
Muscle Strength and Functional Ability in Recreational Female Golfers and Less Active Non-Golfers over the Age of 80 Years


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Recruitment
2.2. Protocol
2.2.1. Handgrip Strength
2.2.2. Quadriceps Strength
2.2.3. Timed Up and Go (TUG)
2.3. Data Analysis
3. Results
3.1. Demographic Details
3.2. Physical Function Tests
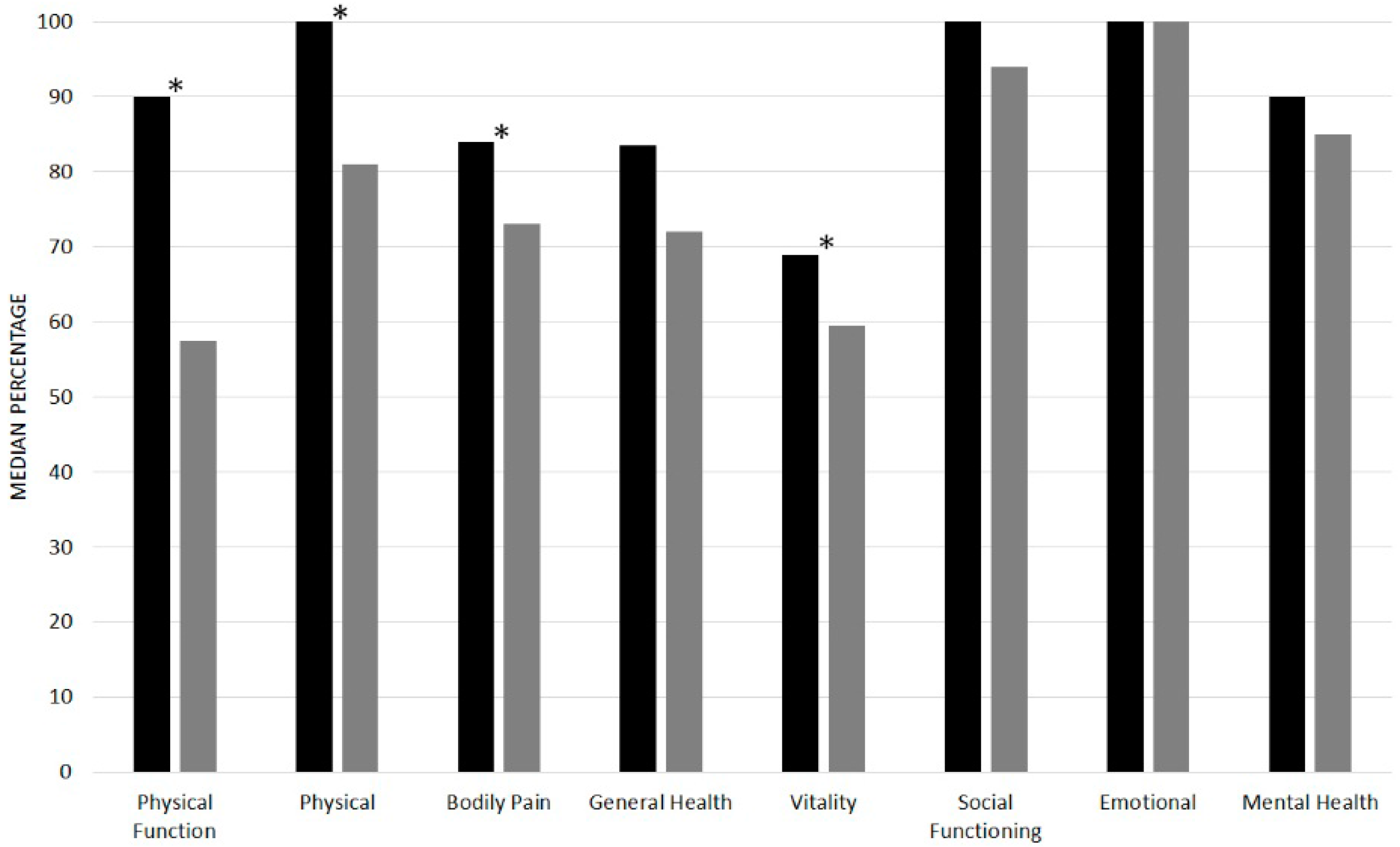
3.3. Quality of Life
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- (ONS) OfNS. National Population Projects, 2012-Based Statistical Bulletin 2012. Available online: http://www.ons.gov.uk/ons/dcp171778_334975.pdf (accessed on 1 March 2017).
- Lauretani, F.; Russo, C.R.; Bandinelli, S.; Bartali, B.; Cavazzini, C.; di Iorio, A.; Corsi, A.M.; Rantanen, T.; Guralnik, J.M.; Ferrucci, L.; et al. Age-associated changes in skeletal muscles and their effect on mobility: An operational diagnosis of sarcopenia. J. Appl. Physiol. 2003, 95, 1851–1860. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E.; Abbatecola, A.M.; Argiles, J.M.; Baracos, V.; Bauer, J.; Bhasin, S.; Cederholm, D.; Fearon, K.; Ferrucci, L.; Inui, A.; et al. Sarcopenia with limited mobility: An international consensus. J. Am. Med. Dir. Assoc. 2011, 12, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Von Haehling, S.; Morley, J.E.; Anker, S.D. An overview of sarcopenia: Facts and numbers on prevalence and clinical impact. J. Cachexia Sarcopenia Muscle 2010, 1, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Frontera, W.R.; Hughes, V.A.; Fielding, R.A.; Fiatarone, M.A.; Evans, W.J.; Roubenoff, R. Aging of skeletal muscle: A 12-yr longitudinal study. J. Appl. Physiol. 2000, 88, 1321–1326. [Google Scholar] [PubMed]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J. American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Marzetti, E.; Martone, A.M.; Bernabei, R.; Onder, G. Exercise as a remedy for sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 25–31. [Google Scholar] [CrossRef] [PubMed]
- BHF. Interpreting the UK Physical Activity Guidelines for Older Adults (65+) 2012. Available online: www.bhfactive.org.uk/userfiles/Documents/frailerolderadults.pdf (accessed on 1 March 2017).
- CMOARHi. Transforming Scotland’s Health; Scottish Government: Scotland, UK, 2011; pp. 13–15.
- Organisation WH. Global Recommendations on Physical Activity for Health: 65 Years and above; World Health Organisation: Geneva, Switzerland, 2011. [Google Scholar]
- Lindsay, D.M.; Horton, J.F.; Vandervoort, A.A. A review of injury characteristics, aging factors and prevention programmes for the older golfer. Sports Med. 2000, 30, 89–103. [Google Scholar] [CrossRef] [PubMed]
- Parkkari, J.; Natri, A.; Kannus, P.; Mänttäri, A.; Laukkanen, R.; Haapasalo, H.; Nenonen, A.; Pasanen, M.; Oja, P.; Vuori, L.; et al. A controlled trial of the health benefits of regular walking on a golf course. Am. J. Med. 2000, 109, 102–108. [Google Scholar] [CrossRef]
- Tsang, W.W.; Hui-Chan, C.W. Effects of exercise on joint sense and balance in elderly men: Tai Chi versus golf. Med. Sci. Sports Exerc. 2004, 36, 658–667. [Google Scholar] [CrossRef] [PubMed]
- Murray, A.; Daines, L.; Archibald, D.; Hawkes, R.; Grant, L.; Mutrie, N. The relationship and effects of golf on physical and mental health: A scoping review protocol. Br. J. Sports Med. 2016, 50, 647–650. [Google Scholar] [CrossRef]
- Roberts, H.C.; Syddall, H.E.; Cooper, C.; Sayer, A.A. Is grip strength associated with length of stay in hospitalised older patients admitted for rehabilitation? Findings from the Southampton grip strength study. Age Ageing 2012, 41, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Syddall, H.; Cooper, C.; Martin, F.; Briggs, R.; Sayer, A.A. Is grip strength a useful single marker of frailty? Age Ageing 2003, 32, 650–656. [Google Scholar] [CrossRef] [PubMed]
- Hairi, N.N.; Cumming, R.G.; Naganathan, V.; Handelsman, D.J.; le Couteur, D.G.; Creasey, H.; Waite, L.M.; Seibel, M.J.; Sambrook, P.N. Loss of muscle strength, mass (sarcopenia), and quality (specific force) and its relationship with functional limitation and physical disability: The Concord Health and Ageing in Men Project. J. Am. Geriatr. Soc. 2010, 58, 2055–2062. [Google Scholar] [CrossRef] [PubMed]
- Skelton, D.A.; Kennedy, J.; Rutherford, O.M. Explosive power and asymmetry in leg muscle function in frequent fallers and non-fallers aged over 65. Age Ageing 2002, 31, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Samuel, D.; Wilson, K.; Martin, H.J.; Allen, R.; Sayer, A.A.; Stokes, M. Age-associated changes in hand grip and quadriceps muscle strength ratios in healthy adults. Aging Clin. Exp. Res. 2012, 24, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [PubMed]
- Beauchet, O.; Fantino, B.; Allali, G.; Muir, S.; Montero-Odasso, M.; Annweiler, C. Timed Up and Go test and risk of falls in older adults: A systematic review. J. Nutr. Health Aging 2011, 15, 933–938. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Washburn, R.A.; McAuley, E.; Katula, J.; Mihalko, S.L.; Boileau, R.A. The physical activity scale for the elderly (PASE): Evidence for validity. J. Clin. Epidemiol. 1999, 52, 643–651. [Google Scholar] [CrossRef]
- Vermeulen, J.; Neyens, J.; Spreeuwenbery, M.; van Rossum, E.; Hewson, D.; de Witte, L. Measuring Grip Strength in Older Adults: Comparing the Grip-ball With the Jamar Dynamometer. J. Geriatr. Phys. Ther. 2015, 38, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Martinez, B.P.; Gomes, I.B.; Oliveira, C.S.D.; Ramos, I.R.; Rocha, M.D.M.; Forgiarini Júnior, L.A.; Camelier, F.W.R.; Camelier, A.A. Accuracy of the Timed Up and Go test for predicting sarcopenia in elderly hospitalized patients. Clinics 2015, 70, 369–372. [Google Scholar] [CrossRef]
- Barnes, J.; Adams, J. Differences in dominant and non-dominant handgrip strength of male golf professionals measured using the Jamar Dynamometer. Br. J. Hand Ther. 2007, 12, 112–116. [Google Scholar]
- Sayer, A.A.; Syddall, H.E.; Martin, H.J.; Dennison, E.M.; Roberts, H.C.; Cooper, C. Is grip strength associated with health-related quality of life? Findings from the Hertfordshire Cohort Study. Age Ageing 2006, 35, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Reid, K.F.; Pasha, E.; Doros, G.; Clark, D.J.; Patten, C.; Phillips, E.M.; Frontera, W.R.; Fielding, R.A. Longitudinal decline of lower extremity muscle power in healthy and mobility-limited older adults: Influence of muscle mass, strength, composition, neuromuscular activation and single fiber contractile properties. Eur. J. Appl. Physiol. 2014, 114, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Hunter, S.K.; Thompson, M.W.; Adams, R.D. Relationships among age-associated strength changes and physical activity level, limb dominance, and muscle group in women. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2000, 55, B264–B273. [Google Scholar] [CrossRef]
- Martin, H.; Yule, V.; Syddall, H.; Dennison, E.; Cooper, C.; Aihie Sayer, A. Is hand-held dynamometry useful for the measurement of quadriceps strength in older people? A comparison with the gold standard Biodex dynamometry. Gerontology 2006, 52, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Kanehisa, H.; Ikegawa, S.; Fukunaga, T. Comparison of Muscle Cross-Sectional Area and Strength between Untrained Women and Men. Eur. J. Appl. Physiol. Occup. Physiol. 1994, 68, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Herrick, I.; Brown, S.; Agyapong-Badu, S.; Warner, M.; Ewings, S.; Samuel, D.; Stokes, D. Anterior thigh tissue thickness measured using ultrasound imaging in older recreational female golfers and sedentary controls. Geriatrics 2017, 2, 10. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Golfer (n = 21) | Non-Golfer (n = 10) |
|---|---|---|
| Age (years) | 82.9 ± 2.1 (80–87) | 80.8 * ± 1.03 (80–83) |
| Height (m) | 1.59 ± 0.05 (1.51–1.65) | 1.57 ± 0.06 (1.47–1.67) |
| Weight (kg) | 62.3 ± 9.22 (46.9–78.8) | 66.2 ± 12.76 (53.4–93.8) |
| BMI (kg/cm²) | 24.7 ± 3.55 (18.78–31.93) | 26.77 ± 4.4 (20.78–33.84) |
| Function | Golfer | Non-Golfer | p Value |
|---|---|---|---|
| Handgrip/BW (kgF/kg) | 0.33 ± 0.06 (0.24–0.46) (n = 20) | 0.29 ± 0.06 (0.24–0.39) (n = 9) | 0.051 |
| Quads/BW (N/kg) | 2.78 ± 0.74 (1.6–4.4) (n = 19) | 2.69 ± 0.83 (1.71–4.00) (n = 8) | 0.774 |
| HG/Q ratio | 1.27 ± 0.35 (0.79–2.00) (n = 18) | 1.17 ± 0.51 (0.58–2.26) (n = 8) | 0.565 |
| * TUG (s) | 10.4 ± 1.95 (7.3–14.9) (n = 21) | 12.6 ± 3.21 (8.9–18.1) (n = 10) | * 0.027 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stockdale, A.; Webb, N.; Wootton, J.; Drennan, J.; Brown, S.; Stokes, M. Muscle Strength and Functional Ability in Recreational Female Golfers and Less Active Non-Golfers over the Age of 80 Years. Geriatrics 2017, 2, 12. https://doi.org/10.3390/geriatrics2010012
Stockdale A, Webb N, Wootton J, Drennan J, Brown S, Stokes M. Muscle Strength and Functional Ability in Recreational Female Golfers and Less Active Non-Golfers over the Age of 80 Years. Geriatrics. 2017; 2(1):12. https://doi.org/10.3390/geriatrics2010012
Chicago/Turabian StyleStockdale, Alison, Nicholas Webb, Jessica Wootton, Jonathan Drennan, Simon Brown, and Maria Stokes. 2017. "Muscle Strength and Functional Ability in Recreational Female Golfers and Less Active Non-Golfers over the Age of 80 Years" Geriatrics 2, no. 1: 12. https://doi.org/10.3390/geriatrics2010012
APA StyleStockdale, A., Webb, N., Wootton, J., Drennan, J., Brown, S., & Stokes, M. (2017). Muscle Strength and Functional Ability in Recreational Female Golfers and Less Active Non-Golfers over the Age of 80 Years. Geriatrics, 2(1), 12. https://doi.org/10.3390/geriatrics2010012