

The Assessment of Quality of the Root Canal Filling and the Number of Visits Needed for Completing Primary Root Canal Treatment by Operators with Different Experience

 ,
,  ,
,  ,
,  ,
,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Root Canal Treatment Protocol
2.3. Assessment of the Root Canal Filling
2.4. Statistical Analysis
3. Results
3.1. Quality of Root Canal Filling
3.1.1. Length
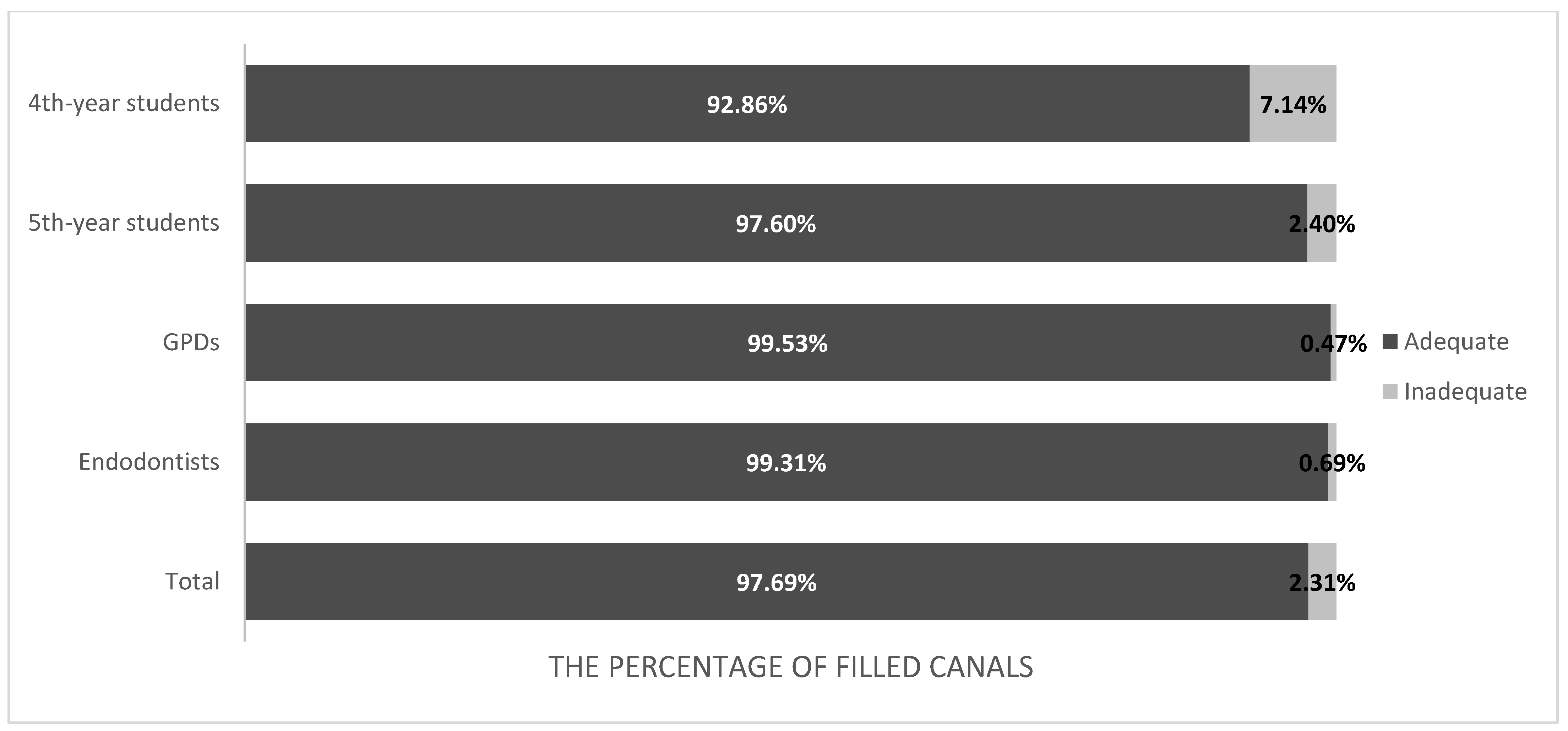
3.1.2. Homogeneity
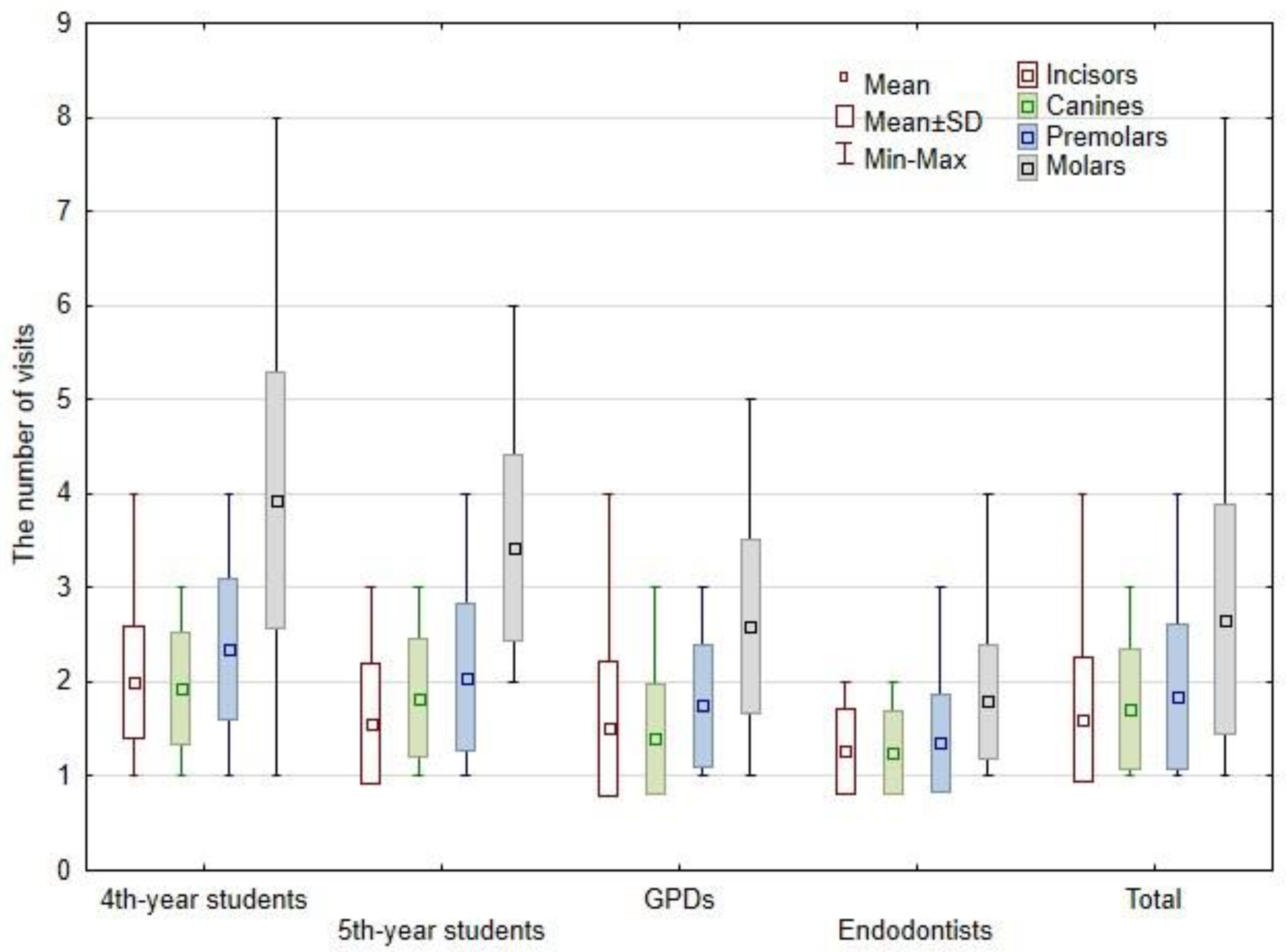
3.2. Number of Visits
3.3. Type of Instruments
3.4. Distribution of Teeth and Diagnoses
4. Discussion
4.1. Quality of Root Canal Filling
4.2. Number of Visits
4.3. Type of Instruments
4.4. Distribution of Teeth
4.5. Distribution of Diagnoses
5. Conclusions
- The larger number of visits and the lower quality of treatment was observed for 4th-year students than for other groups; in contrast, endodontists needed the lowest number of visits to complete RCT and more often overfilled teeth than the other operator groups.
- Interestingly, no difference in quality (homogeneity and length) of root canal filling between 5th-year students, GPDs, and endodontics was noted.
- Endodontists and GDPs more often performed RCT of teeth with more complicated anatomy (premolars and molars).
- The overfilling was observed most frequently in the palatal canal of first maxillary molars and in the case of periapical tissue inflammation, while short-filling was observed most frequently in the mesio-buccal canal of first mandibular molars.
- The treatment of lower teeth demanded more visits than that of upper teeth.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siqueira, J.F., Jr.; Rôças, I.N. Clinical Implications and Microbiology of Bacterial Persistence after Treatment Procedures. J. Endod. 2008, 34, 1291–1301.e3. [Google Scholar] [CrossRef]
- Schilder, H. Cleaning and Shaping the Root Canal. Dent. Clin. N. Am. 1974, 18, 269–296. [Google Scholar] [CrossRef]
- Kharouf, N.; Arntz, Y.; Eid, A.; Zghal, J.; Sauro, S.; Haikel, Y.; Mancino, D. Physicochemical and Antibacterial Properties of Novel, Premixed Calcium Silicate-Based Sealer Compared to Powder–Liquid Bioceramic Sealer. J. Clin. Med. 2020, 9, 3096. [Google Scholar] [CrossRef] [PubMed]
- Fernández, R.; Cadavid, D.; Zapata, S.M.; Alvarez, L.G.; Restrepo, F.A. Impact of Three Radiographic Methods in the Outcome of Nonsurgical Endodontic Treatment: A Five-Year Follow-Up. J. Endod. 2013, 39, 1097–1103. [Google Scholar] [CrossRef] [PubMed]
- Ng, Y.-L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of Primary Root Canal Treatment: Systematic Review of the Literature—Part 1. Effects of Study Characteristics on Probability of Success. Int. Endod. J. 2007, 40, 921–939. [Google Scholar] [CrossRef] [PubMed]
- Ng, Y.-L.; Mann, V.; Gulabivala, K. Outcome of Secondary Root Canal Treatment: A Systematic Review of the Literature. Int. Endod. J. 2008, 41, 1026–1046. [Google Scholar] [CrossRef]
- Ng, Y.-L.; Mann, V.; Gulabivala, K. A Prospective Study of the Factors Affecting Outcomes of Nonsurgical Root Canal Treatment: Part 1: Periapical Health. Int. Endod. J. 2011, 44, 583–609. [Google Scholar] [CrossRef]
- Olcay, K.; Eyüboglu, T.F.; Özcan, M. Clinical Outcomes of Non-Surgical Multiple-Visit Root Canal Retreatment: A Retrospective Cohort Study. Odontology 2019, 107, 536–545. [Google Scholar] [CrossRef]
- European Society of Endodontology. Quality Guidelines for Endodontic Treatment: Consensus Report of the European Society of Endodontology. Int. Endod. J. 2006, 39, 921–930. [Google Scholar] [CrossRef]
- De Moor, R.; Hülsmann, M.; Kirkevang, L.L.; Tanalp, J.; Whitworth, J. Undergraduate Curriculum Guidelines for Endodontology. Int. Endod. J. 2013, 46, 1105–1114. [Google Scholar] [CrossRef]
- Sacha, S.R.; Sonntag, D.; Burmeister, U.; Rüttermann, S.; Gerhardt-Szép, S. A Multicentric Survey to Evaluate Preclinical Education in Endodontology in German-speaking Countries. Int. Endod. J. 2021, 54, 1957–1964. [Google Scholar] [CrossRef] [PubMed]
- Segura-Egea, J.J.; Zarza-Rebollo, A.; Jiménez-Sánchez, M.C.; Cabanillas-Balsera, D.; Areal-Quecuty, V.; Martín-González, J. Evaluation of Undergraduate Endodontic Teaching in Dental Schools within Spain. Int. Endod. J. 2021, 54, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Al Raisi, H.; Dummer, P.M.H.; Vianna, M.E. How Is Endodontics Taught? A Survey to Evaluate Undergraduate Endodontic Teaching in Dental Schools within the United Kingdom. Int. Endod. J. 2019, 52, 1077–1085. [Google Scholar] [CrossRef] [PubMed]
- European Society of Endodontology. Accreditation of Postgraduate Speciality Training Programmes in Endodontology. Minimum Criteria for Training Specialists in Endodontology within Europe. Int. Endod. J. 2010, 43, 725–737. [Google Scholar] [CrossRef] [PubMed]
- Balto, H.; Al Khalifah, S.; Al Mugairin, S.; Al Deeb, M.; Al-Madi, E. Technical Quality of Root Fillings Performed by Undergraduate Students in Saudi Arabia. Int. Endod. J. 2010, 43, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Llena, C.; Nicolescu, T.; Perez, S.; de Pereda, S.; Gonzalez, A.; Alarcon, I.; Monzo, A.; Sanz, J.L.; Melo, M.; Forner, L. Outcome of Root Canal Treatments Provided by Endodontic Postgraduate Students. A Retrospective Study. J. Clin. Med. 2020, 9, 1994. [Google Scholar] [CrossRef]
- Awooda, E.M.; Siddig, R.I.; Alturki, R.S.; Sanhouri, N.M. Radiographic Technical Quality of Root Canal Treatment Performed by Undergraduate. J. Int. Soc. Prev. Community Dent. 2016, 6, 554–558. [Google Scholar] [CrossRef]
- Hayes, S.J.; Gibson, M.; Hammond, M.; Bryant, S.T.; Dummer, P.M. An Audit of Root Canal Treatment Performed by Undergraduate Students. Int. Endod. J. 2001, 34, 501–505. [Google Scholar] [CrossRef]
- AlRahabi, M.K. Evaluation of Complications of Root Canal Treatment Performed by Undergraduate Dental Students. Libyan J. Med. 2017, 12, 1345582. [Google Scholar] [CrossRef]
- Al-Manei, K.K. Radiographic Quality of Single vs. Multiple-Visit Root Canal Treatment Performed by Dental Students: A Case Control Study. Iran. Endod. J. 2018, 13, 149–154. [Google Scholar] [CrossRef]
- Habib, A.A.; Doumani, M.D.; Nassani, M.Z.; Shamsy, E.; Jto, B.S.; Arwadİ, H.A.; Mohamed, S.A. Radiographic Assessment of the Quality of Root Canal Fillings Performed by Senior Dental Students. Eur. Endod. J. 2018, 3, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, A.; Coffey, D.; Duncan, H.F. A Re-Audit of the Technical Quality of Undergraduate Root Canal Treatment after the Introduction of New Technology and Teaching Practices. Int. Endod. J. 2017, 50, 941–950. [Google Scholar] [CrossRef] [PubMed]
- Unal, G.C.; Kececi, A.D.; Kaya, B.U.; Tac, A.G. Quality of Root Canal Fillings Performed by Undergraduate Dental Students. Eur. J. Dent. 2011, 5, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Vukadinov, T.; Blažić, L.; Kantardžić, I.; Lainović, T. Technical Quality of Root Fillings Performed by Undergraduate Students: A Radiographic Study. Sci. World J. 2014, 2014, 751274. [Google Scholar] [CrossRef]
- Ramey, K.; Yaccino, J.; Wealleans, J. A Retrospective, Radiographic Outcomes Assessment of 1960 Initial Posterior Root Canal Treatments Performed by Endodontists and Dentists. J. Endod. 2017, 43, 1250–1254. [Google Scholar] [CrossRef]
- Ricucci, D.; Russo, J.; Rutberg, M.; Burleson, J.A.; Spångberg, L.S. A Prospective Cohort Study of Endodontic Treatments of 1369 Root Canals: Results after 5 Years. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 112, 825–842. [Google Scholar] [CrossRef]
- Yusufoglu, S.İ.; Sarıçam, E. Comparison of Endodontic Treatment Qualities of Molar Teeth Performed by Endodontists and Practitioners: A Radiographic Analysis. Selcuk Dent. J. 2021, 8, 127–132. [Google Scholar] [CrossRef]
- Berrezouga, L.; Bouguezzi, A.; Belkhir, M.S. Outcome of Initial Endodontic Treatment Performed, by One Specialist, in 122 Tunisian Patients: A Retrospective Study. Int. J. Dent. 2018, 2018, 3504245. [Google Scholar] [CrossRef]
- Imura, N.; Pinheiro, E.T.; Gomes, B.P.; Zaia, A.A.; Ferraz, C.C.; Souza-Filho, F.J. The Outcome of Endodontic Treatment: A Retrospective Study of 2000 Cases Performed by a Specialist. J. Endod. 2007, 33, 1278–1282. [Google Scholar] [CrossRef]
- Bierenkrant, D.E.; Parashos, P.; Messer, H.H. The Technical Quality of Nonsurgical Root Canal Treatment Performed by a Selected Cohort of Australian Endodontists. Int. Endod. J. 2008, 41, 561–570. [Google Scholar] [CrossRef]
- Burry, J.C.; Stover, S.; Eichmiller, F.; Bhagavatula, P. Outcomes of Primary Endodontic Therapy Provided by Endodontic Specialists Compared with Other Providers. J. Endod. 2016, 42, 702–705. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.W.-Y.; Zhang, S.; Zhang, C.-F.; Chu, C.-H. Perceptions of Single-Visit and Multiple-Visit Endodontic Treatment: A Survey of Endodontic Specialists and General Dentists in Hong Kong. J. Investig. Clin. Dent. 2016, 7, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Baharin, S.A.; Omar, S.H. Undergraduate Endodontic Clinical Training in Malaysia: A National Survey. Eur. J. Dent. Educ. 2021, 25, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Moussa-Badran, S.; Roy, B.; du Parc, A.S.; Bruyant, M.; Lefevre, B.; Maurin, J.C. Technical Quality of Root Fillings Performed by Dental Students at the Dental Teaching Centre in Reims, France. Int. Endod. J. 2008, 41, 679–684. [Google Scholar] [CrossRef]
- Kharouf, N.; Hemmerlé, J.; Haikel, Y.; Mancino, D. Technical Quality of Root Canal Filling in Preclinical Training at Strasbourg University Using Two Teaching Protocols. Eur. J. Dent. 2019, 13, 521–526. [Google Scholar] [CrossRef][Green Version]
- Ertas, E.T.; Ertas, H.; Sisman, Y.; Sagsen, B.; Er, O. Radiographic Assessment of the Technical Quality and Periapical Health of Root-Filled Teeth Performed by General Practitioners in a Turkish Subpopulation. Sci. World J. 2013, 2013, 514841. [Google Scholar] [CrossRef]
- İlgüy, D.; İlgüy, M.; Fişekçioğlu, E.; Ersan, N.; Tanalp, J.; Dölekoğlu, S. Assessment of Root Canal Treatment Outcomes Performed by Turkish Dental Students: Results After Two Years. J. Dent. Educ. 2013, 77, 502–509. [Google Scholar] [CrossRef]
- Fong, W.; Heidarifar, O.; Killough, S.; Lappin, M.J.; El Karim, I.A. An Audit on Technical Quality of Root Fillings Performed by Undergraduate Students. Int. Endod. J. 2018, 51 (Suppl. S3), e197–e203. [Google Scholar] [CrossRef]
- Ribeiro, D.M.; Henckel, M.D.; Mello, F.W.; Felippe, M.C.S.; Felippe, W.T. Radiographic Analysis the Obturation’s Quality in Root Canal Treatment Performed by a South Brazilian Sample of Undergraduate Students. Rev. Gaúcha Odontol. 2019, 67, e20190040. [Google Scholar] [CrossRef]
- Ribeiro, D.M.; Réus, J.C.; Felippe, W.T.; Pacheco-Pereira, C.; Dutra, K.L.; Santos, J.N.; Porporatti, A.L.; De Luca Canto, G. Technical Quality of Root Canal Treatment Performed by Undergraduate Students Using Hand Instrumentation: A Meta-Analysis. Int. Endod. J. 2018, 51, 269–283. [Google Scholar] [CrossRef]
- Rafeek, R.N.; Smith, W.A.; Mankee, M.S.; Coldero, L.G. Radiographic Evaluation of the Technical Quality of Root Canal Fillings Performed by Dental Students. Aust. Endod. J. 2012, 38, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Pratten, D.H.; McDonald, N.J. Comparison of Radiographic and Electronic Working Lengths. J. Endod. 1996, 22, 173–176. [Google Scholar] [CrossRef]
- Mahmoud, O.; Abdelmagied, M.H.A.; Dandashi, A.H.; Jasim, B.N.; Kayali, H.A.T.; Al Shehadat, S. Comparative Evaluation of Accuracy of Different Apex Locators: Propex IQ, Raypex 6, Root ZX, and Apex ID with CBCT and Periapical Radiograph—In Vitro Study. Int. J. Dent. 2021, 2021, 5563426. [Google Scholar] [CrossRef]
- Adriano, L.Z.; Barasuol, J.C.; Cardoso, M.; Bolan, M. In Vitro Comparison between Apex Locators, Direct and Radiographic Techniques for Determining the Root Canal Length in Primary Teeth. Eur. Arch. Paediatr. Dent. 2019, 20, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Adorno, C.G.; Solaeche, S.M.; Ferreira, I.E.; Pedrozo, A.; Escobar, P.M.; Fretes, V.R. The Influence of Periapical Lesions on the Repeatability of Two Electronic Apex Locators in Vivo. Clin. Oral Investig. 2021, 25, 5239–5245. [Google Scholar] [CrossRef]
- Tsesis, I.; Blazer, T.; Ben-Izhack, G.; Taschieri, S.; Del Fabbro, M.; Corbella, S.; Rosen, E. The Precision of Electronic Apex Locators in Working Length Determination: A Systematic Review and Meta-Analysis of the Literature. J. Endod. 2015, 41, 1818–1823. [Google Scholar] [CrossRef] [PubMed]
- Bajawi, A.; AL-Sagoor, S.; Alhadi, A.; Alhadi, M.; Almasrahi, M.; AL-Ghazali, N.; Al Moaleem, M. Radiographic Assessment of the Quality of Root Canal Treatments Performed by Practitioners with Different Levels of Experience. Biomed. Pharmacol. J. 2018, 11, 1609–1616. [Google Scholar] [CrossRef]
- Malagnino, V.A.; Pappalardo, A.; Plotino, G.; Carlesi, T. The Fate of Overfilling in Root Canal Treatments with Long-Term Follow-up: A Case Series. Restor. Dent. Endod. 2021, 46, e27. [Google Scholar] [CrossRef]
- Ghanaati, S.; Willershausen, I.; Barbeck, M.; Unger, R.; Joergens, M.; Sader, R.; Kirkpatrick, C.; Willershausen, B. Tissue Reaction to Sealing Materials: Different View at Biocompatibility. Eur. J. Med. Res. 2010, 15, 483. [Google Scholar] [CrossRef]
- Szczurko, G.; Pawińska, M.; Łuczaj-Cepowicz, E.; Kierklo, A.; Marczuk-Kolada, G.; Hołownia, A. Effect of Root Canal Sealers on Human Periodontal Ligament Fibroblast Viability: Ex Vivo Study. Odontology 2018, 106, 245–256. [Google Scholar] [CrossRef]
- Goldberg, F.; Cantarini, C.; Alfie, D.; Macchi, R.L.; Arias, A. Relationship between Unintentional Canal Overfilling and the Long-term Outcome of Primary Root Canal Treatments and Nonsurgical Retreatments: A Retrospective Radiographic Assessment. Int. Endod. J. 2020, 53, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez, J.H.; Brizuela, C.; Villota, E. Human Teeth with Periapical Pathosis after Overinstrumentation and Overfilling of the Root Canals: A Scanning Electron Microscopic Study. Int. Endod. J. 1999, 32, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Aminoshariae, A.; Kulild, J.C. The Impact of Sealer Extrusion on Endodontic Outcome: A Systematic Review with Meta-analysis. Aust. Endod. J. 2020, 46, 123–129. [Google Scholar] [CrossRef]
- Chugal, N.M.; Clive, J.M.; Spångberg, L.S. Endodontic Infection: Some Biologic and Treatment Factors Associated with Outcome. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2003, 96, 81–90. [Google Scholar] [CrossRef]
- ElMubarak, A.H.H.; Abu-bakr, N.H.; Ibrahim, Y.E. Postoperative Pain in Multiple-Visit and Single-Visit Root Canal Treatment. J. Endod. 2010, 36, 36–39. [Google Scholar] [CrossRef] [PubMed]
- Madarati, A.A. Preferences of Dentists and Endodontists, in Saudi Arabia, on Management of Necrotic Pulp with Acute Apical Abscess. BMC Oral Health 2018, 18, 110. [Google Scholar] [CrossRef]
- Vera, J.; Siqueira, J.F., Jr.; Ricucci, D.; Loghin, S.; Fernández, N.; Flores, B.; Cruz, A.G. One- versus Two-Visit Endodontic Treatment of Teeth with Apical Periodontitis: A Histobacteriologic Study. J. Endod. 2012, 38, 1040–1052. [Google Scholar] [CrossRef]
- Schwendicke, F.; Göstemeyer, G. Single-Visit or Multiple-Visit Root Canal Treatment: Systematic Review, Meta-Analysis and Trial Sequential Analysis. BMJ Open 2017, 7, e013115. [Google Scholar] [CrossRef]
- Tirupathi, S.P.; Krishna, N.; Rajasekhar, S.; Nuvvula, S. Clinical Efficacy of Single-Visit Pulpectomy over Multiple-Visit Pulpectomy in Primary Teeth: A Systematic Review. Int. J. Clin. Pediatr. Dent. 2019, 12, 453–459. [Google Scholar] [CrossRef]
- Pietrzycka, K.; Pawlicka, H. Effectiveness of One-Visit Treatment of Teeth with Infected Root Canals with and without Ozonotherapy. J. Stomatol. 2011, 64, 37–49. [Google Scholar]
- Pietrzycka, K.; Pawlicka, H. Effectiveness of One-Visit and Two-Visit Treatment of Teeth with Infected Root Canals. J. Stomatol. 2013, 66, 351–365. [Google Scholar] [CrossRef]
- Moreira, M.S.; Anuar, A.S.N.-S.; Tedesco, T.K.; dos Santos, M.; Morimoto, S. Endodontic Treatment in Single and Multiple Visits: An Overview of Systematic Reviews. J. Endod. 2017, 43, 864–870. [Google Scholar] [CrossRef] [PubMed]
- Paredes-Vieyra, J.; Enriquez, F.J.J. Success Rate of Single- versus Two-Visit Root Canal Treatment of Teeth with Apical Periodontitis: A Randomized Controlled Trial. J. Endod. 2012, 38, 1164–1169. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Kim, E. Antimicrobial Effect of Calcium Hydroxide as an Intracanal Medicament in Root Canal Treatment: A Literature Review—Part I. In Vitro Studies. Restor. Dent. Endod. 2014, 39, 241–252. [Google Scholar] [CrossRef]
- Zancan, R.F.; Vivan, R.R.; Lopes, M.R.M.; Weckwerth, P.H.; de Andrade, F.B.; Ponce, J.B.; Duarte, M.A.H. Antimicrobial Activity and Physicochemical Properties of Calcium Hydroxide Pastes Used as Intracanal Medication. J. Endod. 2016, 42, 1822–1828. [Google Scholar] [CrossRef]
- Dechouniotis, G.; Petridis, X.M.; Georgopoulou, M.K. Influence of Specialty Training and Experience on Endodontic Decision Making. J. Endod. 2010, 36, 1130–1134. [Google Scholar] [CrossRef]
- Lee, J.; Kang, S.; Jung, H.-I.; Kim, S.; Karabucak, B.; Kim, E. Dentists’ Clinical Decision-Making about Teeth with Apical Periodontitis Using a Variable-Controlled Survey Model in South Korea. BMC Oral Health 2020, 20, 23. [Google Scholar] [CrossRef]
- McCaul, L.K.; McHugh, S.; Saunders, W.P. The Influence of Specialty Training and Experience on Decision Making in Endodontic Diagnosis and Treatment Planning. Int. Endod. J. 2001, 34, 594–606. [Google Scholar] [CrossRef]
- Sul, H.; Liao, H.-F.; Fiorellini, J.; Kim, S.; Korostoff, J. Factors Affecting Treatment Planning Decisions for Compromised Anterior Teeth. Int. J. Periodontics Restor. Dent. 2014, 34, 389–398. [Google Scholar] [CrossRef]
- Hulsmann, M.; Peters, O.A.; Dummer, P.M.H. Mechanical Preparation of Root Canals: Shaping Goals, Techniques and Means. Endod. Top. 2005, 10, 30–76. [Google Scholar] [CrossRef]
- Peralta-Mamani, M.; Rios, D.; Duarte, M.A.H.; Santiago, J.F., Jr.; Honório, H.M. Manual vs. Rotary Instrumentation in Endodontic Treatment of Permanent Teeth: A Systematic Review and Meta-Analysis. Am. J. Dent. 2019, 32, 311–324. [Google Scholar] [PubMed]
- Chu, D.; Lockwood, C. The Effectiveness of Nickel-Titanium versus Stainless Steel Instrumentation for Non-Surgical Endodontic Therapy: A Systematic Review Protocol. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 127–138. [Google Scholar] [CrossRef]
- Radwański, M.; Łęski, M.; Puszkarz, A.K.; Krucińska, I. Shaping Ability of ProTaper Next, Hyflex CM, and V-Taper 2H Nickel-Titanium Files in Mandibular Molars: A Micro-Computed Tomographic Study. Iran. Endod. J. 2021, 16, 103–108. [Google Scholar] [CrossRef]
- Alsulaimani, R.; Al-Manei, K.; Alsubait, S.; AlAqeely, R.; Al-Shehri, S.; Al-Madi, E.M. Effects of Clinical Training and Case Difficulty on the Radiographic Quality of Root Canal Fillings Performed by Dental Students in Saudi Arabia. Iran. Endod. J. 2015, 10, 268–273. [Google Scholar] [CrossRef]
- Farooq, M.; Kyani, S.G.; Hassan, F.; Toosy, W.J.; Malik, S.; Jabeen, W. Evaluation of Complications of Root Canal Treatment Performed by BDS Fresh Graduates. Med. Forum Mon. 2019, 30, 28–32. [Google Scholar]
- Grock, C.H.; Luz, L.B.; Oliveira, V.F.; Ardenghi, T.M.; Bizarro, L.; Ferreira, M.B.C.; Montagner, F. Experiences during the Execution of Emergency Endodontic Treatment and Levels of Anxiety in Dental Students. Eur. J. Dent. Educ. 2018, 22, e715–e723. [Google Scholar] [CrossRef]
- Adebayo, E.T.; Ahaji, L.E.; Nnachetta, R.N.; Nwankwo, O.; Akabogu-Okpeseyi, N.; Yaya, M.O.; Hussain, N.A. Technical Quality of Root Canal Fillings Done in a Nigerian General Dental Clinic. BMC Oral Health 2012, 12, 42. [Google Scholar] [CrossRef]
- Polyzos, N.K.; Sarris, K.G.; Pita, A.I.; Mikrogeorgis, G.V.; Lyroudia, K.M. Factors Affecting the Outcome of Non-Surgical Endodontic Treatments Performed by Undergraduate Students in a Greek Dental School. Eur. Endod. J. 2018, 3, 93–100. [Google Scholar] [CrossRef]
- Hamasha, A.A.; Hatiwsh, A. Quality of Life and Satisfaction of Patients after Nonsurgical Primary Root Canal Treatment Provided by Undergraduate Students, Graduate Students and Endodontic Specialists. Int. Endod. J. 2013, 46, 1131–1139. [Google Scholar] [CrossRef]
- Touboul, V.; Germa, A.; Lasfargues, J.J.; Bonte, E. Outcome of Endodontic Treatments Made by Postgraduate Students in the Dental Clinic of Bretonneau Hospital. Int. J. Dent. 2014, 2014, 684979. [Google Scholar] [CrossRef]
- Khabbaz, M.G.; Protogerou, E.; Douka, E. Radiographic Quality of Root Fillings Performed by Undergraduate Students. Int. Endod. J. 2010, 43, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Borén, D.L.; Jonasson, P.; Kvist, T. Long-Term Survival of Endodontically Treated Teeth at a Public Dental Specialist Clinic. J. Endod. 2015, 41, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Alley, B.S.; Kitchens, G.G.; Alley, L.W.; Eleazer, P.D. A Comparison of Survival of Teeth Following Endodontic Treatment Performed by General Dentists or by Specialists. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2004, 98, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Pietrzycka, K.; Wujec, P.; Olczyk, I.; Pawlicka, H. Endodontic Procedures Used by Dental Practitioners in Daily Dental Practice—Questionnaire Study. J. Stomatol. 2016, 69, 183–200. [Google Scholar] [CrossRef]
- Patel, S.; Dawood, A.; Whaites, E.; Ford, T.P. New Dimensions in Endodontic Imaging: Part 1. Conventional and Alternative Radiographic Systems. Int. Endod. J. 2009, 42, 447–462. [Google Scholar] [CrossRef]
- Davies, A.; Patel, S.; Foschi, F.; Andiappan, M.; Mitchell, P.J.; Mannocci, F. The Detection of Periapical Pathoses Using Digital Periapical Radiography and Cone Beam Computed Tomography in Endodontically Retreated Teeth—Part 2: A 1 Year Post-Treatment Follow-Up. Int. Endod. J. 2016, 49, 623–635. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter of Root Canal Filling | Criteria | Definition |
|---|---|---|
| Length | Adequate | Root filling ≤2 mm from radiographic apex |
| Overfilling | Root filling beyond the radiographic apex (gutta-percha cones or/and sealer) | |
| Short-filling | Root filling >2 mm from radiographic apex | |
| Density | Adequate | Voids absent, homogeneous root filling |
| Inadequate | Voids present, heterogeneous root filling |
| Number of Root Canals | ||||
|---|---|---|---|---|
| Group/Diagnoses | Adequate | Overfilling | Short-Filling | Total |
| 4th year students | 286 (81.71%) | 40 (11.4%) | 24 (6.86%) | 350 |
| 5th year students | 325 (86.67%) | 41 (10.9%) | 9 (2.40%) | 375 |
| GPDs | 367 (85.75%) | 43 (10.0%) | 18 (4.21%) | 428 |
| Endodontists | 432 (74.48%) | 129 (22.2%) | 19 (3.28%) | 580 |
| Total | 1410 (81.36%) | 253 (14.60%) | 70 (4.04%) | 1733 |
| Group/Rotary System | ProTaper Next (Dentsply Maillefer) | Mtwo (VDW) | E3 Azure (Poldent) | DC-Taper 2H (SS White) |
|---|---|---|---|---|
| Number of Teeth | ||||
| GPDs | 184 | 6 | 1 | 18 |
| Endodontists | 208 | 48 | 1 | 0 |
| Group/Teeth | Incisors | Canines | Premolars | Molars | Total |
|---|---|---|---|---|---|
| 4th year students | 64 (29.63%) | 43 (19.91%) | 63 (29.17%) | 46 (21.30%) | 216 |
| 5th year students | 67 (30.73%) | 41 (18.81%) | 44 (20.18%) | 66 (30.28%) | 218 |
| GPDs | 41 (19.62%) | 25 (11.96%) | 53 (25.36%) | 90 (43.06%) | 209 |
| Endodontists | 52 (20.23%) | 16 (6.23%) | 73 (28.40%) | 116 (45.14%) | 257 |
| Total | 224 (24.89%) | 125 (13.89%) | 233 (25.89%) | 318 (35.33%) | 900 |
| Group/Diagnoses | Pulp | Periapical | Endo-Perio | Total |
|---|---|---|---|---|
| Number of teeth | ||||
| 4th year students | 133 (61.57%) | 83 (38.43%) | 0 | 216 |
| 5th year students | 113 (51.83%) | 105 (48.17%) | 0 | 218 |
| GPDs | 107 (51.20%) | 97 (46.41%) | 5 (2.39%) | 209 |
| Endodontists | 149 (57.98%) | 108 (42.02%) | 0 | 257 |
| Total | 502 (55.78%) | 393 (43.67%) | 5 (0.56%) | 900 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pietrzycka, K.; Radwanski, M.; Hardan, L.; Bourgi, R.; Mancino, D.; Haikel, Y.; Lukomska-Szymanska, M. The Assessment of Quality of the Root Canal Filling and the Number of Visits Needed for Completing Primary Root Canal Treatment by Operators with Different Experience. Bioengineering 2022, 9, 468. https://doi.org/10.3390/bioengineering9090468
Pietrzycka K, Radwanski M, Hardan L, Bourgi R, Mancino D, Haikel Y, Lukomska-Szymanska M. The Assessment of Quality of the Root Canal Filling and the Number of Visits Needed for Completing Primary Root Canal Treatment by Operators with Different Experience. Bioengineering. 2022; 9(9):468. https://doi.org/10.3390/bioengineering9090468
Chicago/Turabian StylePietrzycka, Krystyna, Mateusz Radwanski, Louis Hardan, Rim Bourgi, Davide Mancino, Youssef Haikel, and Monika Lukomska-Szymanska. 2022. "The Assessment of Quality of the Root Canal Filling and the Number of Visits Needed for Completing Primary Root Canal Treatment by Operators with Different Experience" Bioengineering 9, no. 9: 468. https://doi.org/10.3390/bioengineering9090468
APA StylePietrzycka, K., Radwanski, M., Hardan, L., Bourgi, R., Mancino, D., Haikel, Y., & Lukomska-Szymanska, M. (2022). The Assessment of Quality of the Root Canal Filling and the Number of Visits Needed for Completing Primary Root Canal Treatment by Operators with Different Experience. Bioengineering, 9(9), 468. https://doi.org/10.3390/bioengineering9090468