
Transforming Bone Tunnel Evaluation in Anterior Cruciate Ligament Reconstruction: Introducing a Novel Deep Learning System and the TB-Seg Dataset

 , ,
, , 
Abstract
1. Introduction
1.1. Clinical Evaluation After ACLfR Surgery
1.2. Deep Learning-Based Bone Segmentation
2. Materials and Methods
2.1. XtremeCT
2.2. Dataset Information
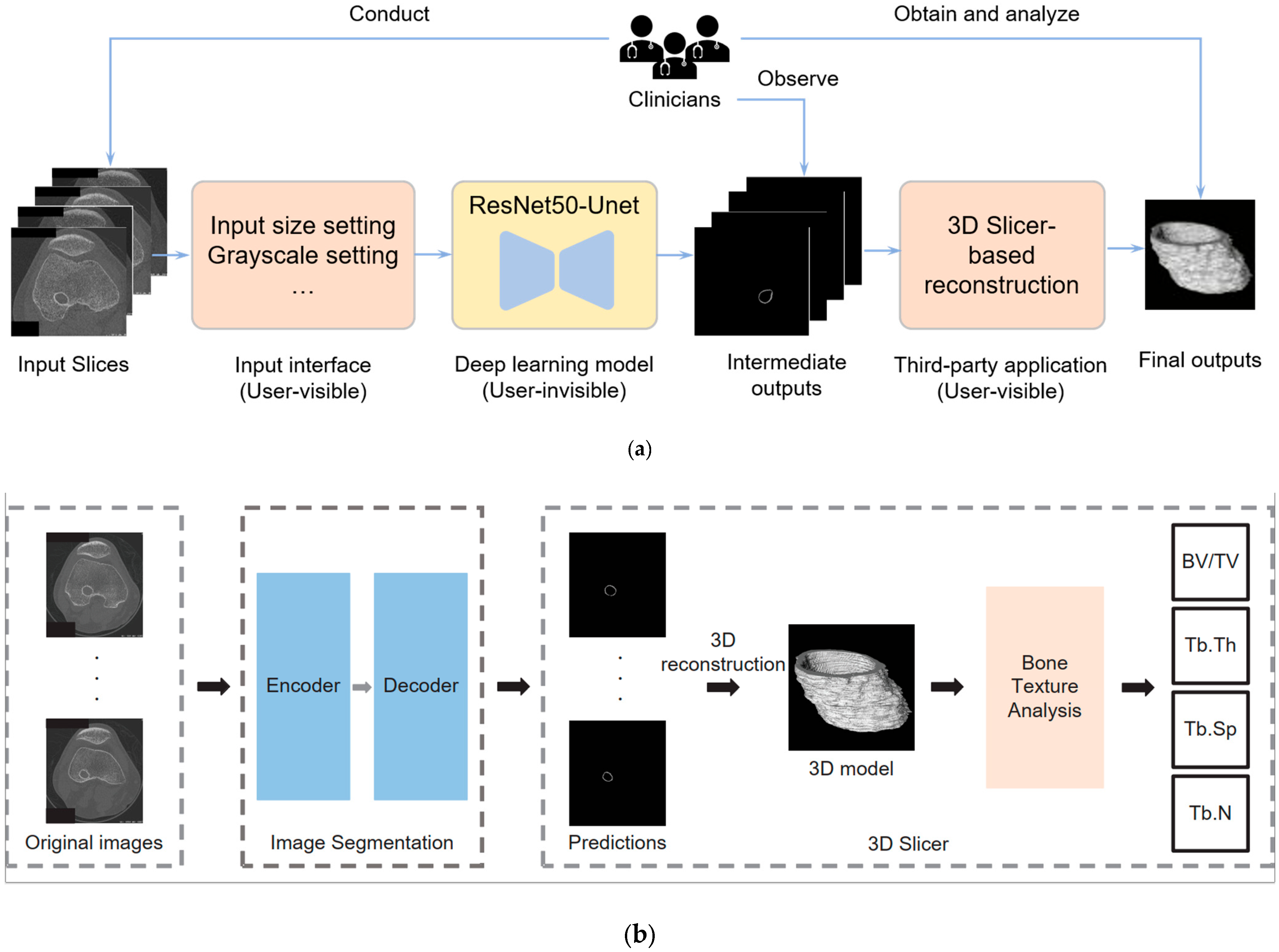
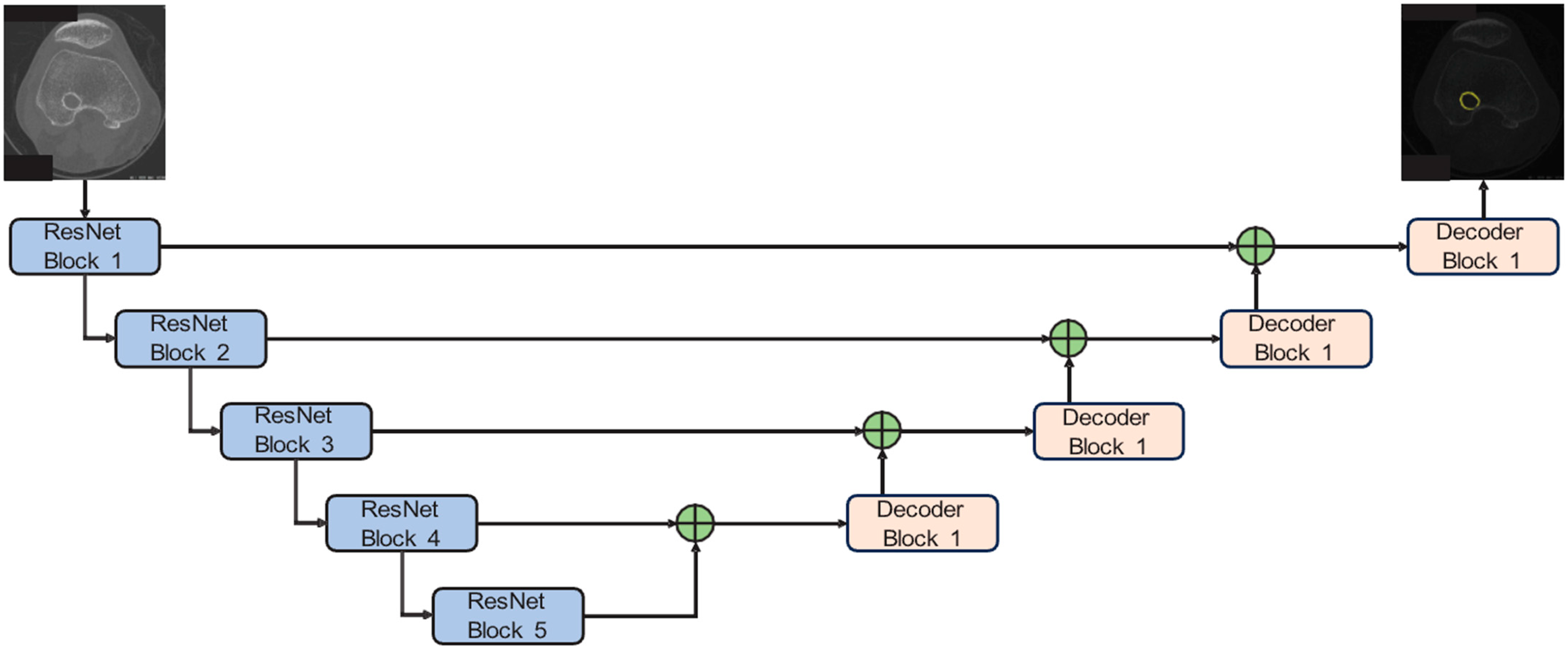
2.3. Detection and Analysis System
3. Results
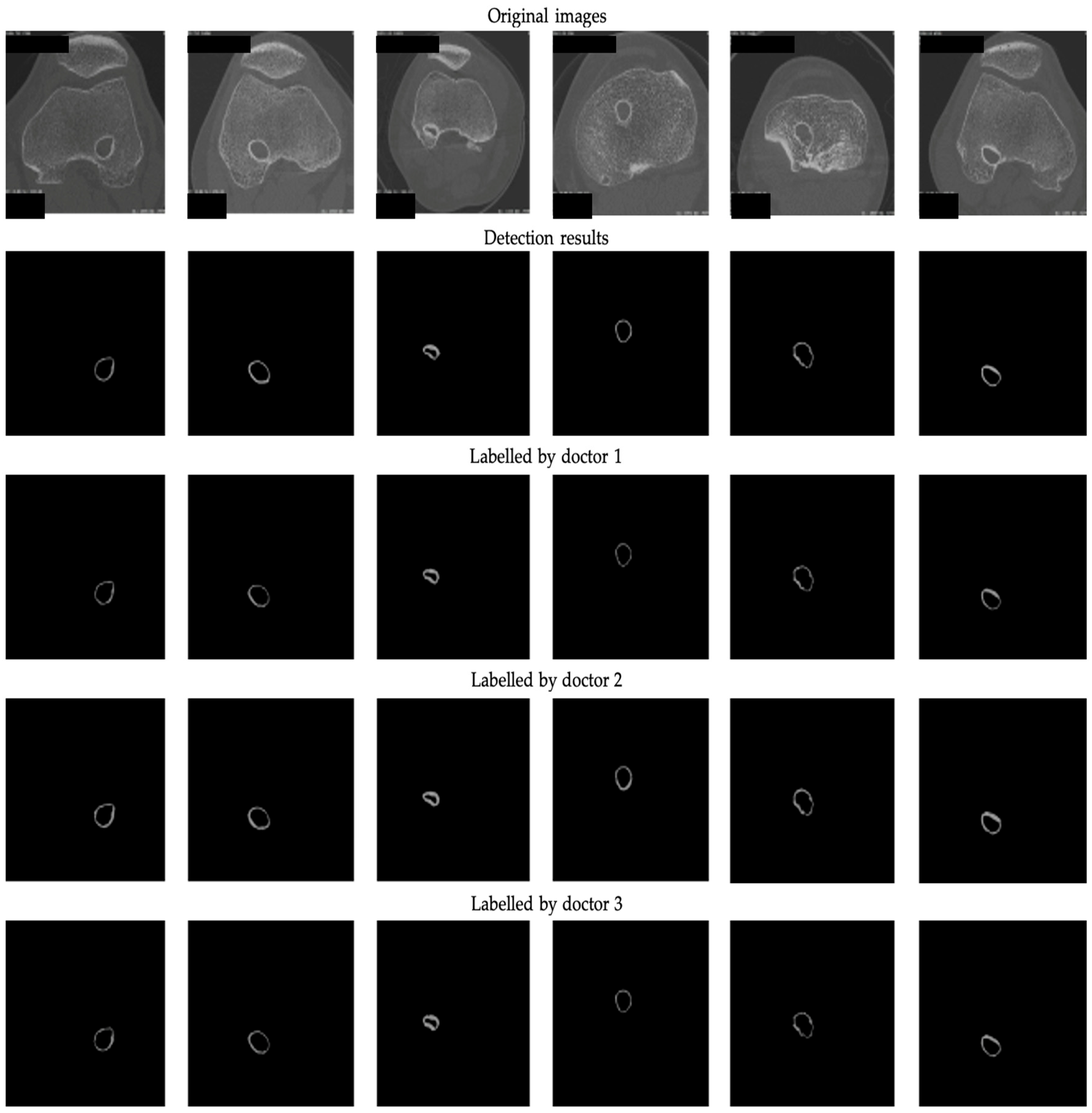
3.1. The 2D Segmentation
3.2. The 3D Reconstruction and Bone Texture Analysis
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bram, J.T.; Magee, L.C.; Mehta, N.N.; Patel, N.M.; Ganley, T.J. Anterior Cruciate Ligament Injury Incidence in Adolescent Athletes: A Systematic Review and Meta-analysis. Am. J. Sports Med. 2021, 49, 1962–1972. [Google Scholar] [CrossRef] [PubMed]
- Ariel de Lima, D.; de Lima, L.L.; de Souza, N.G.R.; de Moraes Perez, R.A.; Sobrado, M.F.; Guimarães, T.M.; Helito, C.P. Clinical Outcomes of Combined Anterior Cruciate Ligament and Anterolateral Ligament Reconstruction: A Systematic Review and Meta-analysis. Knee Surg. Relat. Res. 2021, 33, 33. [Google Scholar] [CrossRef] [PubMed]
- Yue, L.; DeFroda, S.F.; Sullivan, K.; Garcia, D.; Owens, B.D. Mechanisms of Bone Tunnel Enlargement Following Anterior Cruciate Ligament Reconstruction. JBJS Rev. 2020, 8, e0120. [Google Scholar] [CrossRef] [PubMed]
- Stolarz, M.; Ficek, K.; Binkowski, M.; Wróbel, Z. Bone Tunnel Enlargement Following Hamstring Anterior Cruciate Ligament Reconstruction: A Comprehensive Review. Physician Sportsmed. 2017, 45, 31–40. [Google Scholar] [CrossRef]
- Kimura, M.; Nakase, J.; Asai, K.; Yoshimizu, R.; Kanayama, T.; Tsuchiya, H. Tibial Graft Fixation Methods and Bone Tunnel Enlargement: A Comparison Between the TensionLoc Implant System and the Double-Spike Plate. Asia Pac. J. Sports Med. Arthrosc. Rehabil. Technol. 2022, 28, 31–37. [Google Scholar] [CrossRef]
- Webster, K.E.; Feller, J.A.; Elliott, J.; Hutchison, A.; Payne, R. A Comparison of Bone Tunnel Measurements Made Using Computed Tomography and Digital Plain Radiography After Anterior Cruciate Ligament Reconstruction. Arthrosc. J. Arthrosc. Relat. Surg. 2004, 20, 946–950. [Google Scholar] [CrossRef]
- Clatworthy, M.G.; Annear, P.; Bulow, J.U.; Bartlett, R.J. Tunnel Widening in Anterior Cruciate Ligament Reconstruction: A Prospective Evaluation of Hamstring and Patella Tendon Grafts. Knee Surg. Sports Traumatol. Arthrosc. 1999, 7, 138–145. [Google Scholar] [CrossRef]
- Foldager, C.; Jakobsen, B.W.; Lund, B.; Christiansen, S.E.; Kashi, L.; Mikkelsen, L.R.; Lind, M. Tibial Tunnel Widening After Bioresorbable Poly-Lactide Calcium Carbonate Interference Screw Usage in ACL Reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 79–84. [Google Scholar] [CrossRef]
- Peyrache, M.D.; Djian, P.; Christel, P.; Witvoet, J. Tibial Tunnel Enlargement After Anterior Cruciate Ligament Reconstruction by Autogenous Bone-Patellar Tendon-Bone Graft. Knee Surg. Sports Traumatol. Arthrosc. 1996, 4, 2–8. [Google Scholar] [CrossRef]
- Kim, Y.; Brodt, M.D.; Tang, S.Y.; Silva, M.J. MicroCT for Scanning and Analysis of Mouse Bones. In Skeletal Development and Repair; Methods in Molecular Biology; Hilton, M.J., Ed.; Humana: New York, NY, USA, 2021; Volume 2230. [Google Scholar] [CrossRef]
- Nishiyama, K.; Shane, E. Clinical Imaging of Bone Microarchitecture with HR-pQCT. Curr. Osteoporos. Rep. 2013, 11, 147–155. [Google Scholar] [CrossRef]
- Lui, P.P.; Lee, Y.W.; Mok, T.Y.; Cheuk, Y.C. Peri-Tunnel Bone Loss: Does It Affect Early Tendon Graft to Bone Tunnel Healing After ACL Reconstruction? Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 740–751. [Google Scholar] [CrossRef] [PubMed]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an Image Computing Platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [PubMed]
- Nikan, S.; Van Osch, K.; Bartling, M.; Allen, D.G.; Rohani, S.A.; Connors, B.; Agrawal, S.K.; Ladak, H.M. PWD-3DNet: A Deep Learning-Based Fully-Automated Segmentation of Multiple Structures on Temporal Bone CT Scans. IEEE Trans. Image Process. 2021, 30, 739–753. [Google Scholar] [CrossRef] [PubMed]
- Murty, A.N.; el Zebdeh, M.Y.; Ireland, J. Tibial Tunnel Enlargement Following Anterior Cruciate Reconstruction: Does Post-Operative Immobilization Make a Difference? Knee 2001, 8, 39–43. [Google Scholar] [CrossRef]
- Frosch, K.H.; Sawallich, T.; Schütze, G.; Losch, A.; Walde, T.; Balcarek, P.; Konietschke, F.; Stürmer, K.M. Magnetic Resonance Imaging Analysis of the Bioabsorbable Milagro Interference Screw for Graft Fixation in Anterior Cruciate Ligament Reconstruction. Strateg. Trauma Limb Reconstr. 2009, 4, 73–79. [Google Scholar] [CrossRef]
- Araki, D.; Kuroda, R.; Matsumoto, T.; Nagamune, K.; Matsushita, T.; Hoshino, Y.; Oka, S.; Nishizawa, Y.; Kurosaka, M. Three-Dimensional Analysis of Bone Tunnel Changes after Anatomic Double-Bundle Anterior Cruciate Ligament Reconstruction Using Multidetector-Row Computed Tomography. Am. J. Sports Med. 2014, 42, 2234–2241. [Google Scholar] [CrossRef]
- Liu, X.; Song, L.; Liu, S.; Zhang, Y. A Review of Deep-Learning-Based Medical Image Segmentation Methods. Sustainability 2021, 13, 1224. [Google Scholar] [CrossRef]
- Noguchi, S.; Nishio, M.; Yakami, M.; Nakagomi, K.; Togashi, K. Bone Segmentation on Whole-Body CT Using Convolutional Neural Network with Novel Data Augmentation Techniques. Comput. Biol. Med. 2020, 121, 103767. [Google Scholar] [CrossRef]
- Lindgren Belal, S.; Sadik, M.; Kaboteh, R.; Enqvist, O.; Uln, J.; Poulsen, M.H.; Simonsen, J.; Høilund-Carlsen, P.F.; Edenbrandt, L.; Trögårdh, E. Deep Learning for Segmentation of 49 Selected Bones in CT Scans: First Step in Automated PET/CT-Based 3D Quantification of Skeletal Metastases. Eur. J. Radiol. 2019, 113, 89–95. [Google Scholar] [CrossRef]
- Liu, F.; Zhou, Z.; Samsonov, A.; Blankenbaker, D.; Larison, W.; Kanarek, A.; Lian, K.; Kambhampati, S.; Kijowski, R. Deep Learning Approach for Evaluating Knee MR Images: Achieving High Diagnostic Performance for Cartilage Lesion Detection. Radiology 2018, 289, 160–169. [Google Scholar] [CrossRef]
- Liu, X.S.; Zhang, X.H.; Sekhon, K.K.; Adams, M.F.; McMahon, D.J.; Bilezikian, J.P.; Shane, E.; Guo, X.E. High-Resolution Peripheral Quantitative Computed Tomography Can Assess Microstructural and Mechanical Properties of Human Distal Tibial Bone. J. Bone Miner. Res. 2010, 25, 746–756. [Google Scholar] [CrossRef] [PubMed]
- Geusens, P.; Chapurlat, R.; Schett, G.; Ghasem-Zadeh, A.; Seeman, E.; de Jong, J.; van den Bergh, J. High-Resolution In Vivo Imaging of Bone and Joints: A Window to Microarchitecture. Nat. Rev. Rheumatol. 2014, 10, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Manske, S.L.; Zhu, Y.; Sandino, C.; Boyd, S.K. Human Trabecular Bone Microarchitecture Can Be Assessed Independently of Density with Second Generation HR-pQCT. Bone 2015, 79, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Hildebrand, T.; Ruegsegger, P. A New Method for the Model-Independent Assessment of Thickness in Three-Dimensional Images. J. Microsc. 1997, 185, 67–75. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In Proceedings of the 18th International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5–9 October 2015; Springer: New York, NY, USA, 2015; pp. 234–241. [Google Scholar] [CrossRef]
- Milletari, F.; Navab, N.; Ahmadi, S. V-Net: Fully Convolutional Neural Networks for Volumetric Medical Image Segmentation. In Proceedings of the International Conference on 3D Vision (3DV), Stanford, CA, USA, 25–28 October 2016; pp. 565–571. [Google Scholar] [CrossRef]
- Ioffe, S.; Szegedy, C. Batch Normalization: Accelerating Deep Network Training by Reducing Internal Covariate Shift. In Proceedings of the 32nd International Conference on Machine Learning, PMLR 2015, Lille, France, 6–11 July 2015; Volume 37, pp. 448–456. [Google Scholar]
- Paszke, A.; Gross, S.; Massa, F.; Lerer, A.; Bradbury, J.; Chanan, G.; Killeen, T.; Lin, Z.; Gimelshein, N.; Antiga, L.; et al. Pytorch: An imperative style, high-performance deep learning library. Advances in neural information processing systems 32. arxiv 2019, arXiv:1912.01703. Available online: https://arxiv.org/abs/1912.01703 (accessed on 30 December 2024).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Block | Component | Number |
|---|---|---|
| ResNet Block 1 | Convolution (kernel size = 7, stride = 2) Max Pooling (kernel size = 3, stride = 2) | x1 |
| ResNet Block 2 | Convolution (kernel size = 1, stride = 1) | x3 |
| Convolution (kernel size = 3, stride = 1) | ||
| Convolution (kernel size = 1, stride = 1) | ||
| ResNet Block 3 | Convolution (kernel size = 1, stride = 1) | x4 |
| Convolution (kernel size = 3, stride = 2) | ||
| Convolution (kernel size = 1, stride = 1) | ||
| ResNet Block 4 | Convolution (kernel size = 1, stride = 1) | x6 |
| Convolution (kernel size = 3, stride = 2) | ||
| Convolution (kernel size = 1, stride = 1) | ||
| ResNet Block 5 | Convolution (kernel size = 1, stride = 1) | x3 |
| Convolution (kernel size = 3, stride = 2) | ||
| Convolution (kernel size = 1, stride = 1) |
| Results | Inter-Observer Variability | |||||
|---|---|---|---|---|---|---|
| Pair | DR–D1 | DR–D2 | DR–D3 | D1–D2 | D1–D3 | D2–D3 |
| P | 90.42 | 96.45 | 91.62 | 98.16 | 95.21 | 97.28 |
| R | 95.82 | 89.71 | 95.16 | 86.32 | 93.28 | 87.25 |
| mIoU | 87.63 | 87.42 | 88.20 | 85.31 | 89.63 | 85.69 |
| mPA | 95.82 | 89.71 | 95.16 | 86.32 | 93.28 | 87.25 |
| 1 femur | 2 femur | 3 femur | 4 femur | 5 femur | 6 femur | 7 femur | 8 femur | |
| mGV | 95.58 | 77.21 | 123.65 | 92.33 | 118.42 | 63.70 | 121.36 | 104.90 |
| 9 femur | 10 femur | 11 femur | 12 femur | 13 femur | 14 femur | 15 femur | 16 femur | |
| mGV | 106.93 | 54.38 | 114.34 | 55.24 | 59.48 | 118.80 | 50.76 | 49.29 |
| 17 femur | 18 femur | 19 femur | 20 femur | 21 femur | 22 femur | 23 femur | 24 femur | |
| mGV | 97.41 | 117.54 | 94.30 | 110.58 | 103.88 | 124.65 | 73.42 | 109.97 |
| 1 tibia | 2 tibia | 3 tibia | 4 tibia | 5 tibia | 6 tibia | 7 tibia | 8 tibia | |
| mGV | 75.22 | 73.56 | 105.45 | 115.49 | 72.58 | 58.90 | 107.86 | 106.39 |
| 9 tibia | 10 tibia | 11 tibia | 12 tibia | 13 tibia | 14 tibia | 15 tibia | 16 tibia | |
| mGV | 61.54 | 87.11 | 92.82 | 111.38 | 70.12 | 54.64 | 88.30 | 90.49 |
| 17 tibia | 18 tibia | 19 tibia | 20 tibia | 21 tibia | 22 tibia | 23 tibia | 24 tibia | |
| mGV | 104.01 | 118.83 | 106.27 | 102.66 | 91.23 | 103.47 | 97.27 | 97.07 |
| 1 femur | 1 tibia | 2 femur | 2 tibia | 3 femur | 3 tibia | |
 | ||||||
| BV/TV | 0.0716 | 0.0495 | 0.0623 | 0.0488 | 0.1992 | 0.1721 |
| Tb.Th | 0.2668 | 0.2190 | 0.2157 | 0.1985 | 0.4619 | 0.3429 |
| Tb.Sp | 0.6070 | 0.7214 | 0.5647 | 0.6636 | 0.3748 | 0.3226 |
| Tb.N | 1.6402 | 1.3820 | 1.7641 | 1.5024 | 2.6356 | 3.0671 |
| Volume | 243.5359 | 281.6452 | 53.3224 | 287.4996 | 381.7742 | 224.1293 |
| 4 femur | 4 tibia | 5 femur | 5 tibia | 6 femur | 6 tibia | |
 | ||||||
| BV/TV | 0.1068 | 0.1202 | 0.1349 | 0.0260 | 0.1668 | 0.0912 |
| Tb.Th | 0.3310 | 0.3831 | 0.3835 | 0.2197 | 0.4955 | 0.3796 |
| Tb.Sp | 0.5038 | 0.5176 | 0.4613 | 1.3801 | 0.4810 | 0.6769 |
| Tb.N | 1.9720 | 1.9180 | 2.1500 | 0.7234 | 2.0580 | 1.4692 |
| Volume | 218.8271 | 224.1203 | 259.8397 | 81.4737 | 267.7767 | 159.2747 |
| 7 femur | 7 tibia | 8 femur | 8 tibia | 9 femur | 9 tibia | |
 | ||||||
| BV/TV | 0.1429 | 0.1166 | 0.1309 | 0.1593 | 0.1626 | 0.1293 |
| Tb.Th | 0.4680 | 0.3813 | 0.3129 | 0.3706 | 0.4480 | 0.3238 |
| Tb.Sp | 0.5310 | 0.5314 | 0.3879 | 0.3769 | 0.4462 | 0.4066 |
| Tb.N | 1.8668 | 1.8684 | 2.5571 | 2.6274 | 2.2189 | 2.4399 |
| Volume | 303.4012 | 216.5775 | 224.0486 | 261.8792 | 276.8046 | 257.3116 |
| 10 femur | 10 tibia | 11 femur | 11 tibia | 12 femur | 12 tibia | |
 | ||||||
| BV/TV | 0.1578 | 0.1572 | 0.1350 | 0.1265 | 0.1176 | 0.2744 |
| Tb.Th | 0.3918 | 0.4298 | 0.3787 | 0.3521 | 0.3478 | 0.4114 |
| Tb.Sp | 0.4023 | 0.4430 | 0.4552 | 0.4517 | 0.4804 | 0.2412 |
| Tb.N | 2.4617 | 2.2357 | 2.1789 | 2.1968 | 2.0664 | 4.0759 |
| Volume | 302.4606 | 213.9549 | 172.3847 | 159.8268 | 114.9964 | 289.7149 |
| 13 femur | 13 tibia | 14 femur | 14 tibia | 15 femur | 15 tibia | |
 | ||||||
| BV/TV | 0.1508 | 0.0887 | 0.1412 | 0.1417 | 0.1533 | 0.1183 |
| Tb.Th | 0.3358 | 0.2583 | 0.3514 | 0.3566 | 0.3498 | 0.2980 |
| Tb.Sp | 0.3610 | 0.4737 | 0.4038 | 0.4081 | 0.3698 | 0.4093 |
| Tb.N | 2.7447 | 2.0994 | 2.4552 | 2.4290 | 2.6786 | 2.4255 |
| Volume | 315.6059 | 86.5112 | 285.6405 | 207.5080 | 324.8141 | 158.0593 |
| 16 femur | 16 tibia | 17 femur | 17 tibia | 18 femur | 18 tibia | |
 | ||||||
| BV/TV | 0.1279 | 0.1428 | 0.1209 | 0.1214 | 0.1171 | 0.1204 |
| Tb.Th | 0.4100 | 0.2995 | 0.3394 | 0.3400 | 0.4140 | 0.3550 |
| Tb.Sp | 0.5205 | 0.3402 | 0.4558 | 0.4548 | 0.5741 | 0.4788 |
| Tb.N | 1.9062 | 2.9135 | 2.1778 | 2.1824 | 1.7294 | 2.0730 |
| Volume | 389.4614 | 190.8696 | 247.7926 | 120.1776 | 246.2565 | 119.0466 |
| 19 femur | 19 tibia | 20 femur | 20 tibia | 21 femur | 21 tibia | |
 | ||||||
| BV/TV | 0.1431 | 0.1197 | 0.1351 | 0.1339 | 0.1295 | 0.1378 |
| Tb.Th | 0.3955 | 0.3505 | 0.3647 | 0.3490 | 0.3471 | 0.2990 |
| Tb.Sp | 0.4483 | 0.4755 | 0.4379 | 0.4230 | 0.4351 | 0.3517 |
| Tb.N | 2.2113 | 2.0878 | 2.2648 | 2.3451 | 2.2804 | 2.8193 |
| Volume | 273.2562 | 195.7849 | 306.7198 | 220.4959 | 237.2063 | 175.8877 |
| 22 femur | 22 tibia | 23 femur | 23 tibia | 24 femur | 24 tibia | |
 | ||||||
| BV/TV | 0.1539 | 0.1280 | 0.1113 | 0.0712 | 0.1384 | 0.1256 |
| Tb.Th | 0.4124 | 0.3490 | 0.3052 | 0.2326 | 0.3585 | 0.3360 |
| Tb.Sp | 0.4341 | 0.4425 | 0.4454 | 0.5322 | 0.4201 | 0.4342 |
| Tb.N | 2.2819 | 2.2422 | 2.2298 | 1.8707 | 2.3604 | 2.2854 |
| Volume | 376.1578 | 235.0518 | 112.3658 | 173.8293 | 240.8560 | 150.8067 |
| Image Selection | Image Processing | Image Segmentation | 3D Slicer Analysis | Total Time |
|---|---|---|---|---|
| 55.87 | 253.85 | 81.92 | 37.84 | 429.48 |
| 50.60 | 241.58 | 43.71 | 45.56 | 381.45 |
| 51.68 | 256.72 | 64.24 | 53.84 | 426.48 |
| 40.60 | 247.93 | 63.77 | 44.95 | 397.25 |
| 30.66 | 243.83 | 52.17 | 31.00 | 357.66 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xie, K.; Yu, M.; Liu, J.H.-P.; Ma, Q.; Zou, L.; Man, G.C.-W.; Xu, J.; Yung, P.S.-H.; Li, Z.; Ong, M.T.-Y. Transforming Bone Tunnel Evaluation in Anterior Cruciate Ligament Reconstruction: Introducing a Novel Deep Learning System and the TB-Seg Dataset. Bioengineering 2025, 12, 527. https://doi.org/10.3390/bioengineering12050527
Xie K, Yu M, Liu JH-P, Ma Q, Zou L, Man GC-W, Xu J, Yung PS-H, Li Z, Ong MT-Y. Transforming Bone Tunnel Evaluation in Anterior Cruciate Ligament Reconstruction: Introducing a Novel Deep Learning System and the TB-Seg Dataset. Bioengineering. 2025; 12(5):527. https://doi.org/10.3390/bioengineering12050527
Chicago/Turabian StyleXie, Ke, Mingqian Yu, Jeremy Ho-Pak Liu, Qixiang Ma, Limin Zou, Gene Chi-Wai Man, Jiankun Xu, Patrick Shu-Hang Yung, Zheng Li, and Michael Tim-Yun Ong. 2025. "Transforming Bone Tunnel Evaluation in Anterior Cruciate Ligament Reconstruction: Introducing a Novel Deep Learning System and the TB-Seg Dataset" Bioengineering 12, no. 5: 527. https://doi.org/10.3390/bioengineering12050527
APA StyleXie, K., Yu, M., Liu, J. H.-P., Ma, Q., Zou, L., Man, G. C.-W., Xu, J., Yung, P. S.-H., Li, Z., & Ong, M. T.-Y. (2025). Transforming Bone Tunnel Evaluation in Anterior Cruciate Ligament Reconstruction: Introducing a Novel Deep Learning System and the TB-Seg Dataset. Bioengineering, 12(5), 527. https://doi.org/10.3390/bioengineering12050527