Tissue-Derived Biological Particles Restore Cornea Properties in an Enzyme-Mediated Corneal Ectatic Model

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Preparation of TDP-Suspended Medium
2.2. Ectatic Corneal (KC) Culture in TDP-Suspended Medium
2.3. Optical Coherent Tomography (OCT)
2.4. Transmission Electron Microscopy
2.5. Image Analysis
2.6. Tensile Test
2.7. Differential Scanning Calorimetry (DSC)
2.8. Gene Expression
2.9. Statistical Analysis
3. Results
3.1. TDP Treatment Restored Corneal Fibril Density
3.2. TDP Treatment Enhanced Corneal Tensile Strength And Thermal Stability
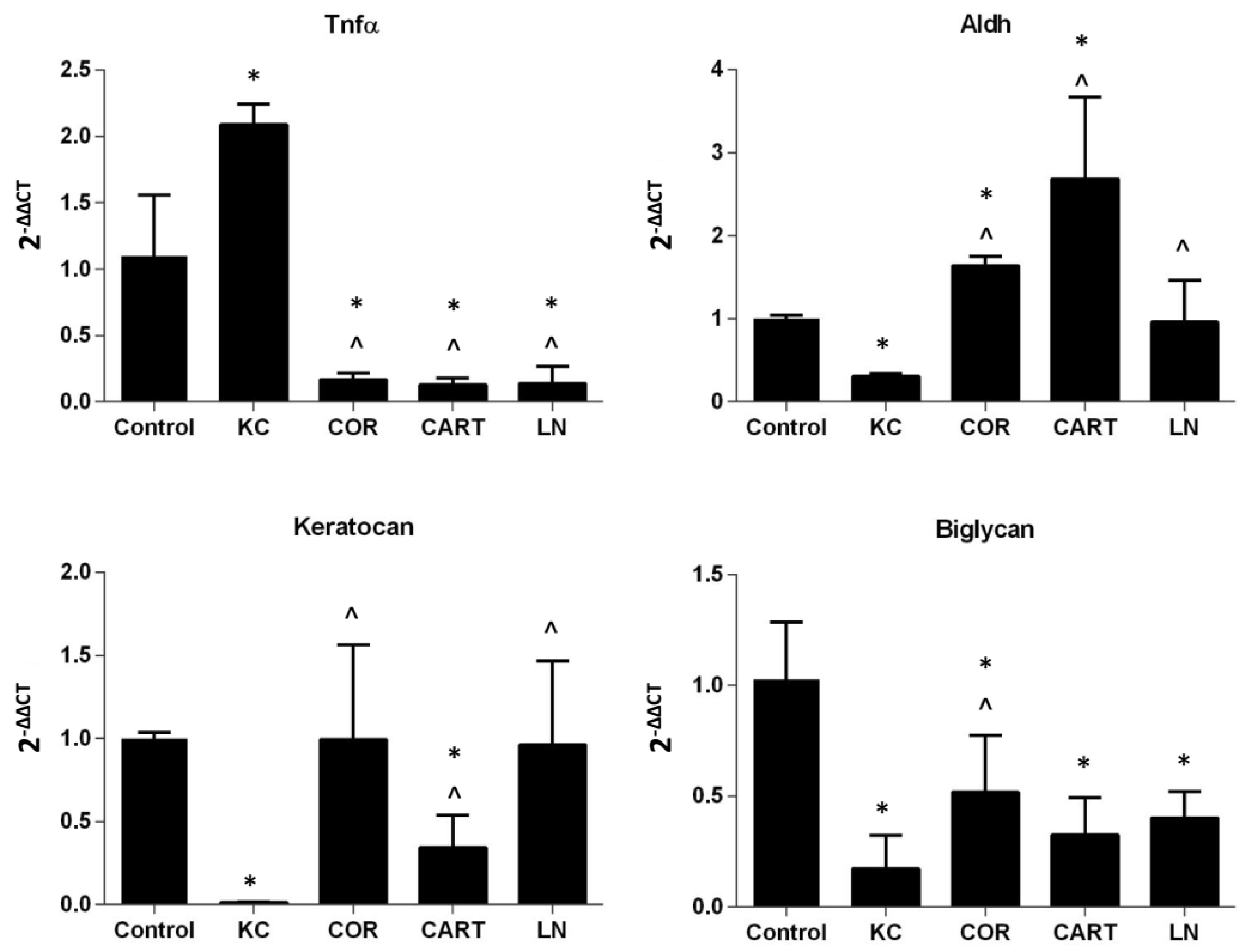
3.3. TDP Treatments Maintain Keratocytes Phenotype
4. Discussion
Author Contributions
Funding
Acknowledgements
Conflicts of Interest
References
- Xuan, M.; Wang, S.; Liu, X.; He, Y.; Li, Y.; Zhang, Y. Proteins of the corneal stroma: Importance in visual function. Cell Tissue Res. 2016, 364, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Roberts, C.J.; Dupps, W.J., Jr. Biomechanics of corneal ectasia and biomechanical treatments. J. Cataract Refract. Surg. 2014, 40, 991–998. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, S.; Bron, A.J.; Salvi, S.M.; Hawksworth, N.R.; Tuft, S.J.; Meek, K.M. Ultrastructural analysis of collagen fibrils and proteoglycans in keratoconus. Acta Ophthalmol. 2008, 86, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Meek, K.M.; Tuft, S.J.; Huang, Y.; Gill, P.S.; Hayes, S.; Newton, R.H.; Bron, A.J. Changes in collagen orientation and distribution in keratoconus corneas. Investig. Ophthalmol. Vis. Sci. 2005, 46, 1948–1956. [Google Scholar] [CrossRef] [PubMed]
- Keating, A.; Pineda, R., 2nd; Colby, K. Corneal cross linking for keratoconus. Semin. Ophthalmol. 2010, 25, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Wollensak, G.; Spoerl, E.; Seiler, T. Stress-strain measurements of human and porcine corneas after riboflavin-ultraviolet-A-induced cross-linking. J. Cataract Refract. Surg. 2003, 29, 1780–1785. [Google Scholar] [CrossRef]
- Wollensak, G.; Spoerl, E.; Wilsch, M.; Seiler, T. Endothelial cell damage after riboflavin-ultraviolet-A treatment in the rabbit. J. Cataract Refract. Surg. 2003, 29, 1786–1790. [Google Scholar] [CrossRef]
- Dhawan, S.; Rao, K.; Natrajan, S. Complications of corneal collagen cross-linking. J. Ophthalmol. 2011, 2011, 869015. [Google Scholar] [CrossRef] [PubMed]
- Michelacci, Y.M. Collagens and proteoglycans of the corneal extracellular matrix. Braz. J. Med. Biol. Res. 2003, 36, 1037–1046. [Google Scholar] [CrossRef]
- Hassell, J.R.; Cintron, C.; Kublin, C.; Newsome, D.A. Proteoglycan changes during restoration of transparency in corneal scars. Arch Biochem. Biophys. 1983, 222, 362–369. [Google Scholar] [CrossRef]
- Metzler, K.M.; Roberts, C.J.; Mahmoud, A.M.; Agarwal, G.; Liu, J. Ex Vivo Transepithelial Collagen Cross-linking in Porcine and Human Corneas Using Human Decorin Core Protein. J. Refract. Surg. 2016, 32, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Sady, C.; Khosrof, S.; Nagaraj, R. Advanced Maillard reaction and crosslinking of corneal collagen in diabetes. Biochem. Biophys. Res. Commun. 1995, 214, 793–797. [Google Scholar] [CrossRef] [PubMed]
- Pati, F.; Jang, J.; Ha, D.-H.; Kim, S.W.; Rhie, J.-W.; Shim, J.-H.; Kim, D.-H.; Cho, D.-W. Printing three-dimensional tissue analogues with decellularized extracellular matrix bioink. Nat. Commun. 2014, 5, 3935. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.W.; Solorio, L.D.; Alsberg, E. Decellularized tissue and cell-derived extracellular matrices as scaffolds for orthopaedic tissue engineering. Biotechnol. Adv. 2014, 32, 462–484. [Google Scholar] [CrossRef] [PubMed]
- Badylak, S.F. Xenogeneic extracellular matrix as a scaffold for tissue reconstruction. Transpl. Immunol. 2004, 12, 367–377. [Google Scholar] [CrossRef] [PubMed]
- Rohaina, C.M.; Then, K.Y.; Ng, A.M.H.; Halim, W.H.W.A.; Zahidina, A.Z.M.; Saimac, A.; Idrus, R.B.H. Reconstruction of limbal stem cell deficient corneal surface with induced human bone marrow mesenchymal stem cells on amniotic membrane. Transl. Res. 2014, 163, 200–210. [Google Scholar] [CrossRef]
- Vlasov, A.; Sia, R.K.; Ryan, D.S.; Mines, M.J.; Stutzman, R.D.; Rivers, B.A.; Tseng, S.C.G.; Bower, K.S. Sutureless cryopreserved amniotic membrane graft and wound healing after photorefractive keratectomy. J. Cataract Refract. Surg. 2016, 42, 435–443. [Google Scholar] [CrossRef]
- Gattazzo, F.; Urciuolo, A.; Bonaldo, P. Extracellular matrix: A dynamic microenvironment for stem cell niche. Biochim. Biophys. Acta 2014, 1840, 2506–2519. [Google Scholar] [CrossRef]
- Swinehart, I.T.; Badylak, S.F. Extracellular matrix bioscaffolds in tissue remodeling and morphogenesis. Dev. Dyn. 2016, 245, 351–360. [Google Scholar] [CrossRef]
- Beachley, V.Z.; Wolf, M.T.; Sadtler, K.; Manda, S.S.; Jacobs, H.; Blatchley, M.R.; Bader, J.S.; Pandey, A.; Pardoll, D.; Elisseeff, J.H. Tissue matrix arrays for high-throughput screening and systems analysis of cell function. Nat. Methods 2015, 12, 1197. [Google Scholar] [CrossRef]
- Wang, X.; Huang, Y.; Jastaneiah, S.; Majumdar, S.; Kang, J.U.; Yiu, S.C.; Stark, W.; Elisseeff, J.H. Protective Effects of Soluble Collagen during Ultraviolet-A Crosslinking on Enzyme-Mediated Corneal Ectatic Models. PLoS ONE 2015, 10, e0136999. [Google Scholar] [CrossRef]
- Kumar, R.J.; Kimble, R.M.; Boots, R.; Pegg, S.P. Treatment of partial-thickness burns: A prospective, randomized trial using TranscyteTM. ANZ J. Surg. 2004, 74, 622–626. [Google Scholar] [CrossRef]
- Sasse, K.C.; Brandt, J.; Lim, D.C.; Ackerman, E. Accelerated healing of complex open pilonidal wounds using MatriStem extracellular matrix xenograft: Nine cases. J. Surg. Case Rep. 2013, 2013. [Google Scholar] [CrossRef]
- Mostow, E.N.; Haraway, G.D.; Dalsing, M.; Hodde, J.P.; King, D.; OASIS Venus Ulcer Study Group. Effectiveness of an extracellular matrix graft (OASIS Wound Matrix) in the treatment of chronic leg ulcers: A randomized clinical trial. J. Vasc. Surg. 2005, 41, 837–843. [Google Scholar] [CrossRef]
- Ashraf, N.N.; Adhi, M.I. Outcome of application of amniotic membrane graft in ocular surface disorders. J. Pak. Med. Assoc. 2017, 67, 1045–1049. [Google Scholar]
- Wang, X.; Majumdar, S.; Ma, G.; Sohn, J.; Yiu, S.C.; Stark, W.; Al-Qarni, A.; Edward, D.P.; Elisseeff, J.H. Chondroitin Sulfate–Based Biocompatible Crosslinker Restores Corneal Mechanics and Collagen Alignment. Investig. Ophthalmol. Vis. Sci. 2017, 58, 3887–3895. [Google Scholar] [CrossRef]
- Dyrlund, T.F.; Poulsen, E.T.; Scavenius, C.; Nikolajsen, C.L.; Thøgersen, I.B.; Vorum, H.; Enghild, J.J. Human cornea proteome: Identification and quantitation of the proteins of the three main layers including epithelium, stroma, and endothelium. J. Proteome Res. 2012, 11, 4231–4239. [Google Scholar] [CrossRef]
- Zhen, E.Y.; Brittain, I.J.; Laska, D.A.; Mitchell, P.G.; Sumer, E.U.; Karsdal, M.A.; Duffin, K.L. Characterization of metalloprotease cleavage products of human articular cartilage. Arthritis Rheumatol. 2008, 58, 2420–2431. [Google Scholar] [CrossRef]
- Dzieciatkowska, M.; Wohlauer, M.V.; Moore, E.E.; Damle, S.; Peltz, E.; Campsen, J.; Kelher, M.; Silliman, C.; Banerjee, A.; Hansen, K.C. Proteomic analysis of human mesenteric lymph. Shock (Augusta Ga) 2011, 35, 331. [Google Scholar] [CrossRef]
- Chakravarti, S.; Petroll, W.M.; Hassell, J.R.; Jester, J.V.; Lass, J.H.; Paul, J.; Birk, D.E. Corneal opacity in lumican-null mice: Defects in collagen fibril structure and packing in the posterior stroma. Investig. Ophthalmol. Vis. Sci. 2000, 41, 3365–3373. [Google Scholar]
- Balasubramanian, S.A.; Mohan, S.; Pye, D.C.; Willcox, M.D.P. Proteases, proteolysis and inflammatory molecules in the tears of people with keratoconus. Acta Ophthalmol. 2012, 90, e303–e309. [Google Scholar] [CrossRef]
- Pahuja, N.; Kumar, N.R.; Shroff, R.; Shetty, R.; Nuijts, R.M.M.A.; Ghosh, A.; Sinha-Roy, A.; Chaurasia, S.S.; Mohan, R.R.; Ghosh, A. Differential Molecular Expression of Extracellular Matrix and Inflammatory Genes at the Corneal Cone Apex Drives Focal Weakening in Keratoconus. Investig. Ophthalmol. Vis. Sci. 2016, 57, 5372–5382. [Google Scholar] [CrossRef]
- Mootha, V.V.; Kanoff, J.M.; Shankardas, J.; Dimitrijevich, S. Marked reduction of alcohol dehydrogenase in keratoconus corneal fibroblasts. Mol. Vis. 2009, 15, 706–712. [Google Scholar]
- Garcia, B.; García-Suárez, O.; Merayo-Lloves, J.; Alcalde, I.; Alfonso, J.F.; Cueto, L.F.V.; Meana, Á.; Vázquez, F.; Quirós, L.M. Differential Expression of Proteoglycans by Corneal Stromal Cells in Keratoconus. Investig. Ophthalmol. Vis. Sci. 2016, 57, 2618–2628. [Google Scholar] [CrossRef]
- Yin, H.; Lu, Q.; Wang, X.; Majumdar, S.; Jun, A.S.; Stark, W.J.; Grant, M.P.; Elisseeff, J.H. Tissue-derived microparticles reduce inflammation and fibrosis in cornea wounds. Acta Biomater. 2019, 85, 192–202. [Google Scholar] [CrossRef]
- Sadtler, K.; Estrellas, K.; Allen, B.W.; Wolf, M.T.; Fan, H.; Tam, A.J.; Patel, C.H.; Luber, B.S.; Wang, H.; Wagner, K.R.; et al. Developing a pro-regenerative biomaterial scaffold microenvironment requires T helper 2 cells. Science 2016, 352, 366–370. [Google Scholar] [CrossRef]
- Tewari-Singh, N.; Goswami, D.G.; Kant, R.; Ammar, D.A.; Kumar, D.; Enzenauer, R.W.; Casillas, R.P.; Croutch, C.R.; Petrash, J.M.; Agarwal, R. Histopathological and Molecular Changes in the Rabbit Cornea from Arsenical Vesicant Lewisite Exposure. Toxicol. Sci. 2017, 160, 420–438. [Google Scholar] [CrossRef]
- Nakamura, H.; Riley, F.; Sakai, H.; Rademaker, W.; Yue, B.Y.J.T.; Edward, D.P. Histopathological and immunohistochemical studies of lenticules after epikeratoplasty for keratoconus. Br. J. Ophthalmol. 2005, 89, 841–846. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gapdh | Forward | 5′-CTCTGGAGTGGATGTT-3′ |
| Reverse | 5′-CCATGGGTGGAATCATACTG-3′ | |
| Tnfα | Forward | 5′-GTAGTAGCAAACCCGCAAGT-3′ |
| Reverse | 5′-GGTTGTCCGTGAGCTTCAT-3′ | |
| Keratocan | Forward | 5′-AGTACCAACAAGCTTCAGCC-3′ |
| Reverse | 5′-ACCCAGATGACGAAACATATT-3′ | |
| Aldh | Forward | 5′-GACGATAACTGCAGAGCACG-3′ |
| Reverse | 5′-ACTCATTCGACAAGCAGACAG-3′ | |
| Biglycan | Forward | 5′-GCATCCCCAAAGATCTGCC-3′ |
| Reverse | 5′-CAACTTGGAGTATCGGAGCAG-3′ |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yin, H.; Wang, X.; Majumdar, S.; Sohn, J.; Kim, B.-J.; Stark, W.; Elisseeff, J.H. Tissue-Derived Biological Particles Restore Cornea Properties in an Enzyme-Mediated Corneal Ectatic Model. Bioengineering 2019, 6, 90. https://doi.org/10.3390/bioengineering6040090
Yin H, Wang X, Majumdar S, Sohn J, Kim B-J, Stark W, Elisseeff JH. Tissue-Derived Biological Particles Restore Cornea Properties in an Enzyme-Mediated Corneal Ectatic Model. Bioengineering. 2019; 6(4):90. https://doi.org/10.3390/bioengineering6040090
Chicago/Turabian StyleYin, Hongbo, Xiaokun Wang, Shoumyo Majumdar, Jeeyeon Sohn, Byung-Jin Kim, Walter Stark, and Jennifer H. Elisseeff. 2019. "Tissue-Derived Biological Particles Restore Cornea Properties in an Enzyme-Mediated Corneal Ectatic Model" Bioengineering 6, no. 4: 90. https://doi.org/10.3390/bioengineering6040090
APA StyleYin, H., Wang, X., Majumdar, S., Sohn, J., Kim, B.-J., Stark, W., & Elisseeff, J. H. (2019). Tissue-Derived Biological Particles Restore Cornea Properties in an Enzyme-Mediated Corneal Ectatic Model. Bioengineering, 6(4), 90. https://doi.org/10.3390/bioengineering6040090