
Therapeutic Effects of Mutian® Xraphconn on 141 Client-Owned Cats with Feline Infectious Peritonitis Predicted by Total Bilirubin Levels

Abstract
:1. Introduction
2. Materials and Methods
2.1. Therapeutic Agent and Administration
2.2. Animals and Diagnosis
2.3. Statistical Analysis
3. Results
3.1. Comparison of Parameters between Cats with and without FIP
3.2. Comparison of Parameters between Surviving and Non-Surviving Cats with FIP
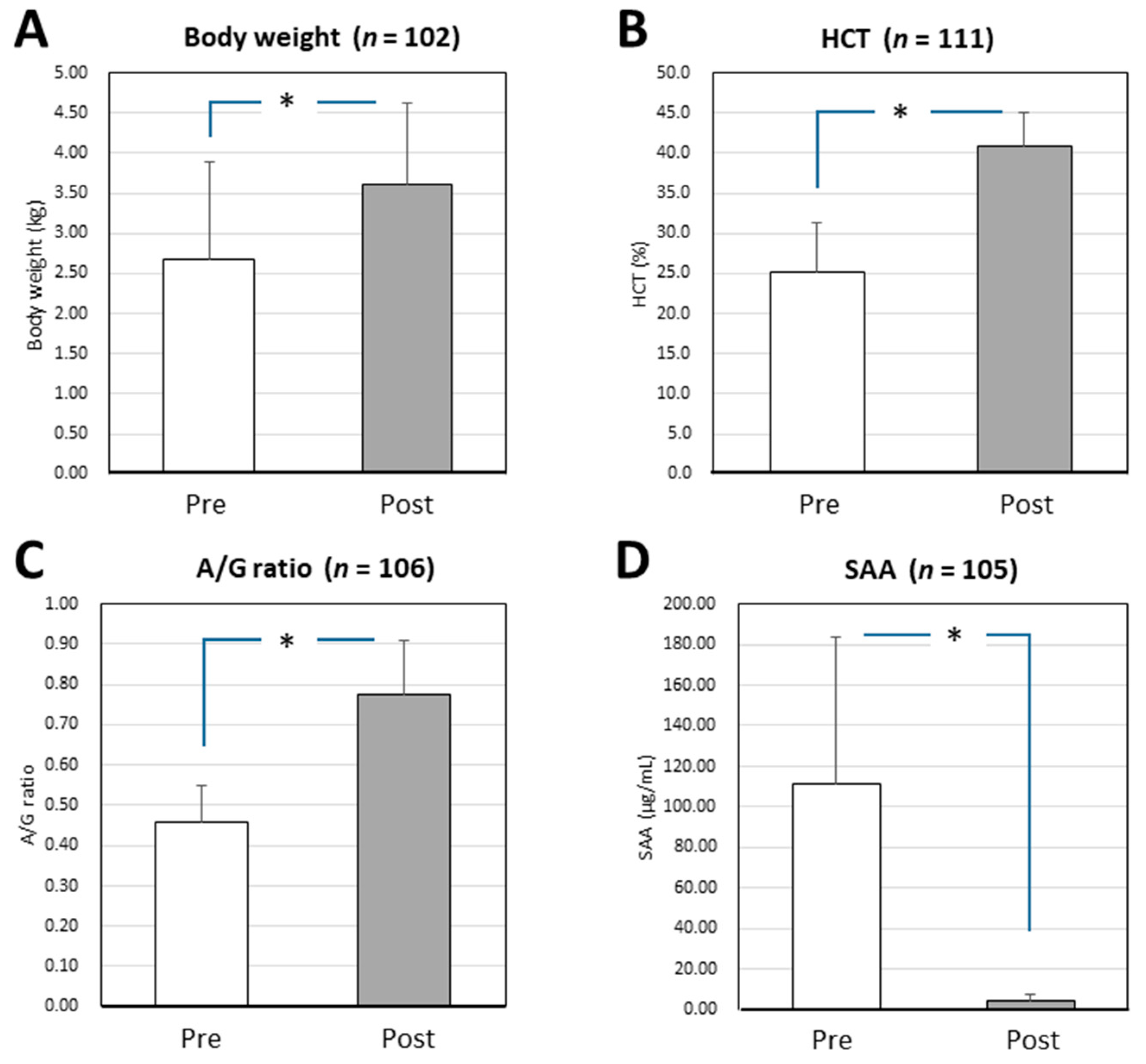
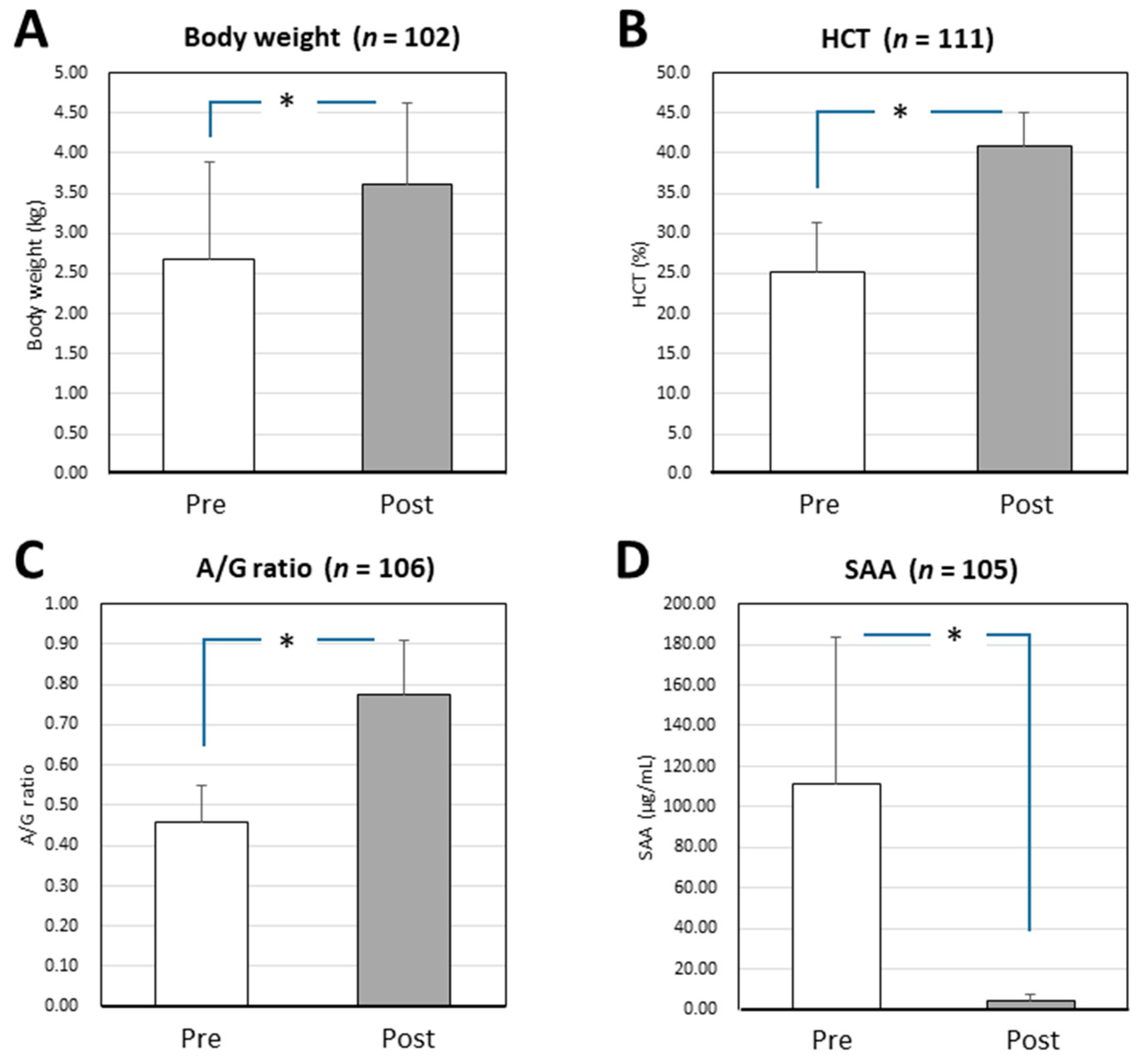
3.3. Changes in the Parameters of Surviving Cats with Effusive FIP before and after Mutian X Treatment
3.4. Circulating T-Bilirubin Levels and Survival Rates of Cats with Effusive FIP
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pedersen, N.C. A review of feline infectious peritonitis virus infection: 1963–2008. J. Feline Med. Sur. 2009, 11, 225–258. [Google Scholar] [CrossRef]
- Tekes, G.; Thiel, H.-J. Feline coronaviruses: Pathogenesis of feline infectious peritonitis. Adv. Virus Res. 2016, 96, 193–218. [Google Scholar]
- Felten, S.; Hartmann, K. Diagnosis of feline infectious peritonitis: A review of the current literature. Viruses 2019, 11, 1068. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, N.C. An update on feline infectious peritonitis: Diagnostics and therapeutics. Vet. J. 2014, 201, 133–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Addie, D.; Belák, S.; Boucraut-Baralon, C.; Egberink, H.; Frymus, T.; Gruffydd-Jones, T.; Hartmann, K.; Hosie, M.J.; Lloret, A.; Lutz, H.; et al. Feline infectious peritonitis. ABCD guidelines on prevention and management. J. Feline Med. Surg. 2009, 11, 594–604. [Google Scholar] [CrossRef]
- Hartmann, K.; Ritz, S. Treatment of cats with feline infectious peritonitis. Vet. Immunol. Immunopathol. 2008, 123, 172–175. [Google Scholar] [CrossRef] [PubMed]
- Ritz, S.; Egberink, H.; Hartmann, K. Effect of feline interferon-omega on the survival time and quality of life of cats with feline infectious peritonitis. J. Vet. Intern. Med. 2007, 21, 1193–1197. [Google Scholar] [CrossRef] [PubMed]
- Fischer, Y.; Ritz, S.; Weber, K.; Sauter-Louis, C.; Hartmann, K. Randomized, placebo controlled study of the effect of propentofylline on survival time and quality of life of cats with feline infectious peritonitis. J. Vet. Intern. Med. 2011, 25, 1270–1276. [Google Scholar] [CrossRef]
- Legendre, A.M.; Kuritz, T.; Galyon, G.; Baylor, V.M.; Heidel, R.E. Polyprenyl immunostimulant treatment of cats with presumptive non-effusive feline infectious peritonitis in a field study. Front. Vet. Sci. 2017, 4, 7. [Google Scholar] [CrossRef] [Green Version]
- Takano, T.; Akiyama, M.; Doki, T.; Hohdatsu, T. Antiviral activity of itraconazole against type I feline coronavirus infection. Vet. Res. 2019, 50, 5. [Google Scholar] [CrossRef] [Green Version]
- Takano, T.; Katoh, Y.; Doki, T.; Hohdatsu, T. Effect of chloroquine on feline infectious peritonitis virus infection in vitro and in vivo. Antivir. Res. 2013, 99, 100–107. [Google Scholar] [CrossRef]
- Tanaka, Y.; Sato, Y.; Sasaki, T. Suppression of coronavirus replication by cyclophilin inhibitors. Viruses 2013, 5, 1250–1260. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, Y.; Sato, Y.; Sasaki, T. Feline coronavirus replication is affected by both cyclophilin A and cyclophilin B. J. Gen. Virol. 2017, 98, 190–200. [Google Scholar] [CrossRef]
- Murphy, B.G.; Perron, M.; Murakami, E.; Bauer, K.; Park, Y.; Eckstrand, C.; Liepnieks, M.; Pedersen, N.C. The nucleoside analog GS-441524 strongly inhibits feline infectious peritonitis (FIP) virus in tissue culture and experimental cat infection studies. Vet. Microbiol. 2018, 219, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Amirian, E.S.; Levy, J.K. Current knowledge about the antivirals remdesivir (GS-5734) and GS-441524 as therapeutic options for coronaviruses. One Health 2020, 9, 100128. [Google Scholar] [CrossRef]
- Pedersen, N.C.; Perron, M.; Bannasch, M.; Montgomery, E.; Murakami, E.; Liepnieks, M.; Liu, H. Efficacy and safety of the nucleoside analog GS-441524 for treatment of cats with naturally occurring feline infectious peritonitis. J. Feline Med. Surg. 2019, 21, 271–281. [Google Scholar] [CrossRef] [Green Version]
- Dickinson, P.J.; Bannasch, M.; Thomasy, S.M.; Murthy, V.D.; Vernau, K.M.; Liepnieks, M.; Montgomery, E.; Knickelbein, K.E.; Murphy, B.; Pedersen, N.C. Antiviral treatment using the adenosine nucleoside analogue GS-441524 in cats with clinically diagnosed neurological feline infectious peritonitis. J. Vet. Intern. Med. 2020, 34, 1587–1593. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, N.C.; Kim, Y.; Liu, H.; Galasiti Kankanamalage, A.C.; Eckstrand, C.; Groutas, W.C.; Bannasch, M.; Meadows, J.M.; Chang, K.O. Efficacy of a 3C-like protease inhibitor in treating various forms of acquired feline infectious peritonitis. J. Feline Med. Surg. 2018, 20, 378–392. [Google Scholar] [CrossRef] [PubMed]
- Facebook Page of Mutian Life Sciences Co., Ltd. Available online: https://m.facebook.com/Mutian-Life-Sciences-Co-Ltd-801346880247796/ (accessed on 13 December 2021).
- Tanaka, Y.; Sasaki, T.; Matsuda, R.; Uematsu, Y.; Yamaguchi, T. Molecular epidemiological study of feline coronavirus strains in Japan using RT-PCR targeting nsp14 gene. BMC Vet. Res. 2015, 11, 57. [Google Scholar] [CrossRef] [Green Version]
- FUJIFILM VET Systems Co., Ltd. Laboratory Analysis Service for Veterinarian. Available online: https://www.fujifilm.com/jp/ja/healthcare/veterinary/examination (accessed on 21 September 2021).
- Addie, D.D.; Covell-Ritchie, J.; Jarrett, O.; Fosbery, M. Rapid resolution of non-effusive feline infectious peritonitis uveitis with an oral adenosine nucleoside analogue and feline interferon omega. Viruses 2020, 12, 1216. [Google Scholar] [CrossRef]
- Krentz, D.; Zenger, K.; Alberer, M.; Felten, S.; Bergmann, M.; Dorsch, R.; Matiasek, K.; Kolberg, L.; Hofmann-Lehmann, R.; Meli, M.L.; et al. Curing cats with feline infectious peritonitis with an oral multi-component drug containing GS-441524. Viruses 2021, 13, 2228. [Google Scholar] [CrossRef] [PubMed]
- Riemer, F.; Kuehner, K.A.; Ritz, S.; Sauter-Louis, C.; Hartmann, K. Clinical and laboratory features of cats with feline infectious peritonitis—A retrospective study of 231 confirmed cases (2000–2010). J. Feline Med. Surg. 2016, 18, 348–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saverio, P.; Alessia, G.; Vito, T.; Stefano, G. Critical assessment of the diagnostic value of feline α1-acid glycoprotein for feline infectious peritonitis using the likelihood ratios approach. J. Vet. Diagn. Invest. 2007, 19, 266–272. [Google Scholar] [CrossRef] [Green Version]
- Jeffery, U.; Deitz, K.; Hostetter, S. Positive predictive value of albumin:globulin ratio for feline infectious peritonitis in a mid-western referral hospital population. J. Feline Med. Surg. 2012, 14, 903–905. [Google Scholar] [CrossRef]
- Hazuchova, K.; Held, S.; Neiger, R. Usefulness of acute phase proteins in differentiating between feline infectious peritonitis and other diseases in cats with body cavity effusions. J. Feline Med. Surg. 2017, 19, 809–816. [Google Scholar] [CrossRef] [PubMed]
- Yuki, M.; Aoyama, R.; Nakagawa, M.; Hirano, T.; Naitoh, E.; Kainuma, D. A clinical investigation on serum amyloid A concentration in client-owned healthy and diseased cats in a primary care animal hospital. Vet. Sci. 2020, 7, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, H.Y.; Chueh, L.L.; Lin, C.N.; Su, B.L. Clinicopathological findings and disease staging of feline infectious peritonitis: 51 cases from 2003 to 2009 in Taiwan. J. Feline Med. Surg. 2011, 13, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Addie, D.D.; Curran, S.; Bellini, F.; Crowe, B.; Sheehan, E.; Ukrainchuk, L.; Decaro, N. Oral Mutian® X stopped faecal feline coronavirus shedding by naturally infected cats. Res. Vet. Sci. 2020, 130, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Baker, E.N.; Stranieri, A.; Helps, C.R.; Porter, E.L.; Davidson, A.D.; Day, M.J.; Knowles, T.; Kipar, A.; Tasker, S. Limitations of using feline coronavirus spike protein gene mutations to diagnose feline infectious peritonitis. Vet. Res. 2017, 48, 60. [Google Scholar] [CrossRef] [Green Version]
- Shmueli, E.; Or, R.; Shapira, M.Y.; Resnick, I.B.; Caplan, O.; Bdolah-Abram, T.; Wolf, D.G. High rate of cytomegalovirus drug resistance among patients receiving preemptive antiviral treatment after haploidentical stem cell transplantation. J. Infect. Dis. 2014, 209, 557–561. [Google Scholar] [CrossRef] [Green Version]
- Tamura, D.; DeBiasi, R.L.; Okomo-Adhiambo, M.; Mishin, V.P.; Campbell, A.P.; Loechelt, B.; Wiedermann, B.L.; Fry, A.M.; Gubareva, L.V. Emergence of multidrug-resistant influenza A (H1N1) pdm09 virus variants in an immunocompromised child treated with oseltamivir and zanamivir. J. Infect. Dis. 2015, 212, 1209–1213. [Google Scholar] [CrossRef] [PubMed]
- Nelson, J.A.E.; Fokar, A.; Hudgens, M.G.; Compliment, K.J.; Hawkins, J.T.; Tegha, G.; Kamwendo, D.D.; Kayira, D.; Mofolo, I.A.; Kourtis, A.P.; et al. Frequent nevirapine resistance in infants infected by HIV-1 via breastfeeding while on nevirapine prophylaxis. AIDS 2015, 29, 2131–2138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, S.; Novicoff, W.; Nadeau, J.; Evans, S. Unlicensed GS-441524-like antiviral therapy can be effective for at-home treatment of feline infectious peritonitis. Animals 2021, 11, 2257. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Parameters | Cats with Effusive FIP | Cats without FIP | p-Value * | ||||
|---|---|---|---|---|---|---|---|
| n | Mean | SE | n | Mean | SE | ||
| Age (months) | 141 | 15.72 | 1.92 | 28 | 19.36 | 3.81 | NS |
| Appetite score | 141 | 3.94 | 0.28 | 28 | 6.29 | 0.69 | <0.003 |
| Activity score | 141 | 4.55 | 0.21 | 28 | 6.61 | 0.68 | <0.002 |
| Body temperature (°C) | 105 | 38.80 | 0.09 | 23 | 38.48 | 0.19 | NS |
| Body weight (kg) | 141 | 2.68 | 0.10 | 28 | 2.68 | 0.19 | NS |
| HCT (%) | 138 | 25.18 | 0.54 | 27 | 34.45 | 1.50 | <0.0001 |
| A/G ratio | 132 | 0.46 | 0.01 | 26 | 0.70 | 0.04 | <0.0001 |
| T-bilirubin (mg/dL) | 101 | 1.46 | 0.17 | 13 | 0.45 | 0.16 | <0.002 |
| SAA (μg/mL) | 130 | 109.96 | 6.36 | 27 | 33.46 | 11.44 | <0.0001 |
| Parameters | Cats with Effusive FIP | Cats without FIP | p-Value * | ||||
|---|---|---|---|---|---|---|---|
| n | Positive | Negative | n | Positive | Negative | ||
| Diarrhea | 141 | 22 | 119 | 28 | 7 | 21 | NS |
| Vomiting | 140 | 10 | 130 | 28 | 5 | 23 | NS |
| PCR testing (blood) | 125 | 114 | 11 | 26 | 0 | 26 | <0.0001 |
| PCR testing (ascites or pleural) ** | 141 | 139 | 2 | 2 | 0 | 2 | <0.0001 |
| α1AG *** | 126 | 125 | 1 | 25 | 15 | 10 | <0.0001 |
| Parameters | Survived | Non-Survived | p-Value * | ||||
|---|---|---|---|---|---|---|---|
| n | Mean | SE | n | Mean | SE | ||
| Age (months) | 116 | 15.18 | 2.10 | 25 | 17.80 | 4.76 | NS |
| Appetite score | 116 | 4.42 | 3.22 | 25 | 1.72 | 2.51 | <0.0001 |
| Activity score | 116 | 4.94 | 2.39 | 25 | 2.72 | 2.48 | <0.0001 |
| Body temperature (℃) | 86 | 38.99 | 0.79 | 19 | 37.94 | 1.21 | <0.0005 |
| Body weight (kg) | 116 | 2.70 | 1.21 | 25 | 2.57 | 1.02 | NS |
| HCT (%) | 113 | 25.11 | 6.30 | 25 | 25.51 | 6.33 | NS |
| A/G ratio | 108 | 0.46 | 0.09 | 24 | 0.45 | 0.09 | NS |
| T-bilirubin (mg/dL) | 77 | 0.94 | 0.95 | 24 | 3.11 | 2.35 | <0.0001 |
| SAA (μg/mL) | 107 | 112.19 | 72.67 | 23 | 99.79 | 72.76 | NS |
| Parameters | Survived | Non-Survived | p-Value * | ||||
|---|---|---|---|---|---|---|---|
| n | Positive | Negative | n | Positive | Negative | ||
| Diarrhea | 116 | 17 | 99 | 25 | 5 | 20 | NS |
| Vomiting | 115 | 4 | 111 | 25 | 6 | 19 | <0.003 |
| PCR testing (blood) | 103 | 92 | 11 | 22 | 22 | 0 | NS |
| PCR testing (ascites or pleural) ** | 116 | 114 | 2 | 25 | 25 | 0 | NS |
| α1AG *** | 104 | 103 | 1 | 22 | 22 | 0 | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katayama, M.; Uemura, Y. Therapeutic Effects of Mutian® Xraphconn on 141 Client-Owned Cats with Feline Infectious Peritonitis Predicted by Total Bilirubin Levels. Vet. Sci. 2021, 8, 328. https://doi.org/10.3390/vetsci8120328
Katayama M, Uemura Y. Therapeutic Effects of Mutian® Xraphconn on 141 Client-Owned Cats with Feline Infectious Peritonitis Predicted by Total Bilirubin Levels. Veterinary Sciences. 2021; 8(12):328. https://doi.org/10.3390/vetsci8120328
Chicago/Turabian StyleKatayama, Masato, and Yukina Uemura. 2021. "Therapeutic Effects of Mutian® Xraphconn on 141 Client-Owned Cats with Feline Infectious Peritonitis Predicted by Total Bilirubin Levels" Veterinary Sciences 8, no. 12: 328. https://doi.org/10.3390/vetsci8120328
APA StyleKatayama, M., & Uemura, Y. (2021). Therapeutic Effects of Mutian® Xraphconn on 141 Client-Owned Cats with Feline Infectious Peritonitis Predicted by Total Bilirubin Levels. Veterinary Sciences, 8(12), 328. https://doi.org/10.3390/vetsci8120328