
Identifying Hypertrophic or Dilated Cardiomyopathy: Development and Validation of a Fine-Tuned ResNet50 Model Based on Electrocardiogram Image


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. ECG Image Preprocessing and Validation
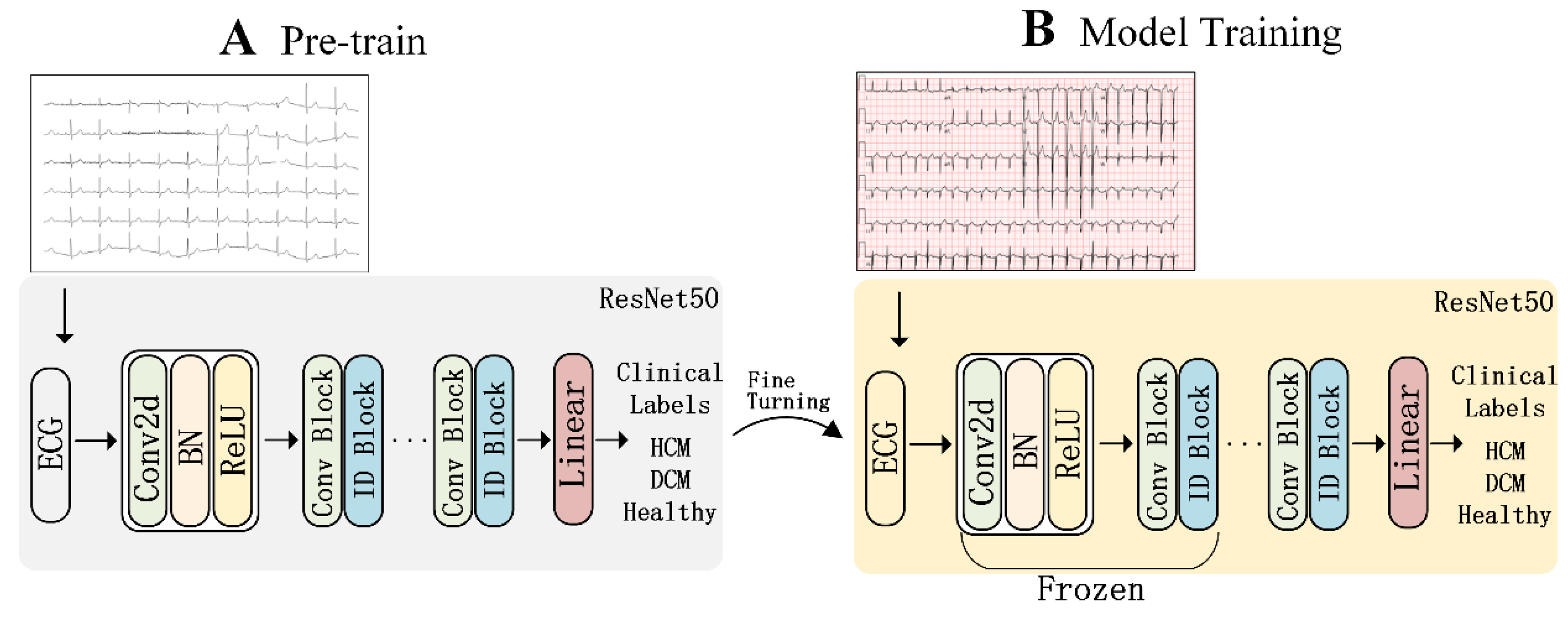
2.3. Model Method
2.4. Model Training
3. Results
3.1. Detection of DCM
3.2. Detection of HCM
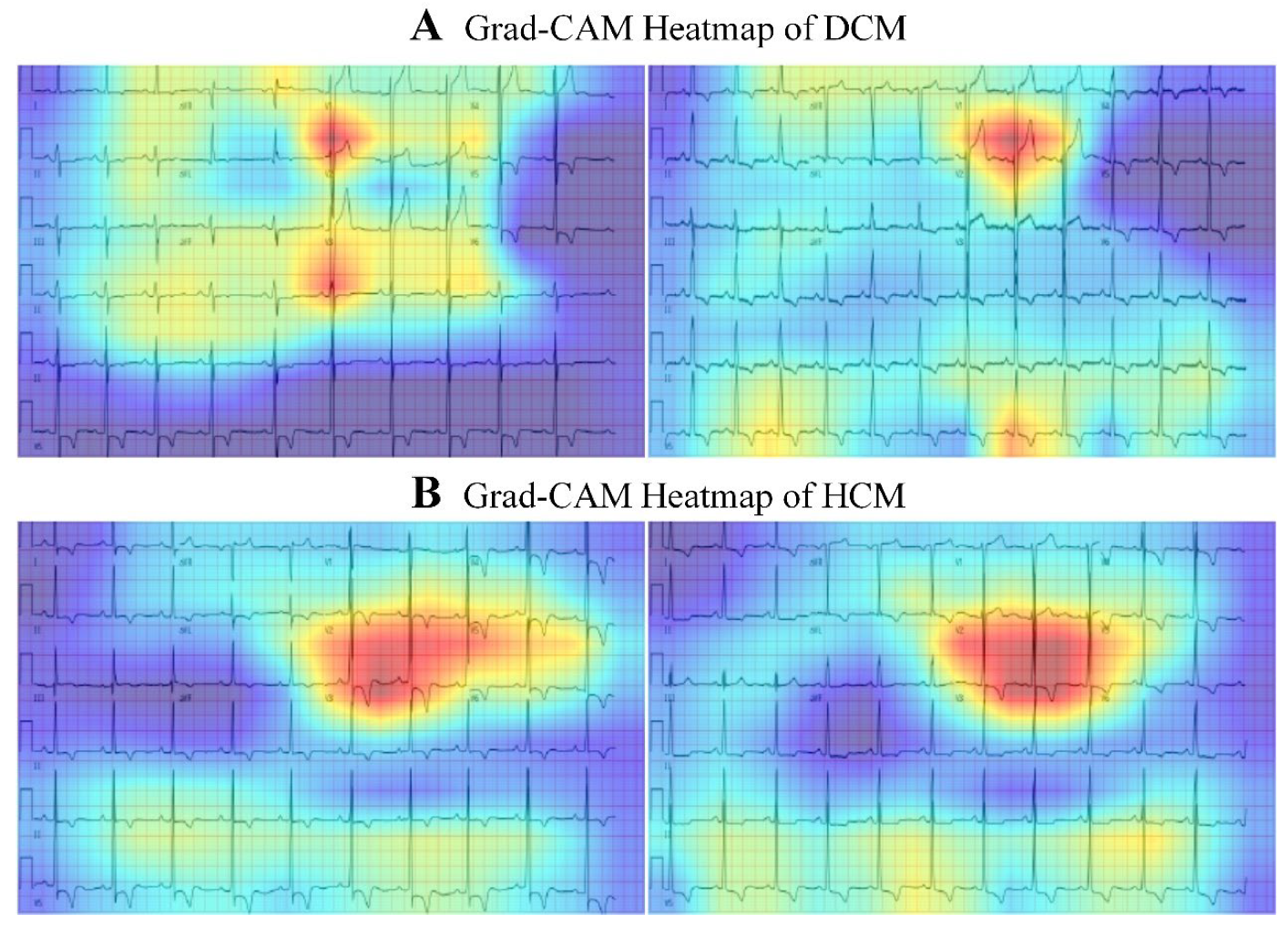
3.3. Localization of Predictive Clues for HCM/DCM
3.4. Temporal Validation
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
References
- Heymans, S.; Lakdawala, N.K.; Tschöpe, C.; Klingel, K. Dilated cardiomyopathy: Causes, mechanisms, and current and future treatment approaches. Lancet 2023, 402, 998–1011. [Google Scholar] [CrossRef]
- Japp, A.G.; Gulati, A.; Cook, S.A.; Cowie, M.R.; Prasad, S.K. The Diagnosis and Evaluation of Dilated Cardiomyopathy. J. Am. Coll. Cardiol. 2016, 67, 2996–3010. [Google Scholar] [CrossRef] [PubMed]
- Finocchiaro, G.; Sheikh, N.; Biagini, E.; Papadakis, M.; Maurizi, N.; Sinagra, G.; Pelliccia, A.; Rapezzi, C.; Sharma, S.; Olivotto, I.; et al. The electrocardiogram in the diagnosis and management of patients with hypertrophic cardiomyopathy. Heart Rhythm 2020, 17, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Gossios, T.; Savvatis, K.; Zegkos, T.; Ntelios, D.; Rouskas, P.; Parcharidou, D.; Karvounis, H.; Efthimiadis, G.K. Deciphering hypertrophic cardiomyopathy with electrocardiography. Heart Fail. Rev. 2022, 27, 1313–1323. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, P.; Suszko, A.M.; Viswanathan, K.; Sheikholeslami, K.; Spears, D.; Adler, A.; Woo, A.; Rakowski, H.; Chauhan, V.S. Microvolt QRS Alternans in Hypertrophic Cardiomyopathy: A Novel Risk Marker of Late Ventricular Arrhythmias. J. Am. Heart Assoc. 2021, 10, e022036. [Google Scholar] [CrossRef]
- Ogura, S.; Nakamura, K.; Morita, H.; Toh, N.; Nakagawa, K.; Yoshida, M.; Watanabe, A.; Nishii, N.; Miyoshi, T.; Ito, H. New Appearance of Fragmented QRS as a Predictor of Ventricular Arrhythmic Events in Patients with Hypertrophic Cardiomyopathy. Circ. J. 2020, 84, 487–494. [Google Scholar] [CrossRef]
- Güner, A.; Kalçık, M.; Çelik, M.; Uzun, F.; Çizgici, A.Y.; Ağuş, H.Z.; Aslan, S.; Güner, E.G.; Ulutaş, A.E.; Bayam, E.; et al. Impaired repolarization parameters may predict fatal ventricular arrhythmias in patients with hypertrophic cardiomyopathy (from the CILICIA Registry). J. Electrocardiol. 2020, 63, 83–90. [Google Scholar] [CrossRef]
- Ratheendran, A.C.; Subramanian, M.; Bhanu, D.K.; Prabhu, M.A.; Kannan, R.; Natarajan, K.U.; Saritha Sekhar, S.; Thachathodiyil, R.; Harikrishnan, M.S.; Pai, P.G. Fragmented QRS on electrocardiography as a predictor of myocardial scar in patients with hypertrophic cardiomyopathy. Acta Cardiol. 2020, 75, 42–46. [Google Scholar] [CrossRef]
- Cau, R.; Pisu, F.; Suri, J.S.; Montisci, R.; Gatti, M.; Mannelli, L.; Gong, X.; Saba, L. Artificial Intelligence in the Differential Diagnosis of Cardiomyopathy Phenotypes. Diagnostics 2024, 14, 156. [Google Scholar] [CrossRef]
- Haimovich, J.S.; Diamant, N.; Khurshid, S.; Di Achille, P.; Reeder, C.; Friedman, S.; Singh, P.; Spurlock, W.; Ellinor, P.T.; Philippakis, A.; et al. Artificial intelligence-enabled classification of hypertrophic heart diseases using electrocardiograms. Cardiovasc. Digit. Health J. 2023, 4, 48–59. [Google Scholar] [CrossRef]
- Tayal, U.; Prasad, S.K.; Voges, I.; Choudhary, P.; Oliver, J.M.; Knight, D.S.; Pennell, D.J.; Frenneaux, M.P.; Newsome, S.; Li, C.; et al. Precision Phenotyping of Dilated Cardiomyopathy Using Multidimensional Data. J. Am. Coll. Cardiol. 2022, 79, 2219–2232. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, S.; Gajjar, S.; Sengupta, P.P.; Narula, J. Artificial Intelligence-Enabled Electrocardiography to Screen Patients with Dilated Cardiomyopathy. Am. J. Cardiol. 2021, 155, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Lin, X.; Wang, K.; Zhou, Y.; Li, Q.; Wang, Y.; Tang, R.; Jin, M.; Deng, L.; Chen, H. Echocardiography-based machine learning algorithm for distinguishing ischemic cardiomyopathy from dilated cardiomyopathy. BMC Cardiovasc. Disord. 2023, 23, 476. [Google Scholar] [CrossRef]
- Stamenov, D.; Gusev, M.; Armenski, G. Interoperability of ECG standards. In Proceedings of the 2018 41st International Convention on Information and Communication Technology, Electronics and Microelectronics (MIPRO), Opatija, Croatia, 21–25 May 2018. [Google Scholar]
- Huang, J.; Chen, B.; Yao, B.; He, W. ECG Arrhythmia Classification Using STFT-Based Spectrogram and Convolutional Neural Network. IEEE Access 2019, 7, 92871–92880. [Google Scholar] [CrossRef]
- Ullah, A.; Anwar, S.M.; Bilal, M.; Mehmood, R.M. Classification of Arrhythmia by Using Deep Learning with 2-D ECG Spectral Image Representation. Remote Sens. 2020, 12, 1685. [Google Scholar] [CrossRef]
- Diker, A.; Avci, D.; Avci, E.; Gedikpınar, M. A Novel Application based on Spectrogram and Convolutional Neural Network for ECG Classification. In Proceedings of the 1st International Informatics and Software Engineering Conference (UBMYK), Ankara, Turkey, 6–7 November 2019. [Google Scholar]
- Maron, B.J.; Desai, M.Y.; Nishimura, R.A.; Spirito, P.; Rakowski, H.; Towbin, J.A.; Rowin, E.J.; Maron, M.S.; Sherrid, M.V. Diagnosis and Evaluation of Hypertrophic Cardiomyopathy: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2022, 79, 372–389. [Google Scholar] [CrossRef]
- Elliott, P.M.; Anastasakis, A.; Borger, M.A.; Borggrefe, M.; Cecchi, F.; Charron, P.; Hagege, A.A.; Lafont, A.; Limongelli, G.; Mahrholdt, H.; et al. 2014 ESC Guidelines on Diagnosis and Management of Hypertrophic Cardiomyopathy. Eur. Heart J. 2014, 35, 2733–2779. [Google Scholar] [CrossRef]
- Ommen, S.R.; Mital, S.; Burke, M.A.; Day, S.M.; Deswal, A.; Elliott, P.; Evanovich, L.L.; Hung, J.; Joglar, J.A.; Kantor, P.; et al. 2020 AHA/ACC Guideline for the Diagnosis and Treatment of Patients with Hypertrophic Cardiomyopathy. Circulation 2020, 142, e533–e557. [Google Scholar] [CrossRef]
- Richardson, P.; McKenna, W.; Bristow, M.; Maisch, B.; Mautner, B.; O’Connell, J.; Olsen, E.; Thiene, G.; Goodwin, J.; Gyarfas, I.; et al. Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the Definition and Classification of Cardiomyopathies. Circulation 1996, 93, 841–842. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016. [Google Scholar]
- Devries, T.; Taylor, G.W. Improved Regularization of Convolutional Neural Networks with Cutout. arXiv 2017, arXiv:1708.04552v2. [Google Scholar]
- Kingma, D.; Ba, J. Adam: A Method for Stochastic Optimization. In Proceedings of the 3rd International Conference for Learning Representations (ICLR 2015), San Diego, CA, USA, 7–9 May 2015. [Google Scholar]
- Nguyen, Q.; Valizadegan, H.; Hauskrecht, M. Learning Classification Models with Soft-Label Information. J. Am. Med. Inform. Assoc. 2014, 21, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Arbelo, E.; Protonotarios, A.; Gimeno, J.R.; Barriales-Villa, R.; Garcia-Pavia, P.; Monserrat, L.; Elliott, P.M.; Anastasakis, A.; Rapezzi, C.; Alonso-Pulpon, L.; et al. 2023 ESC Guidelines for the Management of Cardiomyopathies. Eur. Heart J. 2023, 44, 3503–3626. [Google Scholar] [CrossRef] [PubMed]
- Siontis, K.C.; Liu, K.; Bos, J.M.; Attia, Z.I.; Cohen-Shelly, M.; Arruda-Olson, A.M.; Asirvatham, S.J.; Friedman, P.A.; Noseworthy, P.A. Artificial Intelligence-Enhanced Electrocardiography in Cardiovascular Disease Management. Nat. Rev. Cardiol. 2021, 18, 465–478. [Google Scholar] [CrossRef]
- Sheikh, N.; Papadakis, M.; Ghani, S.; Zaidi, A.; Gati, S.; Adami, P.E.; Carré, F.; Schnell, F.; Wilson, M.G.; Avila, P.; et al. Comparison of Hypertrophic Cardiomyopathy in Afro-Caribbean Versus White Patients in the UK. Heart 2016, 102, 1797–1804. [Google Scholar] [CrossRef]
- Siontis, K.C.; Liu, K.; Bos, J.M.; Attia, Z.I.; Cohen-Shelly, M.; Arruda-Olson, A.M.; Asirvatham, S.J.; Friedman, P.A.; Noseworthy, P.A. Saliency Maps Provide Insights into Artificial Intelligence-Based Electrocardiography Models for Detecting Hypertrophic Cardiomyopathy. J. Electrocardiol. 2023, 81, 286–291. [Google Scholar] [CrossRef]
- Ma, F.; Luo, W.; Sun, B.; Gao, Y.; Wang, J.; Yu, J.; Zhang, H.; Li, Z.; Wang, X.; Li, Y.; et al. Twenty-Four Hour Variability of Inverted T-Waves in Patients with Apical Hypertrophic Cardiomyopathy. Front. Cardiovasc. Med. 2022, 9, 1004178. [Google Scholar] [CrossRef]
- Ko, W.-Y.; Siontis, K.C.; Attia, Z.I.; Carter, R.E.; Kapa, S.; Ommen, S.R.; Demuth, S.J.; Ackerman, M.J.; Gersh, B.J.; Friedman, P.A.; et al. Detection of Hypertrophic Cardiomyopathy Using a Convolutional Neural Network-Enabled Electrocardiogram. J. Am. Coll. Cardiol. 2020, 75, 722–733. [Google Scholar] [CrossRef]
- Orphanou, N.; Papatheodorou, E.; Anastasakis, A. Dilated Cardiomyopathy in the Era of Precision Medicine: Latest Concepts and Developments. Heart Fail. Rev. 2022, 27, 1173–1191. [Google Scholar] [CrossRef]
- Bernardini, A.; Crotti, L.; Olivotto, I.; Cecchi, F. Diagnostic and Prognostic Electrocardiographic Features in Patients with Hypertrophic Cardiomyopathy. Eur. Heart J. Suppl. 2023, 25 (Suppl. C), C173–C178. [Google Scholar] [CrossRef]
- Zhao, Y.; Wang, Q.; Chen, H.; Li, X.; Liu, Y.; Xu, J.; Sun, B.; Zhang, Y.; Wu, J.; Zhou, X.; et al. A Study of the Clinical Application Value of Ultrasound and Electrocardiogram in the Differential Diagnosis of Cardiomyopathy. Am. J. Transl. Res. 2021, 13, 5200–5207. [Google Scholar] [PubMed]
- Chayanopparat, P.; Sanghvi, S.; Kanjanahattakij, N.; Rattanawong, P.; Kewcharoen, J.; Mekara, K.; Dong, Y.; Pumill, C.A.; Lyon, K.; Sutamtewagul, G.; et al. Electrocardiographic Characteristics Associated with Late Gadolinium Enhancement and Prognostic Value in Patients with Dilated Cardiomyopathy. Front. Cardiovasc. Med. 2023, 10, 1281563. [Google Scholar] [CrossRef] [PubMed]
- Becker, M.A.J.; Cornel, J.H.; van de Ven, P.M.; van Rossum, A.C.; Allaart, C.P.; Germans, T. The Prognostic Value of Late Gadolinium-Enhanced Cardiac Magnetic Resonance Imaging in Nonischemic Dilated Cardiomyopathy: A Review and Meta-Analysis. JACC Cardiovasc. Imaging 2018, 11, 1274–1284. [Google Scholar] [CrossRef]
- Zeppenfeld, K.; Tfelt-Hansen, J.; de Riva, M.; Winkel, B.G.; Behr, E.R.; Blom, N.A.; Charron, P.; Corrado, D.; Dagres, N.; Eckardt, L.; et al. 2022 ESC Guidelines for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death. Eur. Heart J. 2022, 43, 3997–4126. [Google Scholar] [CrossRef]
- Goldberger, J.J.; Subačius, H.; Patel, T.; Cunnane, R.; Kadish, A.H. Sudden Cardiac Death Risk Stratification in Patients with Nonischemic Dilated Cardiomyopathy. J. Am. Coll. Cardiol. 2014, 63, 1879–1889. [Google Scholar] [CrossRef]
- Finocchiaro, G.; Merlo, M.; Sheikh, N.; De Angelis, G.; Papadakis, M.; Olivotto, I.; Rapezzi, C.; Carr-White, G.; Sharma, S.; Mestroni, L.; et al. The Electrocardiogram in the Diagnosis and Management of Patients with Dilated Cardiomyopathy. Eur. J. Heart Fail. 2020, 22, 1097–1107. [Google Scholar] [CrossRef]
- Bhattacharya, M.; Lu, D.; Guddeti, R.R.; Matsouaka, R.A.; Chahal, A.A.; Noseworthy, P.A.; Desai, M.Y.; Cremer, P.C.; Wu, K.C.; Taylor, A.L.; et al. Identifying Ventricular Arrhythmias and Their Predictors by Applying Machine Learning Methods to Electronic Health Records in Patients with Hypertrophic Cardiomyopathy (HCM-VAr-Risk Model). Am. J. Cardiol. 2019, 123, 1681–1689. [Google Scholar] [CrossRef]
- Rahman, Q.; Tereshchenko, L.G.; Kongkatong, M.; Abraham, T.; Abraham, M.R.; Shatkay, H. Utilizing ECG-Based Heartbeat Classification for Hypertrophic Cardiomyopathy Identification. IEEE Trans. NanoBiosci. 2015, 14, 505–512. [Google Scholar] [CrossRef]
- Siontis, K.C.; Liu, K.; Bos, J.M.; Attia, Z.I.; Cohen-Shelly, M.; Arruda-Olson, A.M.; Farahani, N.Z.; Friedman, P.A.; Noseworthy, P.A.; Ackerman, M.J. Detection of Hypertrophic Cardiomyopathy by an Artificial Intelligence Electrocardiogram in Children and Adolescents. Int. J. Cardiol. 2021, 340, 42–47. [Google Scholar] [CrossRef]
- Guo, L.; Gao, C.; Yang, W.; Ma, Z.; Zhou, M.; Liu, J.; Shao, H.; Wang, B.; Hu, G.; Zhao, H.; et al. Derivation and Validation of a Detecting Model for Hypertrophic Cardiomyopathy Based on Electrocardiogram Features. Front. Cardiovasc. Med. 2022, 9, 889523. [Google Scholar] [CrossRef]
- Ommen, S.R.; Mital, S.; Burke, M.A.; Day, S.M.; Deswal, A.; Elliott, P.; Evanovich, L.L.; Hung, J.; Joglar, J.A.; Kantor, P.; et al. 2020 AHA/ACC Guideline for the Diagnosis and Treatment of Patients with Hypertrophic Cardiomyopathy: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2020, 142, e558–e631. [Google Scholar] [CrossRef]
- Drezner, J.A.; Ackerman, M.J.; Anderson, J.; Ashley, E.; Asplund, C.A.; Baggish, A.L.; Börjesson, M.; Cannon, B.C.; Corrado, D.; DiFiori, J.P.; et al. Electrocardiographic Interpretation in Athletes: The ’Seattle Criteria’. Br. J. Sports Med. 2013, 47, 122–124. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, N.; Papadakis, M.; Ghani, S.; Zaidi, A.; Gati, S.; Adami, P.E.; Carré, F.; Schnell, F.; Wilson, M.; Avila, P.; et al. Comparison of Electrocardiographic Criteria for the Detection of Cardiac Abnormalities in Elite Black and White Athletes. Circulation 2014, 129, 1637–1649. [Google Scholar] [CrossRef] [PubMed]
- Tison, G.H.; Zhang, J.; Delling, F.N.; Deo, R.C. Automated and Interpretable Patient ECG Profiles for Disease Detection, Tracking, and Discovery. Circ. Cardiovasc. Qual. Outcomes 2019, 12, e005289. [Google Scholar] [CrossRef] [PubMed]
- Dai, H.; Hwang, H.G.; Tseng, V.S. Convolutional Neural Network-Based Automatic Detecting Tool for Cardiovascular Diseases Using Different Intervals of ECG Signals. Comput. Methods Programs Biomed. 2021, 203, 106035. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Labels (DCM/HCM) | No | Precision | Recall | F1 | AUROC | AUPRC |
|---|---|---|---|---|---|---|
| All | 859 | 0.995/0.925 | 0.991/0.877 | 0.991/0.900 | 0.996/0.980 | 0.944/0.951 |
| Male | 485 | 0.993/0.933 | 0.991/0.913 | 0.992/0.923 | 0.993/0.975 | 0.897/0.957 |
| Female | 374 | 0.997/0.9 | 0.994/0.818 | 0.995/0.857 | 0.998/0.998 | 0.955/0.943 |
| ≥65 y | 56 | 1.0/1.0 | 0.959/0.777 | 0.979/0.875 | 1.0/1.0 | 1.0/1.0 |
| <65 y | 803 | 0.993/0.888 | 0.989/0.833 | 0.991/0.860 | 0.995/0.979 | 0.887/0.939 |
| Atrial fibrillation or flutter | 9 | 1.0/1.0 | 0.333/0.333 | 0.5/0.5 | 0.944/0.944 | 0.943/0.902 |
| No atrial fibrillation or flutter | 850 | 0.993/0.901 | 0.99/0.851 | 0.991/0.876 | 0.996/0.979 | 0.906/0.949 |
| left ventricular high voltage | 36 | 0.892/0.892 | 0.961/0.961 | 0.925/0.925 | 0.923/0.942 | 0.812/0.968 |
| No left ventricular high voltage | 823 | 0.996/0.892 | 0.992/0.806 | 0.994/0.847 | 0.997/0.937 | 0.911/0.918 |
| Abnormal Q | 13 | 0.857/0.857 | 0.857/0.857 | 0.923/0.920 | 0.974/0.980 | 0.857/0.857 |
| No Abnormal Q | 846 | 0.992/0.872 | 0.988/0.82 | 0.990/0.845 | 0.995/0.977 | 0.882/0.938 |
| RBBB | 16 | 1.0/1.0 | 0.888/0.833 | 0.941/0.909 | 1.0/1.0 | 1.0/1.0 |
| No RBBB | 843 | 0.991/0.865 | 0.992/0.883 | 0.991/0.883 | 0.996/0.978 | 0.889/0.937 |
| ST-T change | 59 | 0.941/0.941 | 0.888/0.888 | 0.914/0.914 | 0.951/0.956 | 0.921/0.972 |
| No ST-T change | 800 | 0.994/0.863 | 0.997/0.904 | 0.996/0.883 | 0.997/0.951 | 0.863/0.904 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, J.; Chen, B.; Liu, W.; Dong, W.; Zhuang, Y.; Zhang, P.; He, K. Identifying Hypertrophic or Dilated Cardiomyopathy: Development and Validation of a Fine-Tuned ResNet50 Model Based on Electrocardiogram Image. Bioengineering 2025, 12, 250. https://doi.org/10.3390/bioengineering12030250
Xu J, Chen B, Liu W, Dong W, Zhuang Y, Zhang P, He K. Identifying Hypertrophic or Dilated Cardiomyopathy: Development and Validation of a Fine-Tuned ResNet50 Model Based on Electrocardiogram Image. Bioengineering. 2025; 12(3):250. https://doi.org/10.3390/bioengineering12030250
Chicago/Turabian StyleXu, Jiayu, Bo Chen, Weiyang Liu, Wei Dong, Yan Zhuang, Peifang Zhang, and Kunlun He. 2025. "Identifying Hypertrophic or Dilated Cardiomyopathy: Development and Validation of a Fine-Tuned ResNet50 Model Based on Electrocardiogram Image" Bioengineering 12, no. 3: 250. https://doi.org/10.3390/bioengineering12030250
APA StyleXu, J., Chen, B., Liu, W., Dong, W., Zhuang, Y., Zhang, P., & He, K. (2025). Identifying Hypertrophic or Dilated Cardiomyopathy: Development and Validation of a Fine-Tuned ResNet50 Model Based on Electrocardiogram Image. Bioengineering, 12(3), 250. https://doi.org/10.3390/bioengineering12030250