
Biodegradable Bone Implants as a New Hope to Reduce Device-Associated Infections—A Systematic Review



Abstract
:1. Introduction
1.1. Infection
1.2. Implants
2. Methods
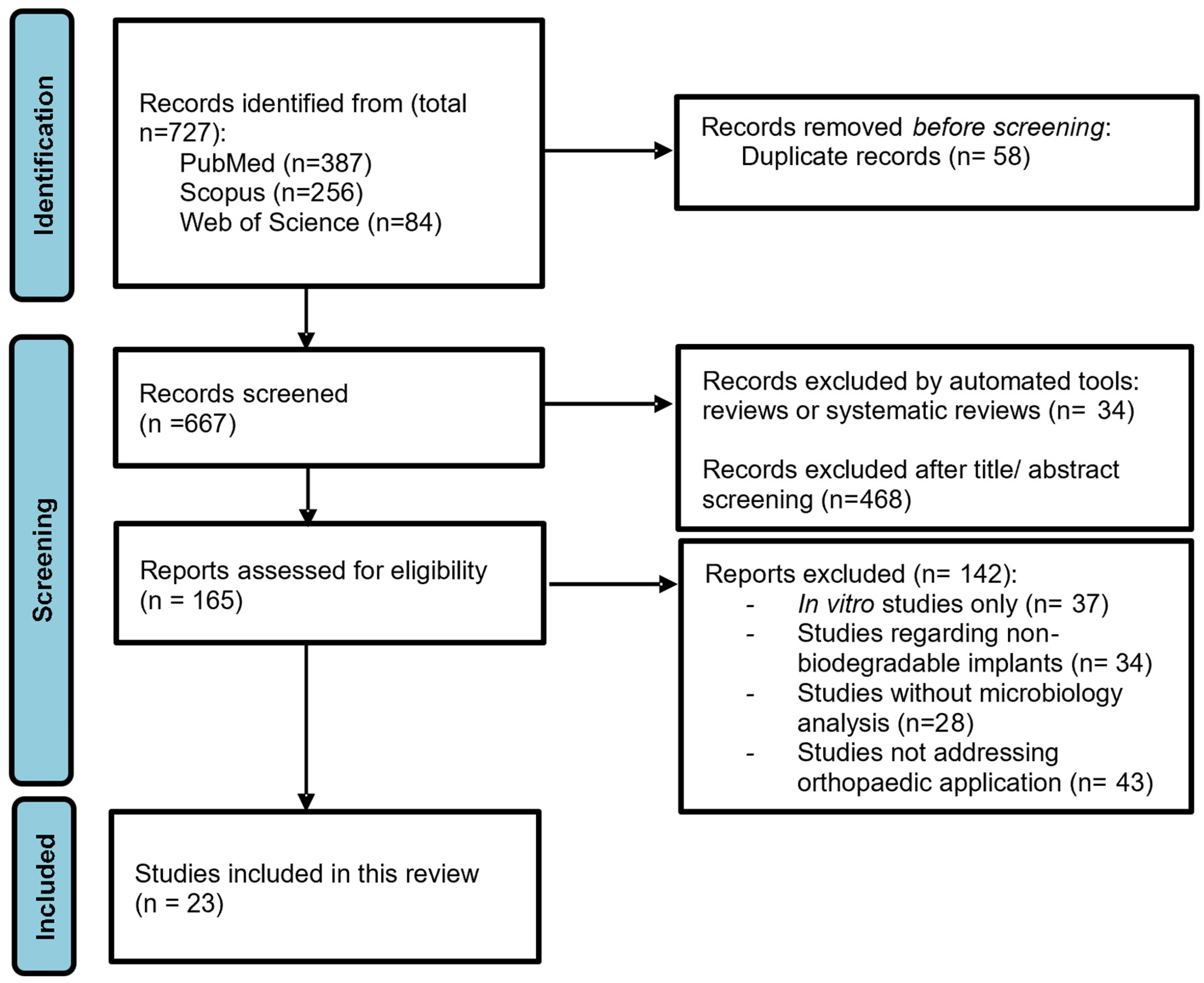
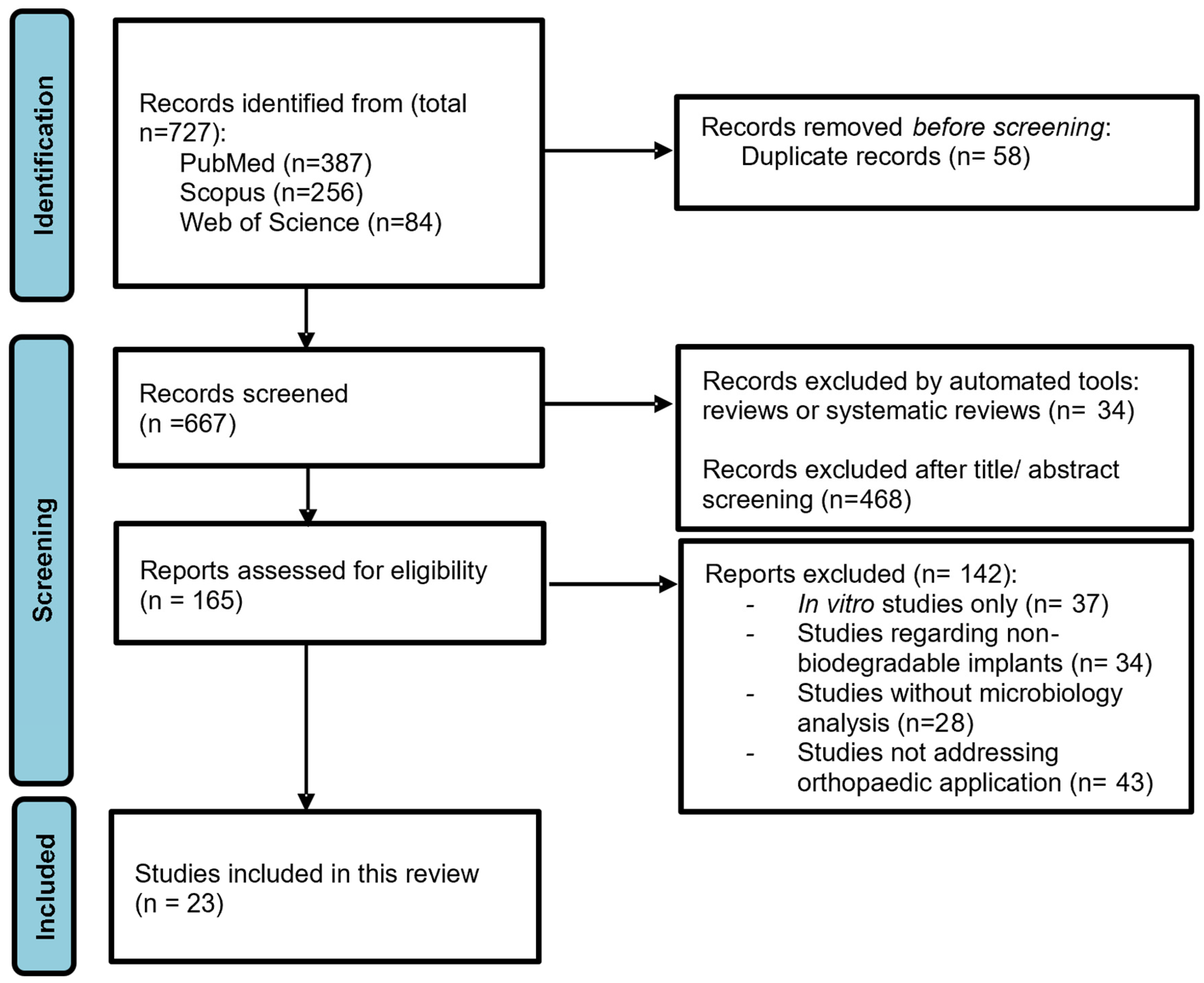
2.1. Data Sources and Search Strategy
2.2. Study Eligibility Criteria
2.3. Data Extraction and Search Results
2.4. Assessment of Risk of Bias
3. Results
3.1. Biomaterials
3.2. Antimicrobial Agents

{kind=link}
{kind=link}
| Ref. | Implant Type | Production Process | Control | Polymers | Calcium Phosfates | Bone | Macromolecules | Silica | Nanoparticles | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PLGA | PEG 400 | PLLA | PLDLA | PU | PCL | P3HB | BCP | β-TCP | HA | n-HA | BHA | DPB | DBBP | CMC | PAA | MSN | RGO | ||||
| [81] | Cylindrical Scaffold | Melt-blending, powder production and moulding | x | x | x | x | |||||||||||||||
| [89] | Scaffold Granules | Emulsification-solvent evaporation; homogeneous method using an in-situ diffusion control system | x | x | x | ||||||||||||||||
| [82] | Cylindrical Scaffold | Bovine cancellous bone deproteinization; 3D Printing using Electrospinning | x | x | |||||||||||||||||
| [91] | Cylindrical Scaffold | Injection molding, hot melt dip coating | x | ||||||||||||||||||
| [83] | Scaffold | 3D printing using Electrospinning, aqueous precipitation of PLLA | x | x | |||||||||||||||||
| [71] | Screw | Mold injection process | x | x | |||||||||||||||||
| [86] | Scaffold | In situ foaming (method), Freeze-drying, mold\die production process | x | x | |||||||||||||||||
| [85] | Scaffold | 3D printed Electrospun PU fibers | x | x | x | ||||||||||||||||
| [87] | Scaffold | 3D printing of in-situ deposition of foams | x | x | x | ||||||||||||||||
| [80] | Disc | 3D Printing, in situ precipitation | x | ||||||||||||||||||
| [79] | Pellets | Bacterial biomass (bacterium Ralstonia eutropha B5786); Granulation, cold molding and water leaching | Bio-Oss® | x | x | ||||||||||||||||
| [84] | Scaffold | 3D Precipitation in aqueous solution | x | x | |||||||||||||||||
| Ref. | Implant Type | Production Process | Control | Metals | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mg | Zn | Cu | Ag | Ga | Sr | Al | Sn | Nd | Zr | ||||
| [68] | Nail | UMAO, Phytic acid conversion coating, electroless copper plating | x | ||||||||||
| [72] | Screw | Additive Manufacturing, laser sintering, cold rolling | Ti | x | |||||||||
| [74] | Rod | Micro-alloying, powder metallurgy | cpTi | x | x | x | |||||||
| [69] | Nail | Metallurgical casting | Ti | x | x | ||||||||
| [73] | Rod | Powder metallurgy | cpTi | x | x | x | |||||||
| [76] | Rod | Solid-phase synthesis | x | x | x | ||||||||
| [77] | Rod | Powder Metalurgy, localized melting of Powders | Ti | x | x | x | |||||||
| [88] | Cylinder | Additive manufacturing; selective laser melting | Ti | x | x | x | x | ||||||
| [78] | Wire | Powder metallurgy | Ti | x | x | ||||||||
| [75] | Rod | Extrusion of heat-treated materials | Ti | x | x | ||||||||
| [70] | Screw | Extrusion of heat-treated materials | Ti | x | x | ||||||||
| Ref. | Implant Type (Scaffold, Screw, …) | Coating/Impregnated Antibiotics | Study Design/Type of Study | Surgical Site | Microorganisms | Previous Stablished Infection | Inoculation/Seeding of Microorganisms | Prophylatic Antimicrobial Admin. | Sacrifice Timepoint/Follow-Up Time after Surgery | Bioabsortion/Biodegradability | Osteointegration | Microbiology analysis In Vitro | Microbiology Analysis In Vivo | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [81] | Cylindrical Scaffold | None | In vivo | Femoral condyle | S. aureus (F2789) | No | At surgery | No | 2 weeks | No | No | - | Presence of S. aureus (F2789) | The scaffold impregnated with 4% Gentamicin + 2.5% Clindamycin was effective at preventing S. aureus infection, whilst supporting a significant amount of new bone growth in a 13 week period. |
| 4% Gentamicin + 2.5% Clindamycin | S. aureus (F2789) | At surgery | 2 weeks | No bacteria found | ||||||||||
| None | None | No | 2 weeks | |||||||||||
| None | None | No | 13 weeks | Yes | Yes | |||||||||
| 4% Gentamicin + 2.5% Clindamycin | S. aureus (F2789) | At surgery | 13 weeks | |||||||||||
| [89] | Scaffold granules | None | In vivo | Tibia metaphysis | S. aureus | Yes | Prior to surgery | No | 4 weeks | - | No | - | - | The V-BHA/PAA scaffold promoted infection clearance and was gradually replaced by new forming bone during degradation. The scaffold and bone almost integrated with one another by the end of the experiment, and the bone defect underwent complete healing. |
| 8 weeks | - | - | ||||||||||||
| 12 weeks | - | - | ||||||||||||
| Vancomycin-encapsulated in PLGA microspheres | S. aureus | 4 weeks | - | Yes | - | |||||||||
| 8 weeks | - | - | ||||||||||||
| 12 weeks | Yes | Clearance of the infection | ||||||||||||
| None | MRSA | 4 weeks | - | No | - | |||||||||
| 8 weeks | - | - | ||||||||||||
| 12 weeks | - | - | ||||||||||||
| Vancomycin-encapsulated in PLGA microspheres | MRSA | 4 weeks | - | Yes | - | |||||||||
| 8 weeks | - | - | ||||||||||||
| 12 weeks | Yes | Clearance of the infection | ||||||||||||
| PMMA Granules | Vancomycin | S. aureus | 4, 8 & 12 weeks | No | No | - | ||||||||
| MRSA | 4, 8 & 12 weeks | No | No | - | ||||||||||
| None(Blank control group) | - | S. aureus | 4, 8 & 12 weeks | - | - | - | ||||||||
| MRSA | 4, 8 & 12 weeks | - | - | - | ||||||||||
| [71] | Screw | None | Case series | Tibia proximal tunnel | P. aeruginosa | Yes | No | Yes | 2–4 years | No | Yes | - | No purulent discharge was observed | The soft-tissue reaction led to extrusion of still intact bioabsorbable screws. |
| [86] | Scaffold | None | In vivo | Tibia proximal metaphysis | S. aureus (ATCC 25923) | Yes | Prior to surgery (4 weeks) | No | 3 weeks | - | Yes | - | Infection progression | n-HA/PU3 and n-HA/PU10 implants were equally efficient in reducing bone infection. There was no significant difference in bone remodeling between these 2 groups, although the degradation of n-HA/PU10 was faster. |
| 6 weeks | Partially | |||||||||||||
| 12 weeks | Yes | |||||||||||||
| Ag (3%) | 3 weeks | Very low | Yes | - | - | |||||||||
| 6 weeks | Partially | - | ||||||||||||
| 12 weeks | Yes | No significant bone infection symptoms | ||||||||||||
| Ag (10%) | 3 weeks | Partially | Yes | - | - | |||||||||
| 6 weeks | Yes | - | ||||||||||||
| 12 weeks | Yes | No significant bone infection symptoms | ||||||||||||
| None(Blank control group) | - | 3, 6 & 12 weeks | - | - | - | Infection progression | ||||||||
| [83] | Scaffold | Silica | In vivo | Femur diaphysis | MRSA (ATCC 43300) | Yes | Prior to surgery (1 week) | No | 1 month | No | No | - | Severe infection | The nanocomposite scaffold with 15 wt% drug can undergo degradation and simultaneously control infection, even though 100% bacterial elimination was not observed. However, it showed higher antibacterial efficiency than the 5 wt% Vancomycin scaffolds. |
| 3 months | - | - | - | |||||||||||
| Silica + Vancomycin (SE-V5) | 1 month | Mostly | - | Significant reduction in infection | ||||||||||
| 3 months | Yes | Yes | ||||||||||||
| Silica + Vancomycin (SA-V5) | 1 month | Mostly | - | |||||||||||
| 3 months | Yes | Yes | ||||||||||||
| Silica + Vancomycin (SE-V15) | 1 month | Mostly | - | |||||||||||
| 3 months | Yes | Yes | ||||||||||||
| Silica + Vancomycin (SA-V15) | 1 month | Mostly | - | |||||||||||
| 3 months | Yes | Yes | ||||||||||||
| [85] | Scaffold | None | In vivo | Radius middle shaft | S. aureus (UAMS-1) | Yes | At surgery | No | 4 weeks | Yes | No | - | Presence of S. aureus | K20 Vancomycin-loaded scaffold prevented infection without compromising the bone regenerative properties of the scaffold itself. The scaffold utility would be compromised in an infected bone defect in the absence of antibiotic. |
| 8 weeks | ||||||||||||||
| 12 weeks | ||||||||||||||
| Vancomycin | 4 weeks | No | Yes | No signs of infection | ||||||||||
| 8 weeks | ||||||||||||||
| 12 weeks | ||||||||||||||
| [87] | Cuboid Scaffold | Gold + Levofloxacin 1 mg | In vivo | Tibia medullary cavit | S. aureus (ATCC 25923) | Yes | Prior to surgery (4 weeks) | - | 1 week | No | No | - | - | 5 mg Lev@ MSNs/n-HA/PU began to degrade 12 weeks after implantation. Prior to 12 weeks, the integrity of the material structure provided mechanical support for bone repair and its degradation contributed to new bone formation. Infection signs were successfully curbed. |
| 3 weeks | Low | - | ||||||||||||
| 6 weeks | - | - | ||||||||||||
| 12 weeks | Partially | Yes | No signs of infection | |||||||||||
| Gold + Levofloxacin 5 mg | 1 week | No | No | - | ||||||||||
| 3 weeks | Low | - | ||||||||||||
| 6 weeks | - | - | ||||||||||||
| 12 weeks | Partially | Yes | No signs of infection | |||||||||||
| None(Blank control group) | - | 1 week | - | No | Infection progression | |||||||||
| 3 weeks | ||||||||||||||
| 6 weeks | ||||||||||||||
| 12 weeks | ||||||||||||||
| PMMA cement | Levofloxacin 1 mg | 1 week | No | No | - | |||||||||
| 3 weeks | - | - | ||||||||||||
| 6 weeks | - | - | ||||||||||||
| 12 weeks | Yes | No signs of infection | ||||||||||||
| Levofloxacin 5 mg | 1 week | No | No | - | ||||||||||
| 3 weeks | - | - | ||||||||||||
| 6 weeks | - | - | ||||||||||||
| 12 weeks | Yes | No signs of infection | ||||||||||||
| [82] | Cylindrical Scaffold | PLGA + Vancomycin | In vivo | Radius diaphysis | MRSA (ATCC 25923) | Yes | At surgery | No | 8 weeks | Yes | Yes | - | Lower bacterial load | ANDB scaffold possesd effective bactericidal activity against MRSA while promoting site-specific bone regeneration. |
| PLGA | Vancomycin | Partially | Partially | Bacterial load in betwen | ||||||||||
| PLGA | No | No | No | Higher bacterial load | ||||||||||
| DPB | PLGA + Vancomycin | In vitro | - | - | - | - | Along 30 days | - | - | Antibacterial effect sustained for 28 days | - | |||
| PLGA | No antibacterial effect | |||||||||||||
| None | No antibacterial effect | |||||||||||||
| [91] | Cylindrical Implantable matrice | PLLA (NPC) + Ciprofloxacin | In vivo | Femur | No | No | No | No | 40 days | No | No | - | No signs of infection | PLLA based CPX-IMs with porous surface are compatible with surrounding bone and muscle tissues and can sustain adequate antibiotic concentrations within defected area, preventing infection. Nevertheless, CPX-IMs of larger pore size showed more successful osteointegration than the smaller pore sized. |
| PLLA/NaCl40% (SPC) + Ciprofloxacin | Partilally | 30–40% of surface area | ||||||||||||
| PLLA/NaCl40% (LPC) + Ciprofloxacin | Mostly | 60–70% of surface area. | ||||||||||||
| Ciprofloxacin | In vitro | - | S. aureus, Bacillus subtilis, Micrococcus luteus, E. coli, P. aeruginosa. | - | Yes | - | Along 40 days | Partially | - | Strong activity within the first 4 days, with similar results and no diminution during the follow-up period from day 1 until 40. | - | |||
| PLLA (NPC) + Ciprofloxacin | ||||||||||||||
| PLLA/NaCl40% (SPC) + Ciprofloxacin | ||||||||||||||
| PLLA/NaCl40% (LPC) + Ciprofloxacin | ||||||||||||||
| [68] | Nail | UMAO-phytic acid-Cu-0 | In vivo | Mandible | No | No | No | No | 2 weeks | In between | No | - | - | The introduction of Cu2+ in the copper plating coating effectively inhibited the growth and propagation of the bacteria, and the antibacterial rate was proportional to the Cu content. (However, the coating Cu-5 inhibited cell growth in vitro and was not evaluated in vivo.) Finally, UMAO-phytic acid-Cu 3min implants slow down the in vivo corrosion rate, promote antimicrobial activity and bone growth. |
| 4 weeks | Partially | |||||||||||||
| 6 weeks | Yes | |||||||||||||
| UMAO-phytic acid-Cu-3 | 2 weeks | Lower | No | |||||||||||
| 4 weeks | Yes | |||||||||||||
| 6 weeks | Yes | |||||||||||||
| UMAO-phytic acid | 2 weeks | Higher | No | |||||||||||
| 4 weeks | Partially | |||||||||||||
| 6 weeks | Yes, but… (desorganized bone structure) | |||||||||||||
| UMAO-phytic acid | In vitro | - | S.aureus (ATCC 6538)E. coli (ATCC 25922) | - | Yes | - | 24 h | - | - | No antibacterial activity | - | |||
| UMAO-phytic acid-Cu-0 | Low antimicrobial activity | |||||||||||||
| UMAO-phytic acid-Cu-1 | Antibacterial rate ~50% | |||||||||||||
| UMAO-phytic acid-Cu-3 | Antibacterial rate >90% | |||||||||||||
| UMAO-phytic acid-Cu-5 | Antibacterial rate >90% | |||||||||||||
| [80] | Disc | CaP | In vivo | Skull | - | No | No | - | 8 weeks | Partially | Yes | - | - | The Se-CaP coating showed antimicrobial and bone-forming properties. The release of soluble HSe− ions from the Se nanoparticles strongly inhibited biofilm formation of S. aureus. |
| Se-CaP | Partially | Higher | ||||||||||||
| CaP | In vitro | - | S. aureus (ATCC 29213) | - | Yes | - | 48 h | - | Extensive biofilm formation | - | ||||
| Se-CaP | - | No bacteria growth | ||||||||||||
| [84] | None | - | In vivo | Radius middle shaft | MRSA | Yes | Prior to implantation (10 days) | No | 4,8 & 12 weeks | - | No | - | - | The AHRG scaffolds effectively eliminated infection and inhibited biofilm formation. The scaffolds antibacterial capacity improved as the AgNP loading increased, becoming the strongest when 4% was reached. |
| Scaffold | None | 4,8 & 12 weeks | Low | |||||||||||
| 4% AgNP | 4,8 & 12 weeks | Yes | ||||||||||||
| 1%/2%/4%/8% AgNP | In vitro | - | MRSA | - | Yes | - | 24 h | - | Excellent antibacterial performance for the 4% and 8% AHRG scaffolds. | - | ||||
| [76] | Rod | None | In vivo | Femoral condyle | - | No | No | Penicillin postop | 4, 8 &12 weeks | - | No | - | - | HA coated AZ91 loaded with PSI effectively inhibited S. aureus growth while promoting the repair of bone function. The HA coating reduced the Mg allow corrosion; antimicrobial peptide incorporated into HA crystals had its activity retained. |
| HA + PSI10 | 4, 8 & 12 weeks | Yes | ||||||||||||
| HA | 4, 8 & 12 weeks | To some extent | ||||||||||||
| HA | In vitro | - | S. aureus (ATCC 25923) | - | Yes | - | Along 1 week | - | - | Lower antibacterial efficiency | - | |||
| PSI10 | In between | |||||||||||||
| HA + PSI10 | Higher and retained antibacterial efficiency | |||||||||||||
| HA | In vitro | - | - | - | - | - | Along 2 weeks | HA-coated Mg alloy showed lower degradation rate than bare Mg alloy | - | - | - | |||
| None |
3.3. Implant Antibacterial Properties, Biodegradability, Osteointegration: In Vitro and In Vivo Studies
3.3.1. Microbiology Analysis
3.3.2. Bioabsorption and Biodegradability
3.3.3. Osteointegration
3.4. Biodegradable vs. Non-Biodegradable: Comparative In Vitro and In Vivo Studies
3.4.1. Microbiology Analysis
3.4.2. Bioabsorption and Biodegradability
3.4.3. Osteointegration
3.5. Risk of Bias Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Lew, D.P.; Waldvogel, F.A. Osteomyelitis. Lancet 2004, 364, 369–379. [Google Scholar] [CrossRef]
- Kavanagh, N.; Ryan, E.J.; Widaa, A.; Sexton, G.; Fennell, J.; O’Rourke, S.; Cahill, K.C.; Kearney, C.J.; O’Brien, F.J.; Kerrigan, S.W. Staphylococcal Osteomyelitis: Disease Progression, Treatment Challenges, and Future Directions. Clin. Microbiol. Rev. 2018, 31, e00084-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richards, J.E.; Kauffmann, R.M.; Obremskey, W.T.; May, A.K. Stress-induced hyperglycemia as a risk factor for surgical-site infection in nondiabetic orthopedic trauma patients admitted to the intensive care unit. J. Orthop. Trauma 2013, 27, 16–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patzakis, M.J.; Wilkins, J. Factors influencing infection rate in open fracture wounds. Clin. Orthop. Relat. Res. 1989, 36–40. [Google Scholar] [CrossRef]
- Metsemakers, W.J.; Onsea, J.; Neutjens, E.; Steffens, E.; Schuermans, A.; McNally, M.; Nijs, S. Prevention of fracture-related infection: A multidisciplinary care package. Int. Orthop. 2017, 41, 2457–2469. [Google Scholar] [CrossRef] [Green Version]
- Metsemakers, W.J.; Kuehl, R.; Moriarty, T.F.; Richards, R.G.; Verhofstad, M.H.J.; Borens, O.; Kates, S.; Morgenstern, M. Infection after fracture fixation: Current surgical and microbiological concepts. Injury 2018, 49, 511–522. [Google Scholar] [CrossRef] [Green Version]
- Kortram, K.; Bezstarosti, H.; Metsemakers, W.J.; Raschke, M.J.; Van Lieshout, E.M.M.; Verhofstad, M.H.J. Risk factors for infectious complications after open fractures; a systematic review and meta-analysis. Int. Orthop. 2017, 41, 1965–1982. [Google Scholar] [CrossRef] [Green Version]
- Zalavras, C.G. Prevention of Infection in Open Fractures. Infect. Dis. Clin. N. Am. 2017, 31, 339–352. [Google Scholar] [CrossRef]
- Gustilo, R.B.; Gruninger, R.P.; Davis, T. Classification of type III (severe) open fractures relative to treatment and results. Orthopedics 1987, 10, 1781–1788. [Google Scholar]
- Yim, G.H.; Hardwicke, J.T. The Evolution and Interpretation of the Gustilo and Anderson Classification. J. Bone Joint Surg. Am. 2018, 100, e152. [Google Scholar] [CrossRef]
- Puetzler, J.; Zalavras, C.; Moriarty, T.F.; Verhofstad, M.H.J.; Kates, S.L.; Raschke, M.J.; Rosslenbroich, S.; Metsemakers, W.J. Clinical practice in prevention of fracture-related infection: An international survey among 1197 orthopaedic trauma surgeons. Injury 2019, 50, 1208–1215. [Google Scholar] [CrossRef]
- Jansen, B.; Peters, G. Foreign body associated infection. J. Antimicrob. Chemother. 1993, 32 (Suppl. A), 69–75. [Google Scholar] [CrossRef]
- Wolcott, R.D.; Ehrlich, G.D. Biofilms and chronic infections. JAMA 2008, 299, 2682–2684. [Google Scholar] [CrossRef]
- Hedrick, T.L.; Adams, J.D.; Sawyer, R.G. Implant-associated infections: An overview. J. Long-Term Eff. Med. Implants 2006, 16, 83–99. [Google Scholar] [CrossRef]
- Ryder, M.A. Catheter-related infections: It’s all about biofilm. Top. Adv. Pract. Nurs. eJ. 2005, 5, 1–6. [Google Scholar]
- Cook, G.E.; Markel, D.C.; Ren, W.; Webb, L.X.; McKee, M.D.; Schemitsch, E.H. Infection in Orthopaedics. J. Orthop. Trauma 2015, 29 (Suppl. 12), S19–S23. [Google Scholar] [CrossRef]
- Flemming, H.C.; Wingender, J.; Szewzyk, U.; Steinberg, P.; Rice, S.A.; Kjelleberg, S. Biofilms: An emergent form of bacterial life. Nat. Rev. Microbiol. 2016, 14, 563–575. [Google Scholar] [CrossRef]
- Dudareva, M.; Hotchen, A.J.; Ferguson, J.; Hodgson, S.; Scarborough, M.; Atkins, B.L.; McNally, M.A. The microbiology of chronic osteomyelitis: Changes over ten years. J. Infect. 2019, 79, 189–198. [Google Scholar] [CrossRef]
- Ma, X.; Han, S.; Ma, J.; Chen, X.; Bai, W.; Yan, W.; Wang, K. Epidemiology, microbiology and therapeutic consequences of chronic osteomyelitis in northern China: A retrospective analysis of 255 Patients. Sci. Rep. 2018, 8, 14895. [Google Scholar] [CrossRef] [Green Version]
- Kuehl, R.; Tschudin-Sutter, S.; Morgenstern, M.; Dangel, M.; Egli, A.; Nowakowski, A.; Suhm, N.; Theilacker, C.; Widmer, A.F. Time-dependent differences in management and microbiology of orthopaedic internal fixation-associated infections: An observational prospective study with 229 patients. Clin. Microbiol. Infect. 2019, 25, 76–81. [Google Scholar] [CrossRef] [Green Version]
- Chambers, H.F.; Deleo, F.R. Waves of resistance: Staphylococcus aureus in the antibiotic era. Nat. Rev. Microbiol. 2009, 7, 629–641. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Song, G.; Sun, M.; Wang, J.; Wang, Y. Prevalence and Therapies of Antibiotic-Resistance in Staphylococcus aureus. Front. Cell. Infect. Microbiol. 2020, 10, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teterycz, D.; Ferry, T.; Lew, D.; Stern, R.; Assal, M.; Hoffmeyer, P.; Bernard, L.; Uçkay, I. Outcome of orthopedic implant infections due to different staphylococci. Int. J. Infect. Dis. 2010, 14, e913–e918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, O.H.; Bae, I.G.; Moon, S.M.; Park, S.Y.; Kwak, Y.G.; Kim, B.N.; Yu, S.N.; Jeon, M.H.; Kim, T.; Choo, E.J.; et al. Therapeutic outcome of spinal implant infections caused by Staphylococcus aureus: A retrospective observational study. Medicine 2018, 97, e12629. [Google Scholar] [CrossRef]
- Van Hengel, I.A.J.; Tierolf, M.; Fratila-Apachitei, L.E.; Apachitei, I.; Zadpoor, A.A. Antibacterial Titanium Implants Biofunctionalized by Plasma Electrolytic Oxidation with Silver, Zinc, and Copper: A Systematic Review. Int. J. Mol. Sci. 2021, 22, 3800. [Google Scholar] [CrossRef]
- Tande, A.J.; Patel, R. Prosthetic joint infection. Clin. Microbiol. Rev. 2014, 27, 302–345. [Google Scholar] [CrossRef] [Green Version]
- Tøttrup, M.; Bue, M.; Koch, J.; Jensen, L.K.; Hanberg, P.; Aalbæk, B.; Fuursted, K.; Jensen, H.E.; Søballe, K. Effects of Implant-Associated Osteomyelitis on Cefuroxime Bone Pharmacokinetics: Assessment in a Porcine Model. J. Bone Joint Surg. Am. 2016, 98, 363–369. [Google Scholar] [CrossRef]
- Emslie, K.R.; Fenner, L.M.; Nade, S.M. Acute haematogenous osteomyelitis: II. The effect of a metaphyseal abscess on the surrounding blood supply. J. Pathol. 1984, 142, 129–134. [Google Scholar] [CrossRef]
- Liu, L.; Webster, T.J. Nanotechnology for reducing orthopedic implant infections: Synthesis, characterization, and properties. In Orthopedic Biomaterials; Springer: Cham, Switzerland, 2017; pp. 31–62. [Google Scholar]
- Berkes, M.; Obremskey, W.T.; Scannell, B.; Ellington, J.K.; Hymes, R.A.; Bosse, M. Maintenance of hardware after early postoperative infection following fracture internal fixation. J. Bone Jt. Surg. Am. 2010, 92, 823–828. [Google Scholar] [CrossRef]
- Zimmerli, W. Clinical presentation and treatment of orthopaedic implant-associated infection. J. Intern. Med. 2014, 276, 111–119. [Google Scholar] [CrossRef]
- Kapoor, S.K.; Thiyam, R. Management of infection following reconstruction in bone tumors. J. Clin. Orthop. Trauma 2015, 6, 244–251. [Google Scholar] [CrossRef] [Green Version]
- Noimark, S.; Dunnill, C.W.; Wilson, M.; Parkin, I.P. The role of surfaces in catheter-associated infections. Chem. Soc. Rev. 2009, 38, 3435–3448. [Google Scholar] [CrossRef]
- Lerner, R.K.; Esterhai, J.L., Jr.; Polomano, R.C.; Cheatle, M.D.; Heppenstall, R.B. Quality of life assessment of patients with posttraumatic fracture nonunion, chronic refractory osteomyelitis, and lower-extremity amputation. Clin. Orthop. Relat. Res. 1993, 295, 28–36. [Google Scholar] [CrossRef]
- Tribble, D.R.; Conger, N.G.; Fraser, S.; Gleeson, T.D.; Wilkins, K.; Antonille, T.; Weintrob, A.; Ganesan, A.; Gaskins, L.J.; Li, P.; et al. Infection-associated clinical outcomes in hospitalized medical evacuees after traumatic injury: Trauma infectious disease outcome study. J. Trauma 2011, 71, S33–S42. [Google Scholar] [CrossRef] [Green Version]
- Espiritu, J.; Meier, M.; Seitz, J.M. The current performance of biodegradable magnesium-based implants in magnetic resonance imaging: A review. Bioact. Mater. 2021, 6, 4360–4367. [Google Scholar] [CrossRef]
- Grainger, D.W. All charged up about implanted biomaterials. Nat. Biotechnol. 2013, 31, 507–509. [Google Scholar] [CrossRef]
- Saini, M.; Singh, Y.; Arora, P.; Arora, V.; Jain, K. Implant biomaterials: A comprehensive review. World J. Clin. Cases 2015, 3, 52–57. [Google Scholar] [CrossRef]
- Mucha, M.; Tylman, M. Novel technique of polymer composite preparation for bone implants. In Advanced Materials Research; Trans Tech Publications Ltd.: Bäch, Switzerland, 2012; pp. 681–685. [Google Scholar]
- Prasad, A.; Bhasney, S.; Katiyar, V.; Sankar, M.R. Biowastes processed hydroxyapatite filled poly (lactic acid) bio-composite for open reduction internal fixation of small bones. Mater. Today Proc. 2017, 4, 10153–10157. [Google Scholar] [CrossRef]
- Regar, E.; Sianos, G.; Serruys, P.W. Stent development and local drug delivery. Br. Med. Bull. 2001, 59, 227–248. [Google Scholar] [CrossRef] [Green Version]
- Domb, A.J.; Khan, W. Focal Controlled Drug Delivery; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- Scarano, A.; de Oliveira, P.S.; Traini, T.; Lorusso, F. Sinus Membrane Elevation with Heterologous Cortical Lamina: A Randomized Study of a New Surgical Technique for Maxillary Sinus Floor Augmentation without Bone Graft. Materials 2018, 11, 1457. [Google Scholar] [CrossRef] [Green Version]
- Thouas, G. Metallic implant biomaterials. Mater. Sci. Eng. R Rep. 2015, 87, 1–57. [Google Scholar]
- Gotman, I. Characteristics of metals used in implants. J. Endourol. 1997, 11, 383–389. [Google Scholar] [CrossRef]
- Prasad, A. Bioabsorbable polymeric materials for biofilms and other biomedical applications: Recent and future trends. Mater. Today Proc. 2021, 44, 2447–2453. [Google Scholar] [CrossRef]
- Ibrahim, A.M.; Koolen, P.G.; Kim, K.; Perrone, G.S.; Kaplan, D.L.; Lin, S.J. Absorbable biologically based internal fixation. Clin. Podiatr. Med. Surg. 2015, 32, 61–72. [Google Scholar] [CrossRef]
- Teo, A.J.; Mishra, A.; Park, I.; Kim, Y.-J.; Park, W.-T.; Yoon, Y.-J. Polymeric biomaterials for medical implants and devices. ACS Biomater. Sci. Eng. 2016, 2, 454–472. [Google Scholar] [CrossRef]
- Adeosun, S.O.; Lawal, G.I.; Gbenebor, O.P. Characteristics of Biodegradable Implants; University of Lagos: Lagos, Nigeria, 2014. [Google Scholar]
- Gogolewski, S. Bioresorbable polymers in trauma and bone surgery. Injury 2000, 31, D28–D32. [Google Scholar] [CrossRef]
- Eberli, D. Tissue Engineering; BoD—Books on Demand: Norderstedt, Germany, 2010. [Google Scholar]
- Andreiotelli, M.; Wenz, H.J.; Kohal, R.J. Are ceramic implants a viable alternative to titanium implants? A systematic literature review. Clin. Oral Implant. Res. 2009, 20, 32–47. [Google Scholar] [CrossRef]
- Al-Sanabani, J.S.; Madfa, A.A.; Al-Sanabani, F.A. Application of calcium phosphate materials in dentistry. Int. J. Biomater. 2013, 2013, 876132. [Google Scholar] [CrossRef] [Green Version]
- Anderson, J.M.; Rodriguez, A.; Chang, D.T. Foreign body reaction to biomaterials. In Seminars in Immunology; Academic Press: Cambridge, MA, USA, 2008; pp. 86–100. [Google Scholar]
- Von Eiff, C.; Jansen, B.; Kohnen, W.; Becker, K. Infections associated with medical devices. Drugs 2005, 65, 179–214. [Google Scholar] [CrossRef]
- Klevens, R.M.; Edwards, J.R.; Richards, C.L., Jr.; Horan, T.C.; Gaynes, R.P.; Pollock, D.A.; Cardo, D.M. Estimating health care-associated infections and deaths in US hospitals, 2002. Public Health Rep. 2007, 122, 160–166. [Google Scholar] [CrossRef]
- Inzana, J.A.; Schwarz, E.M.; Kates, S.L.; Awad, H.A. Biomaterials approaches to treating implant-associated osteomyelitis. Biomaterials 2016, 81, 58–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, R.R.; Mooney, D.J. Polymeric growth factor delivery strategies for tissue engineering. Pharm. Res. 2003, 20, 1103–1112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Nihouannen, D.; Hacking, S.A.; Gbureck, U.; Komarova, S.V.; Barralet, J.E. The use of RANKL-coated brushite cement to stimulate bone remodelling. Biomaterials 2008, 29, 3253–3259. [Google Scholar] [CrossRef] [PubMed]
- Nyska, A.; Schiffenbauer, Y.S.; Brami, C.T.; Maronpot, R.R.; Ramot, Y. Histopathology of biodegradable polymers: Challenges in interpretation and the use of a novel compact MRI for biocompatibility evaluation. Polym. Adv. Technol. 2014, 25, 461–467. [Google Scholar] [CrossRef]
- Ramot, Y.; Haim-Zada, M.; Domb, A.J.; Nyska, A. Biocompatibility and safety of PLA and its copolymers. Adv. Drug Deliv. Rev. 2016, 107, 153–162. [Google Scholar] [CrossRef]
- Ramot, Y.; Nyska, A.; Markovitz, E.; Dekel, A.; Klaiman, G.; Zada, M.H.; Domb, A.J.; Maronpot, R.R. Long-term local and systemic safety of poly (l-lactide-co-epsilon-caprolactone) after subcutaneous and intra-articular implantation in rats. Toxicol. Pathol. 2015, 43, 1127–1140. [Google Scholar] [CrossRef] [Green Version]
- Ramot, Y.; Touitou, D.; Levin, G.; Ickowicz, D.E.; Zada, M.H.; Abbas, R.; Yankelson, L.; Domb, A.J.; Nyska, A. Interspecies differences in reaction to a biodegradable subcutaneous tissue filler: Severe inflammatory granulomatous reaction in the Sinclair minipig. Toxicol. Pathol. 2015, 43, 267–271. [Google Scholar] [CrossRef]
- Rousselle, S.D.; Ramot, Y.; Nyska, A.; Jackson, N.D. Pathology of bioabsorbable implants in preclinical studies. Toxicol. Pathol. 2019, 47, 358–378. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Song, J.; Jin, P.; Li, M.; Liu, J.; Wu, D.; Yao, H.; Wang, J. Antibacterial properties and biocompatibility in vivo and vitro of composite coating of pure magnesium ultrasonic micro-arc oxidation phytic acid copper loaded. J. Mater. Sci. Mater. Med. 2019, 30, 49. [Google Scholar] [CrossRef]
- Li, Y.; Liu, L.; Wan, P.; Zhai, Z.; Mao, Z.; Ouyang, Z.; Yu, D.; Sun, Q.; Tan, L.; Ren, L.; et al. Biodegradable Mg-Cu alloy implants with antibacterial activity for the treatment of osteomyelitis: In vitro and in vivo evaluations. Biomaterials 2016, 106, 250–263. [Google Scholar] [CrossRef]
- Qu, X.; Yang, H.; Jia, B.; Wang, M.; Yue, B.; Zheng, Y.; Dai, K. Zinc alloy-based bone internal fixation screw with antibacterial and anti-osteolytic properties. Bioact. Mater. 2021, 6, 4607–4624. [Google Scholar] [CrossRef]
- Dumlao, P.I.E.; Paner, N.; Bathan, L.; Lim, B.A. Delayed onset bioabsorbable screw reaction, intact screw extrusion and Pseudomonas aeruginosa tibial tunnel osteomyelitis years after arthroscopic anterior cruciate ligament reconstruction using hamstring graft. BMJ Case Rep. 2019, 12, e229927. [Google Scholar] [CrossRef]
- May, H.; Alper Kati, Y.; Gumussuyu, G.; Yunus Emre, T.; Unal, M.; Kose, O. Bioabsorbable magnesium screw versus conventional titanium screw fixation for medial malleolar fractures. J. Orthop. Traumatol. 2020, 21, 9. [Google Scholar] [CrossRef]
- Brooks, E.K.; Ahn, R.; Tobias, M.E.; Hansen, L.A.; Luke-Marshall, N.R.; Wild, L.; Campagnari, A.A.; Ehrensberger, M.T. Magnesium alloy AZ91 exhibits antimicrobial properties in vitro but not in vivo. J. Biomed. Mater. Res. B Appl. Biomater. 2018, 106, 221–227. [Google Scholar] [CrossRef]
- Gao, Z.; Song, M.; Liu, R.L.; Shen, Y.; Ward, L.; Cole, I.; Chen, X.B.; Liu, X. Improving in vitro and in vivo antibacterial functionality of Mg alloys through micro-alloying with Sr and Ga. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 104, 109926. [Google Scholar] [CrossRef]
- Qu, X.; Yang, H.; Jia, B.; Yu, Z.; Zheng, Y.; Dai, K. Biodegradable Zn-Cu alloys show antibacterial activity against MRSA bone infection by inhibiting pathogen adhesion and biofilm formation. Acta Biomater. 2020, 117, 400–417. [Google Scholar] [CrossRef]
- Tian, J.; Shen, S.; Zhou, C.; Dang, X.; Jiao, Y.; Li, L.; Ding, S.; Li, H. Investigation of the antimicrobial activity and biocompatibility of magnesium alloy coated with HA and antimicrobial peptide. J. Mater. Sci. Mater. Med. 2015, 26, 66. [Google Scholar] [CrossRef]
- Zhao, W.; Wang, J.; Weiyang, J.; Qiao, B.; Wang, Y.; Li, Y.; Jiang, D. A novel biodegradable Mg-1Zn-0.5 Sn alloy: Mechanical properties, corrosion behavior, biocompatibility, and antibacterial activity. J. Magnes. Alloy. 2020, 8, 374–386. [Google Scholar] [CrossRef]
- Yu, W.; Chen, D.; Ding, Z.; Qiu, M.; Zhang, Z.; Shen, J.; Zhang, X.; Zhang, S.; He, Y.; Shi, Z. Synergistic effect of a biodegradable Mg–Zn alloy on osteogenic activity and anti-biofilm ability: An in vitro and in vivo study. RSC Adv. 2016, 6, 45219–45230. [Google Scholar] [CrossRef]
- Shishatskaya, E.I.; Kamendov, I.V.; Starosvetsky, S.I.; Vinnik, Y.S.; Markelova, N.N.; Shageev, A.A.; Khorzhevsky, V.A.; Peryanova, O.V.; Shumilova, A.A. An in vivo study of osteoplastic properties of resorbable poly-3-hydroxybutyrate in models of segmental osteotomy and chronic osteomyelitis. Artif. Cells Nanomed. Biotechnol. 2014, 42, 344–355. [Google Scholar] [CrossRef] [PubMed]
- Vaquette, C.; Bock, N.; Tran, P.A. Layered Antimicrobial Selenium Nanoparticle-Calcium Phosphate Coating on 3D Printed Scaffolds Enhanced Bone Formation in Critical Size Defects. ACS Appl. Mater. Interfaces 2020, 12, 55638–55648. [Google Scholar] [CrossRef] [PubMed]
- McLaren, J.S.; White, L.J.; Cox, H.C.; Ashraf, W.; Rahman, C.V.; Blunn, G.W.; Goodship, A.E.; Quirk, R.A.; Shakesheff, K.M.; Bayston, R.; et al. A biodegradable antibiotic-impregnated scaffold to prevent osteomyelitis in a contaminated in vivo bone defect model. Eur. Cell. Mater. 2014, 27, 332–349. [Google Scholar] [CrossRef]
- Gao, J.; Huang, G.; Liu, G.; Liu, Y.; Chen, Q.; Ren, L.; Chen, C.; Ding, Z. A biodegradable antibiotic-eluting PLGA nanofiber-loaded deproteinized bone for treatment of infected rabbit bone defects. J. Biomater. Appl. 2016, 31, 241–249. [Google Scholar] [CrossRef]
- Krishnan, A.G.; Biswas, R.; Menon, D.; Nair, M.B. Biodegradable nanocomposite fibrous scaffold mediated local delivery of vancomycin for the treatment of MRSA infected experimental osteomyelitis. Biomater. Sci. 2020, 8, 2653–2665. [Google Scholar] [CrossRef]
- Weng, W.; Li, X.; Nie, W.; Liu, H.; Liu, S.; Huang, J.; Zhou, Q.; He, J.; Su, J.; Dong, Z.; et al. One-Step Preparation of an AgNP-nHA@RGO Three-Dimensional Porous Scaffold and Its Application in Infected Bone Defect Treatment. Int. J. Nanomed. 2020, 15, 5027–5042. [Google Scholar] [CrossRef]
- Beenken, K.E.; Campbell, M.J.; Ramirez, A.M.; Alghazali, K.; Walker, C.M.; Jackson, B.; Griffin, C.; King, W.; Bourdo, S.E.; Rifkin, R.; et al. Evaluation of a bone filler scaffold for local antibiotic delivery to prevent Staphylococcus aureus infection in a contaminated bone defect. Sci. Rep. 2021, 11, 10254. [Google Scholar] [CrossRef]
- Zhang, D.; Liu, W.; Wu, X.D.; He, X.; Lin, X.; Wang, H.; Li, J.; Jiang, J.; Huang, W. Efficacy of novel nano-hydroxyapatite/polyurethane composite scaffolds with silver phosphate particles in chronic osteomyelitis. J. Mater. Sci. Mater. Med. 2019, 30, 59. [Google Scholar] [CrossRef]
- Wang, Q.; Chen, C.; Liu, W.; He, X.; Zhou, N.; Zhang, D.; Gu, H.; Li, J.; Jiang, J.; Huang, W. Levofloxacin loaded mesoporous silica microspheres/nano-hydroxyapatite/polyurethane composite scaffold for the treatment of chronic osteomyelitis with bone defects. Sci. Rep. 2017, 7, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Xie, K.; Wang, N.; Guo, Y.; Zhao, S.; Tan, J.; Wang, L.; Li, G.; Wu, J.; Yang, Y.; Xu, W.; et al. Additively manufactured biodegradable porous magnesium implants for elimination of implant-related infections: An in vitro and in vivo study. Bioact. Mater. 2022, 8, 140–152. [Google Scholar] [CrossRef]
- Cao, Z.; Jiang, D.; Yan, L.; Wu, J. In vitro and in vivo osteogenic activity of the novel vancomycin-loaded bone-like hydroxyapatite/poly(amino acid) scaffold. J Biomater. Appl. 2016, 30, 1566–1577. [Google Scholar] [CrossRef]
- Ferreira, M.; Rzhepishevska, O.; Grenho, L.; Malheiros, D.; Gonçalves, L.; Almeida, A.J.; Jordão, L.; Ribeiro, I.A.; Ramstedt, M.; Gomes, P.; et al. Levofloxacin-loaded bone cement delivery system: Highly effective against intracellular bacteria and Staphylococcus aureus biofilms. Int. J. Pharm. 2017, 532, 241–248. [Google Scholar] [CrossRef]
- Hanafy, A.F.; Ali, H.S.M.; El Achy, S.N.; Habib, E.E. Dual effect biodegradable ciprofloxacin loaded implantable matrices for osteomyelitis: Controlled release and osteointegration. Drug Dev. Ind. Pharm. 2018, 44, 1023–1033. [Google Scholar] [CrossRef]
- Taljanovic, M.S.; Jones, M.D.; Ruth, J.T.; Benjamin, J.B.; Sheppard, J.E.; Hunter, T.B. Fracture fixation. Radiographics 2003, 23, 1569–1590. [Google Scholar] [CrossRef]
- Torgersen, S.; Gjerdet, N.R.; Erichsen, E.S.; Bang, G. Metal particles and tissue changes adjacent to miniplates. A retrieval study. Acta Odontol. Scand. 1995, 53, 65–71. [Google Scholar] [CrossRef]
- Kannan, M.B. Hydroxyapatite coating on biodegradable magnesium and magnesium-based alloys. In Hydroxyapatite (HAp) for Biomedical Applications; Mucalo, M., Ed.; Woodhead Publishing: Sawston, UK, 2015; pp. 289–306. [Google Scholar]
- Li, C.; Guo, C.; Fitzpatrick, V.; Ibrahim, A.; Zwierstra, M.J.; Hanna, P.; Lechtig, A.; Nazarian, A.; Lin, S.J.; Kaplan, D.L. Design of biodegradable, implantable devices towards clinical translation. Nat. Rev. Mater. 2020, 5, 61–81. [Google Scholar] [CrossRef]
- Chouirfa, H.; Bouloussa, H.; Migonney, V.; Falentin-Daudré, C. Review of titanium surface modification techniques and coatings for antibacterial applications. Acta Biomater. 2019, 83, 37–54. [Google Scholar] [CrossRef]
- Janbozorgi, M.; Karimi Taheri, K.; Karimi Taheri, A. Microstructural evolution, mechanical properties, and corrosion resistance of a heat-treated Mg alloy for the bio-medical application. J. Magnes. Alloy. 2019, 7, 80–89. [Google Scholar] [CrossRef]
- Xu, G.; Zhang, L.; Liu, L.; Du, Y.; Zhang, F.; Xu, K.; Liu, S.; Tan, M.; Jin, Z. Thermodynamic database of multi-component Mg alloys and its application to solidification and heat treatment. J. Magnes. Alloy. 2016, 4, 249–264. [Google Scholar] [CrossRef] [Green Version]
- Shen, X.; Hu, Y.; Xu, G.; Chen, W.; Xu, K.; Ran, Q.; Ma, P.; Zhang, Y.; Li, J.; Cai, K. Regulation of the biological functions of osteoblasts and bone formation by Zn-incorporated coating on microrough titanium. ACS Appl. Mater. Interfaces 2014, 6, 16426–16440. [Google Scholar] [CrossRef]
- Kozerski, S.; Pawlowski, L.; Jaworski, R.; Roudet, F.; Petit, F. Two zones microstructure of suspension plasma sprayed hydroxyapatite coatings. Surf. Coat. Technol. 2010, 204, 1380–1387. [Google Scholar] [CrossRef]
- Liu, G.Y.; Hu, J.-J.; Ding, Z.K.; Wang, C. Bioactive calcium phosphate coating formed on micro-arc oxidized magnesium by chemical deposition. Appl. Surf. Sci. 2011, 257, 2051–2057. [Google Scholar] [CrossRef]
- Lu, X.; Zhao, Z.; Leng, Y. Biomimetic calcium phosphate coatings on nitric-acid-treated titanium surfaces. Mater. Sci. Eng. C 2007, 27, 700–708. [Google Scholar] [CrossRef]
- Förster, Y.; Rentsch, C.; Schneiders, W.; Bernhardt, R.; Simon, J.C.; Worch, H.; Rammelt, S. Surface modification of implants in long bone. Biomatter 2012, 2, 149–157. [Google Scholar] [CrossRef] [Green Version]
- Zasloff, M. Antimicrobial peptides of multicellular organisms. Nature 2002, 415, 389–395. [Google Scholar] [CrossRef]
- Kazemzadeh-Narbat, M.; Noordin, S.; Masri, B.A.; Garbuz, D.S.; Duncan, C.P.; Hancock, R.E.; Wang, R. Drug release and bone growth studies of antimicrobial peptide-loaded calcium phosphate coating on titanium. J. Biomed. Mater. Res. B Appl. Biomater. 2012, 100, 1344–1352. [Google Scholar] [CrossRef]
- Kazemzadeh-Narbat, M.; Kindrachuk, J.; Duan, K.; Jenssen, H.; Hancock, R.E.; Wang, R. Antimicrobial peptides on calcium phosphate-coated titanium for the prevention of implant-associated infections. Biomaterials 2010, 31, 9519–9526. [Google Scholar] [CrossRef]
- Tran, P.A.; O’Brien-Simpson, N.; Reynolds, E.C.; Pantarat, N.; Biswas, D.P.; O’Connor, A.J. Low cytotoxic trace element selenium nanoparticles and their differential antimicrobial properties against S. aureus and E. coli. Nanotechnology 2016, 27, 045101. [Google Scholar] [CrossRef]
- Samani, S.; Hossainalipour, S.M.; Tamizifar, M.; Rezaie, H.R. In vitro antibacterial evaluation of sol-gel-derived Zn-, Ag-, and (Zn + Ag)-doped hydroxyapatite coatings against methicillin-resistant Staphylococcus aureus. J. Biomed. Mater. Res. A 2013, 101, 222–230. [Google Scholar] [CrossRef]
- Brennan, S.A.; Ní Fhoghlú, C.; Devitt, B.M.; O’Mahony, F.J.; Brabazon, D.; Walsh, A. Silver nanoparticles and their orthopaedic applications. Bone Jt. J. 2015, 97, 582–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gosheger, G.; Hardes, J.; Ahrens, H.; Streitburger, A.; Buerger, H.; Erren, M.; Gunsel, A.; Kemper, F.H.; Winkelmann, W.; Von Eiff, C. Silver-coated megaendoprostheses in a rabbit model—An analysis of the infection rate and toxicological side effects. Biomaterials 2004, 25, 5547–5556. [Google Scholar] [CrossRef] [PubMed]
- Nostro, A.; Cellini, L.; Di Giulio, M.; D’Arrigo, M.; Marino, A.; Blanco, A.R.; Favaloro, A.; Cutroneo, G.; Bisignano, G. Effect of alkaline pH on staphylococcal biofilm formation. APMIS 2012, 120, 733–742. [Google Scholar] [CrossRef] [PubMed]
- Qin, H.; Zhao, Y.; Cheng, M.; Wang, Q.; Wang, Q.; Wang, J.; Jiang, Y.; An, Z.; Zhang, X. Anti-biofilm properties of magnesium metal via alkaline pH. RSC Adv. 2015, 5, 21434–21444. [Google Scholar] [CrossRef]
- Seo, H.-J.; Cho, Y.-E.; Kim, T.; Shin, H.-I.; Kwun, I.-S. Zinc may increase bone formation through stimulating cell proliferation, alkaline phosphatase activity and collagen synthesis in osteoblastic MC3T3-E1 cells. Nutr. Res. Pract. 2010, 4, 356–361. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Ito, A.; Sogo, Y.; Li, X.; Oyane, A. Zinc-containing apatite layers on external fixation rods promoting cell activity. Acta Biomater. 2010, 6, 962–968. [Google Scholar] [CrossRef]
- Yusa, K.; Yamamoto, O.; Fukuda, M.; Koyota, S.; Koizumi, Y.; Sugiyama, T. In vitro prominent bone regeneration by release zinc ion from Zn-modified implant. Biochem. Biophys. Res. Commun. 2011, 412, 273–278. [Google Scholar] [CrossRef]
- Szymański, P.; Frączek, T.; Markowicz, M.; Mikiciuk-Olasik, E. Development of copper based drugs, radiopharmaceuticals and medical materials. Biometals 2012, 25, 1089–1112. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Ren, Z.; Xu, Y.; Pang, S.; Zhao, X.; Zhao, Y. Biodegradable Magnesium Alloys Developed as Bone Repair Materials: A Review. Scanning 2018, 2018, 9216314. [Google Scholar] [CrossRef] [Green Version]
- Nabiyouni, M.; Brückner, T.; Zhou, H.; Gbureck, U.; Bhaduri, S.B. Magnesium-based bioceramics in orthopedic applications. Acta Biomater. 2018, 66, 23–43. [Google Scholar] [CrossRef]
- Ciccone, W.J., 2nd; Motz, C.; Bentley, C.; Tasto, J.P. Bioabsorbable implants in orthopaedics: New developments and clinical applications. J. Am. Acad. Orthop. Surg. 2001, 9, 280–288. [Google Scholar] [CrossRef] [Green Version]
- Danna, N.R.M.D.; Leucht, P.M.D. Designing Resorbable Scaffolds for Bone Defects. Bull. NYU Hosp. Jt. Dis. 2019, 77, 39–44. [Google Scholar]
- Smith, L.L.; Niziolek, P.J.; Haberstroh, K.M.; Nauman, E.A.; Webster, T.J. Decreased fibroblast and increased osteoblast adhesion on nanostructured NaOH-etched PLGA scaffolds. Int. J. Nanomed. 2007, 2, 383–388. [Google Scholar]
| Ref. # | Implant Type (Scaffold, Screw, …) | Study Design/Type of Study | Surgical Site | Microorg. | Previous Infection | Inoculation/ Seeding of Microorganisms | Prophylatic Antimicrobial Admin. | Sacrifice Timepoint/Follow-Up Time After Surgery | Infection | Bioabsortion/ Biodegradability | Osteointegration | Main Outcome | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Microbiol. Analysis | Histological Analysis | Imagiology (Radiographic, ect…) | Histological Analysis | Imagiology (Radiographic, ect…) | Histological Analysis | Imagiology (Radiographic, ect…) | ||||||||||
| [79] | P3HB pellets | In vivo | Tibia metaphysis | S. aureus | Yes | Prior to surgery (1 month) | Chlorhexidine [##] | 15 days | - | - | - | - | - | - | - | P3HB/HA and P3HB led to quicker suppression of infection and recovery of the support ability of the affected limb than Bio-Oss®. However, P3HB/HA composite implants showed inferior biomechanical properties than P3HB since cortical bone had large lacunae and was rather loosely structured. P3HB-based materials showed pronounced osteoplastic properties and slow degradation in vivo, enabling normal reparative osteogenesis. |
| 30 days | S. aureus (44.1%) and associations of Gram-positive and Gram-negative anaerobic microorganisms and E. coli (55.9%) | - | - | Partially | - | Partially | - | |||||||||
| 60 days | - | - | - | - | - | Yes | ||||||||||
| 90 days | No bacteria | - | - | Yes (low rate) | - | Yes | Yes | |||||||||
| 120 days | - | - | - | - | - | - | Yes | |||||||||
| P3HB/HA pellets + Tienam | 15 days | - | - | - | - | - | - | - | ||||||||
| 30 days | No bacteria | - | - | Partially (lower rate) | - | Partially | - | |||||||||
| 60 days | - | - | - | - | - | Yes | ||||||||||
| 90 days | No bacteria | - | - | Mostly | - | Yes | Yes | |||||||||
| 120 days | - | - | - | - | - | - | Yes | |||||||||
| Bio-Oss® (control) | 15 days | - | - | - | - | - | - | - | ||||||||
| 30 days | S. aureus (48.2%) and associations of Gram-positive and Gram-negative anaerobic microorganisms and E. coli | - | - | - | - | - | - | |||||||||
| 60 days | - | - | - | - | - | - | - | |||||||||
| 90 days | S. aureus (48.2%) and associations of Gram-positive and Gram-negative anaerobic microorganisms and E. coli | - | - | - | - | No | No | |||||||||
| 120 days | - | - | - | - | - | No | ||||||||||
| [73] | AZ91 rod | In vivo | Humeral head | A. baumannii (Ab307-0294) | Yes | Just before implantation | No | 7 days | No antimicrobial effect | - | - | - | Partially * | - | - | AZ91 did not produce antimicrobial effects. |
| c.p. Ti rod (control) | No antimicrobial effect | - | - | - | No * | - | - | |||||||||
| [74] | Mg-0.1Ga-0.1Sr rod | In vivo | Femur medullary cavity | S. aureus (ATCC 43300) | Yes | Just before implantation | No | 5 days | Few bacterial colonies | - | - | - | Yes (lower)** | Yes | - | Mg alloys outperformed c.p. Ti in inhibiting S. aureus on the rods surface. Such antibacterial activity was improved through addition of micro-content of Ga and Sr (0.1 wt%). |
| Pure Mg rod | Many bacterial colonies | - | - | - | Yes (higher)** | Yes | - | |||||||||
| Mg-0.1Sr rod | Some bacterial colonies | - | - | - | Yes (lower)** | Yes | - | |||||||||
| Mg-0.1Ga rod | Some bacterial colonies | - | - | - | Yes (higher)** | Yes | - | |||||||||
| c.p. Ti rod | Highest number of bacterial colonies | - | - | - | No ** | No | - | |||||||||
| c.p. Ti rod (negative control) | - | No | - | No bacteria | - | - | - | No ** | No | - | ||||||
| None (positive control) | S. aureus (ATCC 43300) | Yes | Just before implantation | - | - | - | - | - | - | - | ||||||
| [72] | Mg screw | Retrospective cohort study | Tibia medial malleolus | - | No | - | - | Mean time of 24.6 ± 10.5 months (12–53 months) | No deep infection | - | - | - | Yes | - | - | Bioabsorbable Mg and titanium screws had similar therapeutic efficacy in MM fracture fixation. There was no implant removal with Mg screws. |
| Ti screw | No deep infection | - | - | - | No | - | - | |||||||||
| [75] | Zn-2Cu cylindric rod | In vivo | Femur medullary cavity | MRSA | Yes | Soaked in implants | No | 3 and 6 weeks | Significantly lesser bacteria were found | Few bacteria | Milder signs | - | - | Yes | - | The Zn-2Cu alloy exerted effective bacterial-killing capability and inhibited the inflammatory and toxic side-effects induced by MRSA bacteria in the rat femur. |
| Ti cylindric rod | Large amounts of bacteria | Large amount of bacteria | Yes | - | - | No | - | |||||||||
| None | - | No | - | - | No | - | - | - | - | |||||||
| [88] | Mg-Nd-Zn-Zr (JDBM BioMg alloy) cylinder | In vivo | Distal femur | MRSA | Yes | - | - | 4 weeks | Small number of bacteria | - | No | - | - | - | - | The JDBM BioMg alloy implant showed antibacterial properties against MRSA, decreasing biofilm formation. |
| Ti cylinder | Large number of bacterial colonies | - | Yes | - | - | - | - | |||||||||
| [69] | Mg0.25Cu intramedullary nail | In vivo | Tibial metaphysis | MRSA | Yes | Prior to surgery (4 weeks) | No | 4 weeks | Almost no bacteria | - | - | - | Partially | Yes | - | The Mg0.25Cu alloy demonstrated antibacterial properties and a therapeutic effect in chronic tibial osteomyelitis. |
| 9 weeks | - | - | - | - | - | - | - | |||||||||
| Ti intramedullary nail | 4 weeks | Multiple bacterial colonies | - | Yes | - | No | No | - | ||||||||
| 9 weeks | - | - | - | - | - | - | - | |||||||||
| [78] | Mg-Zn alloy Kirschner wires | In vivo | Distal femur | MRSA (ATCC 43300) | Yes | Just before implantation | No | 2 weeks | Presence of MRSA | - | - | - | - | - | - | Better bone-implant integration was observed around the Mg-Zn alloy implants compared with Ti in the absence of MRSA. The corrosion product layer deposited on the surface of the Mg-Zn alloy implant retarded the corrosion of the implant, promoting osteointegration. |
| 4 weeks | - | - | - | - | - | - | ||||||||||
| 6 weeks | - | - | - | - | - | - | ||||||||||
| 8 weeks | - | - | - | - | Yes | Yes | ||||||||||
| - | No | - | 2 weeks | No bacteria | - | - | - | - | - | - | ||||||
| 4 weeks | - | - | - | - | - | - | ||||||||||
| 6 weeks | - | - | - | - | - | - | ||||||||||
| 8 weeks | - | - | - | - | Yes | Yes | ||||||||||
| Ti Kirschner wires | MRSA (ATCC 43300) | Yes | Just before implantation | 2 weeks | Presence of MRSA | - | - | - | - | - | - | |||||
| 4 weeks | - | - | - | - | - | - | ||||||||||
| 6 weeks | - | - | - | - | - | - | ||||||||||
| 8 weeks | - | - | - | - | - | No | ||||||||||
| - | No | - | 2 weeks | No bacteria | - | - | - | - | No | - | ||||||
| 4 weeks | - | - | - | - | - | - | ||||||||||
| 6 weeks | - | - | - | - | - | - | ||||||||||
| 8 weeks | - | - | - | - | - | Yes | ||||||||||
| [70] | Zn–2Ag cylindric intramedullary nail | In vivo | Femoral condyles | MRSA | Yes | Soaked in implants | - | 3 and 6 weeks | Very few bacteria in the surrounding bone tissue; no bacteria on the nail surface | Almost completely suppressed | Milder signs | - | - | - | - | Zn–2Ag alloy prevented MRSA infection and no osteomyelitis formation was observed, while promoting osseointegration. |
| c.p. Ti cylindric intramedullary nail | Large number of bacteria on the nail surface and surrounding bone tissue | Yes | Yes | - | - | - | - | |||||||||
| Zn–2Ag screw | Femoral condylar split-fracture | - | No | - | - | 3 months | - | - | - | Yes | - | Yes | Yes | |||
| Ti–6Al–4V screw | - | - | - | - | No | No | ||||||||||
| [77] | Mg-1Zn-0.5Sn rod | In vivo | Femoral condyle | S. aureus (ATCC 25923) [#] E.coli O157 (H7 NTCC 12900) [#] | No | No, Yes [#] | Penicillin postop, No [#] | 1,7 and 14 days | Lowest number of bacterial colonies/smaller colonies [#] | - | - | - | Slower degradation rate *** [#] | - | - | Mg-1Zn-0.5Sn materials exhibited significant antibacterial ability compared to Ti materials. Mg-1Zn-0.5Sn had its degradation rate significantly reduced. |
| Mg-1Zn rod | Low number of bacterial colonies/smaller colonies [#] | - | - | - | - | - | - | |||||||||
| Ti rod [#] | Higher number of bacterial colonies [#] | - | - | - | - | - | - | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paiva, J.C.C.; Oliveira, L.; Vaz, M.F.; Costa-de-Oliveira, S. Biodegradable Bone Implants as a New Hope to Reduce Device-Associated Infections—A Systematic Review. Bioengineering 2022, 9, 409. https://doi.org/10.3390/bioengineering9080409
Paiva JCC, Oliveira L, Vaz MF, Costa-de-Oliveira S. Biodegradable Bone Implants as a New Hope to Reduce Device-Associated Infections—A Systematic Review. Bioengineering. 2022; 9(8):409. https://doi.org/10.3390/bioengineering9080409
Chicago/Turabian StylePaiva, José C. C., Luís Oliveira, Maria Fátima Vaz, and Sofia Costa-de-Oliveira. 2022. "Biodegradable Bone Implants as a New Hope to Reduce Device-Associated Infections—A Systematic Review" Bioengineering 9, no. 8: 409. https://doi.org/10.3390/bioengineering9080409
APA StylePaiva, J. C. C., Oliveira, L., Vaz, M. F., & Costa-de-Oliveira, S. (2022). Biodegradable Bone Implants as a New Hope to Reduce Device-Associated Infections—A Systematic Review. Bioengineering, 9(8), 409. https://doi.org/10.3390/bioengineering9080409