

Fetal Aortic Blood Flow Velocity and Power Doppler Profiles in the First Trimester: A Comprehensive Study Using High-Definition Flow Imaging

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
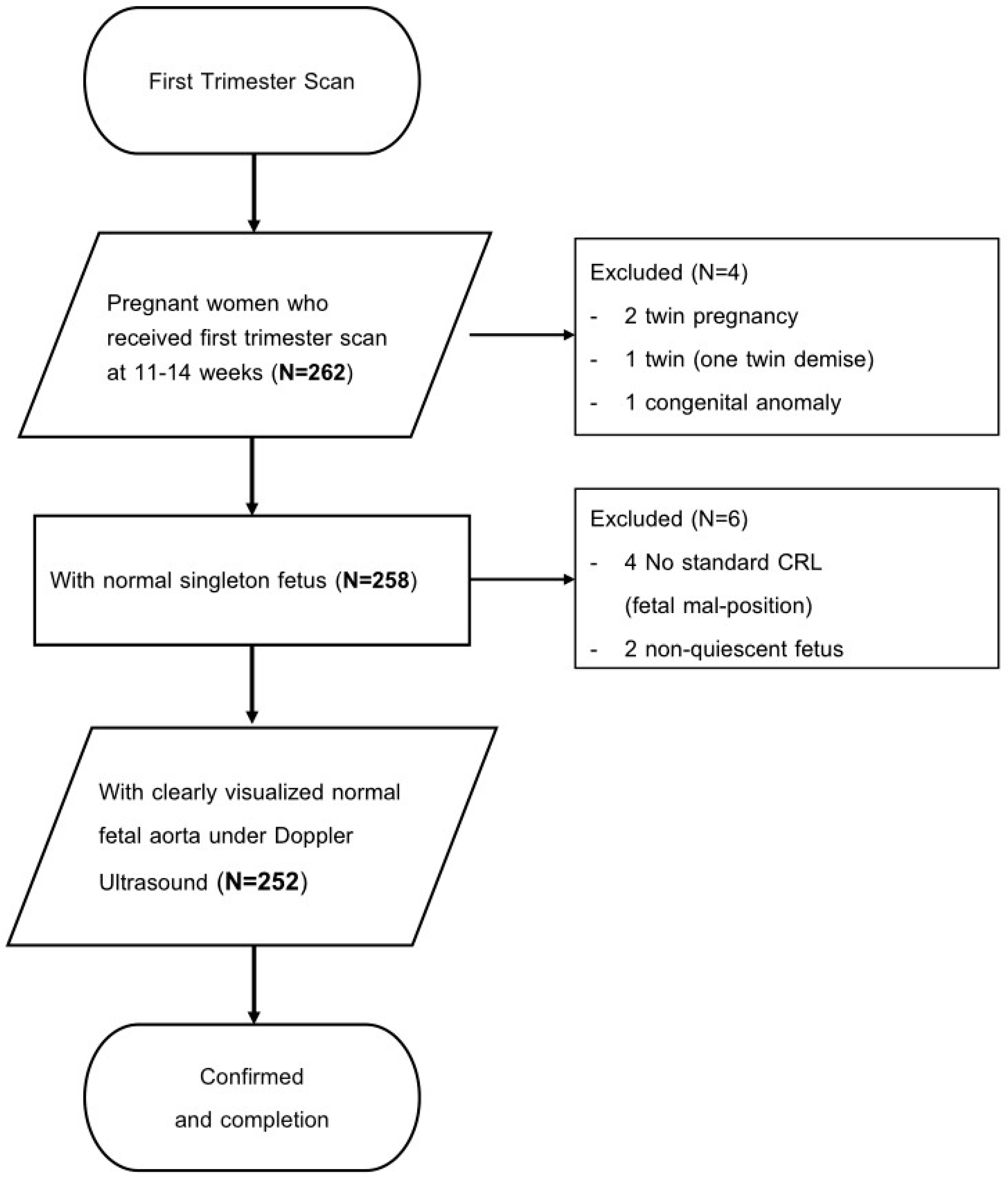
2.1. Study Design and Patient Population
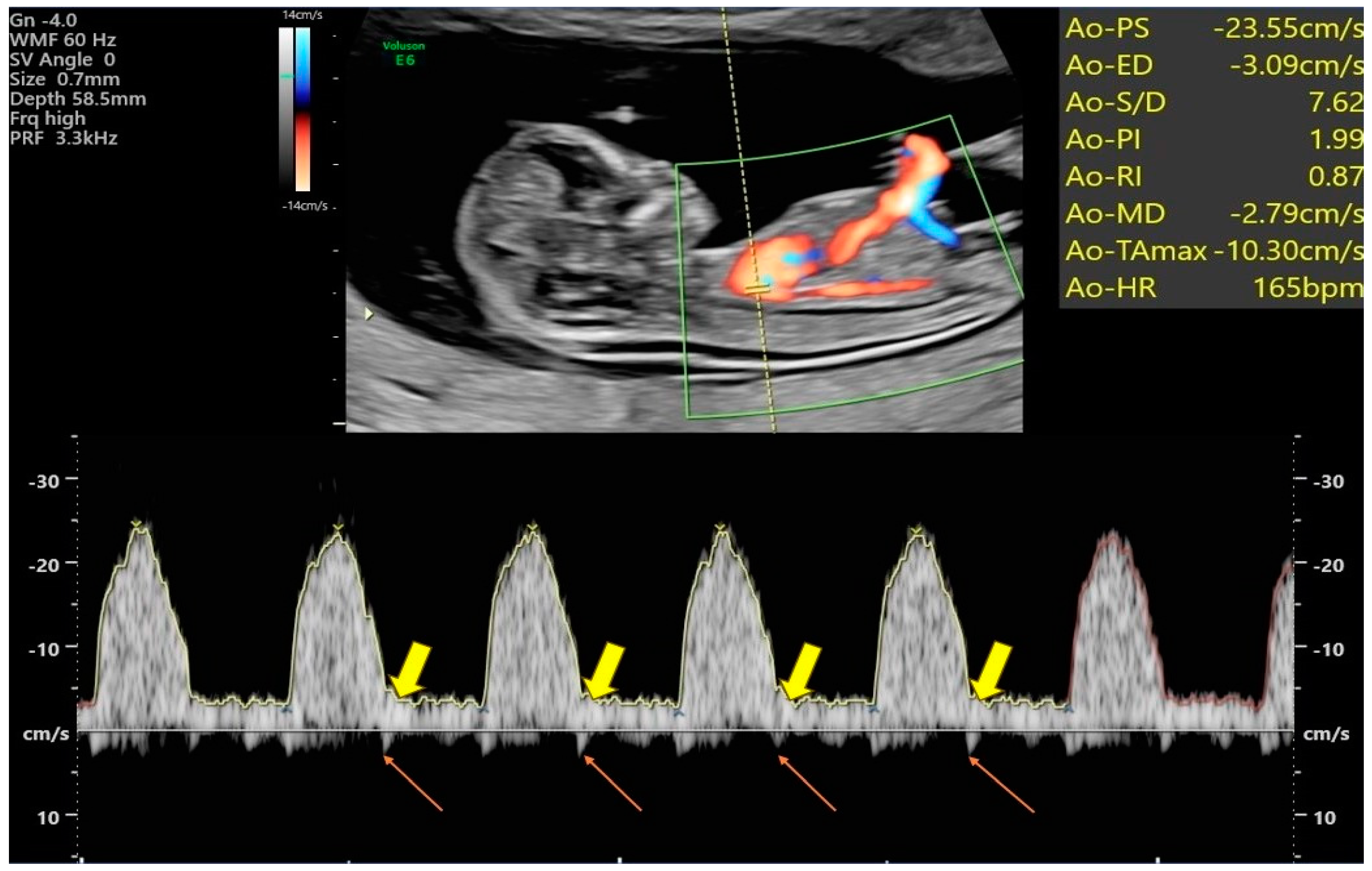
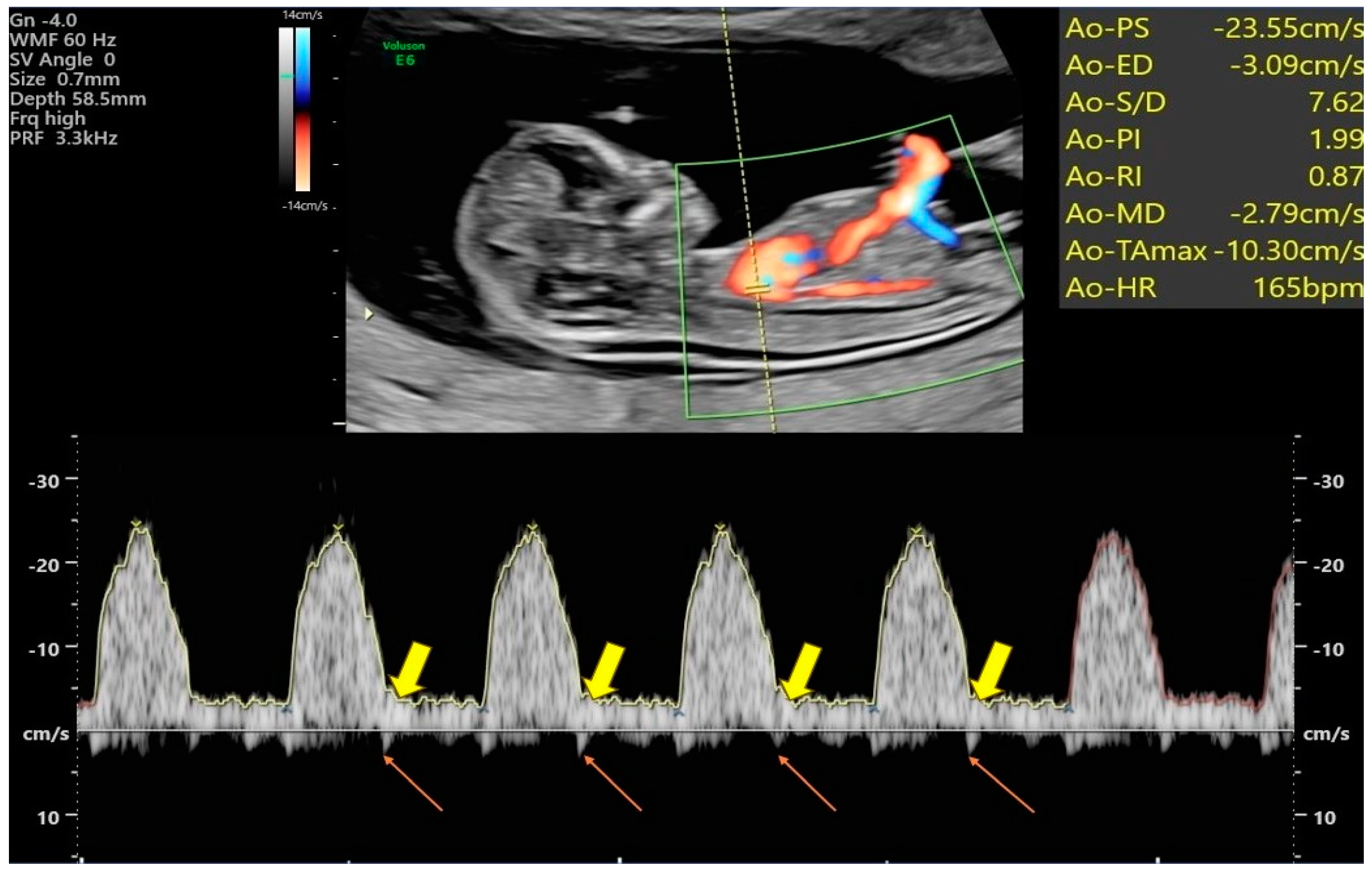
2.2. Power Doppler Angiography of Transabdominal Ultrasound (PDA-TA)
2.3. Assessment of Blood Flow Velocity Waveforms and Indices within the Fetal Aorta
2.4. Statistical Analysis
3. Results
3.1. Basic Data of the General Populations
3.2. Fetal Aortic Artery Doppler Indices
3.3. Additional Fetal Aortic Artery Doppler Indices (IFI and ISI)
3.4. The Intraclass Correlation Coefficients (ICCs) for All Measurements
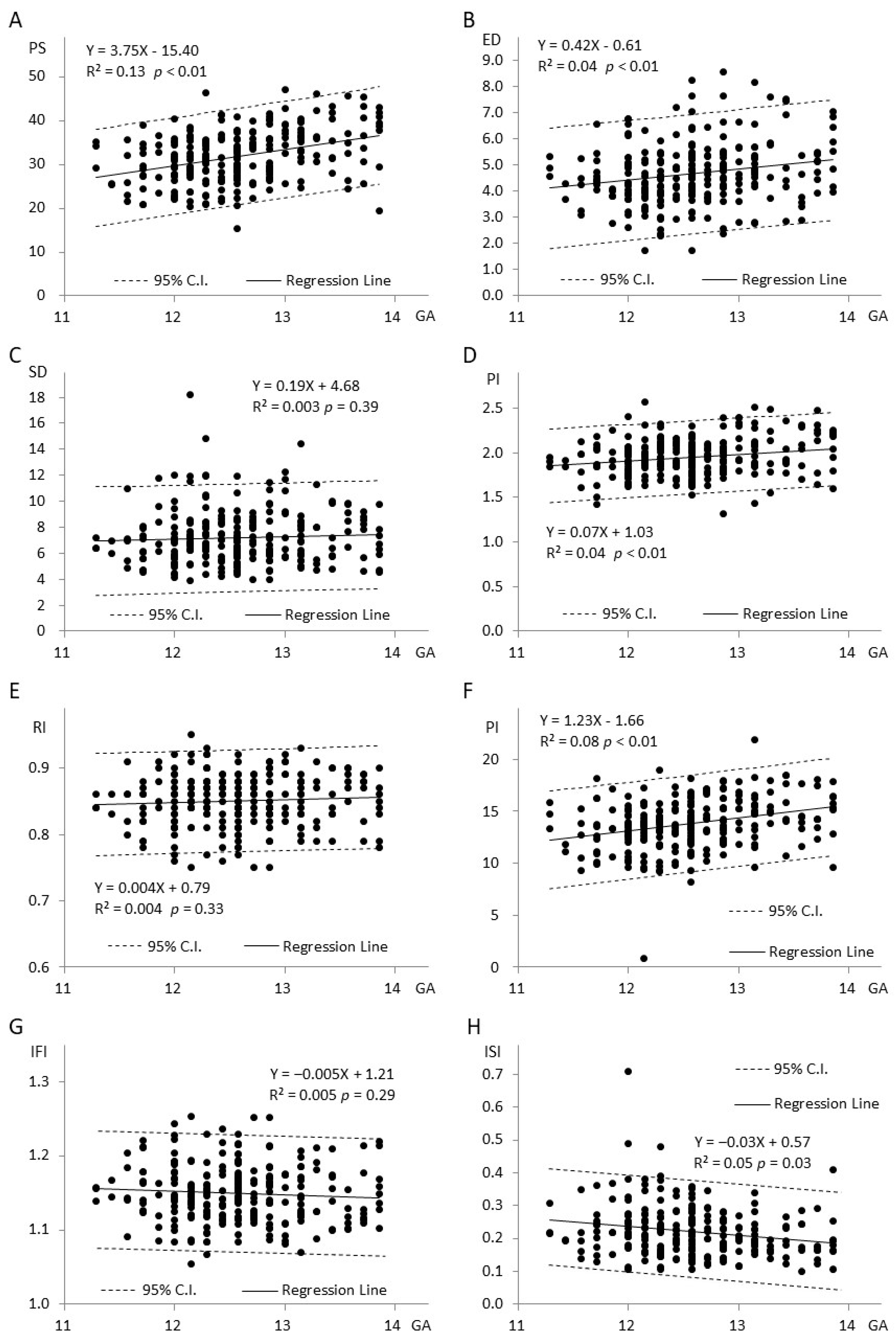
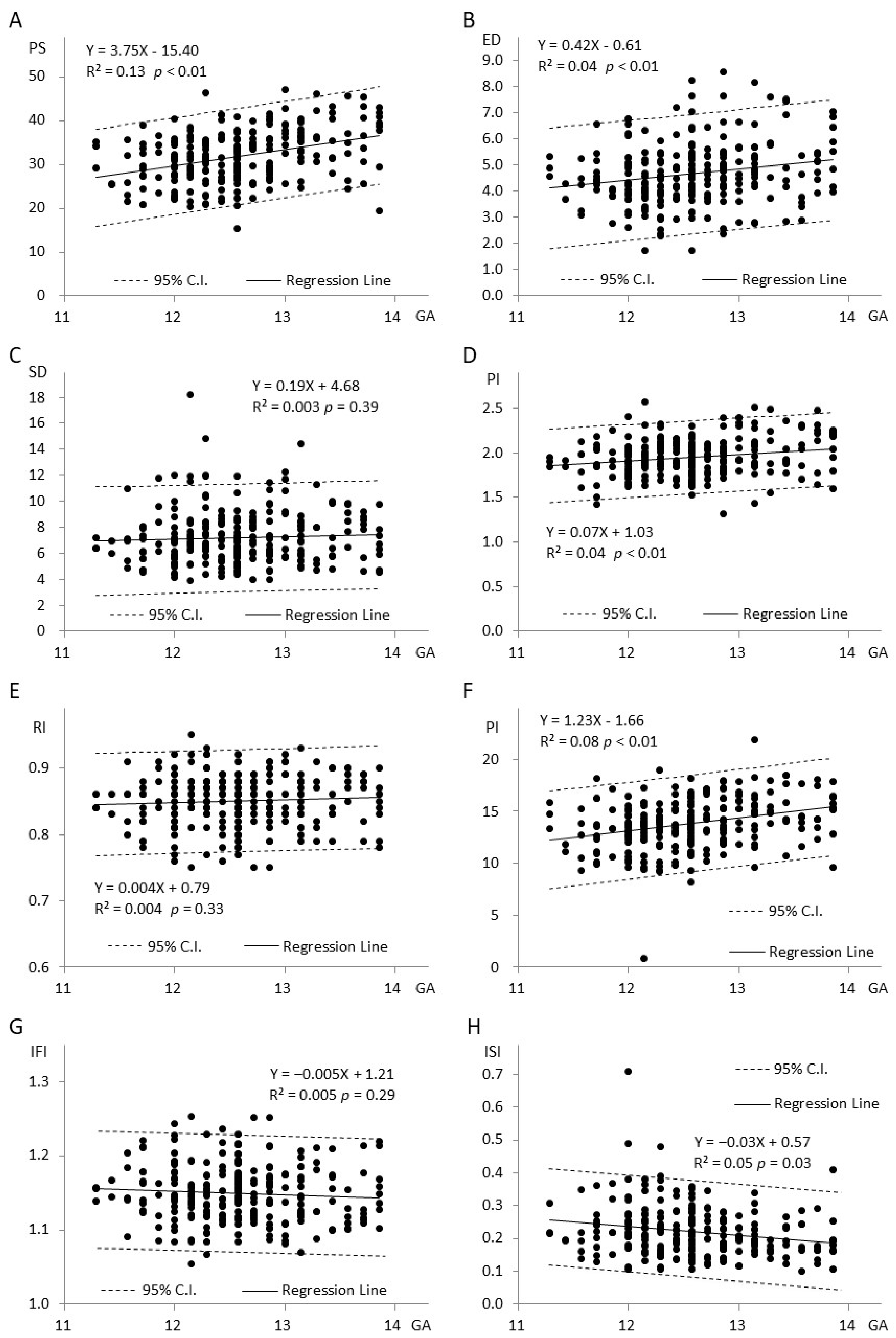
3.5. Relationship between Eight Doppler Indices and Gestational Age (Figure 3A–H)
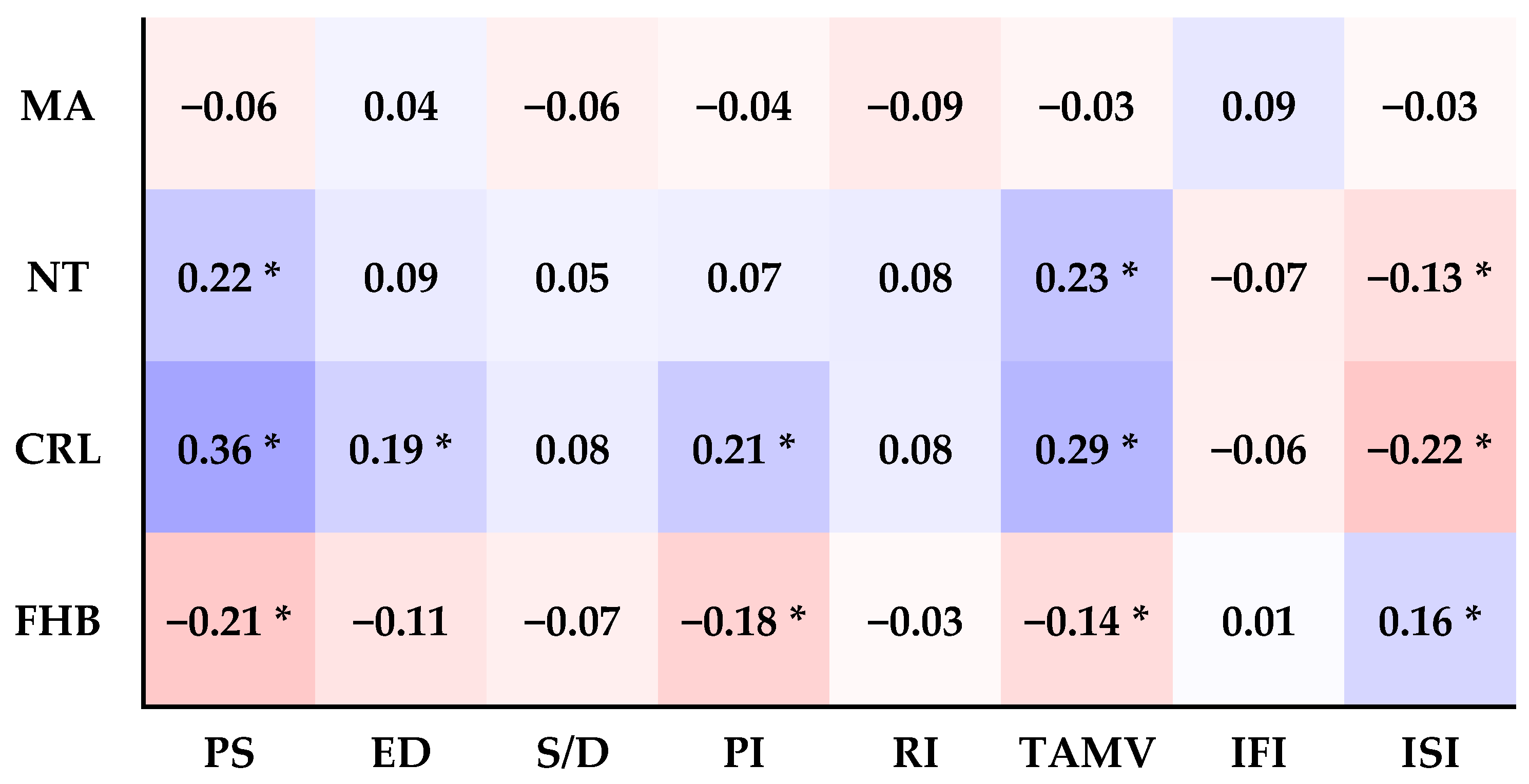
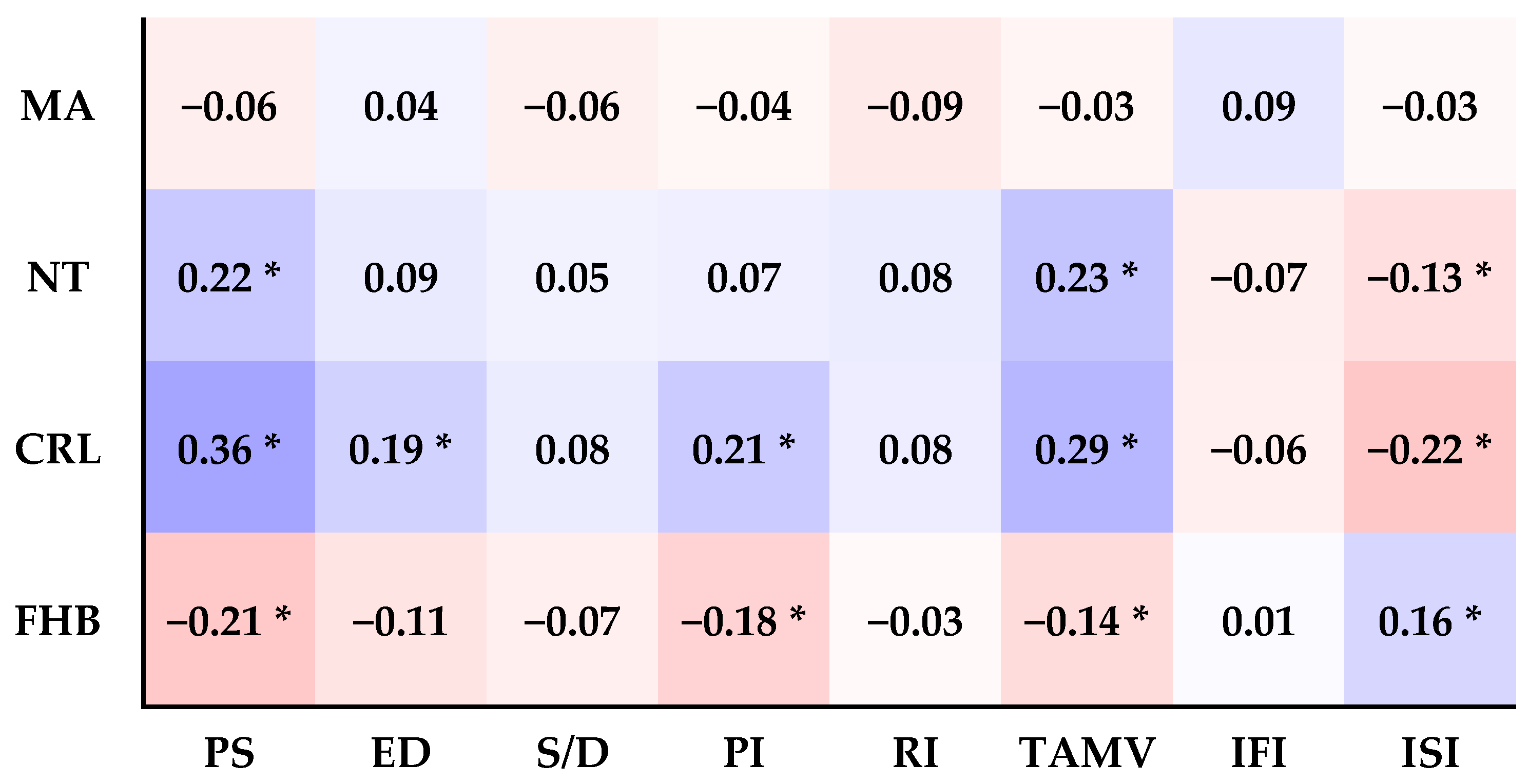
3.6. The Relationship between the Eight Doppler Indices and Maternal Age (MA), Nuchal Thickness (NT), Crown-Rump Length (CRL), and Fetal Heartbeat (FHB) (Figure 4)
- A.
- MA:
- B.
- NT:
- C.
- CRL:
- D.
- FHB:
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fouron, J.C. The unrecognized physiological and clinical significance of the fetal aortic isthmus. Ultrasound Obstet. Gynecol. 2003, 22, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Acharya, G. Technical aspects of aortic isthmus Doppler velocimetry in human fetuses. Ultrasound Obstet. Gynecol. 2009, 33, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Huhta, H.; Junno, J.; Haapsamo, M.; Erkinaro, T.; Ohtonen, P.; Davis, L.E.; Hohimer, A.R.; Acharya, G.; Rasanen, J. Fetal sheep central haemodynamics and cardiac function during occlusion of the ascending aorta. Exp. Physiol. 2018, 103, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Fouron, J.C.; Siles, A.; Montanari, L.; Morin, L.; Ville, Y. Feasibility and reliability of Doppler flow recordings in the fetal aortic isthmus: A multicenter evaluation. Ultrasound Obstet. Gynecol. 2009, 33, 690–693. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Lei, W.; Liu, J.; Yang, B.; Li, H.; Huang, D. The Diastolic and Systolic Velocity-Time Integral Ratio of the Aortic Isthmus Is a Sensitive Indicator of Aortic Coarctation in Fetuses. J. Am. Soc. Echocardiogr. 2019, 32, 1470–1476. [Google Scholar] [CrossRef] [PubMed]
- Tynan, D.; Alphonse, J.; Henry, A.; Welsh, A.W. The Aortic Isthmus: A Significant yet Underexplored Watershed of the Fetal Circulation. Fetal Diagn. Ther. 2016, 40, 81–93. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Martinez, R.; Figueras, F.; Hernández-Andrade, E.; Oros, D.; Gratacós, E. Changes in myocardial performance index and aortic isthmus and ductus venous Doppler in term, small for gestational age fetuses with normal umbilical artery pulsatility index. Ultrasound Obstet. Gynecol. 2011, 38, 400–405. [Google Scholar] [CrossRef] [PubMed]
- Kennelly, M.M.; Farah, N.; Hogan, J.; Reilly, A.; Turner, M.J.; Stuart, B. Longitudinal study of aortic isthmus Doppler in appropriately grown and small-for-gestational-age fetuses with normal and abnormal umbilical artery Doppler. Ultrasound Obstet. Gynecol. 2012, 39, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.M.; Zhu, Y.X.; Tan, Y.; Huang, Y.J.; Yuan, K.; Liu, W.F.; Xu, Z.F. Feasibility of Transabdominal Real-time CDFI and HDFI Techniques for Fetal Pulmonary Vein Display in the First Trimester. Curr. Med. Sci. 2022, 42, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Xie, T.R.; Dimaano, M.M.; Alghrouz, M.I.; Ahmad, M. High-definition blood flow imaging in assessing left ventricular function: Initial experience and comparison with contrast echocardiography. Echocardiography 2019, 36, 546–557. [Google Scholar] [CrossRef]
- Leung, K.-Y.; Wan, Y.-L. Update on Color Flow Imaging in Obstetrics. Life 2022, 12, 226. [Google Scholar] [CrossRef] [PubMed]
- Gama, F.; Custódio, P.; Tsagkridi, A.; Moon, J.; Lloyd, G.; Treibel, T.A.; Bhattacharyya, S. High-definition blood flow imaging improves quantification of left ventricular volumes and ejection fraction. Eur. Heart J. Cardiovasc. Imaging 2024, 25, 278–284. [Google Scholar] [CrossRef] [PubMed]
- He, Y.H.; Liu, K.; Gu, X.Y.; Zhang, Y.; Han, J.C.; Liu, X.W.; Li, Z.A. The application of high-definition flow imaging in fetal hemodynamics. Clin. Exp. Obstet. Gynecol. 2015, 42, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Luo, R.; Zhang, Y.; Jiang, W.; Wang, Y.; Luo, Y. Value of micro-flow imaging and high-definition micro-flow imaging in differentiating malignant and benign breast lesions. Clin. Radiol. 2024, 79, e48–e56. [Google Scholar] [CrossRef] [PubMed]
- Kruizinga, P.; Mastik, F.; van den Oord, S.C.; Schinkel, A.F.; Bosch, J.G.; de Jong, N.; van Soest, G.; van der Steen, A.F. High-definition imaging of carotid artery wall dynamics. Ultrasound Med. Biol. 2014, 40, 2392–2403. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, M.; Wu, G.; Frank, L.; Dimaano, M.M. Validation of left ventricular volume and ejection fraction measurements by high-definition blood flow imaging: Comparisons with cardiac magnetic resonance imaging and contrast echocardiography. Echocardiography 2020, 37, 1975–1980. [Google Scholar] [CrossRef] [PubMed]
- Royston, P.; Wright, E.M. How to construct ‘normal ranges’ for fetal variables. Ultrasound Obstet. Gynecol. 1998, 11, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Del Río, M.; Martínez, J.M.; Figueras, F.; López, M.; Palacio, M.; Gómez, O.; Coll, O.; Puerto, B. Reference ranges for Doppler parameters of the fetal aortic isthmus during the second half of pregnancy. Ultrasound Obstet. Gynecol. 2006, 28, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Vimpeli, T.; Huhtala, H.; Wilsgaard, T.; Acharya, G. Fetal aortic isthmus blood flow and the fraction of cardiac output distributed to the upper body and brain at 11–20 weeks of gestation. Ultrasound Obstet. Gynecol. 2009, 33, 538–544. [Google Scholar] [CrossRef]
- Chabaneix, J.; Fouron, J.C.; Sosa-Olavarria, A.; Gendron, R.; Dahdah, N.; Berger, A.; Brisebois, S. Profiling left and right ventricular proportional output during fetal life with a novel systolic index in the aortic isthmus. Ultrasound Obstet. Gynecol. 2014, 44, 176–181. [Google Scholar] [CrossRef]
- Ruskamp, J.; Fouron, J.C.; Gosselin, J.; Raboisson, M.J.; Infante-Rivard, C.; Proulx, F. Reference values for an index of fetal aortic isthmus blood flow during the second half of pregnancy. Ultrasound Obstet. Gynecol. 2003, 21, 441–444. [Google Scholar] [CrossRef]
- Hata, T.; Inubashiri, E.; Kanenishi, K.; Akiyama, M.; Tanaka, H.; Shiota, A.; Yanagihara, T.; Ohno, M. Nuchal translucency thickness and fetal cardiac flow velocity in normal fetuses at 11–13 weeks of gestation. Gynecol. Obstet. Investig. 2002, 53, 209–213. [Google Scholar] [CrossRef]
- Fouron, J.C.; Zarelli, M.; Drblik, P.; Lessard, M. Flow velocity profile of the fetal aortic isthmus through normal gestation. Am. J. Cardiol. 1994, 74, 483–486. [Google Scholar] [CrossRef] [PubMed]
- Ursem, N.T.; Clark, E.B.; Keller, B.B.; Hop, W.C.; Wladimiroff, J.W. Assessment of fetal heart rate variability and velocity variability by Doppler velocimetry of the descending aorta at 10–20 weeks of gestation. Ultrasound Obstet. Gynecol. 1999, 14, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Zwanenburg, F.; Jongbloed, M.R.M.; van Geloven, N.; Ten Harkel, A.D.J.; van Lith, J.M.M.; Haak, M.C. Assessment of human fetal cardiac autonomic nervous system development using color tissue Doppler imaging. Echocardiography 2021, 38, 974–981. [Google Scholar] [CrossRef] [PubMed]
- Ferraz, M.M.; Araújo, F.D.V.; Carvalho, P.R.N.; Sá, R.A.M. Aortic Isthmus Doppler Velocimetry in Fetuses with Intrauterine Growth Restriction: A Literature Review. Rev. Bras. Ginecol. Obstet. 2020, 42, 289–296. [Google Scholar] [CrossRef]
- Chen, Z.; Zhao, H.; Zhao, Y.; Han, J.; Yang, X.; Throckmorton, A.; Wei, Z.; Ge, S.; He, Y. Retrograde flow in aortic isthmus in normal and fetal heart disease by principal component analysis and computational fluid dynamics. Echocardiography 2022, 39, 166–177. [Google Scholar] [CrossRef]
- Hackmon, R.; Librach, C.; Burwick, R.; Rodrigues, N.; Farine, D.; Berger, H. Do Early Fetal Measurements and Nuchal Translucency Correlate with Term Birth Weight? J. Obstet. Gynaecol. Can. 2017, 39, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, E.; Pajkrt, E.; Snijders, R.J.; Bilardo, C.M. High macrosomia rate in healthy fetuses after enlarged nuchal translucency. Prenat. Diagn. 2014, 34, 103–108. [Google Scholar] [CrossRef]
- Kumar, M.; Singh, S.; Sharma, K.; Singh, R.; Ravi, V.; Bhattacharya, J. Adverse fetal outcome: Is first trimester ultrasound and Doppler better predictor than biomarkers? J. Matern. Fetal Neonatal Med. 2017, 30, 1410–1416. [Google Scholar] [CrossRef]
- Ciccone, M.M.; Scicchitano, P.; Salerno, C.; Gesualdo, M.; Fornarelli, F.; Zito, A.; Filippucci, L.; Riccardi, R.; Cortese, F.; Pini, F.; et al. Aorta structural alterations in term neonates: The role of birth and maternal characteristics. Biomed. Res. Int. 2013, 2013, 459168. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. of participants | 252 cases |
| Maternal characteristics | Mean (SD) or % |
| Age (y/o) | 29.19 (3.32) |
| Gestational Age (week) | 12.57 (1.38) |
| Nulliparity | 54% |
| Fetal characteristics | |
| Birth weight (g): | 2908 (308) |
| >10th centile | 89% |
| <10th centile | 11% |
| Mode of delivery: | |
| Spontaneous | 61% |
| Cesarean section | 39% |
| Apgar score (1 min/5 min) | 8/9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, Y.-C.; Chen, C.-H.; Lu, H.-T.; Lee, Y.-L.; Chen, P.-Y.; Wu, T.-Y.; Tien, M.-H.; Wu, C.-H.; Huang, J.Y.-J.; Hsiao, C.-H.; et al. Fetal Aortic Blood Flow Velocity and Power Doppler Profiles in the First Trimester: A Comprehensive Study Using High-Definition Flow Imaging. Bioengineering 2024, 11, 378. https://doi.org/10.3390/bioengineering11040378
Wu Y-C, Chen C-H, Lu H-T, Lee Y-L, Chen P-Y, Wu T-Y, Tien M-H, Wu C-H, Huang JY-J, Hsiao C-H, et al. Fetal Aortic Blood Flow Velocity and Power Doppler Profiles in the First Trimester: A Comprehensive Study Using High-Definition Flow Imaging. Bioengineering. 2024; 11(4):378. https://doi.org/10.3390/bioengineering11040378
Chicago/Turabian StyleWu, Yi-Cheng, Ching-Hsuan Chen, Hsin-Tzu Lu, Yu-Li Lee, Pi-Yu Chen, Ting-Yu Wu, Ming-Hsun Tien, Chiung-Hui Wu, Jack Yu-Jen Huang, Ching-Hua Hsiao, and et al. 2024. "Fetal Aortic Blood Flow Velocity and Power Doppler Profiles in the First Trimester: A Comprehensive Study Using High-Definition Flow Imaging" Bioengineering 11, no. 4: 378. https://doi.org/10.3390/bioengineering11040378
APA StyleWu, Y.-C., Chen, C.-H., Lu, H.-T., Lee, Y.-L., Chen, P.-Y., Wu, T.-Y., Tien, M.-H., Wu, C.-H., Huang, J. Y.-J., Hsiao, C.-H., & Chu, W.-C. (2024). Fetal Aortic Blood Flow Velocity and Power Doppler Profiles in the First Trimester: A Comprehensive Study Using High-Definition Flow Imaging. Bioengineering, 11(4), 378. https://doi.org/10.3390/bioengineering11040378