
Interpretable Machine Learning Predictions of Bruch’s Membrane Opening-Minimum Rim Width Using Retinal Nerve Fiber Layer Values and Visual Field Global Indexes


Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Subjects
2.3. Optical Coherence Tomography
2.4. Perimetry
2.5. Data Preprocessing
2.6. Machine Learning Algorithm
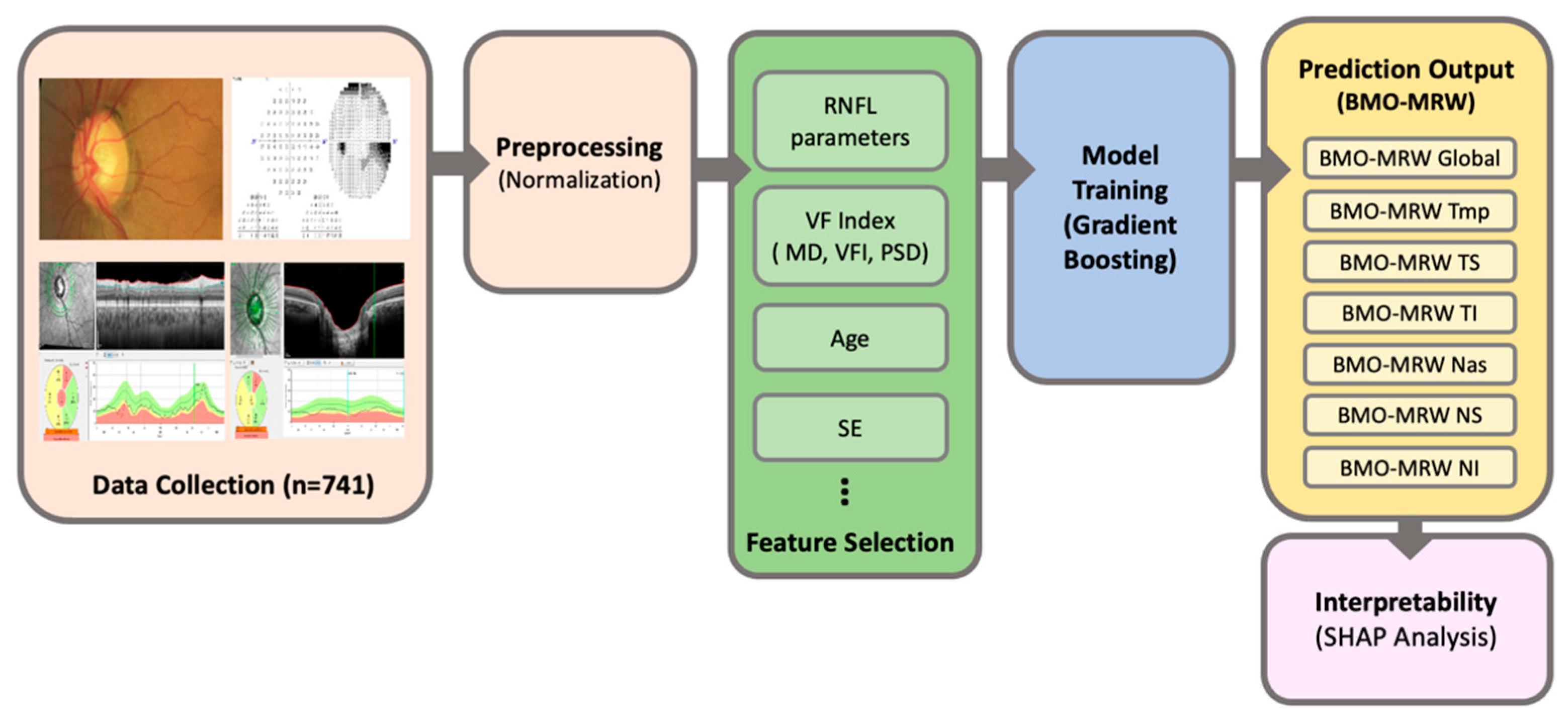
2.7. Workflow of Machine Learning Model for Predicting BMO-MR
2.8. Statistical Analysis
2.9. SHAP (SHapley Additive exPlanations)
3. Results
3.1. Baseline Characteristics of the Dataset
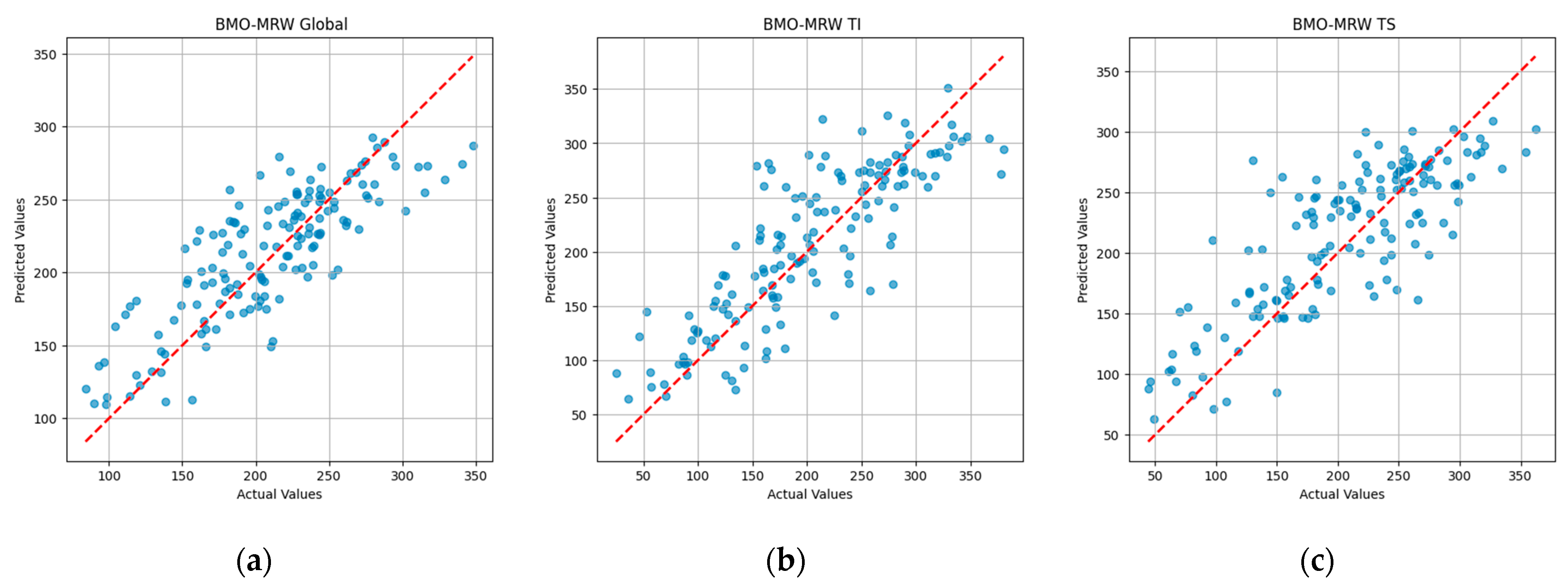
3.2. Prediction Performance a Gradient Boosting Model
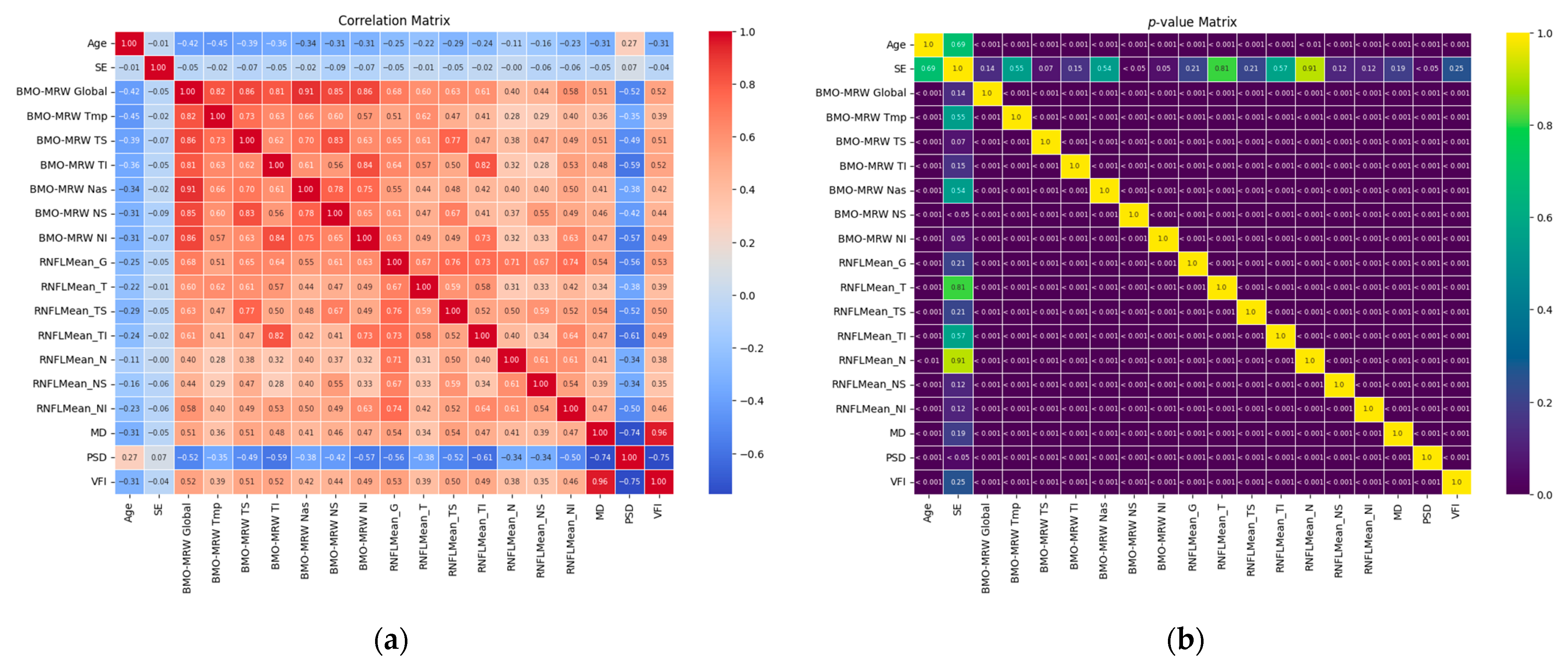
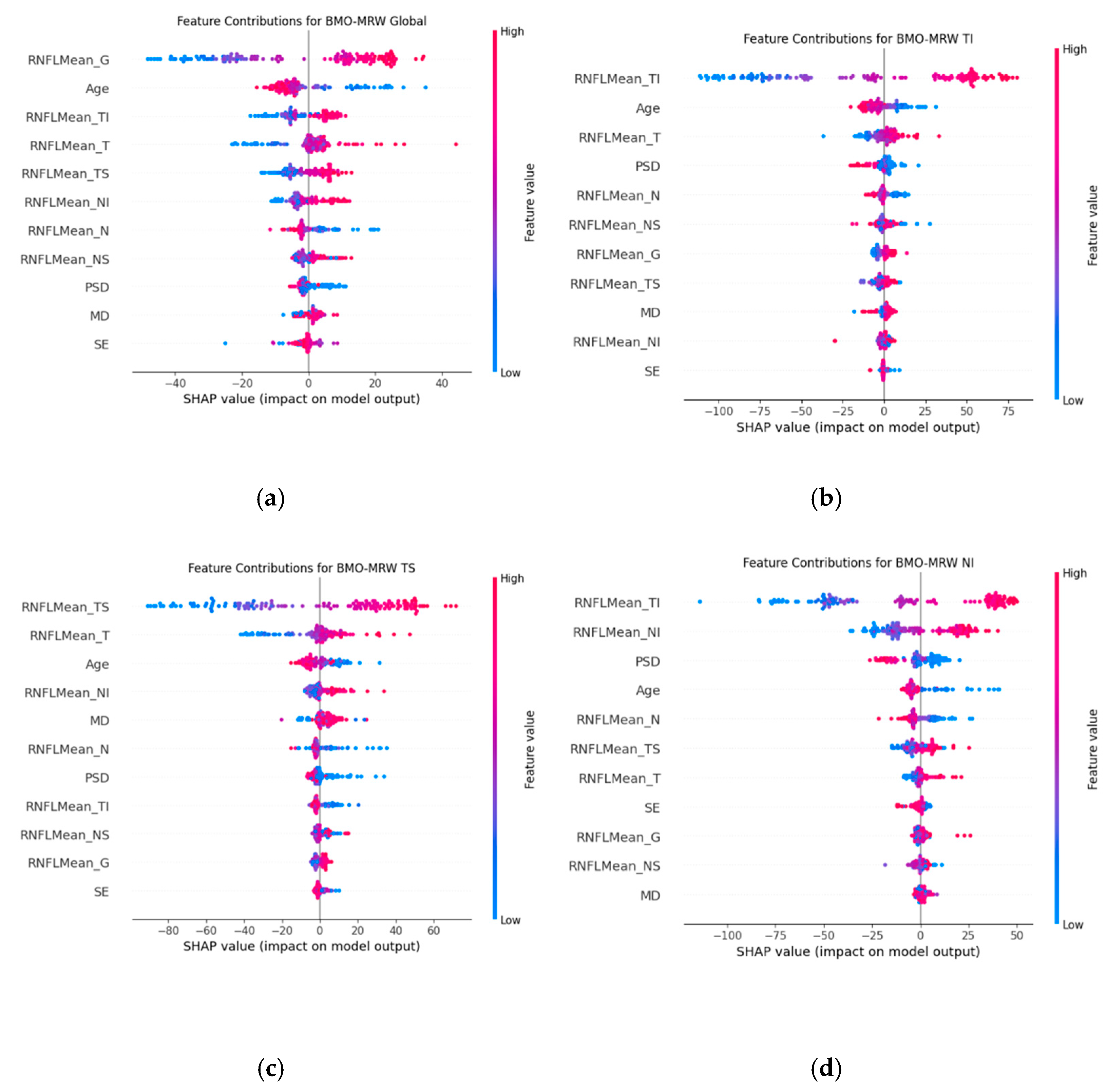
3.3. Correlation Analysis and Interpretable Machine Learning
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| RGCs | retinal ganglion cells |
| RNFL | retinal nerve fibre layer |
| NRR | neuroretinal rim |
| VF | visual field |
| OCT | optical coherence tomography |
| SAP | standard automated perimetry |
| SD-OCT | Spectral-domain optical coherence tomography |
| BMO-MRW | Bruch’s membrane opening-minimum rim width |
| MD | mean deviation |
| PSD | pattern standard deviation |
| VFI | visual field index |
| CNN | convolutional neural network |
| MAE | mean absolute errors |
| NTG | normal tension glaucoma |
| PACG | primary angle closure glaucoma |
| PEX G | pseudoexfoliation glaucoma |
| POAG | primary open-angle glaucoma |
| GS | glaucoma suspect |
| IOP | intraocular pressure |
| FoBMO | fovea-to-Bruch’s membrane opening |
| SITA | Swedish Interactive Threshold Algorithm |
| T | Temporal |
| TS | superotemporal |
| TI | inferotemporal |
| NS | superonasal |
| NI | inferonasal |
| GBR | Gradient Boosting Regression |
| GBDT | Gradient Boosting Decision Trees |
| MAE | Mean Absolute Error |
| MSE | Mean Squared Error |
| SHAP | SHapley Additive exPlanations |
| SE | spherical equivalent |
| CCT | Central corneal thickness |
References
- Weinreb, R.N.; Khaw, P.T. Primary Open-Angle Glaucoma. Lancet 2004, 363, 1711–1720. [Google Scholar] [PubMed]
- Banegas, S.A.; Antón, A.; Morilla, A.; Bogado, M.; Ayala, E.M.; Fernandez-Guardiola, A.; Moreno-Montañes, J. Evaluation of the Retinal Nerve Fiber Layer Thickness, the Mean Deviation, and the Visual Field Index in Progressive Glaucoma. J. Glaucoma 2016, 25, e229–e235. [Google Scholar] [CrossRef] [PubMed]
- Prum, B.E.; Rosenberg, L.F.; Gedde, S.J.; Mansberger, S.L.; Stein, J.D.; Moroi, S.E.; Herndon, L.W.; Lim, M.C.; Williams, R.D. Primary Open-Angle Glaucoma Preferred Practice Pattern(®) Guidelines. Ophthalmology 2016, 123, P41–P111. [Google Scholar] [CrossRef] [PubMed]
- European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 4th Edition—Chapter 3: Treatment principles and options Supported by the EGS Foundation: Part 1: Foreword; Introduction; Glossary; Chapter 3 Treatment principles and options. Br. J. Ophthalmol. 2017, 101, 130–195. [Google Scholar]
- Gardiner, S.K.; Johnson, C.A.; Cioffi, G.A. Evaluation of the Structure-Function Relationship in Glaucoma. Investig. Ophthalmol. Vis. Sci. 2005, 46, 3712–3717. [Google Scholar]
- Ferreras, A.; Pablo, L.E.; Garway-Heath, D.F.; Fogagnolo, P.; García-Feijoo, J. Mapping Standard Automated Perimetry to the Peripapillary Retinal Nerve Fiber Layer in Glaucoma. Investig. Ophthalmol. Vis. Sci. 2008, 49, 3018–3025. [Google Scholar] [CrossRef]
- Leite, M.T.; Zangwill, L.M.; Weinreb, R.N.; Rao, H.L.; Alencar, L.M.; Medeiros, F.A. Structure-Function Relationships Using the Cirrus Spectral Domain Optical Coherence Tomograph and Standard Automated Perimetry. J. Glaucoma 2012, 21, 49–54. [Google Scholar]
- Malik, R.; Swanson, W.H.; Garway-Heath, D.F. ‘Structure-Function Relationship’ in Glaucoma: Past Thinking and Current Concepts. Clin. Exp. Ophthalmol. 2012, 40, 369–380. [Google Scholar]
- The AGIS Investigators. The Advanced Glaucoma Intervention Study (AGIS): 7. The Relationship Between Control of Intraocular Pressure and Visual Field Deterioration. Am. J. Ophthalmol. 2000, 130, 429–440. [Google Scholar] [CrossRef]
- Kass, M.A.; Heuer, D.K.; Higginbotham, E.J.; Johnson, C.A.; Keltner, J.L.; Miller, J.P.; Parrish, R.K., 2nd; Wilson, M.R.; Gordon, M.O. The Ocular Hypertension Treatment Study: A Randomized Trial Determines That Topical Ocular Hypotensive Medication Delays or Prevents the Onset of Primary Open-Angle Glaucoma. Arch. Ophthalmol. 2002, 120, 701–713, Discussion 829–830. [Google Scholar] [CrossRef]
- Keltner, J.L.; Johnson, C.A.; Anderson, D.R.; Levine, R.A.; Fan, J.; Cello, K.E.; Quigley, H.A.; Budenz, D.L.; Parrish, R.K.; Kass, M.A.; et al. The Association Between Glaucomatous Visual Fields and Optic Nerve Head Features in the Ocular Hypertension Treatment Study. Ophthalmology 2006, 113, 1603–1612. [Google Scholar] [CrossRef] [PubMed]
- Hood, D.C.; Kardon, R.H. A Framework for Comparing Structural and Functional Measures of Glaucomatous Damage. Prog. Retin. Eye Res. 2007, 26, 688–710. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, B.C.; Burgoyne, C.F. From Clinical Examination of the Optic Disc to Clinical Assessment of the Optic Nerve Head: A Paradigm Change. Am. J. Ophthalmol. 2013, 156, 218–227.e2. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.C. Spectral Domain Optical Coherence Tomography in Glaucoma: Qualitative and Quantitative Analysis of the Optic Nerve Head and Retinal Nerve Fiber Layer (An AOS Thesis). Trans. Am. Ophthalmol. Soc. 2009, 107, 254–281. [Google Scholar]
- Povazay, B.; Hofer, B.; Hermann, B.M.; Unterhuber, A.; Morgan, J.E.; Glittenberg, C.; Binder, S.; Drexler, W. Minimum Distance Mapping Using Three-Dimensional Optical Coherence Tomography for Glaucoma Diagnosis. J. Biomed. Opt. 2007, 12, 041204. [Google Scholar] [CrossRef]
- Reis, A.S.C.; O’Leary, N.; Yang, H.; Sharpe, G.P.; Nicolela, M.T.; Burgoyne, C.F.; Chauhan, B.C. Influence of Clinically Invisible but Optical Coherence Tomography Detected Optic Disc Margin Anatomy on Neuroretinal Rim Evaluation. Investig. Ophthalmol. Vis. Sci. 2012, 53, 1852–1860. [Google Scholar] [CrossRef]
- Strouthidis, N.G.; Fortune, B.; Yang, H.; Sigal, I.A.; Burgoyne, C.F. Longitudinal Change Detected by Spectral Domain Optical Coherence Tomography in the Optic Nerve Head and Peripapillary Retina in Experimental Glaucoma. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1206–1219. [Google Scholar] [CrossRef]
- Chauhan, B.C.; Danthurebandara, V.M.; Sharpe, G.P.; Demirel, S.; Girkin, C.A.; Mardin, C.Y.; Scheuerle, A.F.; Burgoyne, C.F. Bruch’s Membrane Opening Minimum Rim Width and Retinal Nerve Fiber Layer Thickness in a Normal White Population: A Multicenter Study. Ophthalmology 2015, 122, 1786–1794. [Google Scholar] [CrossRef]
- Chauhan, B.C.; O’Leary, N.; AlMobarak, F.A.; Reis, A.S.; Yang, H.; Sharpe, G.P.; Hutchison, D.M.; Nicolela, M.T.; Burgoyne, C.F. Enhanced Detection of Open-Angle Glaucoma With an Anatomically Accurate Optical Coherence Tomography-Derived Neuroretinal Rim Parameter. Ophthalmology 2013, 120, 535–543. [Google Scholar] [CrossRef]
- Mizumoto, K.; Gosho, M.; Zako, M. Correlation Between Optic Nerve Head Structural Parameters and Glaucomatous Visual Field Indices. Clin. Ophthalmol. 2014, 8, 1203–1208. [Google Scholar]
- Pollet-Villard, F.; Chiquet, C.; Romanet, J.-P.; Noel, C.; Aptel, F. Structure-Function Relationships with Spectral-Domain Optical Coherence Tomography Retinal Nerve Fiber Layer and Optic Nerve Head Measurements. Investig. Ophthalmol. Vis. Sci. 2014, 55, 2953–2962. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, S.K.; Ren, R.; Yang, H.; Fortune, B.; Burgoyne, C.F.; Demirel, S. A Method to Estimate the Amount of Neuroretinal Rim Tissue in Glaucoma: Comparison with Current Methods for Measuring Rim Area. Am. J. Ophthalmol. 2014, 157, 540–549.e2. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.K.; Kee, C. Characteristics of Patients Showing Discrepancy Between Bruch’s Membrane Opening-Minimum Rim Width and Peripapillary Retinal Nerve Fiber Layer Thickness. J. Clin. Med. 2019, 8, 1362. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.C.; Jammal, A.A.; Medeiros, F.A. A Deep Learning Algorithm to Quantify Neuroretinal Rim Loss from Optic Disc Photographs. Am. J. Ophthalmol. 2019, 201, 9. [Google Scholar] [CrossRef]
- Kim, D.; Seo, S.B.; Park, S.J.; Cho, H.K. Deep Learning Visual Field Global Index Prediction with Optical Coherence Tomography Parameters in Glaucoma Patients. Sci. Rep. 2023, 13, 18304. [Google Scholar] [CrossRef]
- Cho, H.K.; Lee, J.; Lee, M.; Kee, C. Initial Central Scotomas vs. Peripheral Scotomas in Normal-Tension Glaucoma: Clinical Characteristics and Progression Rates. Eye 2014, 28, 303–311. [Google Scholar] [CrossRef]
- Foster, P.J.; Buhrmann, R.; Quigley, H.A.; Johnson, G.J. The Definition and Classification of Glaucoma in Prevalence Surveys. Br. J. Ophthalmol. 2002, 86, 238–242. [Google Scholar] [CrossRef]
- Park, D.Y.; Won, H.H.; Cho, H.K.; Kee, C. Evaluation of Lysyl Oxidase-Like 1 Gene Polymorphisms in Pseudoexfoliation Syndrome in a Korean Population. Mol. Vis. 2013, 19, 448–453. [Google Scholar]
- Zemel, R.S.; Pitassi, T. A Gradient-Based Boosting Algorithm for Regression Problems. In Advances in Neural Information Processing Systems 12 (NIPS 2000); MIT Press: Cambridge, MA, USA, 2000. [Google Scholar]
- Seto, H.; Oyama, A.; Kitora, S.; Toki, H.; Yamamoto, R.; Kotoku, J.; Haga, A.; Shinzawa, M.; Yamakawa, M.; Fukui, S.; et al. Gradient Boosting Decision Tree Becomes More Reliable Than Logistic Regression in Predicting Probability for Diabetes with Big Data. Sci. Rep. 2022, 12, 15889. [Google Scholar] [CrossRef]
- Jiang, J.; Wang, R.; Wang, M.; Gao, K.; Nguyen, D.D.; Wei, G.W. Boosting Tree-Assisted Multitask Deep Learning for Small Scientific Datasets. J. Chem. Inf. Model. 2020, 60, 1235–1244. [Google Scholar] [CrossRef]
- Emami, S.; Martínez-Muñoz, G. Multioutput Regression Neural Network Training via Gradient Boosting. In Proceedings of the ESANN 2022, European Symposium on Artificial Neural Networks, Computational Intelligence and Machine Learning, Bruges, Belgium, 5–7 October 2022. [Google Scholar]
- Benesty, J.; Chen, J.; Huang, Y.; Cohen, I. Pearson Correlation Coefficient. In Noise Reduction in Speech Processing; Cohen, I., Huang, Y., Chen, J., Benesty, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2009; pp. 1–4. [Google Scholar]
- Lundberg, S.M.; Lee, S.I. A Unified Approach to Interpreting Model Predictions. Adv. Neural Inf. Process. Syst. 2017, 31, 4765–4774. [Google Scholar]
- Lundberg, S.M.; Erion, G.; Chen, H.; DeGrave, A.; Prutkin, J.M.; Nair, B.; Katz, R.; Himmelfarb, J.; Bansal, N.; Lee, S.I. From Local Explanations to Global Understanding with Explainable AI for Trees. Nat. Mach. Intell. 2020, 2, 56–67. [Google Scholar] [CrossRef] [PubMed]
- Yang, J. Fast TreeSHAP: Accelerating SHAP Value Computation for Trees. arXiv 2021, arXiv:2109.09847. [Google Scholar]
- Toshev, A.P.; Lamparter, J.; Pfeiffer, N.; Hoffmann, E.M. Bruch’s Membrane Opening-Minimum Rim Width Assessment with Spectral-Domain Optical Coherence Tomography Performs Better than Confocal Scanning Laser Ophthalmoscopy in Discriminating Early Glaucoma Patients from Control Subjects. J. Glaucoma 2017, 26, 27. [Google Scholar] [CrossRef]
- Seo, S.B.; Cho, H.K. Deep Learning Classification of Early Normal-Tension Glaucoma and Glaucoma Suspects Using Bruch’s Membrane Opening-Minimum Rim Width and RNFL. Sci. Rep. 2020, 10, 19042. [Google Scholar] [CrossRef]
- Cho, H.K.; Kee, C. Comparison of Rate of Change Between Bruch’s Membrane Opening Minimum Rim Width and Retinal Nerve Fiber Layer in Eyes Showing Optic Disc Hemorrhage. Am. J. Ophthalmol. 2020, 217, 27–37. [Google Scholar] [CrossRef]
- Phu, J.; Khuu, S.K.; Agar, A.; Kalloniatis, M. Clinical Evaluation of Swedish Interactive Thresholding Algorithm-Faster Compared with Swedish Interactive Thresholding Algorithm-Standard in Normal Subjects, Glaucoma Suspects, and Patients with Glaucoma. Am. J. Ophthalmol. 2019, 208, 251–264. [Google Scholar] [CrossRef]
- Sengupta, S.; Singh, A.; Leopold, H.A.; Gulati, T.; Lakshminarayanan, V. Ophthalmic Diagnosis Using Deep Learning with Fundus Images—A Critical Review. Artif. Intell. Med. 2020, 102, 101758. [Google Scholar] [CrossRef]
- Gaasterland, D.; Tanishima, T.; Kuwabara, T. Axoplasmic Flow During Chronic Experimental Glaucoma. 1. Light and Electron Microscopic Studies of the Monkey Optic Nerve Head During Development of Glaucomatous Cupping. Investig. Ophthalmol. Vis. Sci. 1978, 17, 838–846. [Google Scholar]
- Rao, H.L.; Kumar, A.U.; Babu, J.G.; Senthil, S.; Garudadri, C.S. Relationship Between Severity of Visual Field Loss at Presentation and Rate of Visual Field Progression in Glaucoma. Ophthalmology 2011, 118, 249–253. [Google Scholar] [CrossRef]
- Minckler, D.S.; Bunt, A.H.; Johanson, G.W. Orthograde and Retrograde Axoplasmic Transport During Acute Ocular Hypertension in the Monkey. Investig. Ophthalmol. Vis. Sci. 1977, 16, 426–441. [Google Scholar]
- Quigley, H.A.; Addicks, E.M.; Green, W.R.; Maumenee, A.E. Optic Nerve Damage in Human Glaucoma. II. The Site of Injury and Susceptibility to Damage. Arch. Ophthalmol. 1981, 99, 635–649. [Google Scholar]
- Quigley, H.A.; Hohman, R.M.; Addicks, E.M.; Massof, R.W.; Green, R. Morphologic Changes in the Lamina Cribrosa Correlated with Neural Loss in Open-Angle Glaucoma. Am. J. Ophthalmol. 1983, 95, 673–691. [Google Scholar] [PubMed]
- Jonas, J.B.; Fernandez, M.C.; Sturmer, J. Pattern of Glaucomatous Neuroretinal Rim Loss. Ophthalmology 1993, 100, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Jonas, J.B.; Mardin, C.Y.; Schlotzer-Schrehardt, U.; Naumann, G.O. Morphometry of the Human Lamina Cribrosa Surface. Investig. Ophthalmol. Vis. Sci. 1991, 32, 401–405. [Google Scholar]
- Bowd, C.; Zangwill, L.M.; Weinreb, R.N.; Girkin, C.A.; Fazio, M.A.; Liebmann, J.M.; Belghith, A. Racial Differences in Rate of Change of Spectral-Domain Optical Coherence Tomography-Measured Minimum Rim Width and Retinal Nerve Fiber Layer Thickness. Am. J. Ophthalmol. 2018, 196, 154–164. [Google Scholar]
- Casas-Llera, P.; Rebolleda, G.; Munoz-Negrete, F.J.; Arnalich-Montiel, F.; Perez-Lopez, M.; Fernandez-Buenaga, R. Visual Field Index Rate and Event-Based Glaucoma Progression Analysis: Comparison in a Glaucoma Population. Br. J. Ophthalmol. 2009, 93, 1576–1579. [Google Scholar]
- Vianna, J.R.; Danthurebandara, V.M.; Sharpe, G.P.; Hutchison, D.M.; Belliveau, A.C.; Shuba, L.M.; Nicolela, M.T.; Chauhan, B.C. Importance of Normal Aging in Estimating the Rate of Glaucomatous Neuroretinal Rim and Retinal Nerve Fiber Layer Loss. Ophthalmology 2015, 122, 2392–2398. [Google Scholar]
- Cho, H.K.; Kee, C. Population-Based Glaucoma Prevalence Studies in Asians. Surv. Ophthalmol. 2014, 59, 434–447. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mean ± Std |
|---|---|
| Number of subjects | 741 eyes (741 patients) |
| Mean Age (year) | 53.62 ± 13.53 |
| Female gender (%) | 45.21 (335/741) |
| Family history of glaucoma (%) | 8.1 (60/741) |
| Diagnosis | |
| NTG | 308 |
| POAG | 105 |
| PEX G | 63 |
| PACG | 36 |
| Glaucoma suspect | 229 |
| Spherical equivalent (D) | −1.67 ± 3.30 |
| CCT (um) | 542.43 ± 42.70 |
| Baseline IOP (mmHg) | 15.51 ± 4.14 |
| MD (dB) | −5.74 ± 35.11 |
| PSD (dB) | 5.29 ± 4.16 |
| VFI (%) | 88.37 ± 12.29 |
| RNFL Global | 85.08 ± 21.40 |
| RNFL Tmp | 69.81 ± 17.43 |
| RNFL TS | 113.37 ± 37.63 |
| RNFL TI | 111.51 ± 46.90 |
| RNFL Nas | 68.15 ± 18.28 |
| RNFL NS | 100.29 ± 30.94 |
| RNFL NI | 93.09 ± 28.94 |
| BMO-MRW Global | 215.10 ± 58.44 |
| BMO-MRW Tmp | 167.16 ± 48.05 |
| BMO-MRW TS | 212.46 ± 74.42 |
| BMO-MRW TI | 214.36 ± 86.38 |
| BMO-MRW Nas | 233.17 ± 67.92 |
| BMO-MRW NS | 242.01 ± 73.53 |
| BMO-MRW NI | 249.83 ± 82.15 |
| Targets | MAE | MSE | R2 |
|---|---|---|---|
| BMO-MRW Global | 25.17 | 1007.74 | 0.67 |
| BMO-MRW Tmp | 27.95 | 1278.75 | 0.46 |
| BMO-MRW TS | 34.42 | 1876.91 | 0.64 |
| BMO-MRW TI | 34.91 | 1999.98 | 0.68 |
| BMO-MRW Nas | 38.77 | 2403.80 | 0.40 |
| BMO-MRW NS | 35.94 | 2100.00 | 0.54 |
| BMO-MRW NI | 34.08 | 1889.31 | 0.70 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seo, S.B.; Cho, H.-k. Interpretable Machine Learning Predictions of Bruch’s Membrane Opening-Minimum Rim Width Using Retinal Nerve Fiber Layer Values and Visual Field Global Indexes. Bioengineering 2025, 12, 321. https://doi.org/10.3390/bioengineering12030321
Seo SB, Cho H-k. Interpretable Machine Learning Predictions of Bruch’s Membrane Opening-Minimum Rim Width Using Retinal Nerve Fiber Layer Values and Visual Field Global Indexes. Bioengineering. 2025; 12(3):321. https://doi.org/10.3390/bioengineering12030321
Chicago/Turabian StyleSeo, Sat Byul, and Hyun-kyung Cho. 2025. "Interpretable Machine Learning Predictions of Bruch’s Membrane Opening-Minimum Rim Width Using Retinal Nerve Fiber Layer Values and Visual Field Global Indexes" Bioengineering 12, no. 3: 321. https://doi.org/10.3390/bioengineering12030321
APA StyleSeo, S. B., & Cho, H.-k. (2025). Interpretable Machine Learning Predictions of Bruch’s Membrane Opening-Minimum Rim Width Using Retinal Nerve Fiber Layer Values and Visual Field Global Indexes. Bioengineering, 12(3), 321. https://doi.org/10.3390/bioengineering12030321