1. Introduction
In recent years, the potential long-term effects of concussions and repeated sub-concussive head impacts have sparked growing concerns within the athletic community. Numerous athletes have shared the complications they have faced from long exposure to high impact collisions, resulting in the diagnosis of early onset dementia and other neurological disorders [
1,
2,
3]. Chronic traumatic encephalopathy (CTE), a condition resulting from repeated concussions and characterised by symptoms such as depression, memory loss, concentration problems, personality disorders, and other cognitive impairments, has been identified as a particular worry [
4,
5]. This heightened awareness has led researchers to investigate the health consequences of concussions in athletes, and to explore whether soft-shell head protection can help to prevent them or reduce the severity of such injuries.
A concussion is a subset of diffuse traumatic brain injury (TBI) that occurs when the brain absorbs sufficient kinetic energy following a direct or indirect impact, so it undergoes significant motion and intracranial stresses and strains within the skull. Consequently, a temporary disturbance of brain function occurs [
5,
6]. Early research suggested that concussive brain injury was caused primarily by linear acceleration forces, resulting in a back-and-forth motion of the brain within the skull [
7]. However, experimental studies identified that rotational kinematics are correlated with a greater severity of TBI [
8,
9,
10]. This is explained by the shearing and stretching of the brain tissue that rotational forces can cause, resulting in high levels of strain within the brain, and subsequent injury [
11,
12]. Additionally, Ommaya [
13], four decades ago, explained that rotational forces can produce both focal and diffuse brain injuries, while translational force is limited to focal effects. Injury statistics have found the most common accident situations involve an oblique impact, which gives rise to both linear and rotational head kinematics [
10]. These types of impacts are observed frequently in contact sports during tackles or falls, where a person’s head is subjected to both linear and rotational accelerations, resulting in the risk of a sport related concussion (SRC).
Sport Related Concussions (SRCs) are a more complicated type of concussion as athletes can be subjected to sub-concussive head impacts on a regular basis. This is distinguishable from a single-impact TBI, as repeated impacts may contribute to cumulative brain trauma that eventually manifests as a long-term impairment [
14]. Moreover, repeated concussive and sub-concussive head injuries may cause a range of neurological sequelae, including post-traumatic stress disorder (PTSD), chronic traumatic encephalopathy, post-concussion syndrome, and dementia [
14,
15]. The physical nature of the sport, combined with the size and strength of players in contact and collision team sports such as rugby, pose a significant risk of concussive injuries. According to the 2020–2021 English Professional Brain Injury Surveillance Project, concussions were the most often reported match injury for the tenth consecutive season, accounting for 28% of all match injuries and having an incidence rate of 22.2 concussions per 1000 h [
16]. A similar study from Ireland found that concussions occurred during matches at a rate of 20 per 1000 player-match hours [
17]. The risk of injury is particularly high in the tackle, scrum, and ruck phases of the game [
18,
19]. Specifically, research suggests that 50–70% of all concussions are associated with tackles [
16,
17,
18,
19,
20,
21]. These findings, and the heightened awareness of the risks that come with TBIs, have led researchers to further investigate the consequences of concussions in athletes, and to explore whether soft-shell head protection can help to prevent them.
Earlier studies of concussion in rugby have led to the efficacy of traditional headguard models being called into question [
3,
22]. A study conducted by Knouse et al. evaluated the effectiveness of branded rugby headgear in attenuating repetitive linear impact forces [
4]. They compared the attenuation capabilities of two common types of headgear, Honeycomb and Vanguard, using an unprotected headform as control. Diverse International Rugby Board (IRB) approved headgears of these two types were dropped from a fixed height of 30 cm, in accordance with the International Rugby Board (IRB) test standards, to measure force attenuation at two different impact sites (posterior and parietal-lateral regions). The test involved measuring the headform’s peak instantaneous acceleration and Gadd Severity Index (GSI) on contacting an MEP pad. Compared to the unprotected headform, both types of headgear attenuated impact forces. However, after ten drops, the ability to absorb repeated linear impacts decreased by approximately 10 to 36%, depending on the type of headguard and the impact location, and a decrease in performance was evident after just one impact. This and other similar studies [
22,
23,
24,
25,
26] identified the need to research different materials and headgear designs that would successfully attenuate repetitive impact forces experienced during contact sports without losing effectiveness over time. McIntosh et al. [
21] suggested that the “memory effect” of soft, closed-cell foam used in rugby gear may prevent the material from regaining its original thickness after impact, leading to a reduction in headgear effectiveness over time. Therefore, recent research has evaluated several materials for their effectiveness in improving impact absorption, as well as leading to the development of innovative headgear designs that can combat the current limitations.
Draper et al. [
24] conducted a study to evaluate the performance of six commercially available headguards from five different commercial manufacturers, including two size variations (medium and large) for one brand. The headguards assessed were the CCC Ventilator, Kukri, 2nd Skull, N-Pro, and both medium and large version of Gamebreaker Pro. The primary objective of their study was to assess the ability of the different headguards to attenuate peak linear accelerations (PLA) and the head injury criterion (HIC) scores were used to evaluate their relative effectiveness. Those results indicated that the N-Pro and the Gamebreaker Pro headguards significantly reduced both PLA and HIC than did the other three headguard designs. They also indicated that the Gamebreaker Pro designs offered even better reductions in PLA and HIC than the N-Pro design: this was attributed to the thicker layers of protection in the Gamebreaker Pro. In addition, Stitt et al. [
25] conducted a study to examine the potential of headguards to mitigate both linear and rotational accelerations. Their experimental investigation involved analysing peak accelerations that occurred when headguards were attached to instrumented headforms and dropped vertically from four different heights, at various angles, and on different contact points on the head. Five commercially available headguards were tested in that study: CCC Reinforced, Gilber Falcon 200, 2nd Skull, N-Pro and Gamebreaker Pro. The results demonstrated clearly that both the N-Pro and the Gamebreaker Pro significantly reduced the peak linear accelerations (PLA) and peak rotational accelerations (PRA) than did either of the other three headguard designs. In light of those previous studies, the present work does not attempt to compare the performance of alternative commercially available headguards. Nonetheless, some general observations can be made in respect of alternative soft-shell headguard designs. Most tend to rely on using various viscoelastic foam pads that are incorporated into a laced-up form that provide close contact with a wearer’s head. Some of the designs that are certified for use by World Rugby provide greater levels of coverage to vulnerable regions of the head than others. A thorough comprehensive analysis of the relative efficacy of each headguard design and identifying particular aspects of each design that might merit improvement is beyond the scope of this present study.
This present study was completed in conjunction with a leading headguard manufacturer, N-Pro, and focuses on their headguard as a representative design of advanced head protection worn in rugby. This headguard differs from closed-cell foam headguards due to its proprietary viscoelastic polymer foam, Defentex, that is incorporated into the padding [
26]. The material was designed specifically to help attenuate head impacts and aid in the mitigation of concussive injuries. The incorporation of Defentex allows the absorption of impact energy even without a hard outer shell. The headguard is made up of soft, elastic segments that are capable of absorbing energy, and stiffer segments that provide durability and stability [
26]. When compared with two other commercial headguards, the N-Pro significantly reduced linear and rotational accelerations of the head following impact [
24,
25,
26]. Results from mechanical drop tests have shown the headguard’s ability to reduce linear accelerations experienced by the head during an impact by up to 75%, compared to other commercially available headguards, and rotational accelerations by an average of 34% compared to a bare headform [
26].
As discussed above for SRCs, athletes may be exposed to repeated head impacts of a sub-concussive nature on a regular basis. Recent discussion regarding diagnostic criteria for mild traumatic brain injury (mTBI) caused by repetitive concussive and sub-concussive head impacts highlights the heterogeneity of the signs and symptoms that exist for SRC [
15,
27]. Advancements in side-line and clinical assessment of SRC in rugby include the 6th iteration of the Sports Concussion Assessment Tool (SCAT-6) following the 2022 consensus meeting of the Concussion in Sport Group [
28]. While this offers improvements to the evaluation of athletes following a potential SRC, there remains a need to develop enhanced diagnostic tests and objective biological markers of SRC that overcome current drawbacks in outcome sensitivity and subjectivity. Ongoing research into the neurological effects of repeated head impact exposures in athletes has leveraged neuroimaging, neurological blood biomarkers, and oculomotor performance [
27,
28,
29,
30,
31] amid efforts to determine whether a threshold for adverse events exists for exposure to sub-concussive impacts. Laboratory testing and previous in-silico examinations of SRC have proposed tolerances for brain injury based on the kinematic and tissue responses of the head and brain under loading [
8,
32,
33,
34,
35,
36,
37]. Real-time monitoring of head impact exposure alongside enhanced clinical insights into the brain’s structural and metabolic response to repetitive sub-concussive loading would provide further clarity into potential upper and lower thresholds above or below which SRCs may or may not occur for a specific population. This is discussed in further detail following our predictions for real-world injury events in rugby, alongside recommendations on how real-world clinical evidence can be leveraged in conjunction with finite element (FE) predictions of brain deformation to offer improvements for prevention strategies against SRC.
Although mechanical impact tests are useful to determine whether a headguard attenuates force, they do not consider the stresses and strains experienced by the brain during an impact. As mentioned previously, TBI is not only characterized by movement of the brain relative to the skull following an impact, but also by high strains following the deformation of brain tissue [
11]. Therefore, headguards must also be tested for their effect on brain tissue response. FE models have been instrumental in the study and understanding of head injury biomechanics [
36,
37,
38], as well as the protective capabilities of helmets used in sports [
38,
39,
40,
41,
42,
43,
44,
45], such as ice hockey, cycling, motorcycling, skiing and equestrian sports. The models are generally developed from slices of computed tomography (CT) scans or magnetic resonance imaging (MRI) images of human subjects [
38,
39]. Furthermore, their accuracy has been validated by performing comparative tests with results from cadaveric experiments, and the models are continuously being improved to better represent the geometry, anatomy and components of the brain [
40]. These advances make them powerful tools for studying head impact biomechanics.
The UCDBTM is a finite element model developed by Horgan & Gilchrist [
38] to study head impact biomechanics, and has been used to evaluate the efficacy of headgear for rugby [
43], to establish the performance of equestrian helmets [
37,
44], estimate the brain tissue response while a soccer player heads the ball, and to compare different helmet designs for ice hockey goal keeper helmets [
41]. Other similar three-dimensional computational models exist and these include NHTSA’s SIMON (Simulated Injury Monitor) model [
46], which has been used extensively to simulate head protection during car crash events. Duckworth et al. [
47] created a three-dimensional finite element model of a rodent brain to evaluate cerebral vascular injury and to predict microbleed locations. Zhou et al. [
48], Zhang et al. [
49] and Gadjari et al. [
50] also created very refined finite element models of the human brain to properly represent the cerebral ventricles, sulci and gyri, and to account more accurately for the fluid behaviour of the cerebrospinal fluid (CSF).
This study proposes that simulating head impact events in rugby, under both unprotected and protected loading conditions, will advance our understanding of the levels of protection provided by energy-absorbing foam headgear. Such knowledge will lead to improvements in the design of headguards used in rugby, ultimately benefiting player welfare.
5. Conclusions
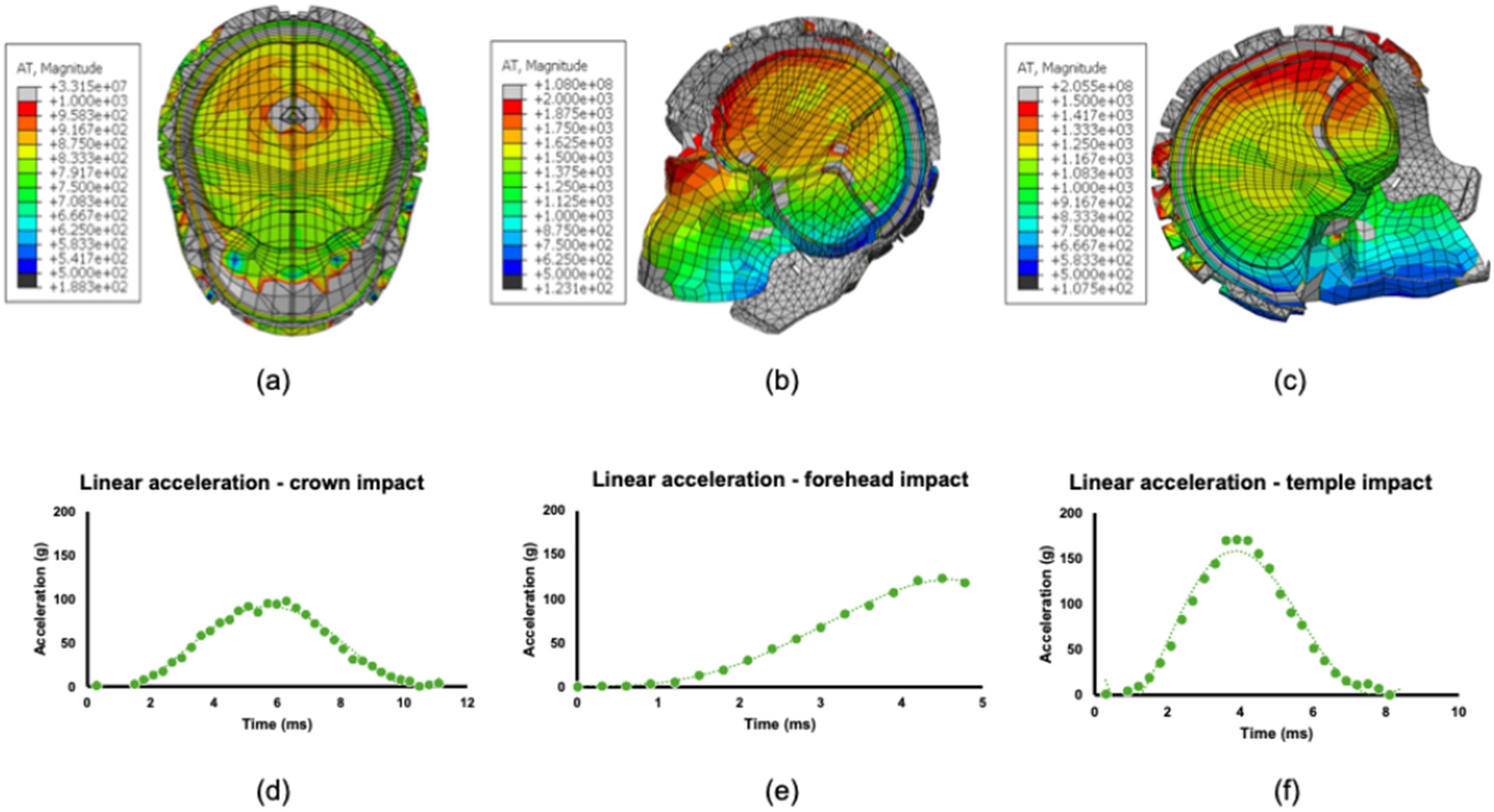
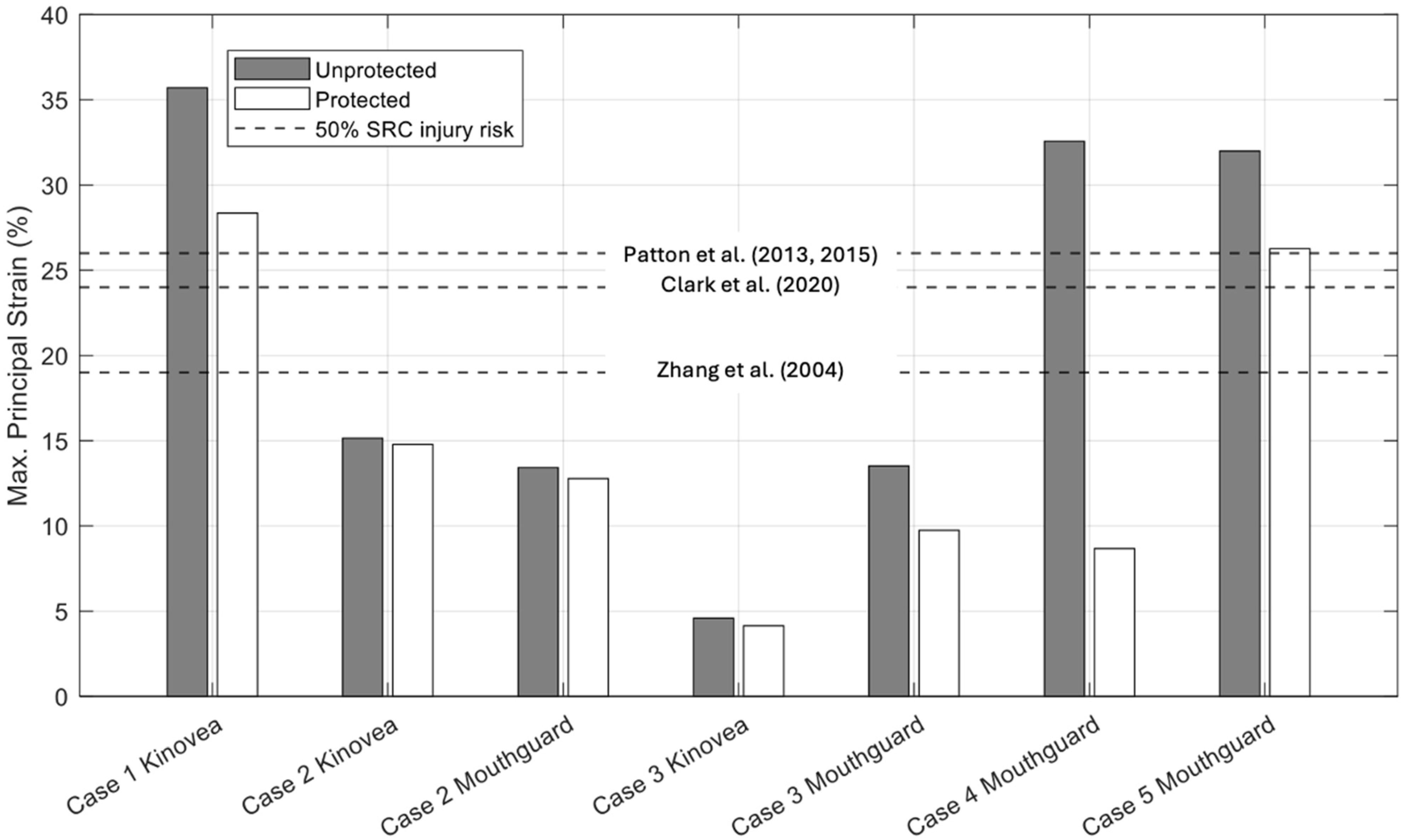
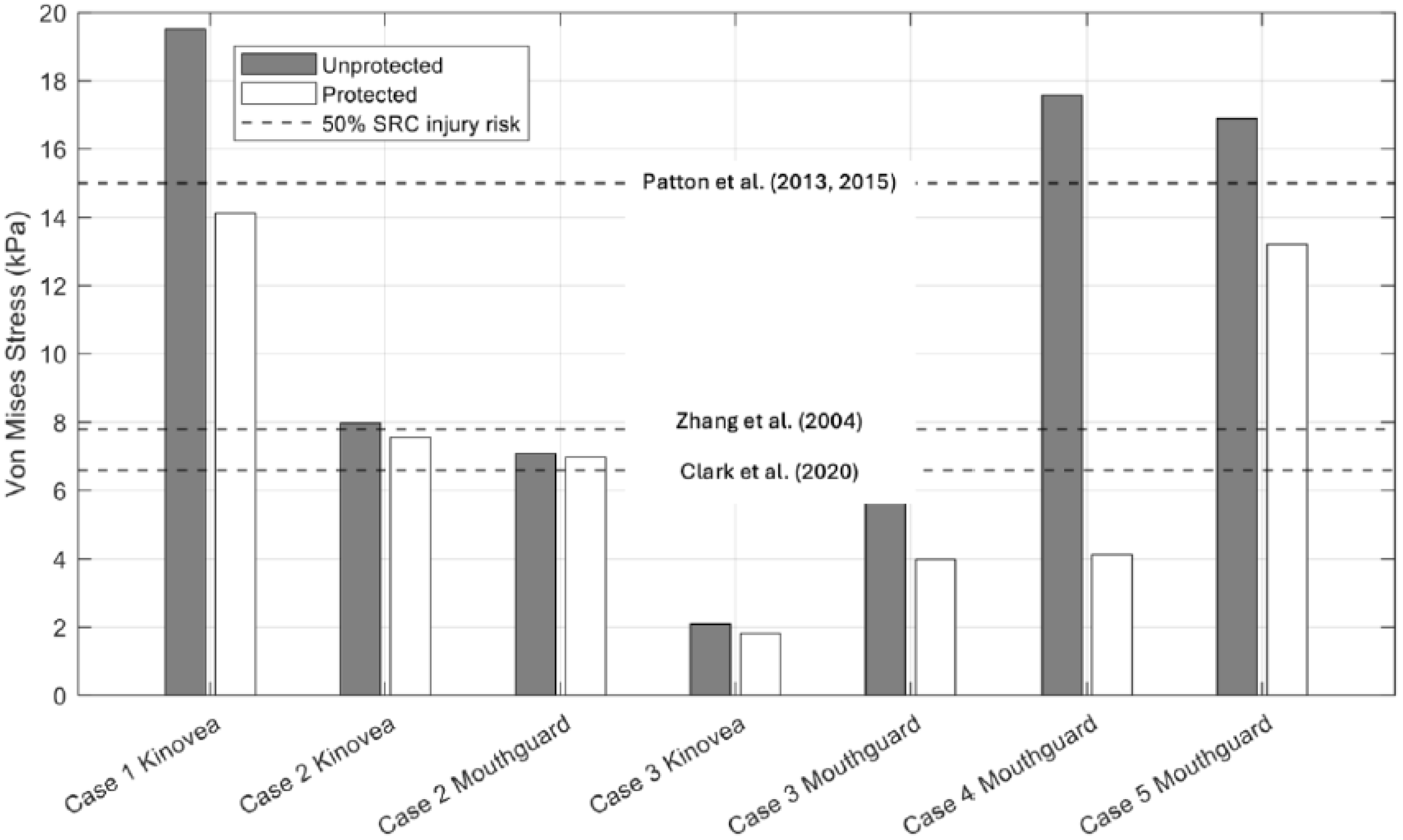
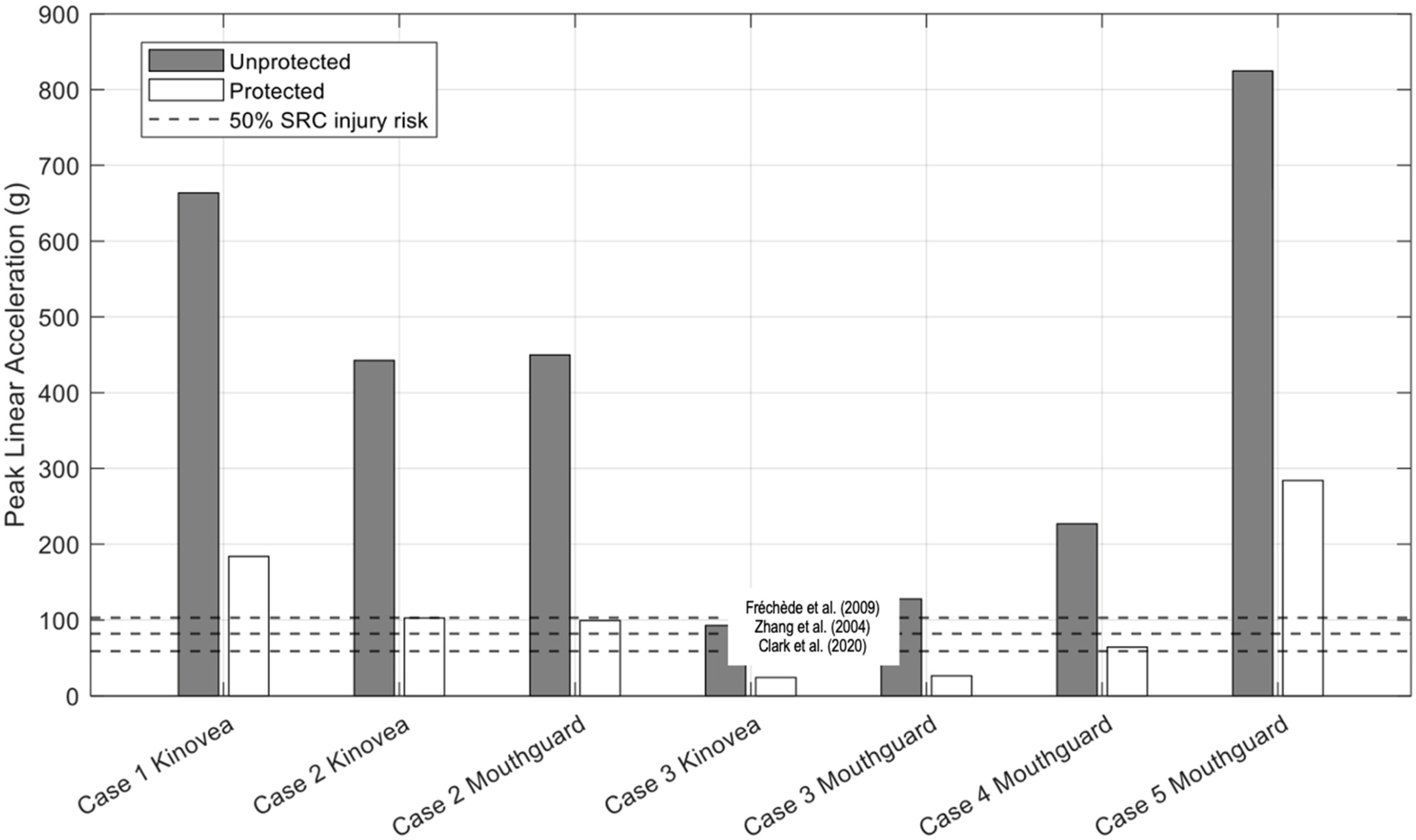
A principal purpose of this study was to evaluate the effectiveness of the N-Pro headguard as a protective device against head impacts for rugby players. This was accomplished by computationally simulating five real-world head impact scenarios using a FE head model, without and with a corresponding headguard model, during impacts against non-compliant surfaces. Additionally, two data acquisition methods were compared for capturing impact kinematics. The results demonstrate clearly that the N-Pro headguard reduces peak resultant head accelerations and brain tissue responses in all simulated cases, resulting in a reduction of typically 70% in peak linear accelerations. Depending on the impact location, the corresponding reductions in peak stresses and strain when wearing a headguard can also be as much as 70%, although not consistently so. In some cases, especially for impacts similar to Case 2 (Top Rear location), there may be negligible reduction in the stresses and strains. Notwithstanding this caveat, the results support the claims made by N-Pro regarding the increased protection against head impacts for players who wear their product, in comparison to those who do not wear any protection.
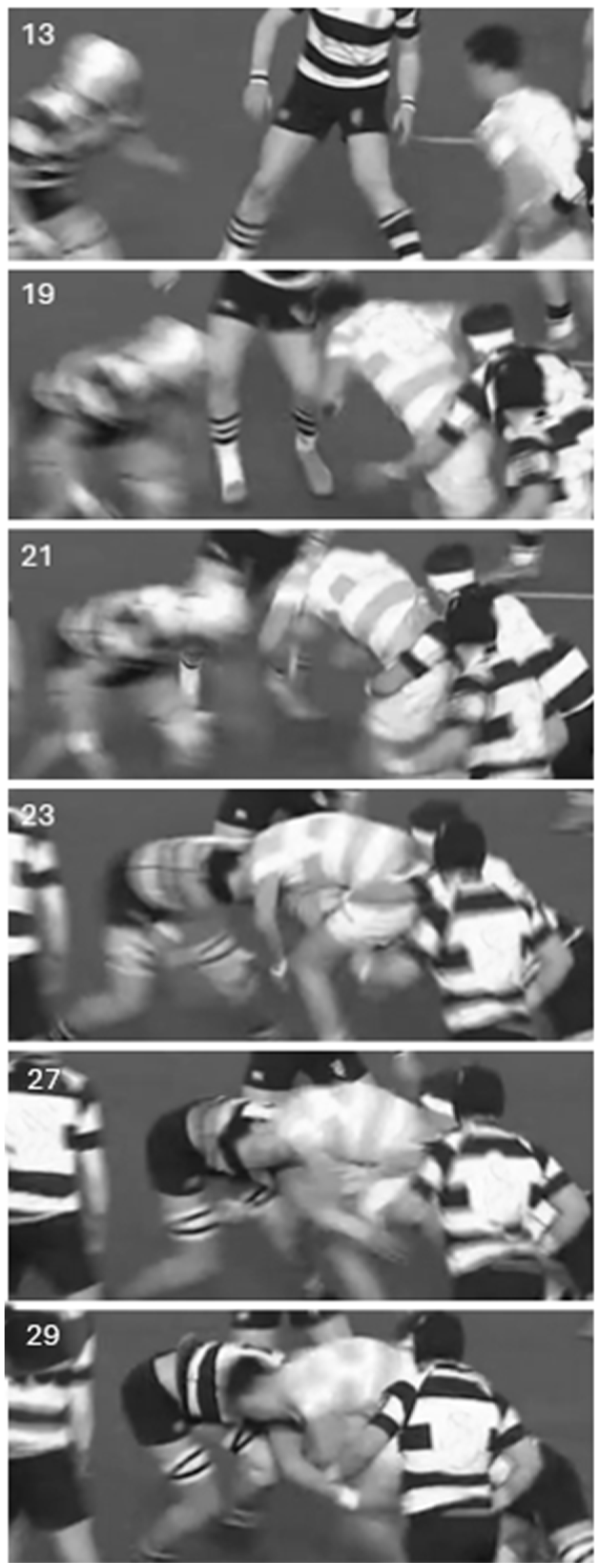
Additionally, the study allowed for an evaluation of the advantages and limitations of two methods for gathering impact kinematics. The use of wearable sensors such as instrumented mouthguards to objectively gather accurate measures of kinematic data is a tool that has gained significant attraction in the past few years. While it has significant potential for gathering accident information in real-time as compared to other methods such as motion tracking through video footage, it does come with its limitations. One of the major limitations in rugby impact reconstructions is that it does not provide a detailed description of the accident, which can limit the ability to fully understand the dynamics of the impact and accurately assess the potential risk of injury. Therefore, it is recommended to use video footage and analysis as a complement to the instrumented mouthguard data.
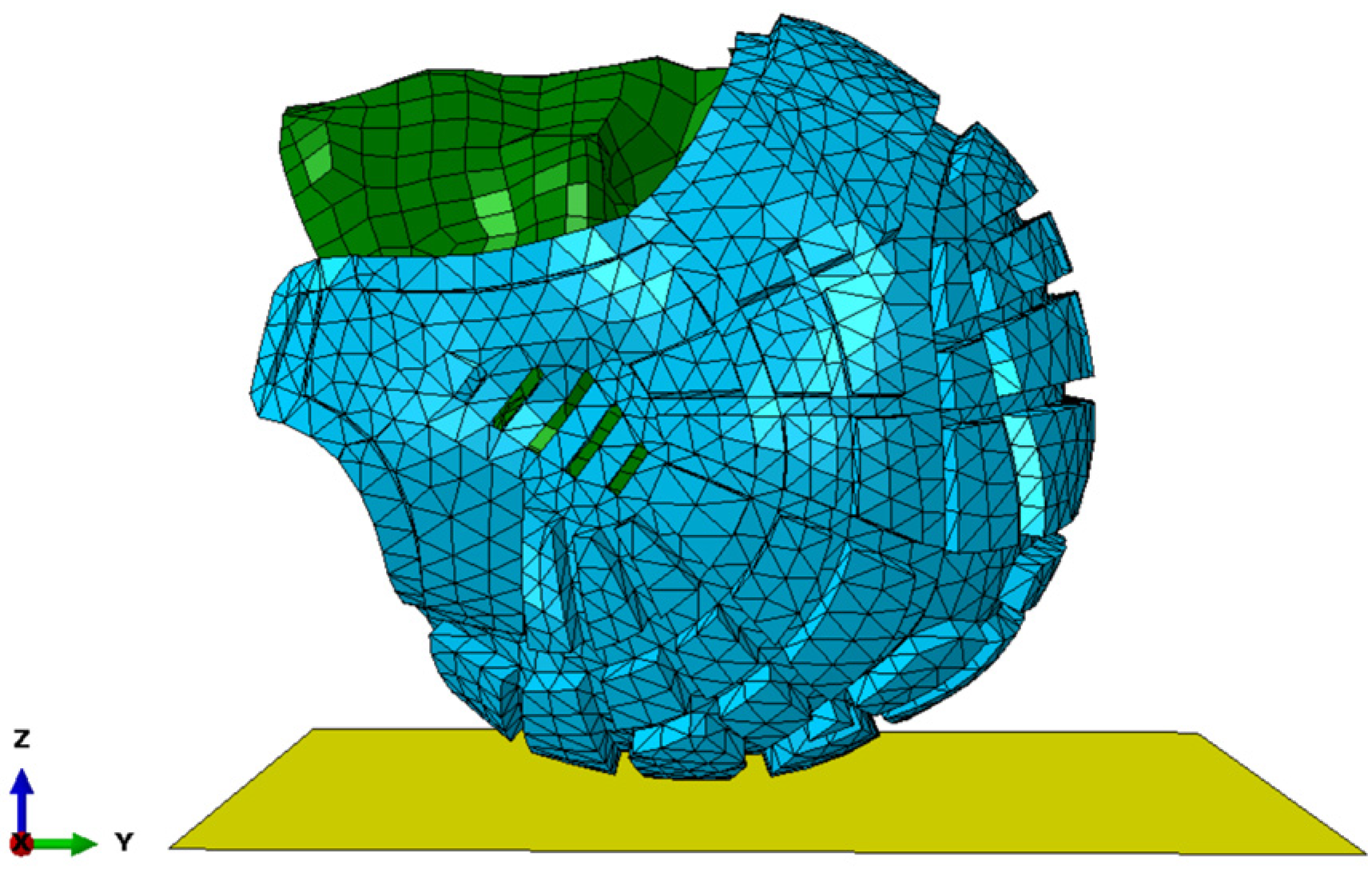
The relatively small sample size of head impact cases simulated in this present study limits the conclusions that can be drawn from the results. However, the results of the simulations do offer preliminary findings which suggest that the N-Pro headguard is effective in attenuating head impacts against a rigid, non-compliant surface, which may be applicable to many cases in contact sports. The primary condition under consideration in our simulations is impact against a rigid, non-compliant surface. While this controlled scenario is valuable for investigating the performance of the headguard without also having to account for many unknown variables, it will not fully represent the diverse range of conditions that are encountered in real-world sporting events. Contact sports involve multiple variables, including different playing surfaces and impact angles, and these have purposely not been considered in this present study. While this approach allows us to assess the effectiveness of the N-Pro headguard in its most conservative scenario, it is essential to acknowledge that real-world head impacts often involve a degree of surface compliance, which serves to absorb and dissipate some of the kinetic energy instead of all the impact energy being transmitted to and absorbed by a player’s head and their headguard. The predicted accelerations, stresses and strains of the present simulations are likely to be lower if ground compliance were to be considered explicitly. Furthermore, the results suggest that a large reduction in rotational and linear accelerations of the head does not necessarily translate to large reductions in brain tissue responses, i.e., Von Mises stresses and maximum principal strains. Hence, the overall results may provide an insight into the added benefits of using a variety of test methods, such as FE modelling, when determining the protective capabilities of sports headguards.




 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}