

Delayed Union and Nonunion: Current Concepts, Prevention, and Correction: A Review


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
1.1. Delayed Union and Nonunion of Fractures
1.2. The Biology and Mechanics of Bone Healing
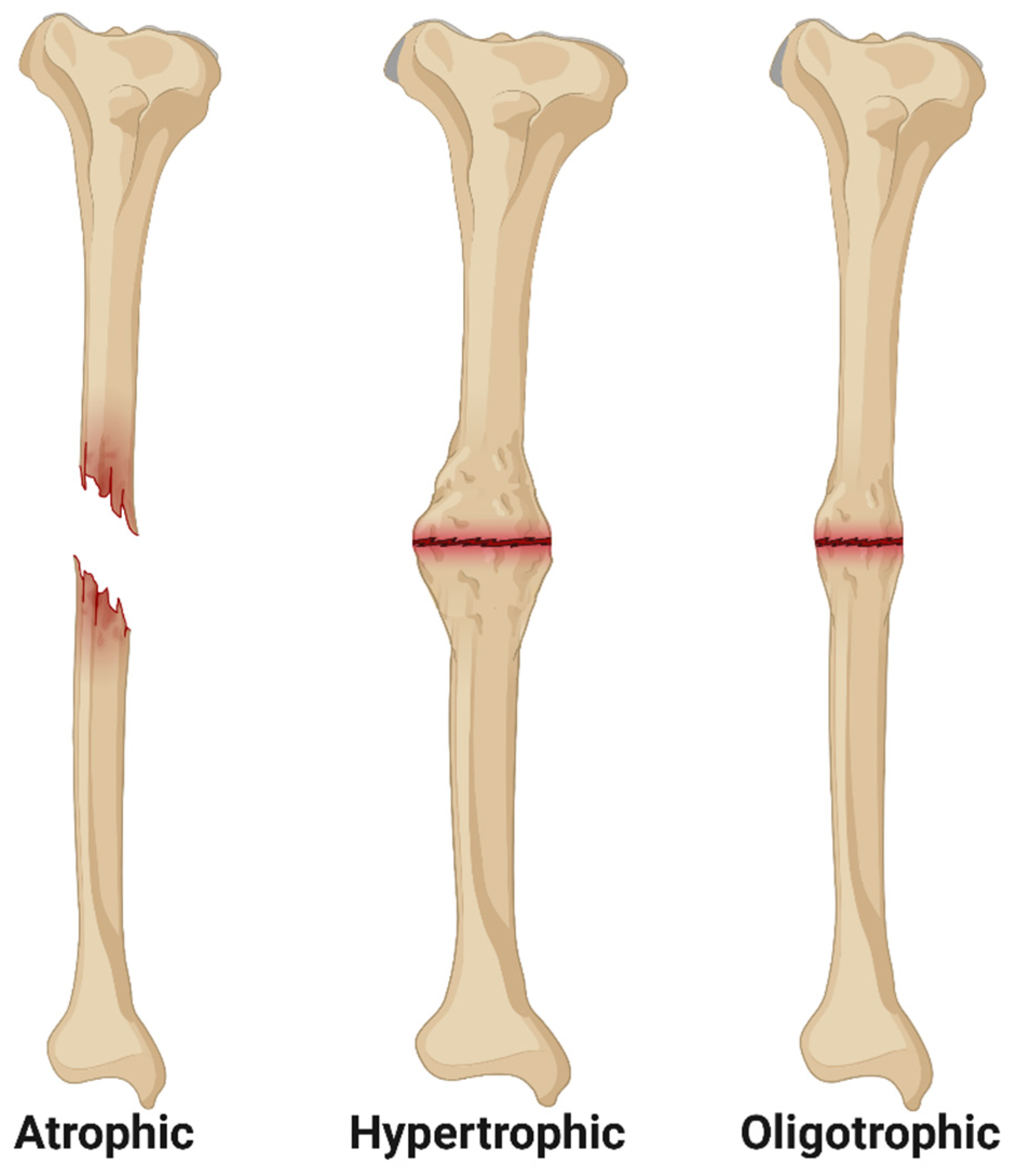
1.3. Classifications of Fracture Nonunion
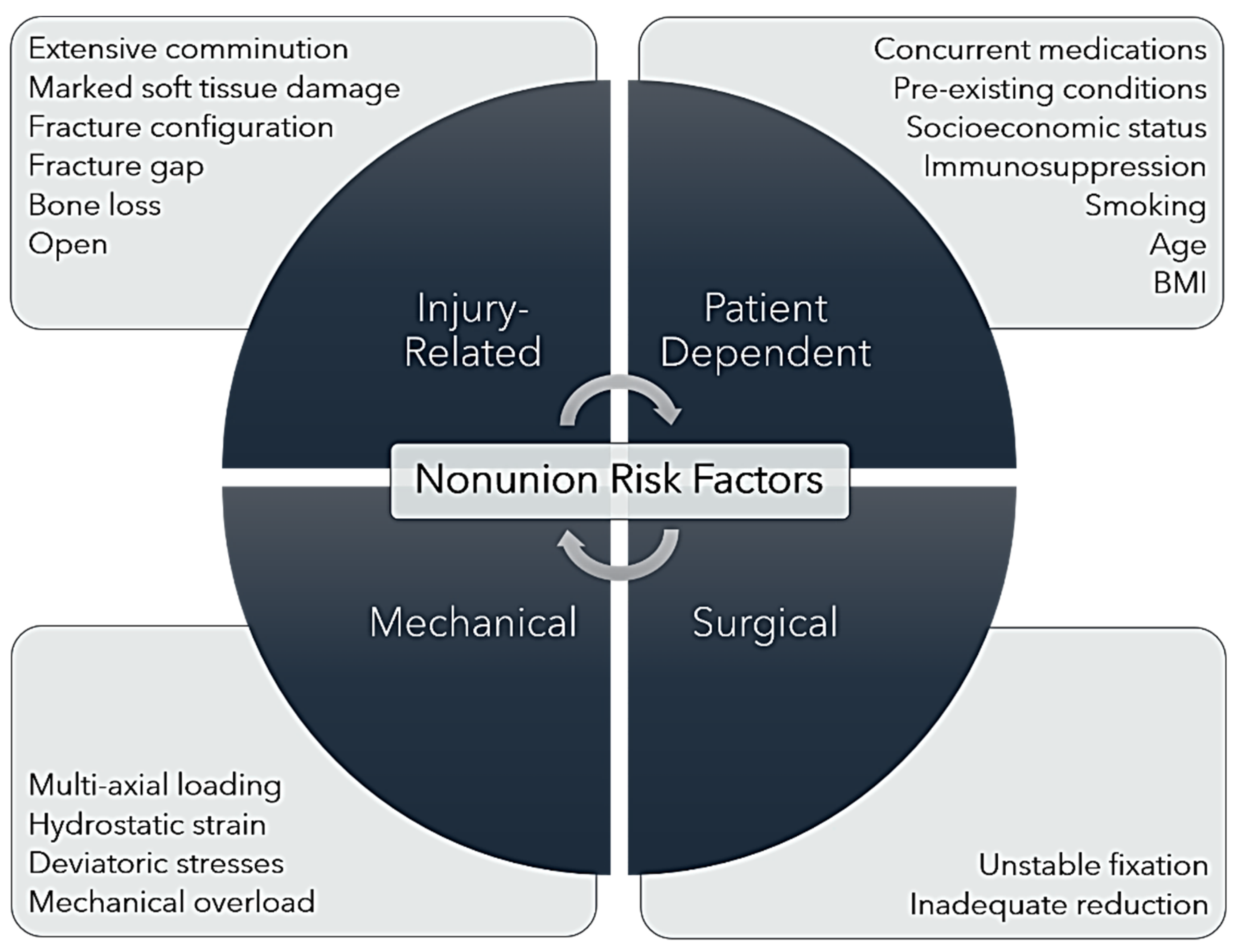
1.4. Nonunion Risk Factors
2. Preventative Techniques and Advances
2.1. Dynamization
2.2. Reverse Dynamization
2.3. Genomics, Transcriptomics, and Proteomics
3. Corrective Techniques and Advances
3.1. Exchange Nailing
3.2. Nail Dynamization
3.3. Augmentation Plating
3.4. Strain-Reduction Screws
3.5. External Fixation
3.6. Bone Grafts
3.7. Tissue Engineering
3.8. Rehabilitation of Patients Suffering Delayed Healing and Nonunion Fracture
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schlundt, C.; Bucher, C.H.; Tsitsilonis, S.; Schell, H.; Duda, G.N.; Schmidt-Bleek, K. Clinical and Research Approaches to Treat Non-union Fracture. Curr. Osteoporos. Rep. 2018, 16, 155–168. [Google Scholar] [CrossRef] [PubMed]
- Rupp, M.; Kern, S.; El Khassawna, T.; Ismat, A.; Malhan, D.; Alt, V.; Heiss, C.; Raschke, M.J. Do Systemic Factors Influence the Fate of Nonunions to Become Atrophic? A Retrospective Analysis of 162 Cases. Biomed. Res. Int. 2019, 2019, 6407098. [Google Scholar] [CrossRef] [PubMed]
- Ekegren, C.L.; Edwards, E.R.; De Steiger, R.; Gabbe, B.J. Incidence, Costs and Predictors of Non-Union, Delayed Union and Mal-Union following Long Bone Fracture. Int. J. Environ. Res. Public Health 2018, 15, 2845. [Google Scholar] [CrossRef]
- Rupp, M.; Biehl, C.; Budak, M.; Thormann, U.; Heiss, C.; Alt, V. Diaphyseal long bone nonunions—Types, aetiology, economics, and treatment recommendations. Int. Orthop. 2018, 42, 247–258. [Google Scholar] [CrossRef] [PubMed]
- Castillo, I.A.; Heiner, J.A.; Meremikwu, R.I.; Kellam, J.; Warner, S.J. Where are we in 2022? A Summary of 11,000 Open Tibia Fractures over Four Decades. J. Orthop. Trauma 2022, 17, 10–97. [Google Scholar]
- Antonova, E.; Le, T.K.; Burge, R.; Mershon, J. Tibia shaft fractures: Costly burden of nonunions. BMC Musculoskelet. Disord. 2013, 14, 42. [Google Scholar] [CrossRef]
- Dailey, H.L.; Wu, K.A.; Wu, P.S.; McQueen, M.M. Tibial Fracture Nonunion and Time to Healing after Reamed Intramedullary Nailing: Risk Factors Based on a Single-Center Review of 1003 Patients. J. Orthop. Trauma 2018, 32, e263–e269. [Google Scholar] [CrossRef] [PubMed]
- Hadjiargyrou, M.; Salichos, L.; Kloen, P. Identification of the miRNAome in human fracture callus and nonunion tissues. J. Orthop. Transl. 2023, 39, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Peng, Y.; Li, J.; Li, M.; Xiong, Y.; Xiao, J.; Zhang, L.; Tang, P. Spatial Bridge Locking Fixator versus Traditional Locking Plates in Treating AO/OTA 32-A3.2 Fracture: Finite Element Analysis and Biomechanical Evaluation. Orthop. Surg. 2022, 14, 1638–1648. [Google Scholar] [CrossRef]
- Claes, L.E.; Heigele, C.A. Magnitudes of local stress and strain along bony surfaces predict the course and type of fracture healing. J. Biomech. 1999, 32, 255–266. [Google Scholar] [CrossRef]
- Ren, T.; Dailey, H.L. Mechanoregulation modeling of bone healing in realistic fracture geometries. Biomech. Model. Mechanobiol. 2020, 19, 2307–2322. [Google Scholar] [CrossRef] [PubMed]
- Augat, P.; von Rüden, C. Evolution of fracture treatment with bone plates. Injury 2018, 49, S2–S7. [Google Scholar] [CrossRef]
- Bigham-Sadegh, A.; Oryan, A. Basic concepts regarding fracture healing and the current options and future directions in managing bone fractures. Int. Wound J. 2015, 12, 238–247. [Google Scholar] [CrossRef]
- Egol, K.A.; Kubiak, E.N.; Fulkerson, E.; Kummer, F.J.; Koval, K.J. Biomechanics of locked plates and screws. J. Orthop. Trauma 2004, 18, 488–493. [Google Scholar] [CrossRef]
- Larson, A.N.; Rizzo, M. Locking plate technology and its applications in upper extremity fracture care. Hand Clin. 2007, 23, 269–278. [Google Scholar] [CrossRef]
- Kim, S.D.; Sohn, O.J.; Kwack, B.H. The Comparison of LC-DCP versus LCP Fixation in the Plate Augmentation for the Nonunion of Femur Shaft Fractures after Intramedullary Nail Fixation. J. Korean Soc. Fract. 2008, 21, 117–123. [Google Scholar] [CrossRef]
- Hasami, N.A.; Smeeing, D.P.; Pull ter Gunne, A.F.; Edwards, M.J.; Nelen, S.D. Operative Fixation of Lateral Malleolus Fractures with Locking Plates vs Nonlocking Plates: A Systematic Review and Meta-analysis. Foot Ankle Int. 2022, 43, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Fu, P.; Liang, W.; Gao, Z.; Chen, G.; Fan, W. Optimal surgical treatment for periprosthetic distal femoral fractures after total knee arthroplasty: A Bayesian-based network analysis. J. Orthop. Surg. Res. 2023, 18, 122. [Google Scholar] [CrossRef] [PubMed]
- Neradi, D.; Sodavarapu, P.; Jindal, K.; Kumar, D.; Kumar, V.; Goni, V. Locked Plating Versus Retrograde Intramedullary Nailing for Distal Femur Fractures: A Systematic Review and Meta-Analysis. Arch. Bone Jt. Surg. 2022, 10, 141–152. [Google Scholar]
- Bliven, E.K.; Greinwald, M.; Hackl, S.; Augat, P. External fixation of the lower extremities: Biomechanical perspective and recent innovations. Injury 2019, 50 (Suppl. S1), S10–S17. [Google Scholar] [CrossRef]
- Xiong, R.; Mai, Q.G.; Yang, C.L.; Ye, S.X.; Zhang, X.; Fan, S.C. Intramedullary nailing for femoral shaft fractures in adults. Cochrane Database Syst. Rev. 2018, 2018, CD010524. [Google Scholar] [CrossRef]
- Uhthoff, H.K.; Poitras, P.; Backman, D.S. Internal plate fixation of fractures: Short history and recent developments. J. Orthop. Sci. 2006, 11, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Taljanovic, M.S.; Jones, M.D.; Ruth, J.T.; Benjamin, J.B.; Sheppard, J.E.; Hunter, T.B. Fracture fixation. Radiographics 2003, 23, 1569–1590. [Google Scholar] [CrossRef] [PubMed]
- Glatt, V.; Evans, C.H.; Tetsworth, K. A Concert between Biology and Biomechanics: The Influence of the Mechanical Environment on Bone Healing. Front. Physiol. 2017, 7, 241602. [Google Scholar] [CrossRef] [PubMed]
- Moens, N.M.M. The Biology of Locking Plate Applications. In Locking Plates in Veterinary Orthopedics; Wiley: Hoboken, NJ, USA, 2018; pp. 13–24. [Google Scholar]
- Schmierer, P.; Pozzi, A. Minimally Invasive Plate Osteosynthesis. In Locking Plates in Veterinary Orthopedics; Wiley: Hoboken, NJ, USA, 2018; pp. 41–50. [Google Scholar]
- Wang, M.T.; An, V.V.G.; Sivakumar, B.S. Non-union in lateral locked plating for distal femoral fractures: A systematic review. Injury 2019, 50, 1790–1794. [Google Scholar] [CrossRef] [PubMed]
- Bishop, J.A.; Palanca, A.A.; Bellino, M.J.; Lowenberg, D.W. Assessment of compromised fracture healing. J. Am. Acad. Orthop. Surg. 2012, 20, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Kostenuik, P.; Mirza, F.M. Fracture healing physiology and the quest for therapies for delayed healing and nonunion. J. Orthop. Res. 2017, 35, 213–223. [Google Scholar] [CrossRef] [PubMed]
- Hak, D.J.; Fitzpatrick, D.; Bishop, J.A.; Marsh, J.L.; Tilp, S.; Schnettler, R.; Simpson, H.; Alt, V. Delayed union and nonunions: Epidemiology, clinical issues, and financial aspects. Injury 2014, 45 (Suppl. S2), S3–S7. [Google Scholar] [CrossRef] [PubMed]
- Weber, B.G.; Cech, O. Pseudarthrosis: Pathophysiology, biomechanics, therapy, results. In Pseudarthrosis: Pathophysiology, Biomechanics, Therapy, Results; Grune & Stratton: New York, NY, USA, 1976; p. 323. [Google Scholar]
- Kloen, P.; Loots, G.G.; Hamdy, R.C.; Smit, T.H. Bridging the gap: Compressing non-unions for proper cellular signaling. Med. Hypotheses 2022, 160, 110794. [Google Scholar] [CrossRef]
- Bajada, S.; Marshall, M.J.; Wright, K.T.; Richardson, J.B.; Johnson, W.E. Decreased osteogenesis, increased cell senescence and elevated Dickkopf-1 secretion in human fracture non union stromal cells. Bone 2009, 45, 726–735. [Google Scholar] [CrossRef]
- Chen, H.; Ji, X.; She, F.; Gao, Y.; Tang, P. miR-628-3p regulates osteoblast differentiation by targeting RUNX2: Possible role in atrophic non-union. Int. J. Mol. Med. 2017, 39, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Liang, C.; Jacoby, J.; Reumann, M.; Braun, B.; Ehnert, S.; Nikolaou, K.; Springer, F.; Almansour, H. The Impact of Injury of the Tibial Nutrient Artery Canal on Type of Nonunion of Tibial Shaft Fractures: A Retrospective Computed Tomography Study. Acad. Radiol. 2023, 30, 2625–2635. [Google Scholar] [CrossRef] [PubMed]
- Al Farii, H.; Farahdel, L.; Frazer, A.; Salimi, A.; Bernstein, M. The effect of NSAIDs on postfracture bone healing: A meta-analysis of randomized controlled trials. OTA Int. 2021, 4, e092. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, A.; Kumar, N.; Gupta, B. Delayed Tibial Shaft Fracture Healing Associated with Smoking: A Systematic Review and Meta-Analysis of Observational Studies Conducted Worldwide. Int. J. Environ. Res. Public Health 2021, 18, 10228. [Google Scholar] [CrossRef] [PubMed]
- Mundi, R.; Axelrod, D.; Chaudhry, H.; Sahota, N.; Heels-Ansdell, D.; Sprague, S.; Petrisor, B.; Schemitsch, E.; Busse, J.W.; Thabane, L.; et al. Association of Three-Month Radiographic Union Score for Tibia Fractures (RUST) with Nonunion in Tibial Shaft Fracture Patients. Cureus 2020, 12, e8314. [Google Scholar] [CrossRef]
- Rodriguez, E.K.; Boulton, C.; Weaver, M.J.; Herder, L.M.; Morgan, J.H.; Chacko, A.T.; Appleton, P.T.; Zurakowski, D.; Vrahas, M.S. Predictive factors of distal femoral fracture nonunion after lateral locked plating: A retrospective multicenter case-control study of 283 fractures. Injury 2014, 45, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Arpey, N.C.; Gaglioti, A.H.; Rosenbaum, M.E. How socioeconomic status affects patient perceptions of health care: A qualitative study. J. Prim. Care Community Health 2017, 8, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Kangovi, S.; Barg, F.K.; Carter, T.; Long, J.A.; Shannon, R.; Grande, D. Understanding why patients of low socioeconomic status prefer hospitals over ambulatory care. Health Aff. 2013, 32, 1196–1203. [Google Scholar] [CrossRef] [PubMed]
- Kangovi, S.; Barg, F.K.; Carter, T.; Long, J.A.; Shannon, R.; Grande, D. Challenges Faced by Patients with Low Socioeconomic Status During the Post-Hospital Transition. J. Gen. Intern. Med. 2014, 29, 283–289. [Google Scholar] [CrossRef]
- Tsang, S.T.; Mills, L.A.; Frantzias, J.; Baren, J.P.; Keating, J.F.; Simpson, A.H. Exchange nailing for nonunion of diaphyseal fractures of the tibia: Our results and an analysis of the risk factors for failure. Bone Jt. J. 2016, 98-B, 534–541. [Google Scholar] [CrossRef]
- Struijs, P.A.; Poolman, R.W.; Bhandari, M. Infected nonunion of the long bones. J. Orthop. Trauma 2007, 21, 507–511. [Google Scholar] [CrossRef] [PubMed]
- Harvin, W.H.; Oladeji, L.O.; Della Rocca, G.J.; Murtha, Y.M.; Volgas, D.A.; Stannard, J.P.; Crist, B.D. Working length and proximal screw constructs in plate osteosynthesis of distal femur fractures. Injury 2017, 48, 2597–2601. [Google Scholar] [CrossRef] [PubMed]
- Meinberg, E.G.; Agel, J.; Roberts, C.S.; Karam, M.D.; Kellam, J.F. Fracture and Dislocation Classification Compendium-2018. J. Orthop. Trauma 2018, 32 (Suppl. S1), S1–S170. [Google Scholar] [CrossRef]
- Kawasaki, N.; Takegami, Y.; Sakai, R.; Todoroki, K.; Uemi, R.; Imagama, S. Prediction of delayed union of tibial shaft fracture treated with intramedullary nailing: Multicenter-study analysis and literature review—The TRON study. Eur. J. Orthop. Surg. Traumatol. 2022, 32, 129–135. [Google Scholar] [CrossRef]
- Nakagawa, T.; Inui, T.; Matsui, K.; Ishii, K.; Suzuki, T.; Kurozumi, T.; Kawano, H.; Watanabe, Y. Effect of postoperative fracture gap on bone union: A retrospective cohort analysis of simple femoral shaft fractures. J. Orthop. Sci. 2023, 29, 632–636. [Google Scholar] [CrossRef]
- McMillan, T.E.; Johnstone, A.J. Technical considerations to avoid delayed and non-union. Injury 2017, 48 (Suppl. S1), S64–S68. [Google Scholar] [CrossRef]
- Reichert, J.C.; Saifzadeh, S.; Wullschleger, M.E.; Epari, D.R.; Schütz, M.A.; Duda, G.N.; Schell, H.; van Griensven, M.; Redl, H.; Hutmacher, D.W. The challenge of establishing preclinical models for segmental bone defect research. Biomaterials 2009, 30, 2149–2163. [Google Scholar] [CrossRef] [PubMed]
- Schemitsch, E.H. Size matters: Defining critical in bone defect size! J. Orthop. Trauma 2017, 31, S20–S22. [Google Scholar] [CrossRef]
- Huang, E.E.; Zhang, N.; Shen, H.; Li, X.; Maruyama, M.; Utsunomiya, T.; Gao, Q.; Guzman, R.A.; Goodman, S.B. Novel techniques and future perspective for investigating critical-size bone defects. Bioengineering 2022, 9, 171. [Google Scholar] [CrossRef]
- Murphy, D.; Raza, M.; Monsell, F.; Gelfer, Y. Modern management of paediatric tibial shaft fractures: An evidence-based update. Eur. J. Orthop. Surg. Traumatol. 2021, 31, 901–909. [Google Scholar] [CrossRef]
- Maresca, A.; Sangiovanni, P.; Cerbasi, S.; Politano, R.; Fantasia, R.; Commessatti, M.; Pascarella, R. Why a surgically treated humeral shaft fracture became a nonunion: Review of 11 years in two trauma centers. Musculoskelet. Surg. 2017, 101 (Suppl. S2), 105–112. [Google Scholar] [CrossRef] [PubMed]
- Orth, M.; Ganse, B.; Andres, A.; Wickert, K.; Warmerdam, E.; Müller, M.; Diebels, S.; Roland, M.; Pohlemann, T. Simulation-based prediction of bone healing and treatment recommendations for lower leg fractures: Effects of motion, weight-bearing and fibular mechanics. Front. Bioeng. Biotechnol. 2023, 11, 1067845. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Carrera, R.; Flamini, V.; Kenny, L.; Cabahug-Zuckerman, P.; George, B.M.; Hunter, D.; Liu, B.; Singh, G.; Leucht, P.; et al. Effects of mechanical loading on cortical defect repair using a novel mechanobiological model of bone healing. Bone 2018, 108, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Giordano, V.; Santos, A.L.; Belangero, W.D.; Pires, R.E.; Labronici, P.J.; Koch, H.A. Mind the gap between the fracture line and the length of the working area: A 2-D finite element analysis using an extramedullary fixation model. Rev. Bras. Ortop. 2018, 53, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Jamshidi, K.; Bahardoust, M.; Karimi Behnagh, A.; Bagherifard, A.; Mirzaei, A. How the Choice of Osteosynthesis Affects the Complication Rate of Intercalary Allograft Reconstruction? A Systematic Review and Meta-analysis. Indian J. Orthop. 2021, 56, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Schultz, B.J.; Amin, N.H.; Mattison, B.J.; Mir, H.R.; Shah, A.R.; Cerynik, D.L. Locking Screws with a Threaded Degradable Polymer Collar Reduce Construct Stiffness Over Time. J. Orthop. Trauma 2020, 34, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, E.C.; Judkins, L.M.; Monogharan, G.; Mehta, S.; Hast, M.W. Current concepts in fracture healing: Temporal dynamization and applications for additive manufacturing. OTA Int. 2022, 5 (Suppl. S1), e164. [Google Scholar] [CrossRef] [PubMed]
- Henschel, J.; Tsai, S.; Fitzpatrick, D.C.; Marsh, J.L.; Madey, S.M.; Bottlang, M. Comparison of 4 Methods for Dynamization of Locking Plates: Differences in the Amount and Type of Fracture Motion. J. Orthop. Trauma 2017, 31, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, E.K.; Zurakowski, D.; Herder, L.; Hall, A.; Walley, K.C.; Weaver, M.J.; Appleton, P.T.; Vrahas, M. Mechanical Construct Characteristics Predisposing to Non-union after Locked Lateral Plating of Distal Femur Fractures. J. Orthop. Trauma 2016, 30, 403–408. [Google Scholar] [CrossRef]
- Bottlang, M.; Doornink, J.; Lujan, T.J.; Fitzpatrick, D.C.; Marsh, J.L.; Augat, P.; von Rechenberg, B.; Lesser, M.; Madey, S.M. Effects of Construct Stiffness on Healing of Fractures Stabilized with Locking Plates. J. Bone Jt. Surg. 2010, 92 (Suppl. S2), 12–22. [Google Scholar] [CrossRef]
- Heyland, M.; Duda, G.N.; Haas, N.P.; Trepczynski, A.; Döbele, S.; Höntzsch, D.; Schaser, K.D.; Märdian, S. Semi-rigid screws provide an auxiliary option to plate working length to control interfragmentary movement in locking plate fixation at the distal femur. Injury 2015, 46 (Suppl. 4), S24–S32. [Google Scholar] [CrossRef]
- Bottlang, M.; Feist, F. Biomechanics of Far Cortical Locking. J. Orthop. Trauma 2011, 25 (Suppl. S1), S21–S28. [Google Scholar] [CrossRef] [PubMed]
- Beltran, M.J.; Collinge, C.A.; Gardner, M.J. Stress Modulation of Fracture Fixation Implants. J. Am. Acad. Orthop. Surg. 2016, 24, 711–719. [Google Scholar] [CrossRef]
- Bottlang, M.; Tsai, S.; Bliven, E.K.; von Rechenberg, B.; Kindt, P.; Augat, P.; Henschel, J.; Fitzpatrick, D.C.; Madey, S.M. Dynamic Stabilization of Simple Fractures with Active Plates Delivers Stronger Healing Than Conventional Compression Plating. J. Orthop. Trauma 2017, 31, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.B.; Yoo, J.S.; Kim, Y.J.; Kim, K.B. Assessment of the efficacy of the far cortical locking technique in proximal humeral fractures: A comparison with the conventional bi-cortical locking technique. BMC Musculoskelet. Disord. 2020, 21, 800. [Google Scholar] [CrossRef]
- Willie, B.M.; Blakytny, R.; Glöckelmann, M.; Ignatius, A.; Claes, L. Temporal variation in fixation stiffness affects healing by differential cartilage formation in a rat osteotomy model. Clin. Orthop. Relat. Res. 2011, 469, 3094–3101. [Google Scholar] [CrossRef]
- Yang, K.-H.; Lee, C.-H.; Park, Y.-C. Effect of Interlocking Mode on the Outcomes of Exchange Nailing for the Treatment of Aseptic Femoral Shaft Nonunion. Clin. Orthop. Surg. 2023, 15, 13. [Google Scholar] [CrossRef]
- Durall, I.; Falcón, C.; Díaz-Bertrana, M.C.; Franch, J. Effects of Static Fixation and Dynamization after Interlocking Femoral Nailing Locked with an External Fixator: An Experimental Study in Dogs. Vet. Surg. 2004, 33, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Claes, L.; Blakytny, R.; Göckelmann, M.; Schoen, M.; Ignatius, A.; Willie, B. Early dynamization by reduced fixation stiffness does not improve fracture healing in a rat femoral osteotomy model. J. Orthop. Res. 2009, 27, 22–27. [Google Scholar] [CrossRef]
- Iobst, C.A.; Milne, E.; Khoury, A.; Ingwer, Z.; Latta, L. A novel way to dynamize a spatial frame and optimize fracture healing. Injury 2021, 52, 106–108. [Google Scholar] [CrossRef]
- Faria, F.F.; Gruhl, C.E.; Ferro, R.R.; Rached, R.N.; Soni, J.F.; Trevilatto, P. Finite Element Analysis of a Controlled Dynamization Device for External Circular Fixation. Rev. Bras. Ortop. 2021, 56, 36–41. [Google Scholar]
- Hutchinson, D.J.; Granskog, V.; von Kieseritzky, J.; Alfort, H.; Stenlund, P.; Zhang, Y.; Arner, M.; Håkansson, J.; Malkoch, M. Highly Customizable Bone Fracture Fixation through the Marriage of Composites and Screws. Adv. Funct. Mater. 2021, 31, 2105187. [Google Scholar] [CrossRef]
- Frank, A.; Brianza, S.; Plecko, M.; Raschke, M.J.; Wähnert, D. Variable Fixation Technology Provides Rigid as Well as Progressive Dynamic Fixation: A Biomechanical Investigation. J. Bone Jt. Surg. Am. 2020, 102, e115. [Google Scholar] [CrossRef] [PubMed]
- Plecko, M.; Klein, K.; Planzer, K.; Wähnert, D.; Behm, P.; Ferguson, S.J.; Brianza, S.; Stadelmann, V.A.; von Rechenberg, B. Variable fixation promotes callus formation: An experimental study on transverse tibial osteotomies stabilized with locking plates. BMC Musculoskelet. Disord. 2020, 21, 806. [Google Scholar] [CrossRef] [PubMed]
- Schultz, B.J.; Koval, K.; Salehi, P.P.; Gardner, M.J.; Cerynik, D.L. Controversies in Fracture Healing: Early Versus Late Dynamization. Orthopedics 2020, 43, e125–e133. [Google Scholar] [CrossRef]
- Fu, R.; Feng, Y.; Liu, Y.; Willie, B.M.; Yang, H. The combined effects of dynamization time and degree on bone healing. J. Orthop. Res. 2022, 40, 634–643. [Google Scholar] [CrossRef] [PubMed]
- Glatt, V.; Bartnikowski, N.; Quirk, N.; Schuetz, M.; Evans, C. Reverse dynamization: Influence of fixator stiffness on the mode and efficiency of large-bone-defect healing at different doses of rhBMP-2. J. Bone Jt. Surg. 2016, 98, 677–687. [Google Scholar] [CrossRef] [PubMed]
- Glatt, V.; Miller, M.; Ivkovic, A.; Liu, F.; Parry, N.; Griffin, D.; Vrahas, M.; Evans, C. Improved Healing of Large Segmental Defects in the Rat Femur by Reverse Dynamization in the Presence of Bone Morphogenetic Protein-2. J. Bone Jt. Surg. 2012, 94, 2063–2073. [Google Scholar] [CrossRef]
- Glatt, V.; Samchukov, M.; Cherkashin, A.; Iobst, C. Reverse Dynamization Accelerates Bone-Healing in a Large-Animal Osteotomy Model. J. Bone Jt. Surg. 2021, 103, 257–263. [Google Scholar] [CrossRef]
- Evans, C.H. Improved Healing of Large, Osseous, Segmental Defects by Reverse Dynamization: Evaluation in a Sheep Model. 2015. [Google Scholar] [CrossRef]
- Glatt, V.; Tepic, S.; Evans, C. Reverse dynamization: A novel approach to bone healing. JAAOS-J. Am. Acad. Orthop. Surg. 2016, 24, e60–e61. [Google Scholar] [CrossRef]
- Tsiridis, E.; Giannoudis, P.V. Transcriptomics and proteomics: Advancing the understanding of genetic basis of fracture healing. Injury 2006, 37, S13–S19. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.M.; Clifton, K.B.; Lorenzo, J.; Hansen, M.F.; Drissi, H. Comparative transcriptomic analysis identifies distinct molecular signatures and regulatory networks of chondroclasts and osteoclasts. Arthritis Res. Ther. 2020, 22, 168. [Google Scholar] [CrossRef] [PubMed]
- Avin, K.G.; Dominguez, J.M., 2nd; Chen, N.X.; Hato, T.; Myslinski, J.J.; Gao, H.; Liu, Y.; McKinley, T.O.; Brown, K.M.; Moe, S.M.; et al. Single-cell RNAseq provides insight into altered immune cell populations in human fracture nonunions. J. Orthop. Res. 2022, 41, 1060–1069. [Google Scholar] [CrossRef] [PubMed]
- Hadjiargyrou, M.; Lombardo, F.; Zhao, S.; Ahrens, W.; Joo, J.; Ahn, H.; Jurman, M.; White, D.W.; Rubin, C.T. Transcriptional Profiling of Bone Regeneration: Insight into the molecular complexity of wound repair* 210. J. Biol. Chem. 2002, 277, 30177–30182. [Google Scholar] [CrossRef] [PubMed]
- Bow, A.J.; Rifkin, R.E.; Priester, C.; Christopher, C.J.; Grzeskowiak, R.M.; Hecht, S.; Adair, S.H.; Mulon, P.Y.; Castro, H.F.; Campagna, S.R.; et al. Temporal metabolic profiling of bone healing in a caprine tibia segmental defect model. Front. Vet. Sci. 2023, 9, 1023650. [Google Scholar] [CrossRef] [PubMed]
- Zheng, N.; Xu, J.; Ruan, Y.C.; Chang, L.; Wang, X.; Yao, H.; Wang, J.; Zhang, R.; Xue, Q.; Tang, N.; et al. Magnesium facilitates the healing of atypical femoral fractures: A single-cell transcriptomic study. Mater. Today 2022, 52, 43–62. [Google Scholar] [CrossRef]
- Liu, C.; Liu, Y.; Yu, Y.; Zhao, Y.; Zhang, D.; Yu, A. Identification of Up-Regulated ANXA3 Resulting in Fracture Non-Union in Patients with T2DM. Front. Endocrinol. 2022, 13, 890941. [Google Scholar] [CrossRef] [PubMed]
- Naeem-ur-Razaq, M.; Qasim, M.; Sultan, S. Exchange nailing for non-union of femoral shaft fractures. J. Ayub Med. Coll. Abbottabad 2010, 22, 106–109. [Google Scholar] [PubMed]
- Bhan, K.; Tyagi, A.; Kainth, T.; Gupta, A.; Umar, M. Reamed Exchange Nailing in Nonunion of Tibial Shaft Fractures: A Review of the Current Evidence. Cureus 2020, 7, e9267. [Google Scholar] [CrossRef]
- Minhas, A.; Berkay, F.; Ehlers, C.B.; Froehle, A.W.; Krishnamurthy, A.B. The statistical fragility of intramedullary reaming in tibial nail fixation: A systematic review. Eur. J. Trauma Emerg. Surg. 2023, 49, 2347–2354. [Google Scholar] [CrossRef]
- Pfeifer, R.; Sellei, R.; Pape, H.C. The biology of intramedullary reaming. Injury 2010, 41 (Suppl. S2), S4–S8. [Google Scholar] [CrossRef] [PubMed]
- Kostic, I.; Mitkovic, M.; Mitkovic, M. The diaphyseal aseptic tibial nonunions after failed previous treatment options managed with the reamed intramedullary locking nail. J. Clin. Orthop. Trauma 2019, 10, 182–190. [Google Scholar] [CrossRef]
- Schemitsch, E.H.; Turchin, D.C.; Anderson, G.I.; Byrick, R.J.; Mullen, J.B.; Richards, R.R. Pulmonary and systemic fat embolization after medullary canal pressurization: A hemodynamic and histologic investigation in the dog. J. Trauma 1998, 45, 738–742. [Google Scholar] [CrossRef]
- Zhang, H.A.; Zhou, C.H.; Meng, X.Q.; Fang, J.; Qin, C.H. Intramedullary reaming and irrigation and antibiotic-loaded calcium sulfate implantation for the treatment of infection after intramedullary nailing: A retrospective study of 19 cases. BMC Musculoskelet. Disord. 2020, 21, 710. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-C. Aseptic femoral nonunion treated with exchange locked nailing with intramedullary augmentation cancellous bone graft. J. Orthop. Surg. Res. 2022, 17, 339. [Google Scholar] [CrossRef]
- Perumal, R.; Shankar, V.; Basha, R.; Jayaramaraju, D.; Rajasekaran, S. Is nail dynamization beneficial after twelve weeks—An analysis of 37 cases. J. Clin. Orthop. Trauma 2018, 9, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Vaughn, J.; Gotha, H.; Cohen, E.; Fantry, A.J.; Feller, R.J.; Van Meter, J.; Hayda, R.; Born, C.T. Nail Dynamization for Delayed Union and Nonunion in Femur and Tibia Fractures. Orthopedics 2016, 39, e1117–e1123. [Google Scholar] [CrossRef] [PubMed]
- Vaughn, J.E.; Shah, R.V.; Samman, T.; Stirton, J.; Liu, J.; Ebraheim, N.A. Systematic review of dynamization vs exchange nailing for delayed/non-union femoral fractures. World J. Orthop. 2018, 9, 92–99. [Google Scholar] [CrossRef]
- Stolberg-Stolberg, J.; Fuchs, T.; Lodde, M.F.; Roßlenbroich, S.; Garcia, P.; Raschke, M.; Everding, J. Addition of shock wave therapy to nail dynamization increases the chance of long-bone non-union healing. J. Orthop. Traumatol. 2022, 23, 4. [Google Scholar] [CrossRef]
- Mohammad, D.; Sajjad, M.; Jatoi, F.; Khoso, R. Effects of Dynamization on Delayed Union of Tibial Shaft Fractures after Reamed Intramedullary Interlocked Nailing. Ann. Jinnah Sindh Med. Univ. 2022, 8, 59–63. [Google Scholar]
- Zhang, W.; Zhang, Z.; Li, J.; Zhang, L.; Chen, H.; Tang, P. Clinical outcomes of femoral shaft non-union: Dual plating versus exchange nailing with augmentation plating. J. Orthop. Surg. Res. 2018, 13, 295. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, M.A.; Noaman, H.H.; Soroor, Y.O.; Elsayed, M. Plate augmentation and bone grafting in treatment of femoral shaft nonunion initially fixed by intramedullary nail. SICOT-J 2022, 8, 19. [Google Scholar] [CrossRef] [PubMed]
- Uliana, C.S.; Bidolegui, F.; Kojima, K. Giordano VAugmentation plating leaving the nail in situ is an excellent option for treating femoral shaft nonunion after IM nailing: A multicentre study. Eur. J. Trauma Emerg. Surg. 2021, 47, 1895–1901. [Google Scholar] [CrossRef] [PubMed]
- Perisano, C.; Cianni, L.; Polichetti, C.; Cannella, A.; Mosca, M.; Caravelli, S.; Maccauro, G.; Greco, T. Plate Augmentation in Aseptic Femoral Shaft Nonunion after Intramedullary Nailing: A Literature Review. Bioengineering 2022, 9, 560. [Google Scholar] [CrossRef] [PubMed]
- Jhunjhunwala, H.R.; Dhawale, A.A. Is augmentation plating an effective treatment for non-union of femoral shaft fractures with nail in situ? Eur. J. Trauma Emerg. Surg. 2016, 42, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Siavashi, B.; Soleimani, M.; Golbakhsh, M.; Rastegar, M.; Shafiei, S.H. The Effect of Augmentative Plating for the Treatment of Nonunion of Femoral Shaft Fractures after Intramedullary Nailing: A Case Series. J. Orthop. Spine Trauma 2022, 8, 57–59. [Google Scholar] [CrossRef]
- Bellringer, S.F.; Jukes, C.; Dirckx, M.; Guryel, E.; Phadnis, J. Strain reduction screws for nonunions following fixation around the elbow—A case series and review of the literature. J. Clin. Orthop. Trauma 2023, 38, 102129. [Google Scholar] [CrossRef] [PubMed]
- Bence, M.; Kothari, A.; Riddick, A.; Eardley, W.; Handley, R.; Trompeter, A. Percutaneous Strain Reduction Screws Are a Reproducible Minimally Invasive Method to Treat Long Bone Nonunion. J. Orthop. Trauma 2022, 36, e343–e348. [Google Scholar] [CrossRef] [PubMed]
- Kothari, A.; Monk, P.; Handley, R. Percutaneous Strain Reduction Screws-A Safe and Simple Surgical Option for Problems with Bony Union. A Technical Trick. J. Orthop. Trauma 2019, 33, e151–e157. [Google Scholar] [CrossRef]
- Simpson, A.H.; Robiati, L.; Jalal, M.M.; Tsang, S.T. Non-union: Indications for external fixation. Injury 2019, 50 (Suppl. S1), S73–S78. [Google Scholar] [CrossRef]
- Yin, P.; Zhang, Q.; Mao, Z.; Li, T.; Zhang, L.; Tang, P. The treatment of infected tibial nonunion by bone transport using the Ilizarov external fixator and a systematic review of infected tibial nonunion treated by Ilizarov methods. Acta Orthop. Belg. 2014, 80, 426–435. [Google Scholar] [PubMed]
- Giannoudis, P.V.; Faour, O.; Goff, T.; Kanakaris, N.; Dimitriou, R. Masquelet technique for the treatment of bone defects: Tips-tricks and future directions. Injury 2011, 42, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Li, M.; Wang, W.; Li, B.; Liu, L. Evolution and Development of Ilizarov Technique in the Treatment of Infected Long Bone Nonunion with or without Bone Defects. Orthop. Surg. 2022, 14, 824–830. [Google Scholar] [CrossRef] [PubMed]
- Borzunov, D.Y.; Kolchin, S.N. Nonunion of the femoral shaft associated with limb shortening treated with a combined technique of external fixation over an intramedullary nail versus the Ilizarov method. Arch. Orthop. Trauma Surg. 2022, 142, 2185–2192. [Google Scholar] [CrossRef] [PubMed]
- Borzunov, D.Y.; Kolchin, S.N.; Malkova, T.A. Role of the Ilizarov non-free bone plasty in the management of long bone defects and nonunion: Problems solved and unsolved. World J. Orthop. 2020, 11, 304–318. [Google Scholar] [CrossRef] [PubMed]
- Roberts, T.T.; Rosenbaum, A.J. Bone grafts, bone substitutes and orthobiologics. Organogenesis 2012, 8, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Visser, N.; Rezaie, E.; Ducharme, A.; Shin, A.Y.; Bishop, A.T. The effect of surgical revascularization on the mechanical properties of cryopreserved bone allograft in a porcine tibia model. J. Orthop. Res. 2023, 41, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Winocour, S.J.; Schultz, K.P.; Davis, M.J.; Abu-Ghname, A.; Bohl, M.; Ropper, A.E.; Maricevich, M.; Reece, E.M. Vascularized Posterior Iliac Crest Bone Grafting: Indications, Techniques, Clinical Outcomes, and Alternatives. In Seminars in Plastic Surgery; Thieme Medical Publishers, Inc.: New York, NY, USA, 2021. [Google Scholar]
- Zhang, H.; Gu, J.; Liu, H.; Yuan, C. Pedicled vascularized versus non-vascularized bone grafts in the treatment of scaphoid non-union: A meta-analysis of comparative studies. ANZ J. Surg. 2021, 91, E682–E689. [Google Scholar] [CrossRef] [PubMed]
- Tsantes, A.G.; Papadopoulos, D.V.; Gelalis, I.D.; Vekris, M.D.; Pakos, E.E.; Korompilias, A.V. The Efficacy of Vascularized Bone Grafts in the Treatment of Scaphoid Nonunions and Kienbock Disease: A Systematic Review in 917 Patients. J. Hand Microsurg. 2019, 11, 6–13. [Google Scholar] [CrossRef]
- Testa, G.; Lucenti, L.; D’Amato, S.; Sorrentino, M.; Cosentino, P.; Vescio, A.; Pavone, V. Comparison between Vascular and Non-Vascular Bone Grafting in Scaphoid Nonunion: A Systematic Review. J. Clin. Med. 2022, 11, 3402. [Google Scholar] [CrossRef]
- Simpson, C.R.; Kelly, H.M.; Murphy, C.M. Synergistic use of biomaterials and licensed therapeutics to manipulate bone remodelling and promote non-union fracture repair. Adv. Drug Deliv. Rev. 2020, 160, 212–233. [Google Scholar] [CrossRef] [PubMed]
- Tang, G.; Liu, Z.; Liu, Y.; Yu, J.; Wang, X.; Tan, Z.; Ye, X. Recent Trends in the Development of Bone Regenerative Biomaterials. Front. Cell Dev. Biol. 2021, 9, 665813. [Google Scholar] [CrossRef]
- Sales, A.; Khodr, V.; Machillot, P.; Chaar, L.; Fourel, L.; Guevara-Garcia, A.; Migliorini, E.; Albigès-Rizo, C.; Picart, C. Differential bioactivity of four BMP-family members as function of biomaterial stiffness. Biomaterials 2022, 281, 121363. [Google Scholar] [CrossRef]
- Xie, Z.; Yan, D.; Zhou, Q.; Wu, Z.; Weng, S.; Boodhun, V.; Bai, B.; Shen, Z.; Tang, J.; Chen, L.; et al. The fast degradation of β-TCP ceramics facilitates healing of bone defects by the combination of BMP-2 and Teriparatide. Biomed. Pharmacother. 2019, 112, 108578. [Google Scholar] [CrossRef] [PubMed]
- Zhu, G.; Zhang, T.; Chen, M.; Yao, K.; Huang, X.; Zhang, B.; Li, Y.; Liu, J.; Wang, Y.; Zhao, Z. Bone physiological microenvironment and healing mechanism: Basis for future bone-tissue engineering scaffolds. Bioact. Mater. 2021, 6, 4110–4140. [Google Scholar] [CrossRef]
- Gariffo, G.; Bottai, V.; Falcinelli, F.; Di Sacco, F.; Cifali, R.; Troiano, E.; Capanna, R.; Mondanelli, N.; Giannotti, S. Use of Teriparatide in preventing delayed bone healing and nonunion: A multicentric study on a series of 20 patients. BMC Musculoskelet. Disord. 2023, 24, 184. [Google Scholar] [CrossRef]
- Thurairajah, K.; Briggs, G.D.; Balogh, Z.J. Stem cell therapy for fracture non-union: The current evidence from human studies. J. Orthop. Surg. 2021, 29, 23094990211036545. [Google Scholar] [CrossRef]
- El-Jawhari, J.J.; Kleftouris, G.; El-Sherbiny, Y.; Saleeb, H.; West, R.M.; Jones, E.; Giannoudis, P.V. Defective Proliferation and Osteogenic Potential with Altered Immunoregulatory phenotype of Native Bone marrow-Multipotential Stromal Cells in Atrophic Fracture Non-Union. Sci. Rep. 2019, 9, 17340. [Google Scholar] [CrossRef] [PubMed]
- Khatkar, H.; See, A. Stem Cell Therapy in the Management of Fracture Non-Union—Evaluating Cellular Mechanisms and Clinical Progress. Cureus 2021, 13. [Google Scholar] [CrossRef]
- Gómez-Barrena, E.; Padilla-Eguiluz, N.; Rosset, P.; Gebhard, F.; Hernigou, P.; Baldini, N.; Rouard, H.; Sensebé, L.; Gonzalo-Daganzo, R.M.; Giordano, R.; et al. Early efficacy evaluation of mesenchymal stromal cells (MSC) combined to biomaterials to treat long bone non-unions. Injury 2020, 51, S63–S73. [Google Scholar] [CrossRef]
- Wittig, O.; Romano, E.; González, C.; Diaz-Solano, D.; Marquez, M.E.; Tovar, P.; Aoun, R.; Cardier, J.E. A method of treatment for nonunion after fractures using mesenchymal stromal cells loaded on collagen microspheres and incorporated into platelet-rich plasma clots. Int. Orthop. 2016, 40, 1033–1038. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Jiao, G.; Ren, S.; Zhang, X.; Li, C.; Wu, W.; Wang, H.; Liu, H.; Zhou, H.; Chen, Y. Exosomes from bone marrow mesenchymal stem cells enhance fracture healing through the promotion of osteogenesis and angiogenesis in a rat model of nonunion. Stem Cell Res. Ther. 2020, 11, 38. [Google Scholar] [CrossRef] [PubMed]
- Colasanti, C.A.; Anil, U.; Rodriguez, K.; Levin, J.M.; Leucht, P.; Simovitch, R.W.; Zuckerman, J.D. Optimal combination of arthroplasty type, fixation method and postoperative rehabilitation protocol for complex proximal humerus fractures in the elderly: A network meta-analysis. J. Shoulder Elb. Surg. 2024, in press. [CrossRef] [PubMed]
- Chen, B.; Ye, Z.; Wu, J.; Wang, G.; Yu, T. The effect of early weight-bearing and later weight-bearing rehabilitation interventions on outcomes after ankle fracture surgery: A systematic review and meta-analysis of randomised controlled trials. J. Foot Ankle Res. 2024, 17, e12011. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsen, C.; Nørgaard, B. Elderly patients’ perspectives on treatment, care and rehabilitation after hip fracture: A qualitative systematic review. Int. J. Orthop. Trauma Nurs. 2021, 41, 100811. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, S.H. Effectiveness of multicomponent home-based rehabilitation in older patients after hip fracture surgery: A systematic review and meta-analysis. J. Clin. Nurs. 2023, 32, 31–48. [Google Scholar] [CrossRef] [PubMed]
- Pinto, D.; Alshahrani, M.; Chapurlat, R.; Chevalley, T.; Dennison, E.; Camargos, B.M.; Papaioannou, A.; Silverman, S.; Kaux, J.F.; Lane, N.E.; et al. The global approach to rehabilitation following an osteoporotic fragility fracture: A review of the rehabilitation working group of the International Osteoporosis Foundation (IOF) committee of scientific advisors. Osteoporos Int. 2022, 33, 527–540. [Google Scholar] [CrossRef] [PubMed]
- Blackburn, J.; Yeowell, G. Patients’ perceptions of rehabilitation in the community following hip fracture surgery. A qualitative thematic synthesis. Physiotherapy 2020, 108, 63–75. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bowers, K.M.; Anderson, D.E. Delayed Union and Nonunion: Current Concepts, Prevention, and Correction: A Review. Bioengineering 2024, 11, 525. https://doi.org/10.3390/bioengineering11060525
Bowers KM, Anderson DE. Delayed Union and Nonunion: Current Concepts, Prevention, and Correction: A Review. Bioengineering. 2024; 11(6):525. https://doi.org/10.3390/bioengineering11060525
Chicago/Turabian StyleBowers, Kristin M., and David E. Anderson. 2024. "Delayed Union and Nonunion: Current Concepts, Prevention, and Correction: A Review" Bioengineering 11, no. 6: 525. https://doi.org/10.3390/bioengineering11060525
APA StyleBowers, K. M., & Anderson, D. E. (2024). Delayed Union and Nonunion: Current Concepts, Prevention, and Correction: A Review. Bioengineering, 11(6), 525. https://doi.org/10.3390/bioengineering11060525