
A Pilot Randomized Controlled Clinical Trial Comparing Piezo Versus Conventional Rotary Surgery for Removal of Impacted Mandibular Third Molars
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Selection
2.3. Surgical Procedure
2.4. Evaluation Parameters
2.4.1. Surgical Difficulty
2.4.2. Postoperative Pain
2.4.3. Swelling
2.4.4. Trismus
2.4.5. Paraesthesia
2.4.6. Operative Bleeding
2.5. Statistical Analysis
3. Results
3.1. Characterization of the Sample According to Age and Gender
3.2. Characterization of the Sample According to the Surgical Difficulty
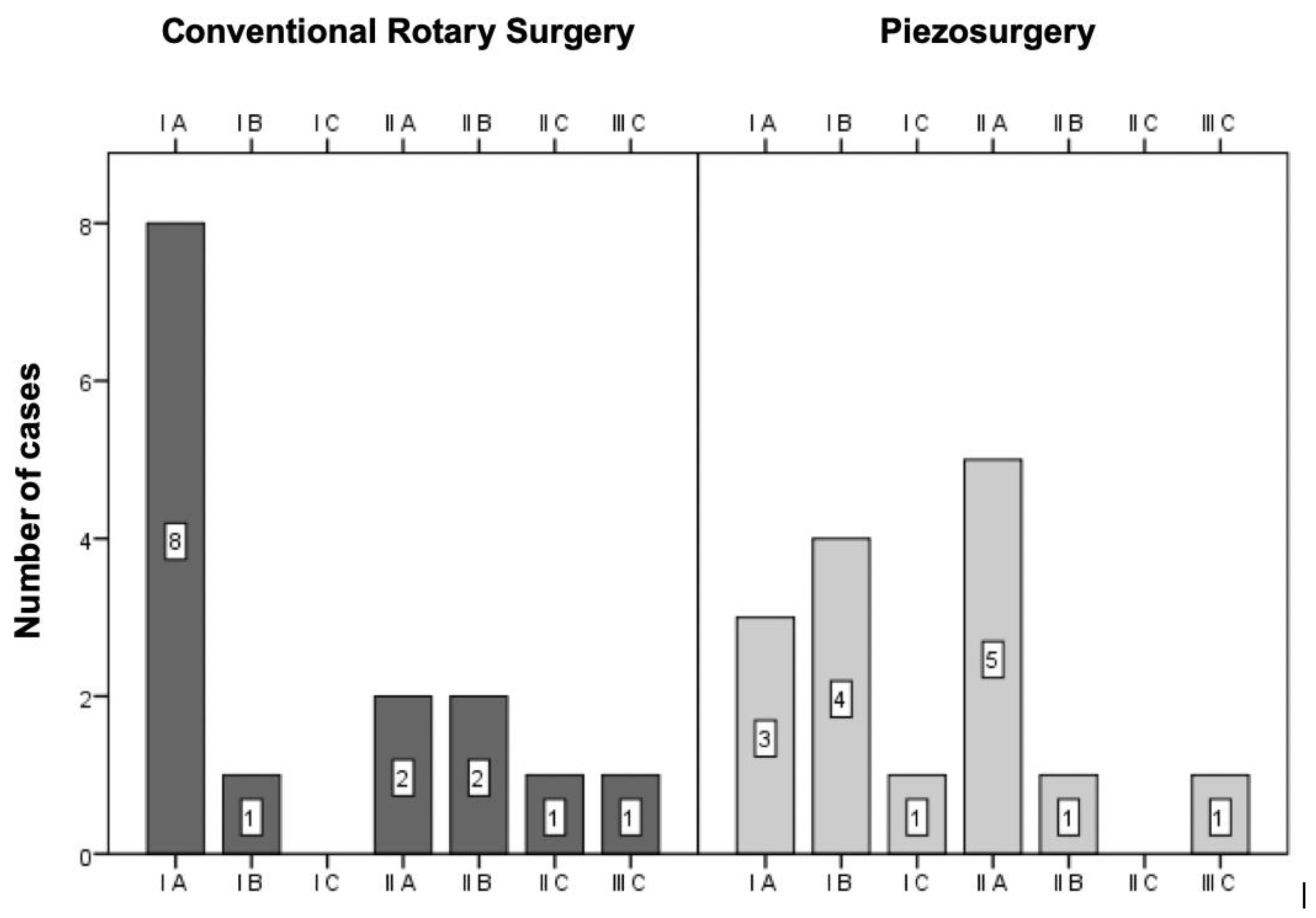
3.2.1. Pell and Gregory Classification
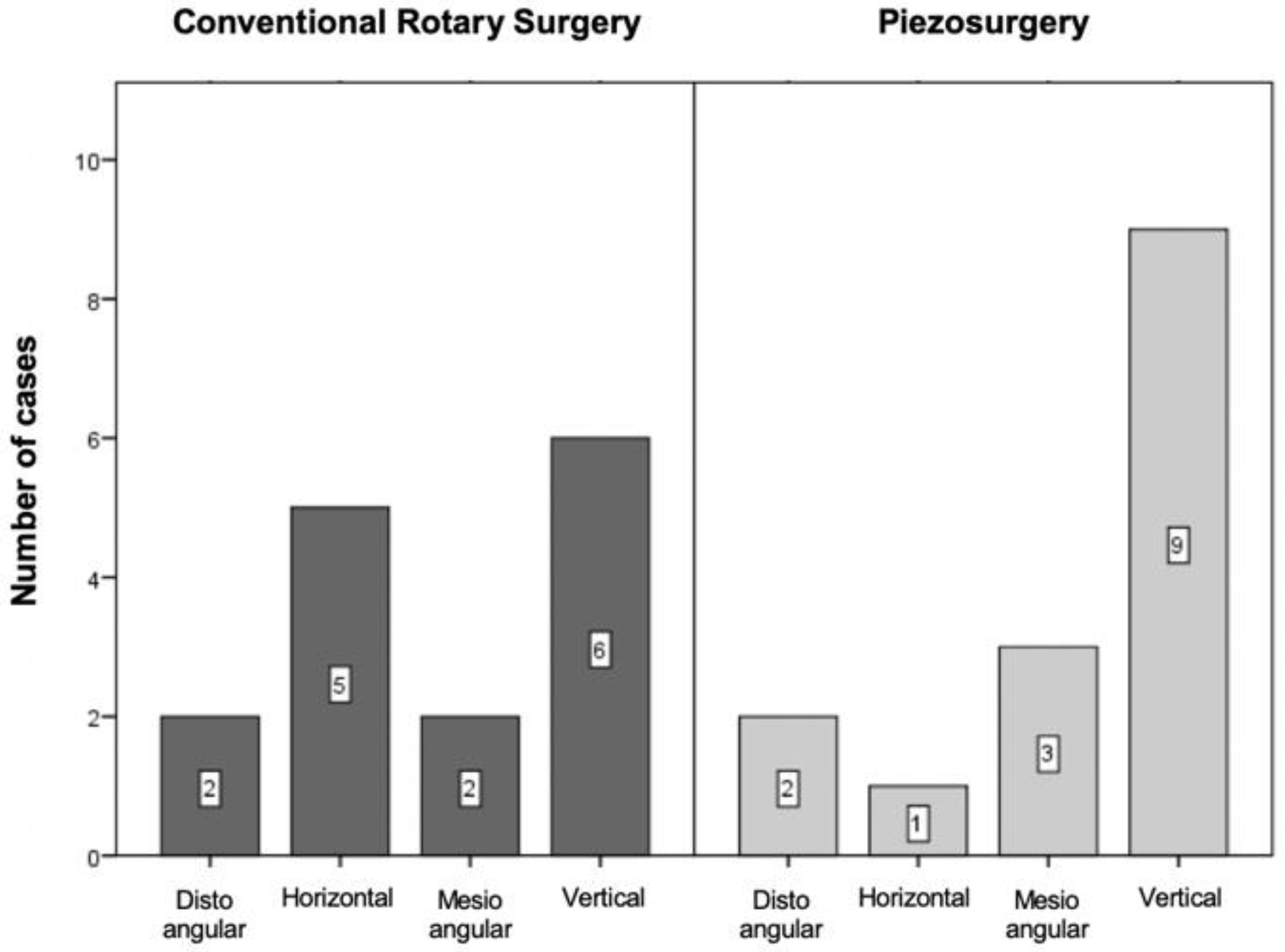
3.2.2. Winter’s Classification
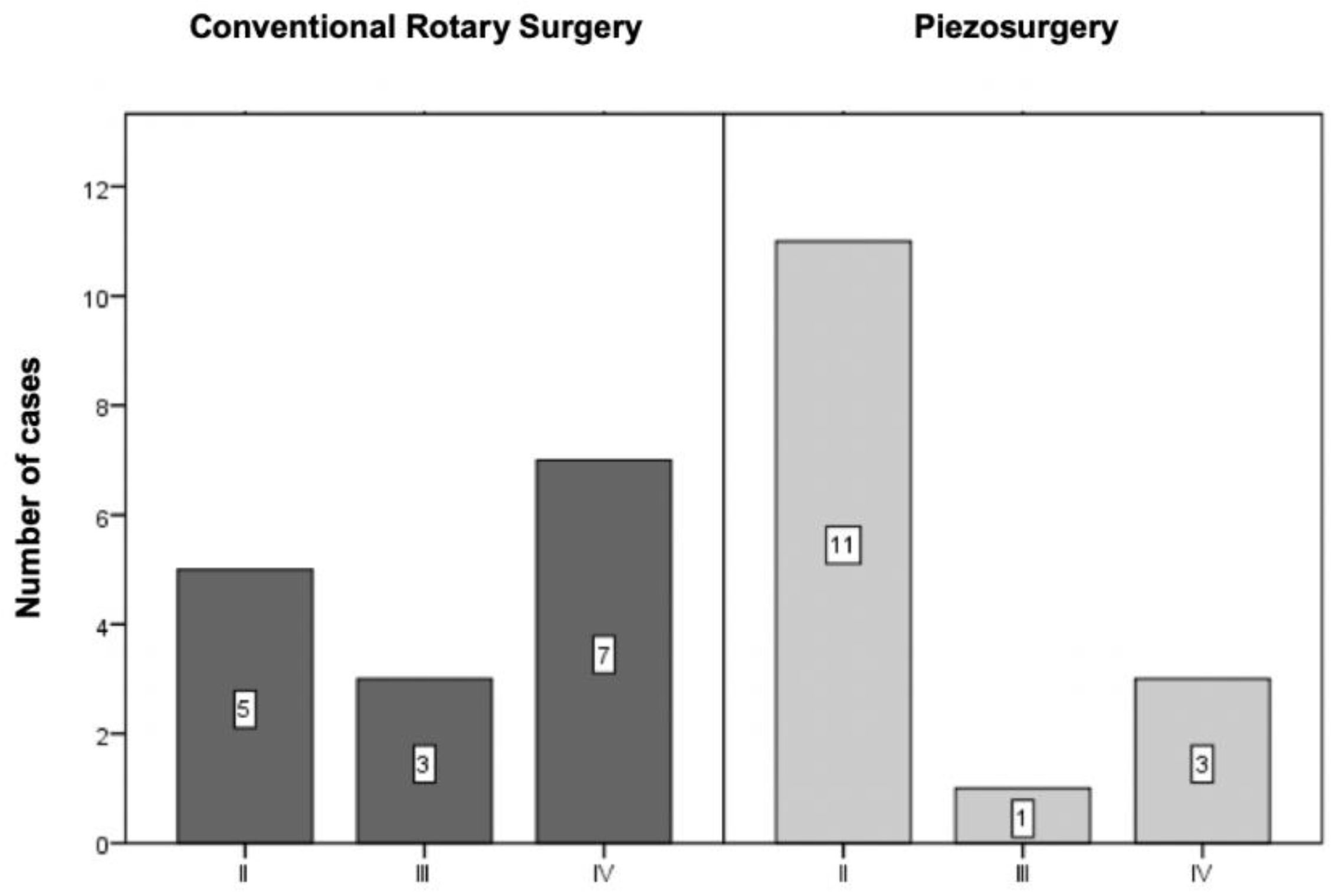
3.2.3. Modified Version of the Parant Scale
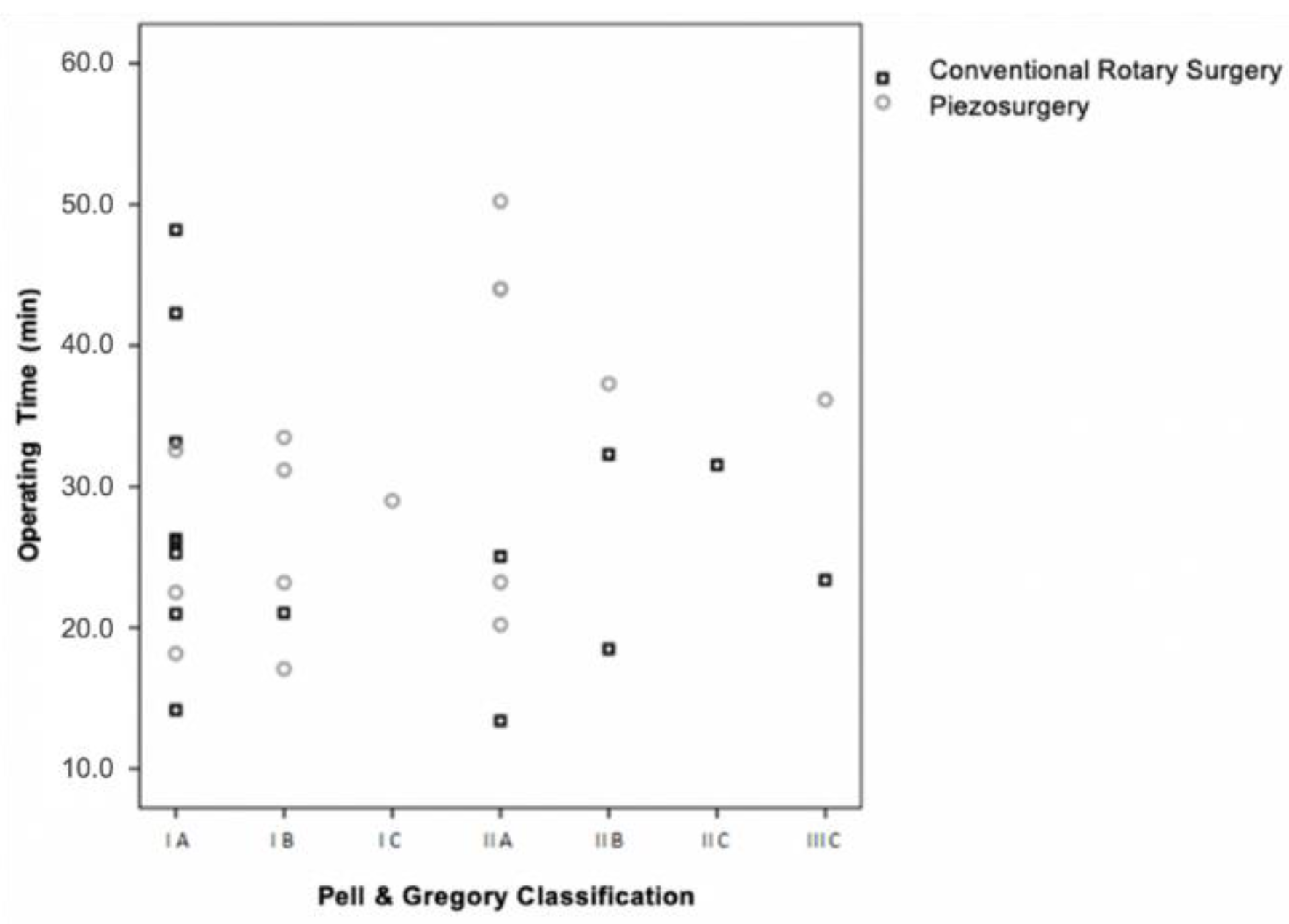
3.3. Operating Time vs. Surgical Difficulty vs. Surgical Technique
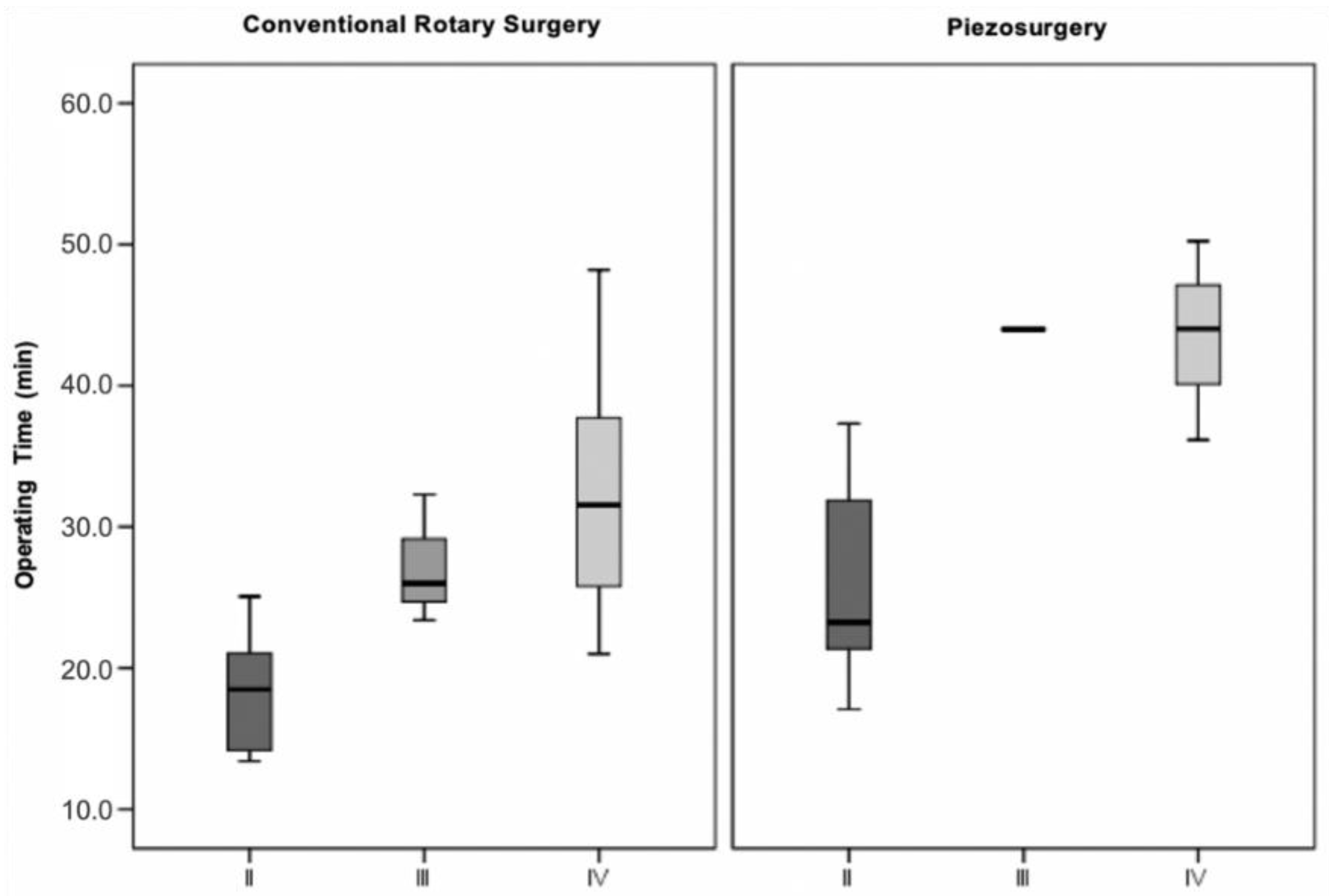
3.3.1. Pell and Gregory Classification
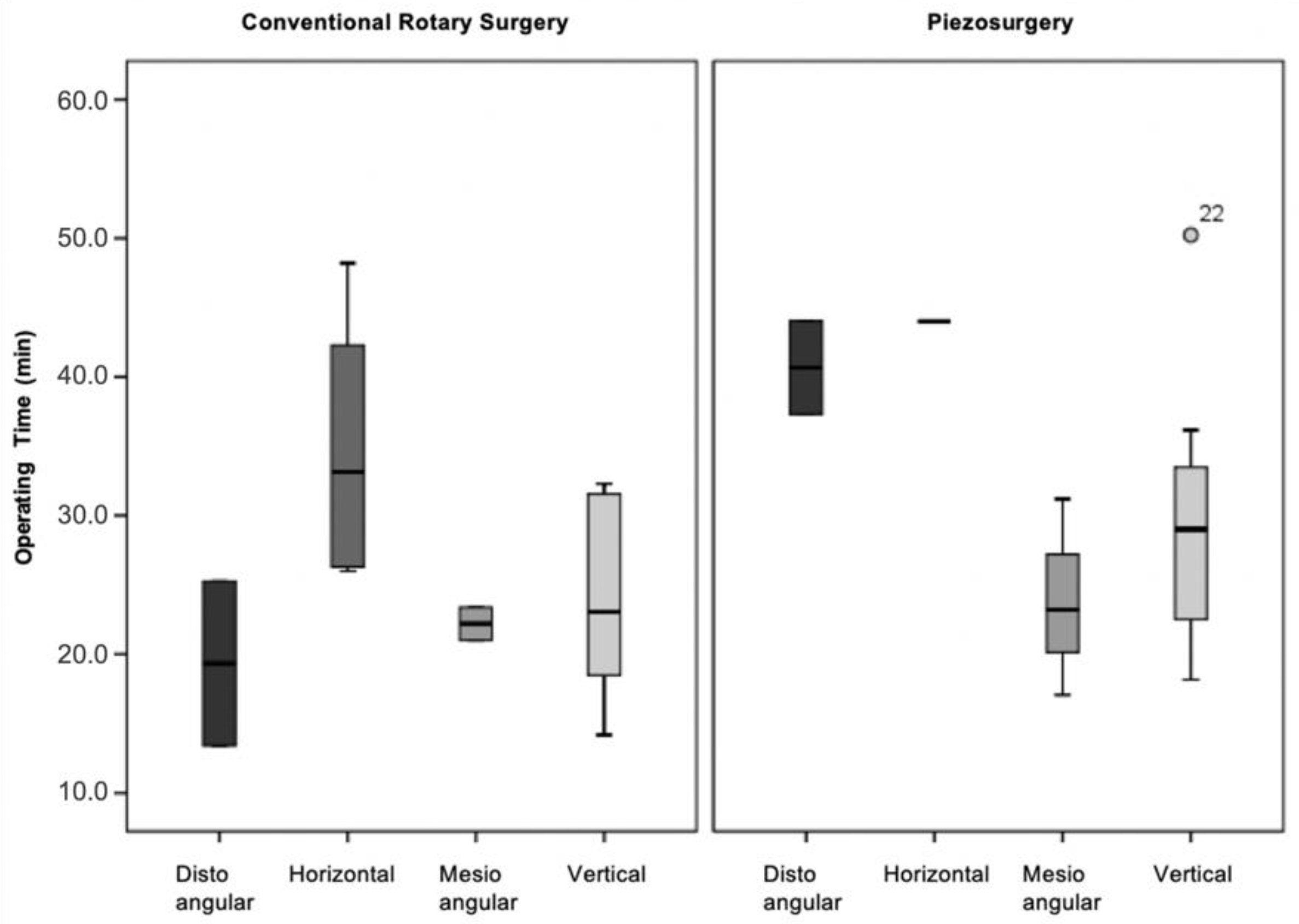
3.3.2. Winter’s Classification
3.3.3. Modified Version of the Parant Scale
3.4. Operating Time vs. Surgical Technique
3.5. Postoperative Pain
3.5.1. Pain vs. Surgical Technique (VAS)
3.5.2. Pain vs. Surgical Technique (Number of Analgesics)
3.6. Swelling
3.6.1. Swelling vs. Surgical Technique (Tg-LC)
3.6.2. Swelling vs. Surgical Technique (Tg-CM)
3.7. Trismus vs. Surgical Technique
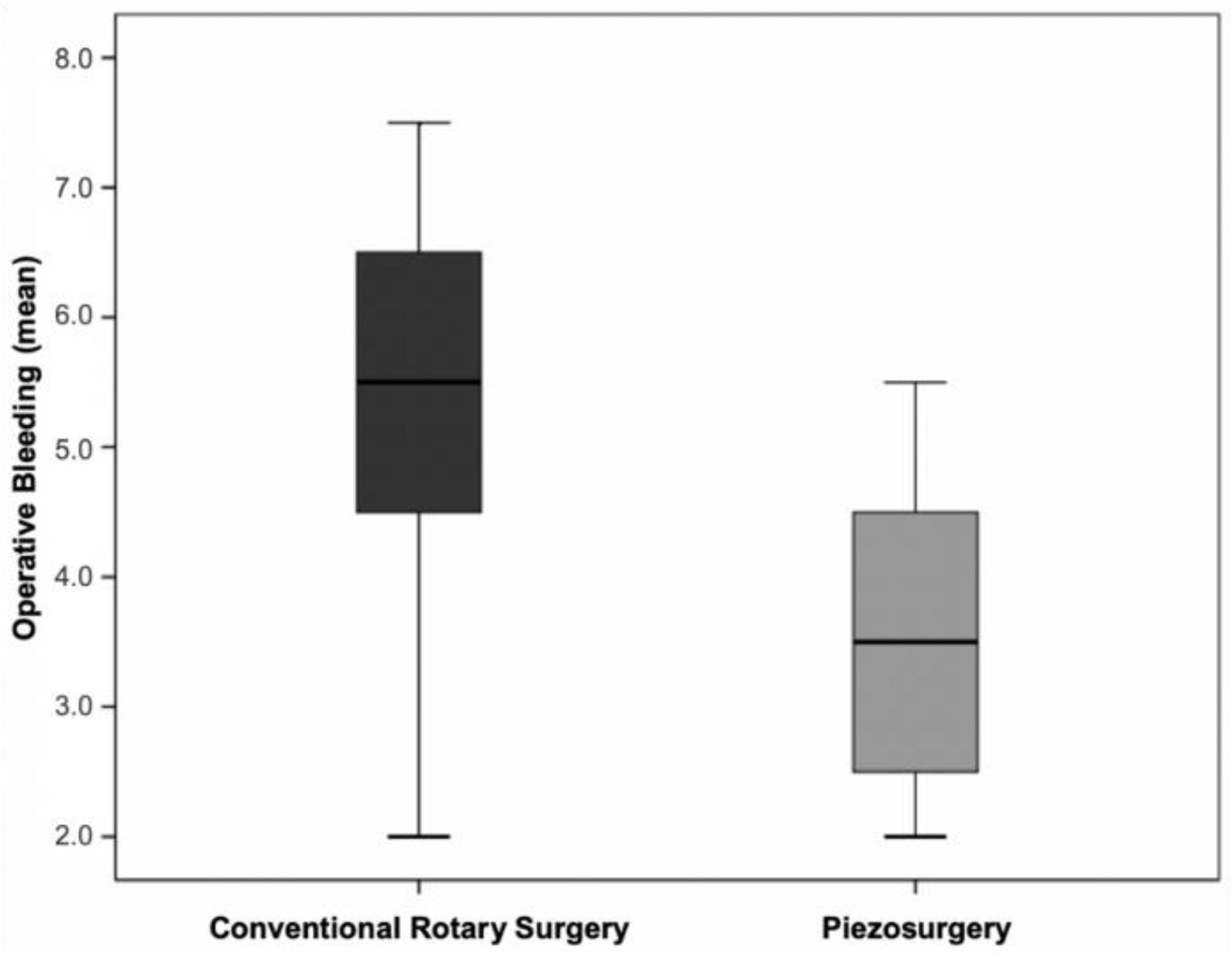
3.8. Operative Bleeding vs. Surgical Technique
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al-Delayme, R.M.A. Randomized Clinical Study Comparing Piezoelectric Surgery with Conventional Rotatory Osteotomy in Mandibular Third Molars Surgeries. Saudi Dent. J. 2021, 33, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Nehme, W.; Fares, Y.; Abou-Abbas, L. Piezo-Surgery Technique and Intramuscular Dexamethasone Injection to Reduce Postoperative Pain after Impacted Mandibular Third Molar Surgery: A Randomized Clinical Trial. BMC Oral Health 2021, 21, 393. [Google Scholar] [CrossRef] [PubMed]
- Ge, J.; Yang, C.; Zheng, J.-W.; He, D.-M.; Zheng, L.-Y.; Hu, Y.-K. Four Osteotomy Methods With Piezosurgery to Remove Complicated Mandibular Third Molars: A Retrospective Study. J. Oral Maxillofac. Surg. 2014, 72, 2126–2133. [Google Scholar] [CrossRef]
- Contar, C.; Oliveira, P.; Kanegusuku, K.; Berticelli, R.; Azevedo-Alanis, L.-R.; Machado, M.-A.-N. Complications in Third Molar Removal: A Retrospective Study of 588 Patients. Med. Oral Patol. Oral Cir. Bucal 2009, 15, e74–e78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bortoluzzi, M.C.; Guollo, A.; Capella, D.L.; Manfro, R. Pain Levels after Third Molar Surgical Removal: An Evaluation of Predictive Variables. J. Contemp. Dent. Pract. 2011, 12, 239–244. [Google Scholar] [CrossRef]
- Barone, A.; Marconcini, S.; Giacomelli, L.; Rispoli, L.; Calvo, J.L.; Covani, U. A Randomized Clinical Evaluation of Ultrasound Bone Surgery versus Traditional Rotary Instruments in Lower Third Molar Extraction. J. Oral Maxillofac. Surg. 2010, 68, 330–336. [Google Scholar] [CrossRef]
- Grossi, G.B.; Maiorana, C.; Garramone, R.A.; Borgonovo, A.; Beretta, M.; Farronato, D.; Santoro, F. Effect of Submucosal Injection of Dexamethasone on Postoperative Discomfort after Third Molar Surgery: A Prospective Study. J. Oral Maxillofac. Surg. 2007, 65, 2218–2226. [Google Scholar] [CrossRef]
- Mistry, F.; Hegde, N.; Hegde, M. Postsurgical Consequences in Lower Third Molar Surgical Extraction Using Micromotor and Piezosurgery. Ann. Maxillofac. Surg. 2016, 6, 251. [Google Scholar] [CrossRef] [Green Version]
- Civak, T.; Ustun, T.; Yilmaz, H.N.; Gursoy, B. Postoperative Evaluation of Er:YAG Laser, Piezosurgery, and Rotary Systems Used for Osteotomy in Mandibular Third-Molar Extractions. J. Craniomaxillofac. Surg. 2021, 49, 64–69. [Google Scholar] [CrossRef]
- Lago-Méndez, L.; Diniz-Freitas, M.; Senra-Rivera, C.; Gude-Sampedro, F.; Gándara Rey, J.M.; García-García, A. Relationships between Surgical Difficulty and Postoperative Pain in Lower Third Molar Extractions. J. Oral Maxillofac. Surg. 2007, 65, 979–983. [Google Scholar] [CrossRef]
- Peñarrocha, M.; Sanchis, J.M.; Sáez, U.; Gay, C.; Bagán, J.V. Oral Hygiene and Postoperative Pain after Mandibular Third Molar Surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2001, 92, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Brüllmann, D.; Jürchott, L.M.; John, C.; Trempler, C.; Schwanecke, U.; Schulze, R.K.W.W. A Contact-Free Volumetric Measurement of Facial Volume after Third Molar Osteotomy: Proof of Concept. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, e51–e56. [Google Scholar] [CrossRef] [PubMed]
- Menziletoglu, D.; Basturk, F.; Isik, B.K.; Esen, A. A Prospective Split-Mouth Clinical Study: Comparison of Piezosurgery and Conventional Rotary Instruments in Impacted Third Molar Surgery. Oral Maxillofac. Surg. 2020, 24, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Rashid, N.; Subbiah, V.; Agarwal, P.; Kumar, S.; Bansal, A.; Reddy, S.G.; Chug, A. Comparison of Piezosurgery and Conventional Rotatory Technique in Transalveolar Extraction of Mandibular Third Molars: A Pilot Study. J. Oral Biol. Craniofac. Res. 2020, 10, 615–618. [Google Scholar] [CrossRef]
- Bhati, B.; Kukreja, P.; Kumar, S.; Rathi, V.C.; Singh, K.; Bansal, S. Piezosurgery versus Rotatory Osteotomy in Mandibular Impacted Third Molar Extraction. Ann. Maxillofac. Surg. 2017, 7, 5–10. [Google Scholar] [CrossRef]
- Lang, N.; Berglundh, T.; Giannobile, W.; Sanz, M. (Eds.) Lindhe’s Clinical Periodontology and Implant Dentistry, 7th ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2021. [Google Scholar]
- Rullo, R.; Addabbo, F.; Papaccio, G.; D’Aquino, R.; Festa, V.M. Piezoelectric Device vs. Conventional Rotative Instruments in Impacted Third Molar Surgery: Relationships between Surgical Difficulty and Postoperative Pain with Histological Evaluations. J. Craniomaxillofac. Surg. 2013, 41, e33–e38. [Google Scholar] [CrossRef]
- Silva, L.D.; Reis, E.N.; Bonardi, J.P.; Lima, V.N.; Aranega, A.M.; Ponzoni, D. Influence of Surgical Ultrasound Used in the Detachment of Flaps, Osteotomy and Odontosection in Lower Third Molar Surgeries. A Prospective, Randomized, and “Split-Mouth” Clinical Study. Med. Oral Patol. Oral Cir. Bucal 2020, 25, e461–e467. [Google Scholar] [CrossRef]
- Gulnahar, Y.; Alpan, A.L. Comparison of Postoperative Morbidity between Piezoelectric Surgery and Conventional Rotary Instruments in Mandibular Third Molar Surgery: A Split-Mouth Clinical Study. Med. Oral Patol. Oral Cir. Bucal 2021, 26, e269–e275. [Google Scholar] [CrossRef]
- Patil, C.; Jadhav, A.; Rajanikanth, K.; Bhola, N.; Borle, R.M.; Mishra, A. Piezosurgery vs. Bur in Impacted Mandibular Third Molar Surgery: Evaluation of Postoperative Sequelae. J. Oral Biol. Craniofac. Res. 2019, 9, 259–262. [Google Scholar] [CrossRef]
- Piersanti, L.; Dilorenzo, M.; Monaco, G.; Marchetti, C. Piezosurgery or Conventional Rotatory Instruments for Inferior Third Molar Extractions? J. Oral Maxillofac. Surg. 2014, 72, 1647–1652. [Google Scholar] [CrossRef]
- Mantovani, E.; Arduino, P.G.; Schierano, G.; Ferrero, L.; Gallesio, G.; Mozzati, M.; Russo, A.; Scully, C.; Carossa, S. A Split-Mouth Randomized Clinical Trial to Evaluate the Performance of Piezosurgery Compared with Traditional Technique in Lower Wisdom Tooth Removal. J. Oral Maxillofac. Surg. 2014, 72, 1890–1897. [Google Scholar] [CrossRef] [PubMed]
- Mozzati, M.; Gallesio, G.; Russo, A.; Staiti, G.; Mortellaro, C. Third-Molar Extraction with Ultrasound Bone Surgery: A Case-Control Study. J. Craniofac. Surg. 2014, 25, 856–859. [Google Scholar] [CrossRef] [PubMed]
- Pippi, R.; Alvaro, R. Piezosurgery for the Lingual Split Technique in Mandibular Third Molar Removal: A Suggestion. J. Craniofacial Surg. 2013, 24, 531–533. [Google Scholar] [CrossRef] [PubMed]
- Gülnahar, Y.; Hüseyin Köşger, H.; Tutar, Y. A Comparison of Piezosurgery and Conventional Surgery by Heat Shock Protein 70 Expression. Int. J. Oral Maxillofac. Surg. 2013, 42, 508–510. [Google Scholar] [CrossRef] [PubMed]
- Cicciù, M.; Stacchi, C.; Fiorillo, L.; Cervino, G.; Troiano, G.; Vercellotti, T.; Herford, A.S.; Galindo-Moreno, P.; Di Lenarda, R. Piezoelectric Bone Surgery for Impacted Lower Third Molar Extraction Compared with Conventional Rotary Instruments: A Systematic Review, Meta-Analysis, and Trial Sequential Analysis. Int. J. Oral Maxillofac. Surg. 2021, 50, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Bilginaylar, K.; Uyanik, L.O. Evaluation of the Effects of Platelet-Rich Fibrin and Piezosurgery on Outcomes after Removal of Impacted Mandibular Third Molars. Br. J. Oral Maxillofac. Surg. 2016, 54, 629–633. [Google Scholar] [CrossRef]
- Goyal, M.; Marya, K.; Jhamb, A.; Chawla, S.; Sonoo, P.R.; Singh, V.; Aggarwal, A. Comparative Evaluation of Surgical Outcome after Removal of Impacted Mandibular Third Molars Using a Piezotome or a Conventional Handpiece: A Prospective Study. Br. J. Oral Maxillofac. Surg. 2012, 50, 556–561. [Google Scholar] [CrossRef]
- Sivolella, S.; Berengo, M.; Bressan, E.; Di Fiore, A.; Stellini, E. Osteotomy for Lower Third Molar Germectomy: Randomized Prospective Crossover Clinical Study Comparing Piezosurgery and Conventional Rotatory Osteotomy. J. Oral Maxillofac. Surg. 2011, 69, e15–e23. [Google Scholar] [CrossRef]
- Bertossi, D.; Nocini, R.; Luciano, U.; Galzignato, P.F.; Ricciardi, G.; Lucchese, A.; Tacchino, U.; Donadello, D.; Lanaro, L.; Gualdi, A.; et al. Piezoelectric Surgery Inserts vs. Conventional Burst: A Clinical Investigation. J. Biol. Regul. Homeost. Agents 2018, 32, 15–19. [Google Scholar]
- Pell, G.J.; Gregory, G.T. Impacted Mandibular Third Molars: Classification and Modified Tecnhique for Removal. Dent. Dig. 1933, 39, 330–338. [Google Scholar]
- Winter, G.B. Principles of Exodontia as Applied to the Impacted Mandibular Third Molar: A Complete Treatise on the Operative Technic with Clinical Diagnoses and Radiographic Interpretations; American Medical Book Company: New York, NY, USA, 1926. [Google Scholar]
- Thibault, R.; Parant, M. Petite Chirurgie de La Bouche; L’ Expansion Scientifique Française: Paris, France, 1974. [Google Scholar]
- Scott, J.; Huskisson, E.C. Graphic Representation of Pain. Pain 1976, 2, 175–184. [Google Scholar] [CrossRef]
- Üstün, Y.; Erdoǧan, Ö.; Esen, E.; Karsli, E.D. Comparison of the Effects of 2 Doses of Methylprednisolone on Pain, Swelling, and Trismus after Third Molar Surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 96, 535–539. [Google Scholar] [CrossRef]
- Poort, L.J.; van Neck, J.W.; van der Wal, K.G.H. Sensory Testing of Inferior Alveolar Nerve Injuries: A Review of Methods Used in Prospective Studies. J. Oral Maxillofac. Surg. 2009, 67, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Hua, C.; Pan, J.; Han, B.; Tang, X. Piezosurgery vs Conventional Rotary Instrument in the Third Molar Surgery: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Dent Sci 2018, 13, 342–349. [Google Scholar] [CrossRef]
- Al-Moraissi, E.A.; Elmansi, Y.A.; Al-Sharaee, Y.A.; Alrmali, A.E.; Alkhutari, A.S. Does the Piezoelectric Surgical Technique Produce Fewer Postoperative Sequelae after Lower Third Molar Surgery than Conventional Rotary Instruments? A Systematic Review and Meta Analysis. Int. J. Oral Maxillofac. Surg. 2016, 45, 383–391. [Google Scholar] [CrossRef]
- Jiang, Q.; Qiu, Y.; Yang, C.; Yang, J.; Chen, M.; Zhang, Z. Piezoelectric Versus Conventional Rotary Techniques for Impacted Third Molar Extraction: A Meta-Analysis of Randomized Controlled Trials. Medicine 2015, 94, e1685. [Google Scholar] [CrossRef]
- Badenoch-Jones, E.K.; David, M.; Lincoln, T. Piezoelectric Compared with Conventional Rotary Osteotomy for the Prevention of Postoperative Sequelae and Complications after Surgical Extraction of Mandibular Third Molars: A Systematic Review and Meta-Analysis. Br. J. Oral Maxillofac. Surg. 2016, 54, 1066–1079. [Google Scholar] [CrossRef]
- Sortino, F.; Pedullà, E.; Masoli, V. The Piezoelectric and Rotatory Osteotomy Technique in Impacted Third Molar Surgery: Comparison of Postoperative Recovery. J. Oral Maxillofac. Surg. 2008, 66, 2444–2448. [Google Scholar] [CrossRef]
- Chang, H.H.; Lee, M.S.; Hsu, Y.C.; Tsai, S.J.; Lin, C.P. Comparison of Clinical Parameters and Environmental Noise Levels between Regular Surgery and Piezosurgery for Extraction of Impacted Third Molars. J. Formos. Med. Assoc. 2015, 114, 929–935. [Google Scholar] [CrossRef] [Green Version]
- Troedhan, A.; Kurrek, A.; Wainwright, M.; Troedhan, A.; Kurrek, A.; Wainwright, M. Ultrasonic Piezotome Surgery: Is It a Benefit for Our Patients and Does It Extend Surgery Time? A Retrospective Comparative Study on the Removal of 100 Impacted Mandibular 3rd Molars. Open J. Stomatol. 2011, 1, 179–184. [Google Scholar] [CrossRef] [Green Version]
- Gümrükçü, Z. The Effects of Piezosurgery and Submucosal Dexamethasone Injection on Post-Operative Complications after Third Molar Surgery. J. Stomatol. Oral Maxillofac. Surg. 2019, 120, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Arakji, H.; Shokry, M.; Aboelsaad, N. Comparison of Piezosurgery and Conventional Rotary Instruments for Removal of Impacted Mandibular Third Molars: A Randomized Controlled Clinical and Radiographic Trial. Int. J. Dent. 2016, 2016, 8169356. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Post-Surgical Days | Conventional Rotary Surgery | Piezosurgery | ||
|---|---|---|---|---|
| VAS | Analgesics Number | VAS | Analgesics Number | |
| Day 0 | 4 ± 3 | 0.87 | 4 ± 3 | 0.87 |
| Day 1 | 5 ± 3 | 1.07 | 4 ± 3 | 0.87 |
| Day 2 | 4 ± 2 | 0.93 | 4 ± 3 | 0.80 |
| Day 3 | 3 ± 2 | 0.73 | 3 ± 2 | 0.40 |
| Day 4 | 2 ± 2 | 0.47 | 2 ± 2 | 0.40 |
| Day 5 | 2 ± 1 | 0.33 | 2 ± 1 | 0.20 |
| Day 6 | 1 ± 1 | 0.2 | 1 ± 1 | 0.13 |
| Day 7 | 0 ± 1 | 0.07 | 1 ± 1 | 0.00 |
| Post-Surgical Days | Conventional Rotary Surgery | Piezosurgery | ||
|---|---|---|---|---|
| Tg-LC | Tg-CM | Tg-LC | Tg-CM | |
| Day 3 | 6.9 ± 6.2 | 7.3 ± 3.4 | 4.1 ± 2.2 | 5.6 ± 4.2 |
| Day 5 | 4.5 ± 2.6 | 5.0 ± 3.5 | 2.7 ± 2.3 | 3.5 ± 4.1 |
| Day 7 | 0.7 ± 1.1 | 0.7 ± 1.6 | 0.8 ± 1.6 | 0.6 ± 1.8 |
| Post-Surgical Days | Conventional Rotary Surgery | Piezosurgery |
|---|---|---|
| Day 3 | −14.5 ± 8.7 | −15.1 ± 8.7 |
| Day 5 | −10.1 ± 7.5 | −9.5 ± 7.1 |
| Day 7 | −4.3 ± 5.5 | −4.1 ± 6.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saraiva Amaral, J.; Marto, C.M.; Farias, J.; Alves Pereira, D.; Ermida, J.; Banaco, Á.; Campos Felino, A.; Caramelo, F.; Matos, S. A Pilot Randomized Controlled Clinical Trial Comparing Piezo Versus Conventional Rotary Surgery for Removal of Impacted Mandibular Third Molars. Bioengineering 2022, 9, 276. https://doi.org/10.3390/bioengineering9070276
Saraiva Amaral J, Marto CM, Farias J, Alves Pereira D, Ermida J, Banaco Á, Campos Felino A, Caramelo F, Matos S. A Pilot Randomized Controlled Clinical Trial Comparing Piezo Versus Conventional Rotary Surgery for Removal of Impacted Mandibular Third Molars. Bioengineering. 2022; 9(7):276. https://doi.org/10.3390/bioengineering9070276
Chicago/Turabian StyleSaraiva Amaral, Joana, Carlos Miguel Marto, João Farias, Daniela Alves Pereira, Jorge Ermida, Álvaro Banaco, António Campos Felino, Francisco Caramelo, and Sérgio Matos. 2022. "A Pilot Randomized Controlled Clinical Trial Comparing Piezo Versus Conventional Rotary Surgery for Removal of Impacted Mandibular Third Molars" Bioengineering 9, no. 7: 276. https://doi.org/10.3390/bioengineering9070276
APA StyleSaraiva Amaral, J., Marto, C. M., Farias, J., Alves Pereira, D., Ermida, J., Banaco, Á., Campos Felino, A., Caramelo, F., & Matos, S. (2022). A Pilot Randomized Controlled Clinical Trial Comparing Piezo Versus Conventional Rotary Surgery for Removal of Impacted Mandibular Third Molars. Bioengineering, 9(7), 276. https://doi.org/10.3390/bioengineering9070276