Laboratory Automation in Clinical Microbiology


Abstract
:
{kind=link}
1. What is Laboratory Automation?
2. Literature Search
3. Definitions
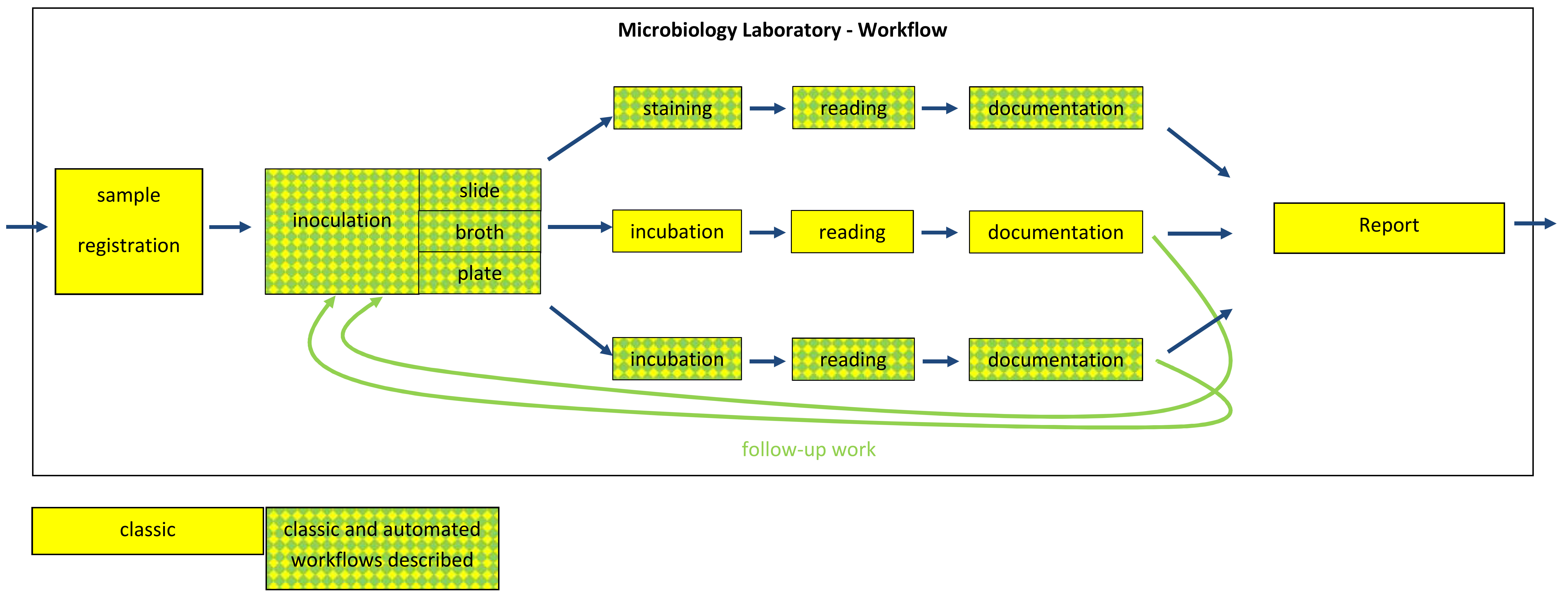
3.1. Workflow
3.2. Lean
3.3. Time to Result
3.4. Time to Report
3.5. Classic System vs. Automation
3.6. Total Lab Automation
3.7. What Is Quality?
4. Hardware
5. Workflow
5.1. Quick Tests for Species Identification
5.2. Quick Tests for Susceptibility Testing
5.3. Agardilution—Susceptibility Testing
5.4. Effects of Laboratory Automation on Incubation Times of Agar Plates
5.4.1. Incubation Times of Chromogenic Plates
5.4.2. Incubation Times of Agar Diffusion Plates
5.5. Effects of Laboratory Automation on Special Sample Types
5.5.1. Effects on Blood Culture
5.5.2. Effects on Urines
5.6. Effects of Laboratory Automation on Time to Report
5.7. Effects of Laboratory Automation on Quality
5.8. Automated Reading
6. IT
6.1. TLA Operating System
6.2. Interface
6.3. LIS
7. Wish List
7.1. Which Steps Are Still Manual?
- (a)
- filling up the machine with consumables;
- (b)
- sorting of sample containers in specialized racks;
- (c)
- loading and unloading of racks into the specimen processor;
- (d)
- follow-up work (that is identification, susceptibility testing, subculture);
- (e)
- reading of plates;
- (f)
- Generating reports for the clinicians;
- (g)
- waste management;
- (a)
- sample registration in the laboratory;
- (b)
- incubation, assessment and documentation of broths;
- (c)
- staining, assessment and documentation of slides;
- (d)
- incubation and further processing of anaerobes and microaerophilic bacteria;
7.2. Which Data Is Needed for Optimization of Automation?
7.3. Do We Need Automated Specimen Storage?
8. Discussion
Funding
Conflicts of Interest
Abbreviations
| ID | identification |
| AST | antimicrobial susceptibility testing |
| MRSA | methicillin-resistant Staphylococcus aureus |
| VRE | vancomycin-resistant enterococci |
| MDRGN | multi-drug resistant gram-negative bacteria |
| MIC | minimal inhibitory concentration |
| TLA | total lab(oratory) automation |
| MALDI-TOF MS | matrix assisted laser desorption ionization—time of flight mass spectrometry |
| LIS | laboratory information system |
References
- Groover, P.M. Fundamentals of Modern Manufacturing: Material, Processes and Systems, 4th ed.; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2010. [Google Scholar]
- Wikipedia. Workflow. Available online: https: //en.wikipedia.org/wiki/Workflow (accessed on 12 September 2018).
- Womack, J.P.; Jones, D.T.; Roos, D. The Machine that Changed the World; Free Press: New York, NY, USA, 1990. [Google Scholar]
- Antierens, A.; Beeckman, D.; Verhaeghe, S.; Myny, D.; Van Hecke, A. How much of toyota’s philosophy is embedded in health care at the organisational level? A review. J. Nurs. Manag. 2018, 26, 348–357. [Google Scholar] [CrossRef] [PubMed]
- Toussaint, J.S.; Berry, L.L. The promise of lean in health care. Mayo Clin. Proc. 2013, 88, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Raab, S.S.; Andrew-Jaja, C.; Condel, J.L.; Dabbs, D.J. Improving papanicolaou test quality and reducing medical errors by using toyota production system methods. Am. J. Obstet. Gynecol. 2006, 194, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Serrano, L.; Hegge, P.; Sato, B.; Richmond, B.; Stahnke, L. Using lean principles to improve quality, patient safety, and workflow in histology and anatomic pathology. Adv. Anat. Pathol. 2010, 17, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Persoon, T.J.; Zaleski, S.; Frerichs, J. Improving preanalytic processes using the principles of lean production (toyota production system). Am. J. Clin. Pathol. 2006, 125, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Burkitt, K.H.; Mor, M.K.; Jain, R.; Kruszewski, M.S.; McCray, E.E.; Moreland, M.E.; Muder, R.R.; Obrosky, D.S.; Sevick, M.A.; Wilson, M.A.; et al. Toyota production system quality improvement initiative improves perioperative antibiotic therapy. Am. J. Manag. Care 2009, 15, 633–642. [Google Scholar] [PubMed]
- Businessdictionary. Quality. Available online: http://www.businessdictionary.com/definition/quality.html (accessed on 12 September 2018).
- Quality.org. Quality. Available online: https://www.quality.org/article/what-quality (accessed on 12 September 2018).
- Croxatto, A.; Prod’hom, G.; Faverjon, F.; Rochais, Y.; Greub, G. Laboratory automation in clinical bacteriology: What system to choose? Clin. Microbiol. Infect. 2016, 22, 217–235. [Google Scholar] [CrossRef] [PubMed]
- Dauwalder, O.; Landrieve, L.; Laurent, F.; de Montclos, M.; Vandenesch, F.; Lina, G. Does bacteriology laboratory automation reduce time to results and increase quality management? Clin. Microbiol. Infect. 2016, 22, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Homem de Mello de Souza, H.A.; Dalla-Costa, L.M.; Vicenzi, F.J.; Camargo de Souza, D.; Riedi, C.A.; Filho, N.A.; Pilonetto, M. Maldi-tof: A useful tool for laboratory identification of uncommon glucose non-fermenting gram-negative bacteria associated with cystic fibrosis. J. Med. Microbiol. 2014, 63, 1148–1153. [Google Scholar] [CrossRef] [PubMed]
- Jamal, W.; Albert, M.J.; Rotimi, V.O. Real-time comparative evaluation of Biomerieux Vitek MS versus Bruker Microflex MS, two matrix-assisted laser desorption-ionization time-of-flight mass spectrometry systems, for identification of clinically significant bacteria. BMC Microbiol. 2014, 14, 289. [Google Scholar] [CrossRef] [PubMed]
- Argemi, X.; Riegel, P.; Lavigne, T.; Lefebvre, N.; Grandpre, N.; Hansmann, Y.; Jaulhac, B.; Prevost, G.; Schramm, F. Implementation of matrix-assisted laser desorption ionization-time of flight mass spectrometry in routine clinical laboratories improves identification of coagulase-negative staphylococci and reveals the pathogenic role of staphylococcus lugdunensis. J. Clin. Microbiol. 2015, 53, 2030–2036. [Google Scholar] [CrossRef] [PubMed]
- Patel, R. MALDI-TOF MS for the diagnosis of infectious diseases. Clin. Chem. 2015, 61, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Sieradzki, K.; Albrecht, V.; McAllister, S.; Lin, W.; Stuchlik, O.; Limbago, B.; Pohl, J.; Kamile Rasheed, J. Evaluation of the Biotyper MALDI-TOF MS system for identification of staphylococcus species. J. Microbiol. Methods 2015, 117, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Ayeni, F.A.; Andersen, C.; Norskov-Lauritsen, N. Comparison of growth on mannitol salt agar, matrix-assisted laser desorption/ionization time-of-flight mass spectrometry, VITEK((r)) 2 with partial sequencing of 16s rrna gene for identification of coagulase-negative staphylococci. Microbial Pathogenes. 2017, 105, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Trevisoli, L.E.; Bail, L.; Rodrigues, L.S.; Conte, D.; Palmeiro, J.K.; Dalla-Costa, L.M. Matrix-assisted laser desorption ionization-time of flight: A promising alternative method of identifying the major coagulase-negative staphylococci species. Revista da Sociedade Brasileira de Medicina Tropical 2018, 51, 85–87. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Camacho, J.L.; Calva-Espinosa, D.Y.; Leal-Leyva, Y.Y.; Elizalde-Olivas, D.C.; Campos-Romero, A.; Alcantar-Fernandez, J. Transformation from a conventional clinical microbiology laboratory to full automation. Lab. Med. 2017, 49, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Bauer, A.W.; Kirby, W.M.; Sherris, J.C.; Turck, M. Antibiotic susceptibility testing by a standardized single disk method. Am. J. Clin. Pathol. 1966, 45, 493–496. [Google Scholar] [CrossRef] [PubMed]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters; Version 8.1, valid from 2018-05-15; EUCAST: Basel, Switzerland, 2018. [Google Scholar]
- Hombach, M.; Jetter, M.; Blochliger, N.; Kolesnik-Goldmann, N.; Bottger, E.C. Fully automated disc diffusion for rapid antibiotic susceptibility test results: A proof-of-principle study. J. Antimicrob. Chemother. 2017, 72, 1659–1668. [Google Scholar] [CrossRef] [PubMed]
- Burckhardt, I.; Panitz, J.; Burckhardt, F.; Zimmermann, S. Identification of streptococcus pneumoniae: Development of a standardized protocol for optochin susceptibility testing using total lab automation. Biomed. Res. Int. 2017, 2017, 4174168. [Google Scholar] [CrossRef] [PubMed]
- Heather, C.S.; Maley, M. Automated direct screening for resistance of gram-negative blood cultures using the bd kiestra workcell. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 117–125. [Google Scholar] [CrossRef] [PubMed]
- The European Committee on Antimicrobial Susceptibility Testing. Eucast Frequently Asked Questions; EUCAST: Basel, Switzerland, 2018. [Google Scholar]
- Jonasson, E.; Matuschek, E.; Sundqvist, M.V.; Kahlmeter, M. Tentative breakpoints for rapid antimicrobial susceptibility testing with disk diffusion tests direct from positive blood cultures for Escherichia coli, Klebsiella pneumoniae, Staphylococcus aureus and Streptococcus pneumoniae. In Proceedings of the Twenty-sixth European Congress of Clinical Microbiology and Infectious Diseases (ECCMID 2016), European Society of Clinical Microbiology and Infectious Diseases Amsterdam, Amsterdam, The Netherlands, 9–12 April 2016. [Google Scholar]
- Froding, I.; Vondracek, M.; Giske, C.G. Rapid eucast disc diffusion testing of mdr escherichia coli and klebsiella pneumoniae: Inhibition zones for extended-spectrum cephalosporins can be reliably read after 6 h of incubation. J. Antimicrob. Chemother. 2017, 72, 1094–1102. [Google Scholar] [PubMed]
- Jonasson, E.; Matuschek, E.; Kahlmeter, M. Proposed breakpoints for EUCAST rapid antimicrobial susceptibility testing with disk-dissusion tests direct froom positive blood cultures for Pseudomonas aeruginosa, Haemophilus influenzae, Enterococcus faecalis and Enterococcus faecium. In Proceedings of the Twenty-eighth European Congress of Clinical Microbiology and Infectious Diseases (ECCMID 2018), Madrid, Spain, 21–24 April 2018; European Society of Clinical Microbiology and Infectious Diseases: Madrid, Spain, 2018. [Google Scholar]
- De Socio, G.V.; Di Donato, F.; Paggi, R.; Gabrielli, C.; Belati, A.; Rizza, G.; Savoia, M.; Repetto, A.; Cenci, E.; Mencacci, A. Laboratory automation reduces time to report of positive blood cultures and improves management of patients with bloodstream infection. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 2313–2322. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.; Nurjadi, D.; Horner, S.; Heeg, K.; Zimmermann, S.; Burckhardt, I. Significant increase in cultivation of gardnerella vaginalis, alloscardovia omnicolens, actinotignum schaalii, and actinomyces spp. In urine samples with total laboratory automation. Eur. J. Clin Microbiol. Infect. Dis. 2018, 37, 1305–13011. [Google Scholar] [CrossRef] [PubMed]
- Lainhart, W.; Burnham, C.A. Enhanced recovery of fastidious organisms from urine culture in the setting of total laboratory automation. J. Clin. Microbiol. 2018, 56, 5–46. [Google Scholar] [CrossRef] [PubMed]
- Theparee, T.; Das, S.; Thomson, R.B., Jr. Total laboratory automation and matrix-assisted laser desorption ionization-time of flight mass spectrometry improve turnaround times in the clinical microbiology laboratory: A retrospective analysis. J. Clin. Microbiol. 2018, 56, e01242-e17. [Google Scholar] [CrossRef] [PubMed]
- Yarbrough, M.L.; Lainhart, W.; McMullen, A.R.; Anderson, N.W.; Burnham, C.D. Impact of total laboratory automation on workflow and specimen processing time for culture of urine specimens. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 2405–2411. [Google Scholar] [CrossRef] [PubMed]
- Graham, M.; Tilson, L.; Streitberg, R.; Hamblin, J.; Korman, T.M. Improved standardization and potential for shortened time to results with bd kiestra total laboratory automation of early urine cultures: A prospective comparison with manual processing. Diagn. Microbiol. Infec. Dis. 2016, 86, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Burckhardt, I.; Horner, S.; Burckhardt, F.; Zimmermann, S. Detection of MRSA in nasal swabs-marked reduction of time to report for negative reports by substituting classical manual workflow with total lab automation. Eur. J Clin. Microbiol. Infect. Dis. 2018, 37, 1745–1751. [Google Scholar] [CrossRef] [PubMed]
- Croxatto, A.; Dijkstra, K.; Prod’hom, G.; Greub, G. Comparison of inoculation with the inoqula and wasp automated systems with manual inoculation. J. Clin. Microbiol. 2015, 53, 2298–2307. [Google Scholar] [CrossRef] [PubMed]
- Mischnik, A.; Trampe, M.; Zimmermann, S. Evaluation of the impact of automated specimen inoculation, using previ isola, on the quality of and technical time for stool cultures. Ann. Lab. Med. 2015, 35, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Froment, P.; Marchandin, H.; Vande Perre, P.; Lamy, B. Automated versus manual sample inoculations in routine clinical microbiology: A performance evaluation of the fully automated inoqula instrument. J. Clin. Microbiol. 2014, 52, 796–802. [Google Scholar] [CrossRef] [PubMed]
- Faron, M.L.; Buchan, B.W.; Vismara, C.; Lacchini, C.; Bielli, A.; Gesu, G.; Liebregts, T.; van Bree, A.; Jansz, A.; Soucy, G.; et al. Automated scoring of chromogenic media for detection of methicillin-resistant staphylococcus aureus by use of wasplab image analysis software. J. Clin. Microbiol. 2016, 54, 620–624. [Google Scholar] [CrossRef] [PubMed]
- Faron, M.L.; Buchan, B.W.; Coon, C.; Liebregts, T.; van Bree, A.; Jansz, A.R.; Soucy, G.; Korver, J.; Ledeboer, N.A. Automatic digital analysis of chromogenic media for vancomycin-resistant-enterococcus screens using copan wasplab. J. Clin. Microbiol. 2016, 54, 2464–2469. [Google Scholar] [CrossRef] [PubMed]
- Glasson, J.; Hill, R.; Summerford, M.; Olden, D.; Papadopoulos, F.; Young, S.; Giglio, S. Multicenter evaluation of an image analysis device (apas): Comparison between digital image and traditional plate reading using urine cultures. Annals Lab. Med. 2017, 37, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Glasson, J.; Hill, R.; Summerford, M.; Giglio, S. Evaluation of an image analysis device (apas) for screening urine cultures. J. Clin. Microbiol. 2016, 54, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Croxatto, A.; Marcelpoil, R.; Orny, C.; Morel, D.; Prod’hom, G.; Greub, G. Towards automated detection, semi-quantification and identification of microbial growth in clinical bacteriology: A proof of concept. Biomed. J. 2017, 40, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Bourbeau, P.P.; Ledeboer, N.A. Automation in clinical microbiology. J. Clin. Microbiol. 2013, 51, 1658–1665. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.P.; Kang, A.D.; Kirby, J.E. Automated interpretation of blood culture gram stains by use of a deep convolutional neural network. J. Clin. Microbiol. 2018, 56, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Strittmatter, N.; Rebec, M.; Jones, E.A.; Golf, O.; Abdolrasouli, A.; Balog, J.; Behrends, V.; Veselkov, K.A.; Takats, Z. Characterization and identification of clinically relevant microorganisms using rapid evaporative ionization mass spectrometry. Anal. Chem. 2014, 86, 6555–6562. [Google Scholar] [CrossRef] [PubMed]
- Van den Poel, B.; Klak, A.; Desmet, S.; Verhaegen, J. How small modifications in laboratory workflow of blood cultures can have a significant impact on time to results. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1753–1760. [Google Scholar] [CrossRef] [PubMed]
- Broyer, P.; Perrot, N.; Rostaing, H.; Blaze, J.; Pinston, F.; Gervasi, G.; Charles, M.H.; Dachaud, F.; Dachaud, J.; Moulin, F.; et al. An automated sample preparation instrument to accelerate positive blood cultures microbial identification by maldi-tof mass spectrometry (vitek((r))ms). Front. Microbiol. 2018, 9, 911. [Google Scholar] [CrossRef] [PubMed]
- Timbrook, T.T.; Morton, J.B.; McConeghy, K.W.; Caffrey, A.R.; Mylonakis, E.; LaPlante, K.L. The effect of molecular rapid diagnostic testing on clinical outcomes in bloodstream infections: A systematic review and meta-analysis. Clin. Infect. Dis. 2017, 64, 15–23. [Google Scholar] [CrossRef] [PubMed]
© 2018 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burckhardt, I. Laboratory Automation in Clinical Microbiology. Bioengineering 2018, 5, 102. https://doi.org/10.3390/bioengineering5040102
Burckhardt I. Laboratory Automation in Clinical Microbiology. Bioengineering. 2018; 5(4):102. https://doi.org/10.3390/bioengineering5040102
Chicago/Turabian StyleBurckhardt, Irene. 2018. "Laboratory Automation in Clinical Microbiology" Bioengineering 5, no. 4: 102. https://doi.org/10.3390/bioengineering5040102
APA StyleBurckhardt, I. (2018). Laboratory Automation in Clinical Microbiology. Bioengineering, 5(4), 102. https://doi.org/10.3390/bioengineering5040102