Bisexual, and Transgender (LGBT) Older Adults: A Scoping Review. Geriatrics 2017, 2, 13. https://doi.org/10.3390/geriatrics2010013
Stinchcombe A, Smallbone J, Wilson K, Kortes-Miller K. Healthcare and End-of-Life Needs of Lesbian, Gay, Bisexual, and Transgender (LGBT) Older Adults: A Scoping Review. Geriatrics. 2017; 2(1):13. https://doi.org/10.3390/geriatrics2010013
Chicago/Turabian StyleStinchcombe, Arne, Jeffrey Smallbone, Kimberley Wilson, and Katherine Kortes-Miller. 2017. "Healthcare and End-of-Life Needs of Lesbian, Gay, Bisexual, and Transgender (LGBT) Older Adults: A Scoping Review" Geriatrics 2, no. 1: 13. https://doi.org/10.3390/geriatrics2010013
APA StyleStinchcombe, A., Smallbone, J., Wilson, K., & Kortes-Miller, K. (2017). Healthcare and End-of-Life Needs of Lesbian, Gay, Bisexual, and Transgender (LGBT) Older Adults: A Scoping Review. Geriatrics, 2(1), 13. https://doi.org/10.3390/geriatrics2010013