
Tissue Engineering Strategies for Treating Avascular Necrosis of the Femoral Head


Abstract
1. Introduction
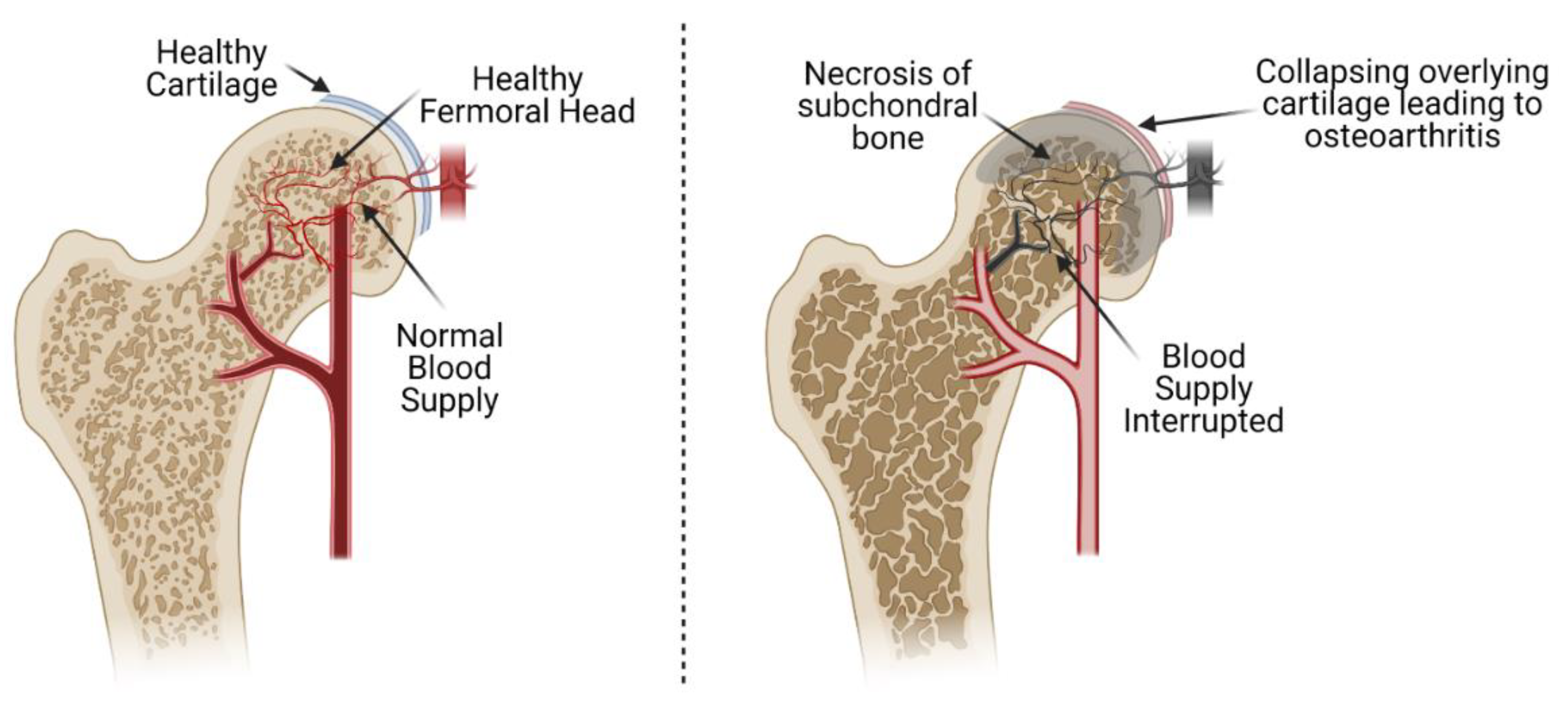
1.1. Avascular Necrosis
1.2. Etiologies
1.3. Pathophysiology of AVN
1.3.1. Ischemia
1.3.2. Regeneration
1.4. Cell and Tissue Necrosis
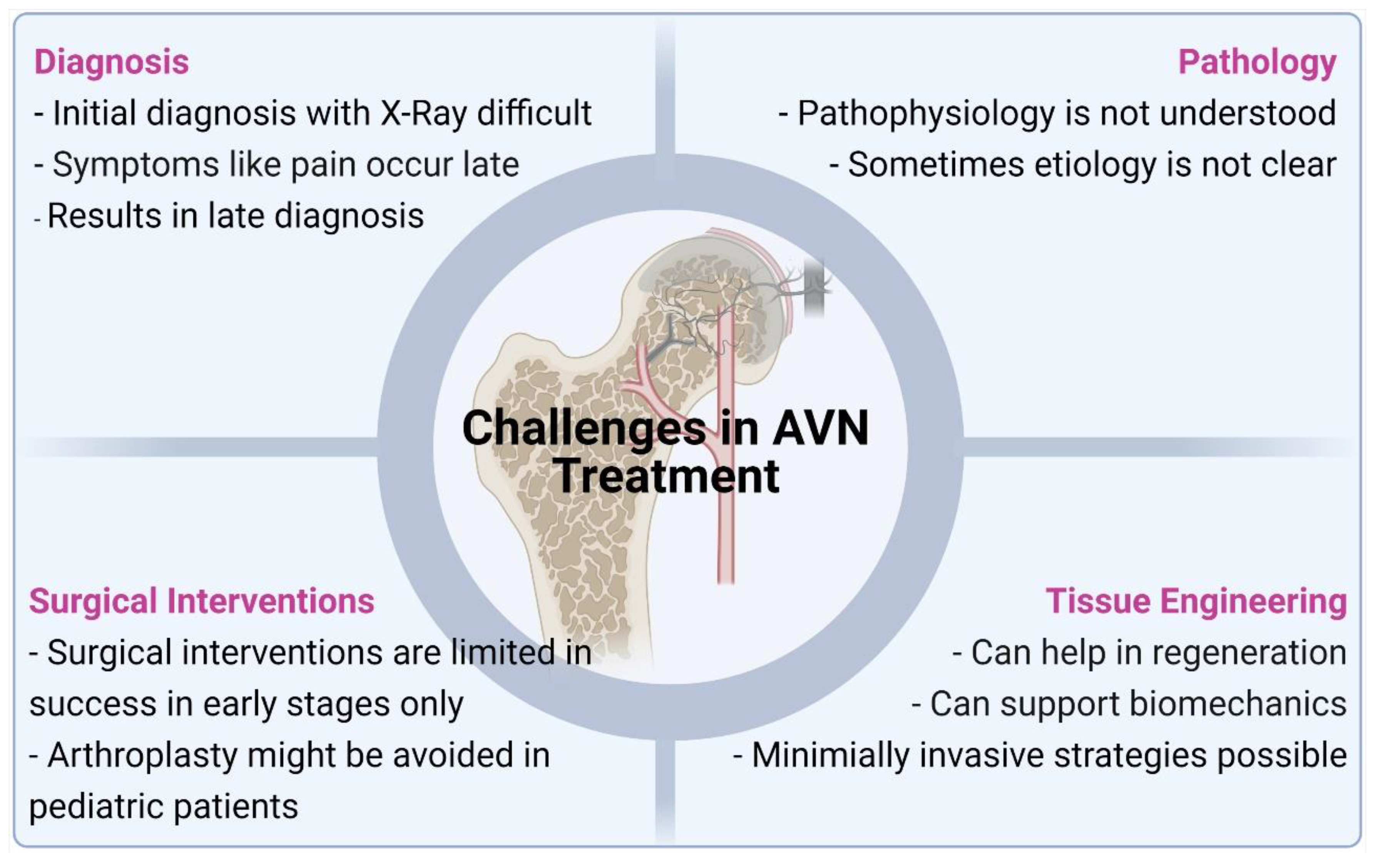
1.5. Disadvantages of Surgical Strategies
2. Desired Characteristics of 3D Scaffolds
2.1. Biocompatibility and Degradability
2.2. Porosity
2.3. Mechanical Performance
2.4. Effect of Growth Factors and Other Small Molecules
2.5. Effect of Cell Combinations
2.6. In Vivo Regeneration
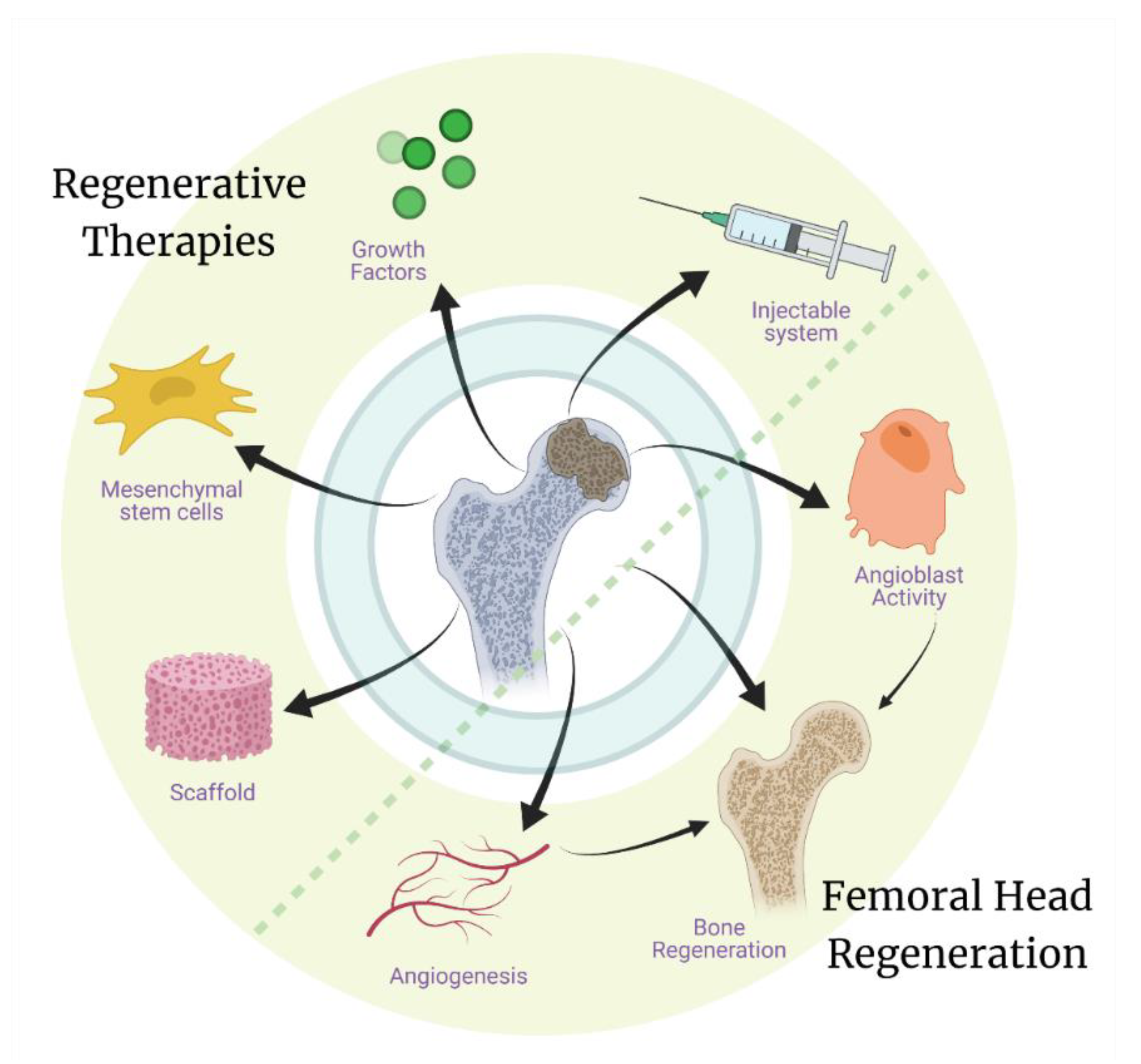
3. Tissue Engineering/Regenerative Therapies
3.1. Cellular Therapies
3.2. Growth Factor Therapies
3.3. Metallic Implants
3.3.1. Porous Titanium Rods
3.3.2. Porous Tantalum Rods
3.4. Ceramic/Polymeric Scaffolds
4. Future Perspective
Author Contributions
Funding
Conflicts of Interest
References
- Petek, D.; Hannouche, D.; Suva, D. Osteonecrosis of the femoral head: Pathophysiology and current concepts of treatment. EFORT Open Rev. 2019, 4, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Patterson, J.T.; Tangtiphaiboontana, J.; Pandya, N.K. Management of Pediatric Femoral Neck Fracture. J. Am. Acad. Orthop. Surg. 2018, 26, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Zalavras, C.G.; Lieberman, J.R. Osteonecrosis of the femoral head: Evaluation and treatment. J. Am. Acad. Orthop. Surg. 2014, 22, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Sevitt, S. Avascular necrosis and revascularisation of the femoral head after intracapsular fractures; a combined arteriographic and histological necropsy study. J. Bone Jt. Surg. Br. 1964, 46, 270–296. [Google Scholar] [CrossRef]
- Sevjtt, F.S.; Thompson, R.G. Distribution and anastomoses of arteries supplying the head neck of the femur. J. Bone Jt. Surg. Br. 1965, 47, 560–573. [Google Scholar] [CrossRef]
- Catto, M. A histological study of avascular necrosis of the femoral head after transcervical fracture. J. Bone Jt. Surg. Br. Vol. 1965, 47-B, 749–776. [Google Scholar] [CrossRef]
- Holmberg, S.; Dalen, N. Intracapsular Pressure and Caput Circulation in Nondisplaced Femoral Neck Fractures. Clin. Orthop. Relat. Res. 1987, 219, 124–126. [Google Scholar] [CrossRef]
- Baig, A.S.; Baig, M.N. Osteonecrosis of the Femoral Head: Etiology, Investigations, and Management. Cureus 2018, 10, e3171. [Google Scholar]
- Kahlenberg, C.A.; Richardson, S.S.; Schairer, W.W.; Cross, M.B. Rates and Risk Factors of Conversion Hip Arthroplasty After Closed Reduction Percutaneous Hip Pinning for Femoral Neck Fractures—A Population Analysis. J. Arthroplast. 2018, 33, 771–776. [Google Scholar] [CrossRef]
- Cherian, S.F.; Laorr, A.; Saleh, K.J.; Kuskowski, M.A.; Bailey, R.F.; Cheng, E.Y. Quantifying the Extent of Femoral Head Involvement in Osteonecrosis. J. Bone Jt. Surg. 2003, 85, 309–315. [Google Scholar] [CrossRef]
- Han, S.; Oh, M.; Yoon, S.; Kim, J.; Kim, J.-W.; Chang, J.-S.; Ryu, J.-S. Risk Stratification for Avascular Necrosis of the Femoral Head After Internal Fixation of Femoral Neck Fractures by Post-Operative Bone SPECT/CT. Nucl. Med. Mol. Imaging 2016, 51, 49–57. [Google Scholar] [CrossRef][Green Version]
- MacNeil, J.A.M.; Francis, A.; El-Hawary, R. A Systematic Review of Rigid, Locked, Intramedullary Nail Insertion Sites and Avascular Necrosis of the Femoral Head in the Skeletally Immature. J. Pediatr. Orthop. 2011, 31, 377–380. [Google Scholar] [CrossRef]
- Guerado, E.; Caso, E. The physiopathology of avascular necrosis of the femoral head: An update. Injury 2016, 47, S16–S26. [Google Scholar] [CrossRef]
- Nishio, A. Legg-Calve-Perthes disease;histology and treatment. Yonago Acta Med. 1962, 6, 1. [Google Scholar]
- Kleinman, R.G.; Bleck, E.E. Increased Blood Viscosity in Patients with Legg-Perthes Disease. J. Pediatr. Orthop. 1981, 1, 131–136. [Google Scholar] [CrossRef]
- Douglas, G.; Rang, M. The Role of Trauma in the Pathogenesis of the Osteochondroses. Clin. Orthop. Relat. Res. 1981, 158, 28–32. [Google Scholar] [CrossRef]
- Phemister, D.B. Repair of Bone in the Presence of Aseptic Necrosis Resulting from Fractures, Tranplantations, and Vascular Obstruction. JBJS 2005, 87, 672. [Google Scholar] [CrossRef]
- Tsao, A.K.; Dias, L.S.; Conway, J.J.; Straka, P. The Prognostic Value and Significance of Serial Bone Scintigraphy in Legg-Calvé-Perthes Disease. J. Pediatr. Orthop. 1997, 17, 230–239. [Google Scholar] [CrossRef] [PubMed]
- de Sanctis, N.; Rondinella, F. Prognostic Evaluation of Legg–Calvé–Perthes Disease by MRI Part II: Pathomorphogenesis and New Classification. J. Pediatr. Orthop. 2000, 20, 463–470. [Google Scholar] [CrossRef]
- Meirelles, L.D.S.; Caplan, A.I.; Nardi, N.B. In Search of the In Vivo Identity of Mesenchymal Stem Cells. Stem Cells 2008, 26, 2287–2299. [Google Scholar] [CrossRef]
- Kenzora, J.E.; Steele, R.E.; Yosipovitch, Z.H.; Glimcher, M.J. Experimental Osteonecrosis of the Femoral Head in Adult Rabbits. Clin. Orthop. Relat. Res. 1978, 130, 8–46. [Google Scholar] [CrossRef]
- Glueck, C.J.; Freiberg, R.; Tracy, T.; Stroop, D.; Wang, P. Thrombophilia and Hypofibrinolysis; Pathophysiologies of Osteonecrosis. Clin. Orthop. Relat. Res. 1997, 334, 43–56. [Google Scholar] [CrossRef]
- Feng, Y.; Yang, S.-H.; Xiao, B.-J.; Xu, W.-H.; Ye, S.; Xia, T.; Zheng, D.; Liu, X.-Z.; Liao, Y.-F. Decreased in the number and function of circulation endothelial progenitor cells in patients with avascular necrosis of the femoral head. Bone 2010, 46, 32–40. [Google Scholar] [CrossRef]
- Song, H.-J. Peripheral Blood Stem Cell Transplantation for Ischemic Femoral Head Necrosis. Transplant. Proc. 2010, 42, 1862–1864. [Google Scholar] [CrossRef] [PubMed]
- Chung, S. The arterial supply of the developing proximal end of the human femur. J. Bone Jt. Surg. Am. Vol. 1976, 58, 961–970. [Google Scholar] [CrossRef]
- Zhang, H.-X.; Zhang, X.-P.; Xiao, G.-Y.; Hou, Y.; Cheng, L.; Si, M.; Wang, S.-S.; Li, Y.-H.; Nie, L. In vitro and in vivo evaluation of calcium phosphate composite scaffolds containing BMP-VEGF loaded PLGA microspheres for the treatment of avascular necrosis of the femoral head. Mater. Sci. Eng. C 2016, 60, 298–307. [Google Scholar] [CrossRef]
- Muirhead-Allwood, W.; Ca1terall, A. The treatment of perthes’ disease the results of a trial of management. J. Bone Jt. Surg. Br. 1982, 64, 282–285. [Google Scholar] [CrossRef]
- Zinn, W.M. Idiopathic ischaemic necrosis of the femoral head in adults. Mod. Trends Rheumatol. 1971, 2, 348–365. [Google Scholar] [PubMed]
- Davidson, J.K.; Harrison, J.A.; Jacobs, P.; Hilditch, T.E.; Catto, M.; Hendry, W. The significance of bone islands, cystic areas and sclerotic areas in dysbaric osteonecrosis. Clin. Radiol. 1977, 28, 381–393. [Google Scholar] [CrossRef]
- Ohzono, K.; Saito, M.; Takaoka, K.; Ono, K.; Saito, S.; Nishina, T.; Kadowaki, T. Natural history of nontraumatic avascular necrosis of the femoral head. J. Bone Jt. Surg. Br. Vol. 1991, 73-B, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Milgram, J.W. Reparative Cartilaginous Callus in Subarticular Osteonecrosis of Bone. A histopathological study of the femoral head. Clin. Orthop. Relat. Res. 1984, 186, 272–283. [Google Scholar] [CrossRef]
- Callaghan, J.J.; Rosenburg, A.G.; Rubash, H.E. Osteonecrosis: Etiology, Natural History, Pathophysiology, and Diagnosis. In The Adult Hip; Lippincot, Williams & Wilkins: Baltimore, MD, USA, 2007. [Google Scholar]
- James, J.; Steijn-Myagkaya, G. Death of osteocytes. Electron microscopy after in vitro ischaemia. J. Bone Jt. Surg. Br. Vol. 1986, 68-B, 620–624. [Google Scholar] [CrossRef]
- Glimcher, M.J.; Kenzora, J.E. The biology of osteonecrosis of the human femoral head and its clinical implication: I. Tissue biology. Clin. Orthop. Relat. Res. 1979, 138, 284–309. [Google Scholar]
- Brown, T.D.; Baker, K.J.; Brand, R.A. Structural consequences of subchondral bone involvement in segmental osteonecrosis of the femoral head. J. Orthop. Res. 1992, 10, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.N.; Racine, J.; Jones, L.C.; Aaron, R.K. Pathophysiology and risk factors for osteonecrosis. Curr. Rev. Musculoskelet. Med. 2015, 8, 201–209. [Google Scholar] [CrossRef]
- Wang, Y.; Ma, X.; Chai, W.; Tian, J. Multiscale Stem Cell Technologies for Osteonecrosis of the Femoral Head. Stem Cells Int. 2019, 2019, 1–13. [Google Scholar] [CrossRef]
- Zhu, T.; Cui, Y.; Zhang, M.; Zhao, D.; Liu, G.; Ding, J. Engineered three-dimensional scaffolds for enhanced bone regeneration in osteonecrosis. Bioact. Mater. 2020, 5, 584–601. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.; Li, Y.; Cao, H.; Long, J.; Wang, X.; Li, L.; Li, C.; Jia, Q.; Teng, B.; Tang, T.; et al. Osteogenic magnesium incorporated into PLGA/TCP porous scaffold by 3D printing for repairing challenging bone defect. Biomaterials 2019, 197, 207–219. [Google Scholar] [CrossRef] [PubMed]
- Qin, L.; Yao, D.; Zheng, L.; Liu, W.-C.; Liu, Z.; Lei, M.; Huang, L.; Xie, X.; Wang, X.; Chen, Y.; et al. Phytomolecule icaritin incorporated PLGA/TCP scaffold for steroid-associated osteonecrosis: Proof-of-concept for prevention of hip joint collapse in bipedal emus and mechanistic study in quadrupedal rabbits. Biomaterials 2015, 59, 125–143. [Google Scholar] [CrossRef]
- Deng, G.; Niu, K.; Zhou, F.; Li, B.; Kang, Y.; Liu, X.; Hu, J.; Li, B.; Wang, Q.; Yi, C.; et al. Treatment of steroid-induced osteonecrosis of the femoral head using porous Se@SiO2 nanocomposites to suppress reactive oxygen species. Sci. Rep. 2017, 7, srep43914. [Google Scholar] [CrossRef] [PubMed]
- Xia, T.; Gao, R.; Zhou, G.; Liu, J.; Li, J.; Shen, J. Trans-Cinnamaldehyde Inhibits IL-1β-Stimulated Inflammation in Chondrocytes by Suppressing NF-κB and p38-JNK Pathways and Exerts Chondrocyte Protective Effects in a Rat Model of Osteoarthritis. BioMed Res. Int. 2019, 2019, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Gao, R.; Ji, W.; Xia, T.; Fan, Y.; Wei, W.; Shi, L.; Liu, J.; Zhang, C.; Xue, L.; Shen, J. Three-dimensional-printed titanium alloy porous scaffold combined with trans-cinnamaldehyde for repairing osteonecrosis of the femoral head in a dog model. Am. J. Transl. Res. 2020, 12, 1070–1079. [Google Scholar] [PubMed]
- Kawai, T.; Shanjani, Y.; Fazeli, S.; Behn, A.W.; Okuzu, Y.; Goodman, S.B.; Yang, Y.P. Customized, degradable, functionally graded scaffold for potential treatment of early stage osteonecrosis of the femoral head. J. Orthop. Res. 2017, 36, 1002–1011. [Google Scholar] [CrossRef]
- Shen, J.; Wang, W.; Zhai, X.; Chen, B.; Qiao, W.; Li, W.; Li, P.; Zhao, Y.; Meng, Y.; Qian, S.; et al. 3D-printed nanocomposite scaffolds with tunable magnesium ionic microenvironment induce in situ bone tissue regeneration. Appl. Mater. Today 2019, 16, 493–507. [Google Scholar] [CrossRef]
- Yan, Y.; Chen, H.; Zhang, H.; Guo, C.; Yang, K.; Chen, K.; Cheng, R.; Qian, N.; Sandler, N.; Zhang, Y.S.; et al. Vascularized 3D printed scaffolds for promoting bone regeneration. Biomaterials 2018, 190, 97–110. [Google Scholar] [CrossRef]
- Guillaume, O.; Geven, M.; Sprecher, C.; Stadelmann, V.; Grijpma, D.; Tang, T.; Qin, L.; Lai, Y.; Alini, M.; De Bruijn, J.; et al. Surface-enrichment with hydroxyapatite nanoparticles in stereolithography-fabricated composite polymer scaffolds promotes bone repair. Acta Biomater. 2017, 54, 386–398. [Google Scholar] [CrossRef] [PubMed]
- Torres-Sanchez, C.; Al Mushref, F.; Norrito, M.; Yendall, K.; Liu, Y.; Conway, P. The effect of pore size and porosity on mechanical properties and biological response of porous titanium scaffolds. Mater. Sci. Eng. C 2017, 77, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Grier, W.K.; Iyoha, E.M.; Harley, B.A. The influence of pore size and stiffness on tenocyte bioactivity and transcriptomic stability in collagen-GAG scaffolds. J. Mech. Behav. Biomed. Mater. 2016, 65, 295–305. [Google Scholar] [CrossRef]
- Xiao, X.; Wang, W.; Liu, D.; Zhang, H.; Gao, P.; Geng, L.; Yuan, Y.; Lu, J.; Wang, Z. The promotion of angiogenesis induced by three-dimensional porous beta-tricalcium phosphate scaffold with different interconnection sizes via activation of PI3K/Akt pathways. Sci. Rep. 2015, 5, srep09409. [Google Scholar] [CrossRef]
- Feng, C.; Zhang, W.; Deng, C.; Li, G.; Chang, J.; Zhang, Z.; Jiang, X.; Wu, C. 3D Printing of Lotus Root-Like Biomimetic Materials for Cell Delivery and Tissue Regeneration. Adv. Sci. 2017, 4, 1700401. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Sun, M.; Chen, B.; Saiding, Q.; Zhang, J.; Song, H.; Deng, L.; Wang, P.; Gong, W.; Cui, W. Lotus seedpod-inspired internal vascularized 3D printed scaffold for bone tissue repair. Bioact. Mater. 2020, 6, 1639–1652. [Google Scholar] [CrossRef]
- Rnjak-Kovacina, J.; Wray, L.S.; Golinski, J.M.; Kaplan, D.L. Arrayed Hollow Channels in Silk-Based Scaffolds Provide Functional Outcomes for Engineering Critically Sized Tissue Constructs. Adv. Funct. Mater. 2013, 24, 2188–2196. [Google Scholar] [CrossRef]
- Cui, Z.-K.; Kim, S.; Baljon, J.J.; Wu, B.M.; Aghaloo, T.; Lee, M. Microporous methacrylated glycol chitosan-montmorillonite nanocomposite hydrogel for bone tissue engineering. Nat. Commun. 2019, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-H.; Lin, C.-Y.; Liu, F.-H.; Chen, M.H.-C.; Lin, C.-P.; Ho, H.-N.; Liao, Y.-S. 3D Printing Bioceramic Porous Scaffolds with Good Mechanical Property and Cell Affinity. PLoS ONE 2015, 10, e0143713. [Google Scholar] [CrossRef]
- Khodaei, M.; Valanezhad, A.; Watanabe, I.; Yousefi, R. Surface and mechanical properties of modified porous titanium scaffold. Surf. Coat. Technol. 2017, 315, 61–66. [Google Scholar] [CrossRef]
- Lin, H.; Tang, Y.; Lozito, T.P.; Oyster, N.; Wang, B.; Tuan, R.S. Efficient in vivo bone formation by BMP-2 engineered human mesenchymal stem cells encapsulated in a projection stereolithographically fabricated hydrogel scaffold. Stem Cell Res. Ther. 2019, 10, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Xia, P.; Wang, S.; Qi, Z.; Zhang, W.; Sun, Y. BMP-2-releasing gelatin microspheres/PLGA scaffolds for bone repairment of X-ray-radiated rabbit radius defects. Artif. Cells Nanomed. Biotechnol. 2019, 47, 1662–1673. [Google Scholar] [CrossRef] [PubMed]
- Ren, Q.; Cai, M.; Zhang, K.; Ren, W.; Su, Z.; Yang, T.; Sun, T.; Wang, J. Effects of bone morphogenetic protein-2 (BMP-2) and vascular endothelial growth factor (VEGF) release from polylactide-poly (ethylene glycol)-polylactide (PELA) microcapsule-based scaffolds on bone. Braz. J. Med. Biol. Res. 2018, 51, e6520. [Google Scholar] [CrossRef] [PubMed]
- Dou, D.; Zhou, G.; Liu, H.; Zhang, J.; Liu, M.; Xiao, X.; Fei, J.; Guan, X.; Fan, Y. Sequential releasing of VEGF and BMP-2 in hydroxyapatite collagen scaffolds for bone tissue engineering: Design and characterization. Int. J. Biol. Macromol. 2018, 123, 622–628. [Google Scholar] [CrossRef]
- Momose, T.; Miyaji, H.; Kato, A.; Ogawa, K.; Yoshida, T.; Nishida, E.; Murakami, S.; Kosen, Y.; Sugaya, T.; Kawanami, M. Collagen Hydrogel Scaffold and Fibroblast Growth Factor-2 Accelerate Periodontal Healing of Class II Furcation Defects in Dog. Open Dent. J. 2016, 10, 347–359. [Google Scholar] [CrossRef]
- Yao, Q.; Liu, Y.; Selvaratnam, B.; Koodali, R.T.; Sun, H. Mesoporous silicate nanoparticles/3D nanofibrous scaffold-mediated dual-drug delivery for bone tissue engineering. J. Control. Release 2018, 279, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Liyanage, A.D.T.; Chen, A.J.; Puleo, D.A. Vancomycin- and Poly(simvastatin)-Loaded Scaffolds with Time-Dependent Development of Porosity. ACS Appl. Bio Mater. 2019, 2, 2511–2519. [Google Scholar] [CrossRef]
- Encarnação, I.C.; Sordi, M.B.; Aragones, A.; Müller, C.M.O.; Moreira, A.C.; Fernandes, C.P.; Ramos, J.V.; Cordeiro, M.M.R.; Fredel, M.C.; Magini, R.S. Release of simvastatin from scaffolds of poly(lactic-co-glycolic) acid and biphasic ceramic designed for bone tissue regeneration. J. Biomed. Mater. Res. Part B Appl. Biomater. 2018, 107, 2152–2164. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.; Wang, Y.; Ma, W.; Dong, W.; Zhang, M.; Sun, D. Dual-Drug-Loaded Silk Fibroin/PLGA Scaffolds for Potential Bone Regeneration Applications. J. Nanomater. 2019, 2019, 1–16. [Google Scholar] [CrossRef]
- Sun, Z.; Wu, F.; Gao, H.; Cui, K.; Xian, M.; Zhong, J.; Tian, Y.; Fan, S.; Wu, G. A Dexamethasone-Eluting Porous Scaffold for Bone Regeneration Fabricated by Selective Laser Sintering. ACS Appl. Bio Mater. 2020, 3, 8739–8747. [Google Scholar] [CrossRef]
- Sadeghi-Ataabadi, M.; Mostafavi-Pour, Z.; Vojdani, Z.; Sani, M.; Latifi, M.; Talaei-Khozani, T. Fabrication and characterization of platelet-rich plasma scaffolds for tissue engineering applications. Mater. Sci. Eng. C 2017, 71, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Sun, T.; Man, Z.; Peng, C.; Wang, G.; Sun, S. A specific affinity cyclic peptide enhances the adhesion, expansion and proliferation of rat bone mesenchymal stem cells on β-tricalcium phosphate scaffolds. Mol. Med. Rep. 2019, 20, 1157–1166. [Google Scholar] [CrossRef]
- Xu, H.; Wang, C.; Liu, C.; Peng, Z.; Li, J.; Jin, Y.; Wang, Y.; Guo, J.; Zhu, L. Cotransplantation of mesenchymal stem cells and endothelial progenitor cells for treating steroid-induced osteonecrosis of the femoral head. Stem Cells Transl. Med. 2021, 10, 781–796. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Umebayashi, M.; Abdallah, M.-N.; Dong, G.; Roskies, M.G.; Zhao, Y.F.; Murshed, M.; Zhang, Z.; Tran, S.D. Combination of polyetherketoneketone scaffold and human mesenchymal stem cells from temporomandibular joint synovial fluid enhances bone regeneration. Sci. Rep. 2019, 9, 1–13. [Google Scholar] [CrossRef]
- Dębski, T.; Kurzyk, A.; Ostrowska, B.; Wysocki, J.; Jaroszewicz, J.; Święszkowski, W.; Pojda, Z. Scaffold vascularization method using an adipose-derived stem cell (ASC)-seeded scaffold prefabricated with a flow-through pedicle. Stem Cell Res. Ther. 2020, 11, 1–14. [Google Scholar] [CrossRef]
- Jiménez, N.T.; Munévar, J.C.; González, J.M.; Infante, C.; Lara, S.J.P. In vitro response of dental pulp stem cells in 3D scaffolds: A regenerative bone material. Heliyon 2018, 4, e00775. [Google Scholar] [CrossRef] [PubMed]
- Salgado, C.L.; Barrias, C.C.; Monteiro, F.J.M. Clarifying the Tooth-Derived Stem Cells Behavior in a 3D Biomimetic Scaffold for Bone Tissue Engineering Applications. Front. Bioeng. Biotechnol. 2020, 8, 724. [Google Scholar] [CrossRef]
- Liu, J.; Chen, G.; Xu, H.; Hu, K.; Sun, J.; Liu, M.; Zhang, F.; Gu, N. Pre-vascularization in fibrin Gel/PLGA microsphere scaffolds designed for bone regeneration. NPG Asia Mater. 2018, 10, 827–839. [Google Scholar] [CrossRef]
- Chen, L.; Wu, J.; Wu, C.; Xing, F.; Li, L.; He, Z.; Peng, K.; Xiang, Z. Three-Dimensional Co-Culture of Peripheral Blood-Derived Mesenchymal Stem Cells and Endothelial Progenitor Cells for Bone Regeneration. J. Biomed. Nanotechnol. 2019, 15, 248–260. [Google Scholar] [CrossRef]
- Chen, J.; Deng, L.; Porter, C.; Alexander, G.; Patel, D.; Vines, J.; Zhang, X.; Chasteen-Boyd, D.; Sung, H.-J.; Li, Y.-P.; et al. Angiogenic and Osteogenic Synergy of Human Mesenchymal Stem Cells and Human Umbilical Vein Endothelial Cells Cocultured on a Nanomatrix. Sci. Rep. 2018, 8, 1–12. [Google Scholar] [CrossRef]
- Li, D.; Xie, X.; Yang, Z.; Wang, C.; Wei, Z.; Kang, P. Enhanced bone defect repairing effects in glucocorticoid-induced osteonecrosis of the femoral head using a porous nano-lithium-hydroxyapatite/gelatin microsphere/erythropoietin composite scaffold. Biomater. Sci. 2018, 6, 519–537. [Google Scholar] [CrossRef]
- Zhu, W.; Zhao, Y.; Ma, Q.; Wang, Y.; Wu, Z.; Weng, X. 3D-printed porous titanium changed femoral head repair growth patterns: Osteogenesis and vascularisation in porous titanium. J. Mater. Sci. Mater. Electron. 2017, 28, 62. [Google Scholar] [CrossRef]
- Luo, Y.; Li, D.; Xie, X.; Kang, P. Porous, lithium-doped calcium polyphosphate composite scaffolds containing vascular endothelial growth factor (VEGF)-loaded gelatin microspheres for treating glucocorticoid-induced osteonecrosis of the femoral head. Biomed. Mater. 2019, 14, 35013. [Google Scholar] [CrossRef]
- Wang, J.; Mi, R.; Zhao, G.; Shi, J.; Chen, J.; Liu, C.; Shao, Z.; Xia, J. A silk-based high impact composite for the core decompression of the femoral head. J. Mater. Chem. B 2020, 8, 9734–9743. [Google Scholar] [CrossRef]
- Wang, P.; Li, G.; Qin, W.; Shi, B.; Liu, F.-J.; Wang, L.-L.; Zhao, B.; Sun, T.-F.; Lin, L.; Wang, D.-D. Repair of osteonecrosis of the femoral head. Der Orthop. 2019, 48, 213–223. [Google Scholar] [CrossRef]
- Zhu, H.; Shi, Z.; Cai, X.; Yang, X.; Zhou, C. The combination of PLLA/PLGA/PCL composite scaffolds integrated with BMP-2-loaded microspheres and low-intensity pulsed ultrasound alleviates steroid-induced osteonecrosis of the femoral head. Exp. Ther. Med. 2020, 20, 1. [Google Scholar] [CrossRef] [PubMed]
- Mou, P.; Peng, H.; Zhou, L.; Li, L.; Li, H.; Huang, Q. A novel composite scaffold of Cu-doped nano calcium-deficient hydroxyapatite/multi-(amino acid) copolymer for bone tissue regeneration. Int. J. Nanomed. 2019, 14, 3331–3343. [Google Scholar] [CrossRef]
- Kang, P.; Xie, X.; Tan, Z.; Yang, J.; Shen, B.; Zhou, Z.; Pei, F. Repairing defect and preventing collapse of femoral head in a steroid-induced osteonecrotic of femoral head animal model using strontium-doped calcium polyphosphate combined BM-MNCs. J. Mater. Sci. Mater. Electron. 2015, 26, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Maruyama, M.; Nabeshima, A.; Pan, C.-C.; Behn, A.W.; Thio, T.; Lin, T.; Pajarinen, J.; Kawai, T.; Takagi, M.; Goodman, S.B.; et al. The effects of a functionally-graded scaffold and bone marrow-derived mononuclear cells on steroid-induced femoral head osteonecrosis. Biomaterials 2018, 187, 39–46. [Google Scholar] [CrossRef]
- Xia, T.W.; Liu, J.Z.; Shi, L.; Gao, R.Z.; Wei, W.; Zhang, C.; Shen, J.R. New idea of tissue engineering technology in the treatment of osteonecrosis of femoral head. Chin. J. Tissue Eng. Res. 2020, 24, 2919–2925. [Google Scholar] [CrossRef]
- Drescher, W.; Pufe, T.; Smeets, R.; Eisenhart-Rothe, R.V.; Jager, M.; Tingart, M. Hüftkopfnekrose—Diagnostik und Differenzialtherapie. Z. Orthop. Unfall. 2011, 149, 231–242. [Google Scholar] [CrossRef]
- Andriolo, L.; Merli, G.; Tobar, C.; Altamura, S.A.; Kon, E.; Filardo, G. Regenerative therapies increase survivorship of avascular necrosis of the femoral head: A systematic review and meta-analysis. Int. Orthop. 2018, 42, 1689–1704. [Google Scholar] [CrossRef]
- Shu, P.; Sun, D.L.; Shu, Z.X.; Tian, S.; Pan, Q.; Wen, M.C.; Xi, J.Y.; Ye, S.N. Therapeutic Applications of Genes and Gene-Engineered Mesenchymal Stem Cells for Femoral Head Necrosis. Hum. Gene Ther. 2020, 31, 286–296. [Google Scholar] [CrossRef]
- Rosset, P.; Deschaseaux, F.; Layrolle, P. Cell therapy for bone repair. Orthop. Traumatol. Surg. Res. 2014, 100, S107–S112. [Google Scholar] [CrossRef] [PubMed]
- Fernández Vallone, V.B.; Romaniuk, M.A.; Choi, H.; Labovsky, V.; Otaegui, J.; Chasseing, N.A. Mesenchymal stem cells and their use in therapy: What has been achieved? Differentiation 2013, 85, 1–10. [Google Scholar] [CrossRef]
- Abe, T.; Sumi, K.; Kunimatsu, R.; Oki, N.; Tsuka, Y.; Nakajima, K.; Ando, K.; Tanimoto, K. The effect of mesenchymal stem cells on osteoclast precursor cell differentiation. J. Oral Sci. 2019, 61, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Liao, W.; Zhao, Q.; Liu, M.; Xia, W.; Yang, Y.; Shao, N. Angiogenesis and bone regeneration by allogeneic mesenchymal stem cell intravenous transplantation in rabbit model of avascular necrotic femoral head. J. Surg. Res. 2012, 183, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Pak, J. Autologous Adipose Tissue-Derived Stem Cells Induce Persistent Bone-Like Tissue in Osteonecrotic Femoral Heads. Pain Physician 2012, 1, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Liu, J.S.; Wang, K. Bone marrow mesenchymal stem cell transplantation and pravastatin treatment via artery for early femoral head avascular necrosis. J. Clin. Rehabil. Tissue Eng. Res. 2010, 14, 7568–7571. [Google Scholar]
- Li, W.; Lu, X.W.; Xian, C.; Lao, S. Bone marrow mesenchymal stem cell transplantation combined with lithium chloride treatment for avascular necrosis of the femoral head in rabbits. Chin. J. Tissue Eng. Res. 2016, 20, 868–875. [Google Scholar] [CrossRef]
- Wu, Y.; Zhang, C.; Wu, J.; Han, Y.; Wu, C. Angiogenesis and bone regeneration by mesenchymal stem cell transplantation with danshen in a rabbit model of avascular necrotic femoral head. Exp. Ther. Med. 2019, 18, 163–171. [Google Scholar] [CrossRef]
- Peng, W.; Dong, W.; Zhang, F.; Wang, J.; Zhang, J.; Wu, J.; Wang, L.; Ye, C.; Li, Q.; Deng, J. Effects of transplantation of FGF-2-transfected MSCs and XACB on TNF-α expression with avascular necrosis of the femoral head in rabbits. Biosci. Rep. 2019, 39. [Google Scholar] [CrossRef] [PubMed]
- Liao, H.; Zhong, Z.; Liu, Z.; Li, L.; Ling, Z.; Zou, X. Bone mesenchymal stem cells co-expressing VEGF and BMP-6 genes to combat avascular necrosis of the femoral head. Exp. Ther. Med. 2017, 15, 954–962. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.-X.; Wang, L. Adenovirus-Mediated Expression of BMP-2 and BFGF in Bone Marrow Mesenchymal Stem Cells Combined with Demineralized Bone Matrix For Repair of Femoral Head Osteonecrosis in Beagle Dogs. Cell. Physiol. Biochem. 2017, 43, 1648–1662. [Google Scholar] [CrossRef]
- Abudusaimi, A.; Aihemaitijiang, Y.; Wang, Y.-H.; Cui, L.; Maimaitiming, S.; Abulikemu, M. Adipose-Derived Stem Cells Enhance Bone Regeneration in Vascular Necrosis of the Femoral Head in the Rabbit. J. Int. Med. Res. 2011, 39, 1852–1860. [Google Scholar] [CrossRef] [PubMed]
- Rackwitz, L.; Eden, L.; Reppenhagen, S.; Reichert, J.C.; Jakob, F.; Walles, H.; Pullig, O.; Tuan, R.S.; Rudert, M.; Nöth, U. Stem cell- and growth factor-based regenerative therapies for avascular necrosis of the femoral head. Stem Cell Res. Ther. 2012, 3, 7. [Google Scholar] [CrossRef]
- Wen, Q.; Ma, L.; Chen, Y.-P.; Yang, L.; Luo, W.; Wang, X.-N. Treatment of avascular necrosis of the femoral head by hepatocyte growth factor-transgenic bone marrow stromal stem cells. Gene Ther. 2008, 15, 1523–1535. [Google Scholar] [CrossRef]
- Wu, X.; Yang, S.; Duan, D.; Liu, X.; Zhang, Y.; Wang, J.; Yang, C.; Jiang, S. A combination of granulocyte colony-stimulating factor and stem cell factor ameliorates steroid-associated osteonecrosis in rabbits. J. Rheumatol. 2008, 35, 2241–2248. [Google Scholar] [CrossRef]
- Yang, C.; Yang, S.; Du, J.; Li, J.; Xu, W.; Xiong, Y. Vascular endothelial growth factor gene transfection to enhance the repair of avascular necrosis of the femoral head of rabbit. Chin. Med. J. 2003, 116, 1544–1548. [Google Scholar] [PubMed]
- Tang, T.T.; Lu, B.; Yue, B.; Xie, X.H.; Xie, Y.Z.; Dai, K.R.; Lu, J.X.; Lou, J.R. Treatment of osteonecrosis of the femoral head with hBMP-2-gene-modified tissue-engineered bone in goats. J. Bone Jt. Surg. Br. Vol. 2007, 89, 127–129. [Google Scholar] [CrossRef]
- Simank, H.-G.; Manggold, J.; Sebald, W.; Ries, R.; Richter, W.; Ewerbeck, V.; Sergi, C. Bone Morphogenetic Protein-2 and Growth and Differentiation Factor-5 Enhance the Healing of Necrotic Bone in a Sheep Model. Growth Factors 2001, 19, 247–257. [Google Scholar] [CrossRef]
- Dailiana, Z.H.; Stefanou, N.; Khaldi, L.; Dimakopoulos, G.; Bowers, J.R.; Fink, C.; Urbaniak, J.R. Vascular endothelial growth factor for the treatment of femoral head osteonecrosis: An experimental study in canines. World J. Orthop. 2018, 9, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, Y.; Asada, R.; So, K.; Yonezawa, A.; Nankaku, M.; Mukai, K.; Ito-Ihara, T.; Tada, H.; Yamamoto, M.; Murayama, T.; et al. A pilot study of regenerative therapy using controlled release of recombinant human fibroblast growth factor for patients with pre-collapse osteonecrosis of the femoral head. Int. Orthop. 2015, 40, 1747–1754. [Google Scholar] [CrossRef] [PubMed]
- Cao, K.; Huang, W.; An, H.; Jiang, D.-M.; Shu, Y.; Han, Z.-M. Deproteinized bone with VEGF gene transfer to facilitate the repair of early avascular necrosis of femoral head of rabbit. Chin. J. Traumatol. 2009, 12, 269–274. [Google Scholar] [PubMed]
- Hang, D.; Wang, Q.; Guo, C.; Chen, Z.; Yan, Z. Treatment of Osteonecrosis of the Femoral Head with VEGF165Transgenic Bone Marrow Mesenchymal Stem Cells in Mongrel Dogs. Cells Tissues Organs 2012, 195, 495–506. [Google Scholar] [CrossRef]
- Sun, W.; Li, Z.; Gao, F.; Shi, Z.; Zhang, Q.; Guo, W. Recombinant Human Bone Morphogenetic Protein-2 in Debridement and Impacted Bone Graft for the Treatment of Femoral Head Osteonecrosis. PLoS ONE 2014, 9, e100424. [Google Scholar] [CrossRef]
- Papanagiotou, M.; Malizos, K.N.; Vlychou, M.; Dailiana, Z.H. Autologous (non-vascularised) fibular grafting with recombinant bone morphogenetic protein-7 for the treatment of femoral head osteonecrosis. Bone Jt. J. 2014, 96, 31–35. [Google Scholar] [CrossRef]
- Vandermeer, J.S.; Kamiya, N.; Aya-Ay, J.; Garces, A.; Browne, R.; Kim, H.K. Local Administration of Ibandronate and Bone Morphogenetic Protein-2 After Ischemic Osteonecrosis of the Immature Femoral Head. J. Bone Jt. Surg. Am. Vol. 2011, 93, 905–913. [Google Scholar] [CrossRef]
- Wen, Q.; Zhou, L.; Zhou, C.; Zhou, M.; Luo, W.; Ma, L. Change in hepatocyte growth factor concentration promote mesenchymal stem cell-mediated osteogenic regeneration. J. Cell. Mol. Med. 2011, 16, 1260–1273. [Google Scholar] [CrossRef]
- Ma, X.-W.; Cui, D.-P.; Zhao, D.-W. Vascular endothelial growth factor/bone morphogenetic protein-2 bone marrow combined modification of the mesenchymal stem cells to repair the avascular necrosis of the femoral head. Int. J. Clin. Exp. Med. 2015, 8, 15528–15534. [Google Scholar]
- Wang, P.; Shi, B.; Gao, Z.-H.; Sun, T.-F.; Yang, W.-B.; Han, S.-F.; Liu, P.; Wang, L.-L.; Zhao, B.-N.; Wang, D.-D. Effect of colla cornus cervi combined with lv-mediated bmp7 transfected BMSCs on anfh in rats. Acta Pol. Pharm. 2016, 73, 1521–1530. [Google Scholar]
- Wen, Q.; Zhou, C.; Luo, W.; Zhou, M.; Ma, L. Pro-osteogenic effects of fibrin glue in treatment of avascular necrosis of the femoral head in vivo by hepatocyte growth factor-transgenic mesenchymal stem cells. J. Transl. Med. 2014, 12, 114. [Google Scholar] [CrossRef]
- Nandeesh, N.H.; Janardhan, K.; Subramanian, V.; Ashtekar, A.B.; Srikruthi, N.; Koka, P.S.; Deb, K. Treatment of AVN Using Autologous BM Stem Cells and Activated Platelet-Derived Growth Factor Concentrates. J. Stem Cells 2016, 11, 135–148. [Google Scholar] [PubMed]
- Zhang, Y.; Zhang, L.; Sun, R.; Jia, Y.; Chen, X.; Liu, Y.; Oyang, H.; Feng, L. A new 3D printed titanium metal trabecular bone reconstruction system for early osteonecrosis of the femoral head. Medicine 2018, 97, e11088. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Liu, D.; Xie, Q.; Liu, J.; Deng, S.; Gong, K.; Huang, C.; Yin, L.; Xie, M.; Guo, Z.; et al. A 3D Printed Porous Titanium Alloy Rod with Diamond Crystal Lattice for Treatment of the Early-Stage Femoral Head Osteonecrosis in Sheep. Int. J. Med. Sci. 2019, 16, 486–493. [Google Scholar] [CrossRef]
- Wang, C.; Xie, Q.; Yang, L.; Liu, J.; Liu, D.; Li, Z.; Gong, K.; Yin, L.; Wang, W.; Guo, Z.; et al. A 3D printed porous titanium alloy rod with biogenic lamellar configuration for treatment of the early-stage femoral head osteonecrosis in sheep. J. Mech. Behav. Biomed. Mater. 2020, 106, 103738. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Pei, X.; Zhou, C.; Fan, Y.; Jiang, Q.; Ronca, A.; D’Amora, U.; Chen, Y.; Li, H.; Sun, Y.; et al. The biomimetic design and 3D printing of customized mechanical properties porous Ti6Al4V scaffold for load-bearing bone reconstruction. Mater. Des. 2018, 152, 30–39. [Google Scholar] [CrossRef]
- Wang, X.; Xu, H.; Zhang, J. Using personalized 3D printed Titanium sleeve-prosthetic composite for reconstruction of severe segmental bone loss of proximal femur in revision total hip arthroplasty. Medicine 2020, 99, e18784. [Google Scholar] [CrossRef]
- Zhao, D.; Ma, Z. Application of biomaterials for the repair and treatment of osteonecrosis of the femoral head. Regen. Biomater. 2020, 7, 1–8. [Google Scholar] [CrossRef]
- Tsao, A.; Roberson, J.; Christie, M.; Dore, D.; Heck, D.; Robertson, D.; Poggie, R. Biomechanical and Clinical Evaluations of a Porous Tantalum Implant for the Treatment of Early-Stage Osteonecrosis. J. Bone Jt. Surg. Am. Vol. 2005, 87, 22–27. [Google Scholar] [CrossRef]
- Veillette, C.J.H.; Mehdian, H.; Schemitsch, E.H.; Mckee, M.D. Survivorship analysis and radiographic outcome following tantalum rod insertion for osteonecrosis of the femoral head. J. Bone Jt. Surg. Ser. A 2006, 88, 48–55. [Google Scholar]
- Pakos, E.E. Modified porous tantalum rod technique for the treatment of femoral head osteonecrosis. World J. Orthop. 2015, 6, 829–837. [Google Scholar] [CrossRef]
- Tanzer, M.; Bobyn, J.; Krygier, J.; Karabasz, D. Histopathologic Retrieval Analysis of Clinically Failed Porous Tantalum Osteonecrosis Implants. J. Bone Jt. Surg. Am. Vol. 2008, 90, 1282–1289. [Google Scholar] [CrossRef]
- Wang, L.; Xu, L.; Peng, C.; Teng, G.; Wang, Y.; Xie, X.; Wu, D. The effect of bone marrow mesenchymal stem cell and nano-hydroxyapatite/collagen I/poly-L-lactic acid scaffold implantation on the treatment of avascular necrosis of the femoral head in rabbits. Exp. Ther. Med. 2019, 18, 2021–2028. [Google Scholar] [CrossRef]
- Wang, G.; Li, Y.; Sun, T.; Wang, C.; Qiao, L.; Wang, Y.; Dong, K.; Yuan, T.; Chen, J.; Chen, G.; et al. BMSC affinity peptide-functionalized β-tricalcium phosphate scaffolds promoting repair of osteonecrosis of the femoral head. J. Orthop. Surg. Res. 2019, 14, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.; Cao, H.; Wang, X.; Chen, S.; Zhang, M.; Wang, N.; Yao, Z.; Dai, Y.; Xie, X.; Zhang, P.; et al. Porous composite scaffold incorporating osteogenic phytomolecule icariin for promoting skeletal regeneration in challenging osteonecrotic bone in rabbits. Biomaterials 2018, 153, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.; Wen, C.; Wang, A.; Wang, Y.; Xu, W.; Zhao, B.; Zhang, L.; Lu, S.; Qin, L.; Guo, Q.; et al. Micro-CT-based bone ceramic scaffolding and its performance after seeding with mesenchymal stem cells for repair of load-bearing bone defect in canine femoral head. J. Biomed. Mater. Res. Part B Appl. Biomater. 2011, 96B, 316–325. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Growth Factor | Associated Cells | Delivery Strategy | Regeneration Results | Reference |
|---|---|---|---|---|
| Hepatocyte growth factor (HGF) | BMSCs | HGF transgenic BMSCs transplanted using core decompression (CD) with fibrinogen drug delivery mixture (FG) | Formation of new capillaries on bone plates of the trabeculae. Bone marrow rich in hematopoietic tissue. | [103] |
| Granulocyte colony stimulating factor (G-CSF) and stem cell factor (SCF) | G-CSF and SCF injected subcutaneously for 5 days mobilizing BMSCs | Increase in osteocalcin protein expression. Vessel formation was 3.3 fold greater & vessel density was 2.6 fold greater than the control. | [104] | |
| Vascular endothelial growth factor (VEGF) | Plasmid encoding VEGF immobilized on a cartilage carrier into the necrotic area of the femoral head | Increase in bone formation after 8 weeks. | [105] | |
| Bone morphogenetic protein (BMP-2) | BMSCs | Modified BMSCs loaded onto β-TCP cylinder and implanted into core tract from CD | Increased amounts of new bone and higher maximum compressive strength and bone density. | [106] |
| BMP-2 and BMP-14 | BMP-laden collagen scaffolds transplanted following CD | BMP-14 loaded scaffolds improved bony remodeling of the necrotic area | [107] | |
| VEGF | VEGF injected continuously or through osmotic micropump | Reversal of osteonecrosis. | [108] | |
| Recombinant human fibroblast growth factor (rhFGF)-2 | rhFFGF-2 impregnated gelatin hydrogel administered locally | Increased Harris hip score. Reduction in pain level. | [109] | |
| VEGF | Deproteinized bone (DPB) with recombinant plasmid pcDNA3.1-hVEGF165 was implanted into the drilled tunnel of necrotic femoral head | Increased bone formation and capillary vessel regeneration | [110] | |
| VEGF | BMSCs | Transgenic autologous BMSCs implanted following CD | Enhanced bone reconstruction and blood vessel regeneration. | [111] |
| rhBMP-2 | Cavity was made using the light bulb technique and autologous cancellous bone combination of rhBMP-2 filled the cavity | May be effective in avoiding future THR in younger patients and improve the speed of bone repair (Lack of statistical significance) | [112] | |
| rhBMP-7 | Fibular graft harvested from femoral neck, sprinkled with rhBMP-7 and implanted in the tunnel | Increased Harris hip score. Decrease in pain. Retention in the sphericity of the femoral head. | [113] | |
| BMP-2 | Percutaneous intraosseous injection of BMP-2 and ibandronate | Decreased femoral head deformity and increased bone formation. | [114] | |
| HGF | MSCs | Transplantation of HGF-transgenic MSCs through CD tunnel | Increased the number of MSCs and osteogenic differentiation of MSCs. | [115] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murab, S.; Hawk, T.; Snyder, A.; Herold, S.; Totapally, M.; Whitlock, P.W. Tissue Engineering Strategies for Treating Avascular Necrosis of the Femoral Head. Bioengineering 2021, 8, 200. https://doi.org/10.3390/bioengineering8120200
Murab S, Hawk T, Snyder A, Herold S, Totapally M, Whitlock PW. Tissue Engineering Strategies for Treating Avascular Necrosis of the Femoral Head. Bioengineering. 2021; 8(12):200. https://doi.org/10.3390/bioengineering8120200
Chicago/Turabian StyleMurab, Sumit, Teresa Hawk, Alexander Snyder, Sydney Herold, Meghana Totapally, and Patrick W. Whitlock. 2021. "Tissue Engineering Strategies for Treating Avascular Necrosis of the Femoral Head" Bioengineering 8, no. 12: 200. https://doi.org/10.3390/bioengineering8120200
APA StyleMurab, S., Hawk, T., Snyder, A., Herold, S., Totapally, M., & Whitlock, P. W. (2021). Tissue Engineering Strategies for Treating Avascular Necrosis of the Femoral Head. Bioengineering, 8(12), 200. https://doi.org/10.3390/bioengineering8120200