
Assessment of Radiation Attenuation Properties in Dental Implants Using Monte Carlo Method †


Abstract
1. Introduction
2. Materials and Methods
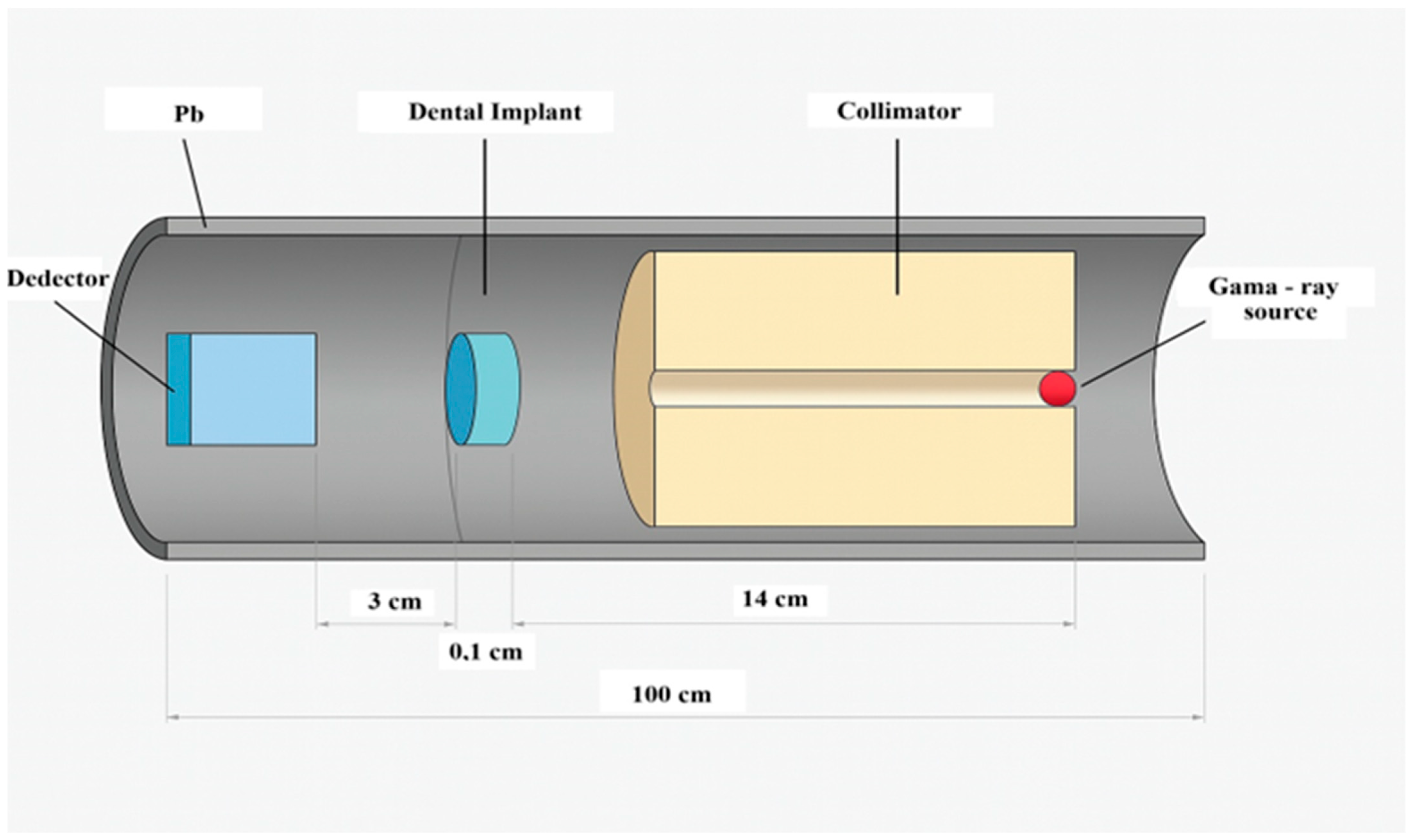
2.1. Study Design
2.2. Analysis
3. Results

{kind=link}
{kind=link}
{kind=link}
| Energy (keV) | NTA Implant (cm2 g−1) | Bilimplant (cm2 g−1) | Z-Systems (cm2 g−1) | Teeth [32] | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| XCOM | MCNP6 | %R.D | XCOM | MCNP6 | %R.D | XCOM | MCNP6 | %R.D | ||
| 50 | 1.173 | 1.173 | 0.033 | 0.915 | 0.915 | 0.046 | 4.613 | 4.615 | 0.034 | |
| 54 | 0.963 | 0.964 | 0.039 | 0.759 | 0.760 | 0.064 | 3.742 | 3.746 | 0.100 | |
| 59.5 | 0.758 | 0.758 | 0 | 0.606 | 0.606 | 0.132 | 2.877 | 2.880 | 0.104 | 0.35 ± 0.02 |
| 60 | 0.743 | 0.743 | 0.030 | 0.595 | 0.594 | 0.154 | 2.813 | 2.816 | 0.101 | |
| 64 | 0.638 | 0.638 | 0.053 | 0.517 | 0.517 | 0.068 | 2.365 | 2.367 | 0.088 | |
| 70 | 0.522 | 0.521 | 0.069 | 0.430 | 0.430 | 0.027 | 1.863 | 1.865 | 0.087 | |
| 75 | 0.451 | 0.450 | 0.146 | 0.377 | 0.377 | 0.062 | 1.554 | 1.554 | 0.019 | |
| 80 | 0.396 | 0.396 | 0.069 | 0.335 | 0.335 | 0.045 | 1.314 | 1.314 | 0.032 | |
| 81 | 0.386 | 0.386 | 0.047 | 0.328 | 0.320 | 0.002 | 1.273 | 1.273 | 0.010 | 0.22 ± 0.01 |
| 84 | 0.360 | 0.360 | 0.027 | 0.309 | 0.309 | 0.021 | 1.160 | 1.160 | 0.003 | |
| 90 | 0.318 | 0.318 | 0.032 | 0.277 | 0.277 | 0.077 | 0.975 | 0.974 | 0.116 | |
| 95 | 0.290 | 0.290 | 0.039 | 0.256 | 0.256 | 0.273 | 0.853 | 0.852 | 0.125 | |
| 100 | 0.267 | 0.268 | 0.306 | 0.238 | 0.239 | 0.368 | 0.753 | 0.753 | 0.078 | |
| Energy (keV) | NTA Implant (cm−1) | Bilimplant (cm−1) | Z-Systems (cm−1) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| XCOM | MCNP6 | %R.D | XCOM | MCNP6 | %R.D | XCOM | MCNP6 | %R.D | |
| 50 | 5.194 | 5.194 | 0 | 0.278 | 0.280 | 0.883 | 27.909 | 27.918 | 0.034 |
| 54 | 4.264 | 4.269 | 0.104 | 0.228 | 0.229 | 0.724 | 22.639 | 22.662 | 0.100 |
| 59.5 | 3.357 | 3.357 | 0 | 2.735 | 2.731 | 0.132 | 17.406 | 17.424 | 0.104 |
| 60 | 3.290 | 3.290 | 0 | 0.200 | 0.202 | 0.699 | 17.019 | 17.036 | 0.101 |
| 64 | 2.825 | 2.825 | 0 | 0.183 | 0.185 | 0.774 | 14.308 | 14.321 | 0.088 |
| 70 | 2.311 | 2.307 | 0.192 | 0.172 | 0.173 | 0.798 | 11.271 | 11.281 | 0.087 |
| 75 | 1.997 | 1.993 | 0.222 | 0.163 | 0.164 | 0.791 | 9.402 | 9.403 | 0.019 |
| 80 | 1.753 | 1.753 | 0 | 0.156 | 0.157 | 0.634 | 7.950 | 7.952 | 0.032 |
| 81 | 1.710 | 1.710 | 0.046 | 1.480 | 1.480 | 0.002 | 7.702 | 7.701 | 0.010 |
| 84 | 1.594 | 1.594 | 0 | 0.151 | 0.152 | 0.644 | 7.018 | 7.018 | 0.003 |
| 90 | 1.408 | 1.408 | 0 | 0.146 | 0.147 | 0.637 | 5.897 | 5.890 | 0.116 |
| 95 | 1.284 | 1.284 | 0 | 0.142 | 0.143 | 0.768 | 5.160 | 5.154 | 0.125 |
| 100 | 1.182 | 1.187 | 0 | 0.138 | 0.139 | 0.824 | 4.557 | 4.553 | 0.078 |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CT | Computed tomography |
| CBCT | Cone-beam computed tomography |
| Ti | Titanium |
| MC | Monte Carlo |
| MCNP | Monte Carlo N-particle |
| MFP | Mean free path |
| TVL | Tenth-value layer |
| HVL | Half-value layer |
| ZiO2 | Zirconium dioxide |
| Al2O3 | Aluminum oxide |
| Y2O3 | Yttrium oxide |
| FOV | Field of view |
References
- Steigenga, J.T.; Al-Shammari, K.F.; Nociti, F.H.; Misch, C.E.; Wang, H.L. Dental Implant Design and Its Relationship to Long-Term Implant Success. Implant. Dent. 2003, 12, 306–317. [Google Scholar] [CrossRef] [PubMed]
- Schiegnitz, E.; Müller, L.K.; Sagheb, K.; Theis, L.; Cagiran, V.; Kämmerer, P.W.; Wegener, J.; Wagner, W.; Al-Nawas, B. Clinical Long-Term and Patient-Reported Outcomes of Dental Implants in Oral Cancer Patients. Int. J. Implant. Dent. 2021, 7, 93. [Google Scholar] [CrossRef]
- Adell, R. A 15-Year Study of Osseointegrated Implants in the Treatment of the Edentulous Jaw. Int. J. Oral Surg. 1981, 10, 387–416. [Google Scholar] [CrossRef]
- Van Oirschot, B.A.J.A.; Zhang, Y.; Alghamdi, H.S.; Cordeiro, J.M.; Nagay, B.E.; Barao, V.A.R.; De Avila, E.D.; Van Den Beucken, J.J.J.P. Surface Engineering for Dental Implantology: Favoring Tissue Responses Along the Implant. Tissue Eng. Part A 2022, 28, 555–572. [Google Scholar] [CrossRef]
- Thanissorn, C.; Guo, J.; Jing Ying Chan, D.; Koyi, B.; Kujan, O.; Khzam, N.; Miranda, L.A. Success Rates and Complications Associated with Single Immediate Implants: A Systematic Review. Dent. J. 2022, 10, 31. [Google Scholar] [CrossRef]
- Kirsch, A.; Ackermann, K.L. The IMZ Osteointegrated Implant System. Dent. Clin. N. Am. 1989, 33, 733–791. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Sennerby, L.; De Bruyn, H. Modern Implant Dentistry Based on Osseointegration: 50 Years of Progress, Current Trends and Open Questions. Periodontol. 2000 2017, 73, 7–21. [Google Scholar] [CrossRef] [PubMed]
- Cionca, N.; Hashim, D.; Mombelli, A. Zirconia Dental Implants: Where Are We Now, and Where Are We Heading? Periodontol. 2000 2017, 73, 241–258. [Google Scholar] [CrossRef]
- Schulze, R. CBCT Artefact-Burden of Zirconia-Based as Compared to Titanium Implants for Different Beam Energies: An Analytical Approach. Sci. Rep. 2022, 12, 15276. [Google Scholar] [CrossRef]
- Salian, S.S.; Subhadarsanee, C.P.; Patil, R.T.; Dhadse, P. V Radiographic Evaluation in Implant Patients: A Review. Cureus 2024, 16, e54783. [Google Scholar] [CrossRef]
- Almulhim, S.A.N.; Busaeed, A.R.A.; Alhaji, Y.B.; Sallam, J.A.; Aljuaid, A.S.E.; Eishan, A.A.M.; Alharbi, M.A.; Shehatah, A.U.; Asiri, M.H.M.; al Baqshi, H.A.; et al. Comparative study of different imaging modalities in assessing dental implant stability. J. Popul. Ther. Clin. Pharmacol. 2022, 29, 2743–2751. [Google Scholar] [CrossRef]
- Freitas, D.Q.; Fontenele, R.C.; Nascimento, E.H.L.; Vasconcelos, T.V.; Noujeim, M. Influence of Acquisition Parameters on the Magnitude of Cone Beam Computed Tomography Artifacts. Dentomaxillofac. Radiol. 2018, 47, 20180151. [Google Scholar] [CrossRef] [PubMed]
- Schulze, R.; Heil, U.; Groß, D.; Bruellmann, D.D.; Dranischnikow, E.; Schwanecke, U.; Schoemer, E. Artefacts in CBCT: A Review. Dentomaxillofac. Radiol. 2011, 40, 265–273. [Google Scholar] [CrossRef]
- Kovalchuk, O.; Ponton, A.; Filkowski, J.; Kovalchuk, I. Dissimilar Genome Response to Acute and Chronic Low-Dose Radiation in Male and Female Mice. Mutat. Res. Mol. Mech. Mutagen. 2004, 550, 59–72. [Google Scholar] [CrossRef] [PubMed]
- Van Gompel, G.; Van Slambrouck, K.; Defrise, M.; Batenburg, K.J.; De Mey, J.; Sijbers, J.; Nuyts, J. Iterative Correction of Beam Hardening Artifacts in CT. Med. Phys. 2011, 38, S36–S49. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Rahman, M.A.; Badawi, E.A.; Abdel-Hady, Y.L.; Kamel, N. Effect of Sample Thickness on the Measured Mass Attenuation Coefficients of Some Compounds and Elements for 59.54, 661.6 and 1332.5 KeV γ-Rays. Nucl. Instrum. Methods Phys. Res. A 2000, 447, 432–436. [Google Scholar] [CrossRef]
- Singh, K.; Kaur, G.; Sandhu, G.K.; Lark, B.S. Interaction of Photons with Some Solutions. Radiat. Phys. Chem. 2001, 61, 537–540. [Google Scholar] [CrossRef]
- Shakhreet, B.Z.; Chong, C.S.; Bandyopadhyay, T.; Bradley, D.A.; Tajuddin, A.A.; Shukri, A. Measurement of Photon Mass-Energy Absorption Coefficients of Paraffin Wax and Gypsum at 662 KeV. Radiat. Phys. Chem. 2003, 68, 757–764. [Google Scholar] [CrossRef]
- Ozdogan, H.; Kilicoglu, O.; Akman, F.; Agar, O. Comparison of Monte Carlo Simulations and Theoretical Calculations of Nuclear Shielding Characteristics of Various Borate Glasses Including Bi, V., Fe, and Cd. Appl. Radiat. Isot. 2022, 189, 110454. [Google Scholar] [CrossRef]
- Akman, F.; Kilicoglu, O.; Agar, O. Feasibility of a Novel Shield of Nuclear Radiation with W–Ni–Fe–Co and La–Bi Alloys Alternative to Pb and Ordinary Concrete Absorbers. Prog. Nucl. Energy 2023, 156, 104537. [Google Scholar] [CrossRef]
- Tousi, E.T. Monte Carlo Simulation of the Mass Attenuation Coefficient and Effective Atomic Number of the Eremurus-Rhizophora Ssp. Particleboard Phantom at the Mammography Energy Range. Prog. Nucl. Energy 2022, 149, 104281. [Google Scholar] [CrossRef]
- Lee, H. Monte Carlo Methods for Medical Imaging Research. Biomed. Eng. Lett. 2024, 14, 1195–1205. [Google Scholar] [CrossRef] [PubMed]
- Saidi, P.; Sadeghi, M.; Tenreiro, C.; Saidi, P.; Sadeghi, M.; Tenreiro, C. Variance Reduction of Monte Carlo Simulation in Nuclear Engineering Field. In Theory and Applications of Monte Carlo Simulations; IntechOpen: London, UK, 2013. [Google Scholar] [CrossRef]
- Metropolis Monte Carlo and The Maniac | PDF | Physical Sciences. Available online: https://mcnp.lanl.gov/pdf_files/Article_1986_LAS_Anderson_96--108.pdf (accessed on 22 June 2025).
- Harrison, R.L. Introduction to Monte Carlo Simulation. AIP Conf. Proc. 2010, 1204, 17. [Google Scholar] [CrossRef] [PubMed]
- Boone, J.M.; McNitt-Gray, M.F.; Hernandez, A.M. Monte Carlo Basics for Radiation Dose Assessment in Diagnostic Radiology. J. Am. Coll. Radiol. 2017, 14, 793–794. [Google Scholar] [CrossRef]
- Andreo, P. Monte Carlo Techniques in Medical Radiation Physics. Phys. Med. Biol. 1991, 36, 861. [Google Scholar] [CrossRef]
- Goorley, J.T.; James, M.R.; Booth, T.E.; Brown, F.B.; Bull, J.S.; Cox, L.J.; Durkee, J.W., Jr.; Elson, J.S.; Fensin, M.L.; Forster, R.A., III; et al. Initial MCNP6 Release Overview-MCNP6 Version 1.0; LA-UR-13-22934; Los Alamos National Lab. (LANL): Los Alamos, NM, USA, 2013. [Google Scholar]
- Gerward, L.; Guilbert, N.; Jensen, K.B.; Levring, H. WinXCom—A Program for Calculating X-Ray Attenuation Coefficients. Radiat. Phys. Chem. 2004, 71, 653–654. [Google Scholar] [CrossRef]
- Stults, K.A.; James, M.R.; Lombardi, M.; Klasky, M.L. Comparison of Modeled to Measured Spectra Using MCNP and GADRAS to Benchmark and Contrast Modeling Limitations; Los Alamos National Laboratory (LANL): Los Alamos, NM, USA, 2020. [Google Scholar]
- Bashter, I.I. Calculation of Radiation Attenuation Coefficients for Shielding Concretes. Ann. Nucl. Energy 1997, 24, 1389–1401. [Google Scholar] [CrossRef]
- Kurudirek, M.; Topcuoglu, S. Investigation of Human Teeth with Respect to the Photon Interaction, Energy Absorption and Buildup Factor. Nucl. Instrum. Methods Phys. Res. B 2011, 269, 1071–1081. [Google Scholar] [CrossRef]
- Sancho-Puchades, M.; Hämmerle, C.H.F.; Benic, G.I. In Vitro Assessment of Artifacts Induced by Titanium, Titanium-Zirconium and Zirconium Dioxide Implants in Cone-Beam Computed Tomography. Clin. Oral. Implant. Res. 2015, 26, 1222–1228. [Google Scholar] [CrossRef]
- Shokri, A.; Vafaee, F.; Haghighat, L.; Shahabi, S.; Farhadian, M.; Jamalpour, M.R. Comparison of the Amount of Artifacts Induced by Zirconium and Titanium Implants in Cone-Beam Computed Tomography Images. BMC Med. Imaging 2022, 22, 156. [Google Scholar] [CrossRef]
- Huang, C.C.; Li, M.J.; Tsai, P.I.; Kung, P.C.; Chen, S.Y.; Sun, J.S.; Tsou, N.T. Novel Design of Additive Manufactured Hollow Porous Implants. Dent. Mater. 2020, 36, 1437–1451. [Google Scholar] [CrossRef] [PubMed]
- Tchinda, A.; Lerebours, A.; Kouitat-Njiwa, R.; Bravetti, P. Zirconia Dental Implants: A Closer Look at Surface Condition and Intrinsic Composition by SEM-EDX. Bioengineering 2023, 10, 1102. [Google Scholar] [CrossRef] [PubMed]
- Choudhury, N.R.R.; Vilaplana, R.; Botet, R.; Sen, A.K. Comparison of Light Scattering Properties of Porous Dust Particle with Connected and Unconnected Dipoles. Planet. Space Sci. 2020, 190, 104974. [Google Scholar] [CrossRef]
- Halliwell, E.; Couch, C.; Begum, R.; Li, W.; Maqbool, M. Increase in Linear Attenuation Coefficient by Changing Crystal Structure of Materials for Radiation Shielding and Biomedical Devices Safety. Colloids Surf. A Physicochem. Eng. Asp. 2021, 622, 126646. [Google Scholar] [CrossRef]
- Assessment of Radiation Attenuation Properties in Dental Implants Using Monte Carlo Method. In Proceedings of the 35th International Congress of Oral Diagnosis and Maxillofacial Radiology Association, Cyprus, Oral Presentation, 23–27 April 2025.


| Implant | Element | Weight (%) | Implant Density (g/cm3) |
|---|---|---|---|
| NTA Implant | Titanium (Ti) | 90.39 | 4.428 |
| Aluminum (Al) | 5.4 | ||
| Vanadium (V) | 4.21 | ||
| Bilimplant | Carbon (C) | 1.00 | 4.510 |
| Nitrogen (N) | 1.00 | ||
| Iron (FE) | 7.00 | ||
| Oxygen (O) | 33.00 | ||
| Titanium (Ti) | 58.00 | ||
| Z-Systems | Zirconia (ZrO2) | 94.75 | 6.05 |
| Yttrium Oxide (Y2O3) | 5.00 | ||
| Aluminum Oxide (Al2O3) | 0.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rasat, A.; Tunc, S.; Uncu, Y.A.; Ozdogan, H. Assessment of Radiation Attenuation Properties in Dental Implants Using Monte Carlo Method. Bioengineering 2025, 12, 762. https://doi.org/10.3390/bioengineering12070762
Rasat A, Tunc S, Uncu YA, Ozdogan H. Assessment of Radiation Attenuation Properties in Dental Implants Using Monte Carlo Method. Bioengineering. 2025; 12(7):762. https://doi.org/10.3390/bioengineering12070762
Chicago/Turabian StyleRasat, Ali, Selmi Tunc, Yigit Ali Uncu, and Hasan Ozdogan. 2025. "Assessment of Radiation Attenuation Properties in Dental Implants Using Monte Carlo Method" Bioengineering 12, no. 7: 762. https://doi.org/10.3390/bioengineering12070762
APA StyleRasat, A., Tunc, S., Uncu, Y. A., & Ozdogan, H. (2025). Assessment of Radiation Attenuation Properties in Dental Implants Using Monte Carlo Method. Bioengineering, 12(7), 762. https://doi.org/10.3390/bioengineering12070762