

The Biomechanical Profile of an Osseo-Integrated Rectangular Block Implant: A Pilot In Vivo Strain Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. The Rectangular Block Implant
2.2. Animal Surgery and Ethics
2.3. Osseo-Integration
2.4. Embedding
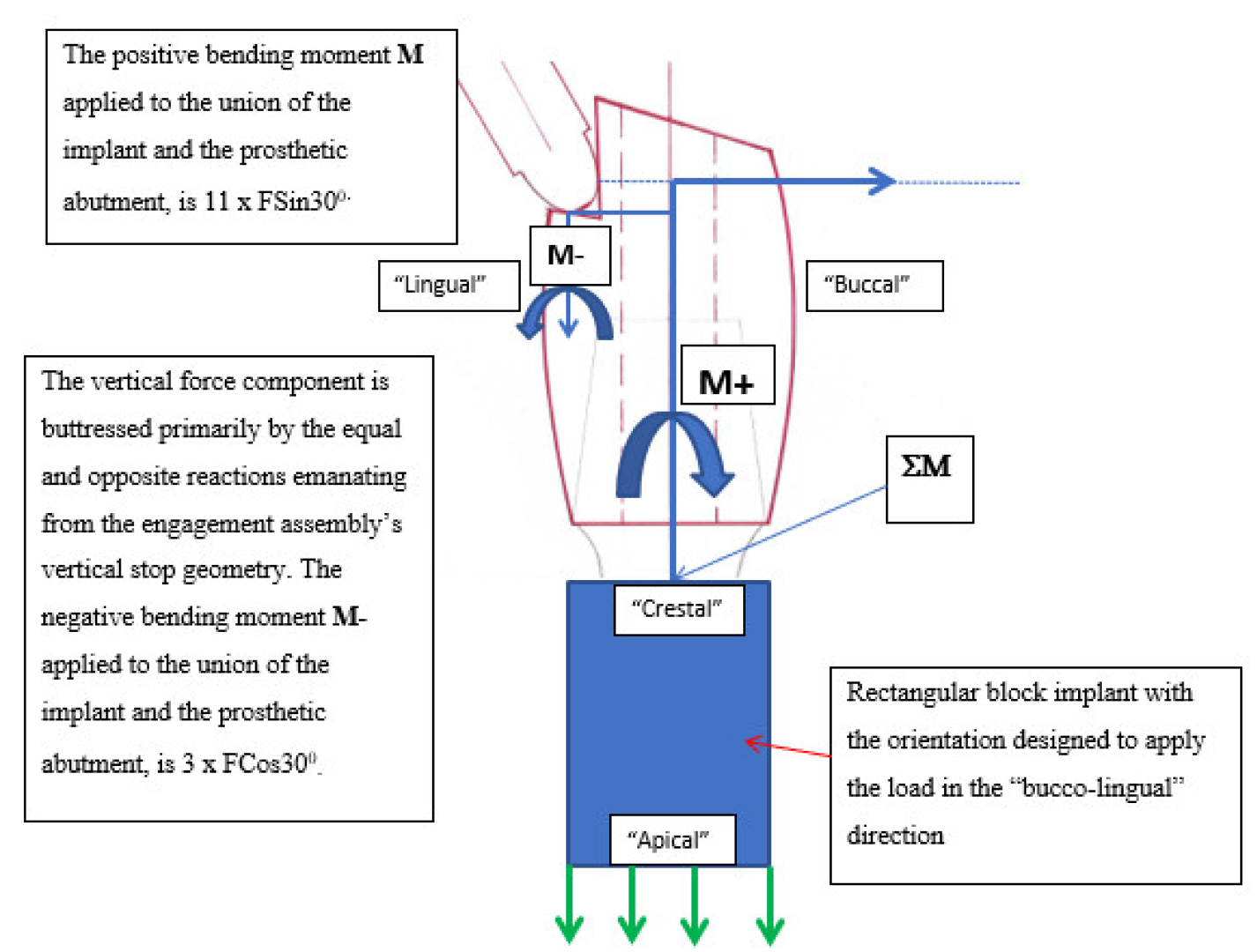
2.5. Prosthetic Crown and the Force Application
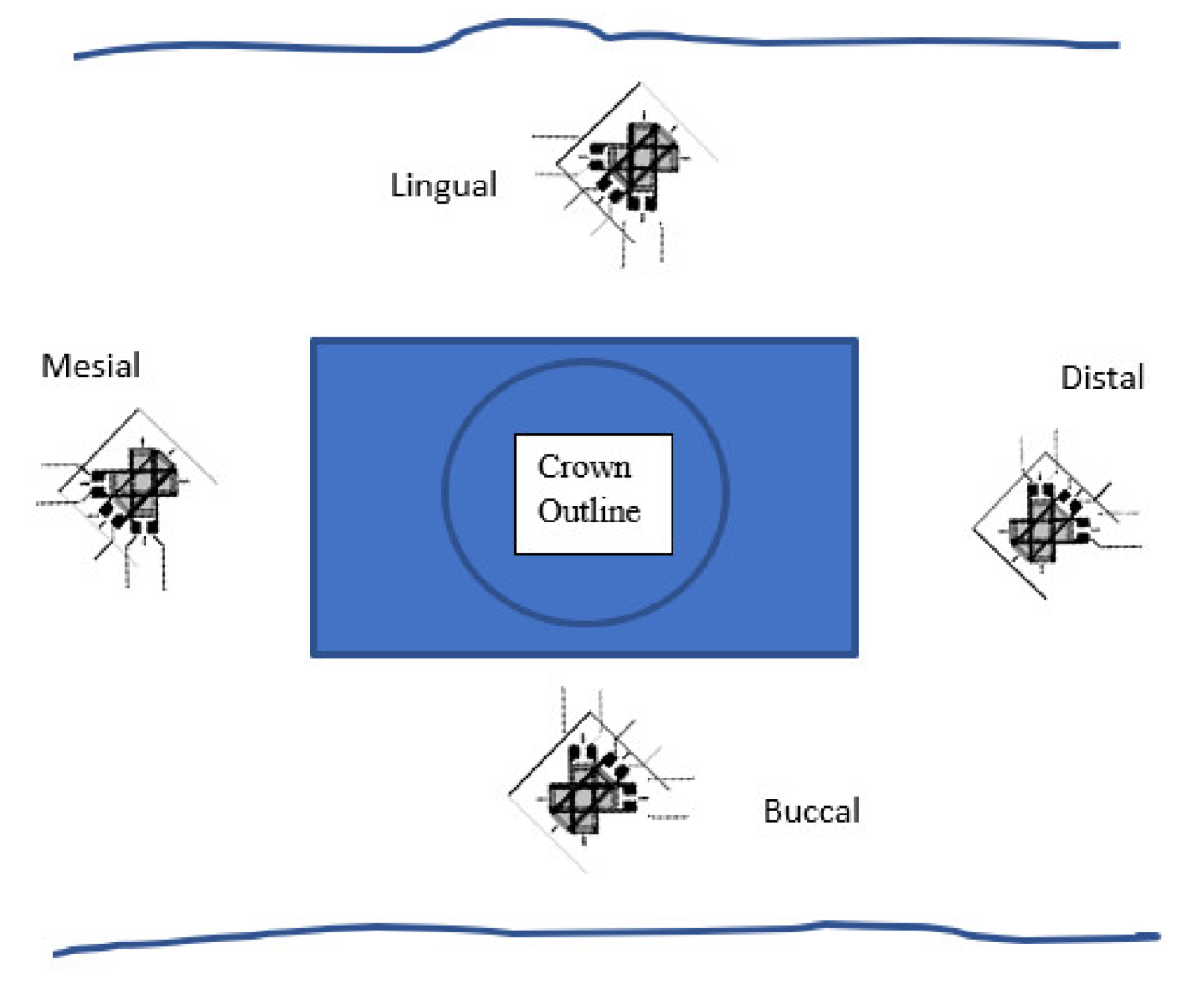
2.6. Strain Gauges
2.7. The Mounted Set-Up
3. Results
3.1. Channel Data
3.2. Principal Strains
- (a)
- If ε1 > ε3, then ϕp,q = ϕp: the reference is from ε1 to εp.
- (b)
- If ε1 < ε3, then ϕp,q = ϕq: the reference is from ε3 to εq.
- (c)
- If ε1 = ε3 and ε2 < ε1, then ϕp,q = ϕp = −45°.
- (d)
- If ε1 = ε3 and ε2 > ε1, then ϕp,q = ϕp = +45°.
- (e)
- If ε1 = ε2 = ε3, then ϕp,q is indeterminate (equal bi-axial strain).
- (i)
- Relative to the associated absolute ε1 and ε3 readings for that output;
- (ii)
- Indicative of a high torsional element affecting that peri-implant cortex.
3.3. Observational Summary
4. Discussion
4.1. Measured Cortical Strains
- (a)
- In the buco-lingual horizontal dimension: dominant “horizontal” compressive stresses on the lingual aspect, coupled with “horizontal” tensile stresses on the buccal aspect.
- (b)
- In the bucco-lingual “vertical” dimension: dominant vertical torsional stresses oriented buccally and apically.
- (c)
- In the mesio-distal “horizontal” dimension: dominant torsional stresses oriented as a distal-buccal “counter-clockwise” rotation.
4.2. Tensile and Compressive Elements in the Bucco-Lingual (Horizontal) Dimension
- (i)
- Horizontally. In the horizontal bucco-lingual aspect, this could be seen as an elastic deformation of the body of the mandible. The deformation of the lingual cortex would have resulted in concavity, while that of the buccal cortex would have resulted in convexity. This equated to a three-point bending configuration.
- (ii)
- Vertically. The second ramification of this strain pattern was in the vertical (axial) and bucco-lingual aspect, where there was an overall buccally inclined torsional effect (Figure 8). This was evidenced on the lingual aspect, where there remained high torsional rotation elements (high Φ and ε2), giving a complex picture of lingual compression and a buccally directed torsion.
4.3. Mesio-Distal Torsion
4.4. Combined Mesio-Distal and Bucco-Lingual Torsion
4.5. The Complexity of the Principal Strains and their Angular Orientations
- (i)
- The angulation and rotation of the block in the mandible, e.g., the bucco-lingual slant. This factor varied with respect to the differences between the crestal morphology of the alveolar ridge and the underlying cross-sectional morphology of the body of the mandible.
- (ii)
- The particular pattern of osseo-integration around the block itself. Judge [34] extensively studied the trabecular and cortical architecture of the dog mandible, depicting a high level of variation and heterogeneity in its make-up, while Monje et al. [35] have highlighted the variability in trabecular density and volume in the posterior mandible from site to site.
- (iii)
- The particular relative thicknesses of the cortical and cancellous bone, as well as the shape of the mandible at the position of the implant. These factors would have affected the critical elements of cortical flexural stress and cancellous tensile shear stress, as defined by the mathematical principles of such a bi-layered composite beam [36,37].
- (iv)
- The inability to perfectly align the application of the force. The step on the crown and the engaging push rod would inevitably have some degree of variation in their orientations. Deviations from perfect parallelism would be expressed as a bias in force resolution, as well as the resultant axial moments, torsional stress concentrations, and strain levels.
4.6. Physiological Limits
- (i)
- The importance of the role of the mandible as a single and flexible composite beam.
- (ii)
- The rectangular design.
4.7. Limitations
5. Conclusions
- (i)
- Tensile and compressive strains were expressed bucco-lingually and mesio-distally.
- (ii)
- Bucco-lingually, there was a “horizontal” flexure of the body of the mandible, producing buccal tensile strains and lingual compressive strains.
- (iii)
- Bucco-lingually, there were strong “vertical” torsional stresses directed apically on the buccal aspect.
- (iv)
- Mesio-distally, there were strong horizontal torsional stresses in a disto-buccal orientation.
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rosentiel, S.F.; Land, M.F.; Fujimoto, J. Contemporary Fixed Prosthodontics, 4th ed.; Mosby Publishing Co.: St. Louis, MO, USA, 2006; p. 381. [Google Scholar]
- Kan, J.; Judge, R.B.; Palamara, J. In Vitro bone strain analysis of implant following occlusal overload. Clin. Oral Implant. Res. 2014, 25, e73–e82. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E.; Suzuki, J.B.; Dietsh-Misch, F.; Bidez, M.W. A positive correlation between occlusal trauma and peri-implant bone loss: Literature support. Implant. Dent. 2005, 14, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Cehreli, M.; Sahin, S.; Akca, K. Role of mechanical environment and implant design on bone tissue differentiation: Current knowledge and future contexts. J. Dent. 2004, 32, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Gazelakis, E.; Judge, R.B.; Palamara, J.E. The biomechanical profile of an osseo-integrated rectangular block implant: A pilot in vivo experimental study. Clin. Oral Implant. Res. 2021, 32, 1274–1287. [Google Scholar] [CrossRef]
- Isidor, F. Loss of osseo-integration caused by occlusal load of oral implants–A clinical and radiographic study in monkeys. Clin. Oral Implant. Res. 1996, 7, 143–152. [Google Scholar] [CrossRef]
- Rilo, B.; da Silva, J.L.; Mora, M.J.; Santana, U. Guidelines for occlusion strategy in implant-borne prostheses. A review. Int. Dent. J. 2008, 58, 139–145. [Google Scholar] [CrossRef]
- Kim, Y.; Oh, T.J.; Misch, C.E.; Wang, H.L. Occlusal considerations in implant therapy: Clinical guidelines with biomechanical rationale. Clin. Oral Implant. Res. 2005, 16, 26–35. [Google Scholar] [CrossRef]
- Klineberg, I.; Kingston, D.; Murray, G. The bases for using a particular occlusal design in tooth and implant-borne reconstructions and complete dentures. Clin. Oral Implant. Res. 2007, 18, 151–167. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.; Schmid, B.; Weigel, C.; Gerber, S.; Bosshardt, D.D.; Johnsson, J.; Lang, N.P. Does excessive occlusal load affect osseo-integration? An experimental study in the dog. Clin. Oral Implant. Res. 2004, 159, 259–268. [Google Scholar] [CrossRef]
- Jemt, T.; Albrektsson, T. Do long-term followed-up of Branemark implants commonly show evidence of pathological bone breakdown? A review based on recently published data. Periodontology 2000 2008, 47, 133–142. [Google Scholar] [CrossRef]
- Chambrone, L.A.; Lima, L.A. Effects of occlusal overload on peri implant tissue health: A systematic review of animal-model studies. J. Periodontol. 2010, 81, 1367–1378. [Google Scholar] [CrossRef]
- Naert, I.; Quirynen, M.; van Steenberghe, D.; Darius, P. A study of 589 consecutive implants supporting complete fixed prosthesis. Part II: Prosthetic aspects. J. Prosthet. Dent. 1992, 68, 949–956. [Google Scholar] [CrossRef]
- Quirynen, M.; Naert, I.; van Steenberghe, D. Fixture design and overload influence marginal bone loss and fixture success in Branemark system. Clin. Oral Implant. Res. 1992, 3, 104–111. [Google Scholar] [CrossRef]
- Esposito, M.; Hirsch, J.M.; Lekholm, U.; Thomsen, P. Biological factors contributing to failures of osseo-integrated oral implants. (I). Success criteria and epidemiology. Eur. J. Oral Sci. 1998, 106, 527–551. [Google Scholar] [CrossRef]
- Ekfeldt, A.; Christiansson, U.; Eriksson, T.; Linden, U.; Lundqvist, S.; Rundcrantz, T.; Johansson, L.; Nilner, K.; Billstrom, C. A retrospective analysis of factors associated with multiple implant failures in maxillae. Clin. Oral Implant. Res. 2001, 12, 462–467. [Google Scholar] [CrossRef]
- Fugazzotto, P.A. A comparison of the success of root resected molars and molar position implants in function in a private practice: Results of up to 15-plus years. J. Periodontol. 2001, 72, 1113–1123. [Google Scholar] [CrossRef]
- Shackleton, J.L.; Carr, L.; Slabbert, J.C.G.; Becker, P.J. Survival of fixed implant-supported prostheses related to cantilever lengths. J. Prosthet. Dent. 1994, 71, 23–26. [Google Scholar] [CrossRef]
- Duyck, J.; Van Oosterwyck, H.; Vander Sloten, J.; De Cooman, M.; Puers, R.; Naert, I. Magnitude and distribution of occlusal forces on oral implants supporting fixed prostheses: An in vivo study. Clin. Oral Implant. Res. 2000, 11, 465–475. [Google Scholar] [CrossRef]
- Wyatt, C.C.; Zarb, G.A. Bone level changes proximal to oral implants supporting fixed partial prostheses. Clin. Oral Implant. Res. 2002, 13, 162–168. [Google Scholar] [CrossRef]
- Rangert, B.; Krogh, P.; Langer, B.; Van Roekel, N. Bending overload and implant fracture: A retrospective clinical analysis. Int. J. Oral Maxillofac. Implant. 1995, 10, 326–334. [Google Scholar]
- Engel, G.R.G.; Axmann-Krcmar, D. Effect of occlusal wear on bone loss and Periotest value of dental implants. Int. J. Prosthodont. 2001, 14, 444–450. [Google Scholar] [PubMed]
- Wennerberg, A.; Carlsson, G.; Jemt, T. Influence of occlusal factors on treatment outcome: A study of 109 consecutive patients with mandibular implant-supported fixed prostheses opposing maxillary complete dentures. Int. J. Prosthodont. 2001, 14, 550–555. [Google Scholar] [PubMed]
- Lobbezoo, F.; Van Der Zaag, J.; Naeije, M. Bruxism: Its multiple causes and its effects on dental implants—An updated review. J. Oral Rehabil. 2006, 33, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Blanes, R. To what extent does the crown-implant ratio affect the survival and complications of implant supported reconstructions? A systematic review. Clin. Oral Implant. Res. 2009, 20 (Suppl. 4), 67–72. [Google Scholar] [CrossRef]
- Salvi, G.E.; Bragger, U. Mechanical and technical risks in implant therapy. Int. J. Oral Maxillofac. Implant. 2009, 24 (Suppl. 2009), 69–85. [Google Scholar]
- Zurdo, J.; Romao, C.; Wennstrom, J. Survival and complication rates of implant-supported fixed partial dentures with cantilevers: A systematic review. Clin. Oral Implant. Res. 2009, 20 (Suppl. 4), 59–66. [Google Scholar] [CrossRef]
- Johansson, A.; Omar, R.; Carlsson, G.E. Bruxism and prosthetic treatment: A critical review. J. Prosthodont. Res. 2011, 55, 127–136. [Google Scholar] [CrossRef]
- Herring, S.W.; Rafferty, K.L.; Liu, Z.J.; Marshall, C.D. Jaw muscles and the skull in mammals: The biomechanics of mastication. Comp. Biochem. Physiol. Part A Mol. Integr. Physiol. 2001, 131, 207–219. [Google Scholar] [CrossRef]
- Frost, H.M. Bone “Mass” and the “Mechanostat”: A proposal. Anat. Rec. 1987, 219, 1–9. [Google Scholar] [CrossRef]
- Frost, H.M. The Utah paradigm of skeletal physiology: An overview of its insights for bone, cartilage and collagenous tissue organs. J. Bone Miner. Metab. 2000, 18, 305–316. [Google Scholar] [CrossRef]
- Frost, H.M. Why should many skeletal scientists and clinicians learn the Utah paradigm of skeletal physiology? J. Musculoskelet. Neuronal Interact. 2001, 2, 121–130. [Google Scholar]
- Percie du Sert, N.; Ahluwalia, A.; Alam, S.; Avey, M.T.; Baker, M.; Browne, W.J.; Clark, A.; Cuthill, I.C.; Dirnagl, U.; Emerson, M.; et al. Reporting animal research: Explanation and elaboration for the ARRIVE guidelines 2.0. PLoS Biol. 2020, 18, e3000411. [Google Scholar] [CrossRef]
- Judge, R.B. An In Vitro and In Vivo Investigation into Masticatory Bone Strain Using a Dog Model. Ph.D. Thesis, Melbourne Dental School, University of Melbourne, Parkville, VIC, Australia, 2006. [Google Scholar]
- Monje, A.; Chan, H.L.; Galindo-Moreno, P.; Elnayef, B.; Suarez-Lopez del Amo, F.; Wang, F.; Wang, H.L. Alveolar Bone Architecture: A systematic review and meta-analysis. J. Periodontol. 2015, 86, 1231–1248. [Google Scholar] [CrossRef]
- Zenkert, D. An Introduction to Sandwich Construction; Engineering Materials Advisory Services Ltd.: Worcestershire, UK, 1995. [Google Scholar]
- Silva, M.J.; Reed, K.L.; Robertson, D.D.; Bragdon, C.; Harris, W.H.; Maloney, W.J. Reduced bone stress predicted by composite beam theory correlates with bone loss following total hip arthroplasty. J. Orthop. Res. 1999, 17, 525–531. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mesial, Buccal, Distal, and Lingual Gauges (All Readings in Micro-Strain: με) | ||||
|---|---|---|---|---|
| Channel | ε1 | ε2 | ε3 | |
| mesial gauge | ||||
| mean max-min difference | 798 ± 35 | −1551 ± 98 | −639 ± 47 | |
| tens/comp | tension | compression | compression | |
| 1000 N | ||||
| buccal gauge | ||||
| mean max-min difference | −1029 ± 104 | 489 ± 23 | 1618 ± 121 | |
| tens/comp | compression | tension | tension | |
| distal gauge | ||||
| mean max-min difference | −285 ± 31 | −1281 ± 127 | −1742 ± 186 | |
| tens/comp | compression | compression | compression | |
| 1000 N | ||||
| lingual gauge | ||||
| mean max-min difference | −707 ± 56 | 732 ± 17 | 757 ± 98 | |
| tens/comp | compression | tension | tension | |
| Principle Strains: Magnitudes (με) and Angular Resolve | |||||
|---|---|---|---|---|---|
| Load | Gauge | εp | εq | θ/φ0 | Absolute Value |
| Mesial | 1822 | −1663 | 33.0 | ε1 > ε3 (ε2 large) | |
| 1000 N | Distal | 67 | −2094 | 10.0 | ε1 > ε3 (ε2 large) |
| Buccal | 1632 | −1043 | 4.2 | ε1 < ε3 | |
| Lingual | 2096 | −2047 | 21.9 | ε1 > ε3 (ε2 large) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gazelakis, E.; Judge, R.B.; Palamara, J.E.A.; Nazir, M. The Biomechanical Profile of an Osseo-Integrated Rectangular Block Implant: A Pilot In Vivo Strain Analysis. Bioengineering 2022, 9, 425. https://doi.org/10.3390/bioengineering9090425
Gazelakis E, Judge RB, Palamara JEA, Nazir M. The Biomechanical Profile of an Osseo-Integrated Rectangular Block Implant: A Pilot In Vivo Strain Analysis. Bioengineering. 2022; 9(9):425. https://doi.org/10.3390/bioengineering9090425
Chicago/Turabian StyleGazelakis, Efthimios, Roy B. Judge, Joseph E. A. Palamara, and Mohsin Nazir. 2022. "The Biomechanical Profile of an Osseo-Integrated Rectangular Block Implant: A Pilot In Vivo Strain Analysis" Bioengineering 9, no. 9: 425. https://doi.org/10.3390/bioengineering9090425
APA StyleGazelakis, E., Judge, R. B., Palamara, J. E. A., & Nazir, M. (2022). The Biomechanical Profile of an Osseo-Integrated Rectangular Block Implant: A Pilot In Vivo Strain Analysis. Bioengineering, 9(9), 425. https://doi.org/10.3390/bioengineering9090425