

Assessment of Postural Control in Children with Movement Disorders by Means of a New Technological Tool: A Pilot Study

 , , , , ,
, , , , ,  ,
,  and
and 
Abstract

1. Introduction
1.1. Movement Disorders in Children: Definition and State of Art
1.2. Postural Control Assessment and Treatment with Technology: State of the Art
2. Materials and Methods
2.1. Participants
- -
- Presence of MD as dystonia, chorea, or chorea–dystonia, with different etiology;
- -
- Level I to III of the Gross Motor Function Classification System (GMFCS);
- -
- Exclusion criteria were:
- -
- GMFCS level > III;
- -
- Verbal Intelligence Quotient < 80, as assessed with the Wechsler Intelligence Scale for Children that prevented understanding the required tasks.
2.2. VRRS System
2.3. VRRS Balance Assessment
2.4. VRRS Data Collection
- -
- Mean distance of the COP (MD_COP), AP (MD_AP) and ML (MD_ML), i.e., average displacement of the COP, AP and ML components from the central point of the stabilogram, respectively [mm];
- -
- Root mean square distance of the COP (RMS_COP), AP (RMS_AP) and ML (RMS_ML) from the central point of the stabilogram [mm];
- -
- Total path length (excursion) of the COP (ESC_COP), i.e., the sum of the distances between consecutive points on the COP path and its AP (ESC_AP) and ML (ESC_ML) components [mm];
- -
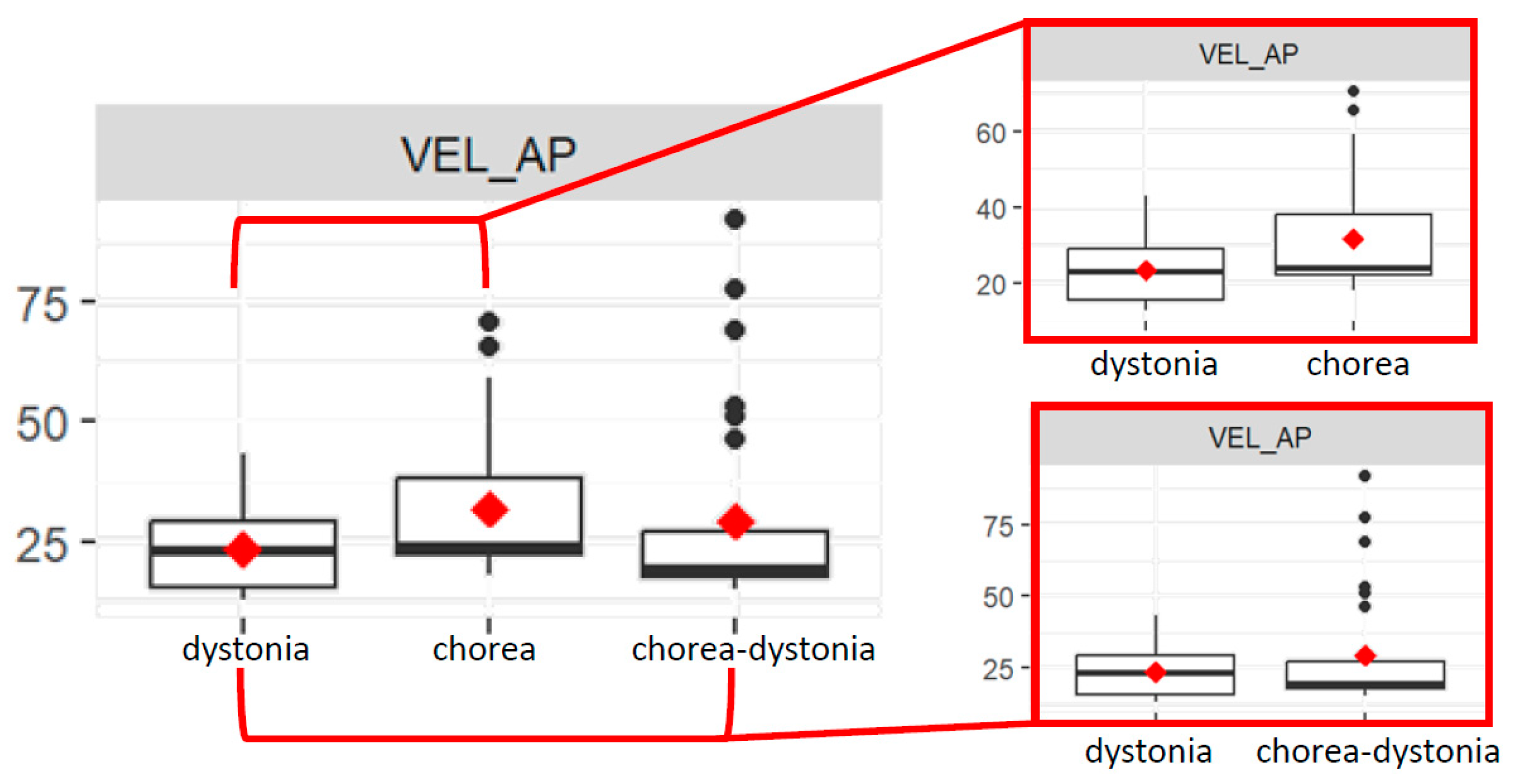
- Average velocity of the COP (VEL_COP), AP (VEL_AP) and ML (VEL_ML), defined as the total excursion divided by an analysed temporal interval (60 s) [mm/s];
- -
- Sway area enclosed by the COP path per unit of time (SWAY) [mm2/s];
- -
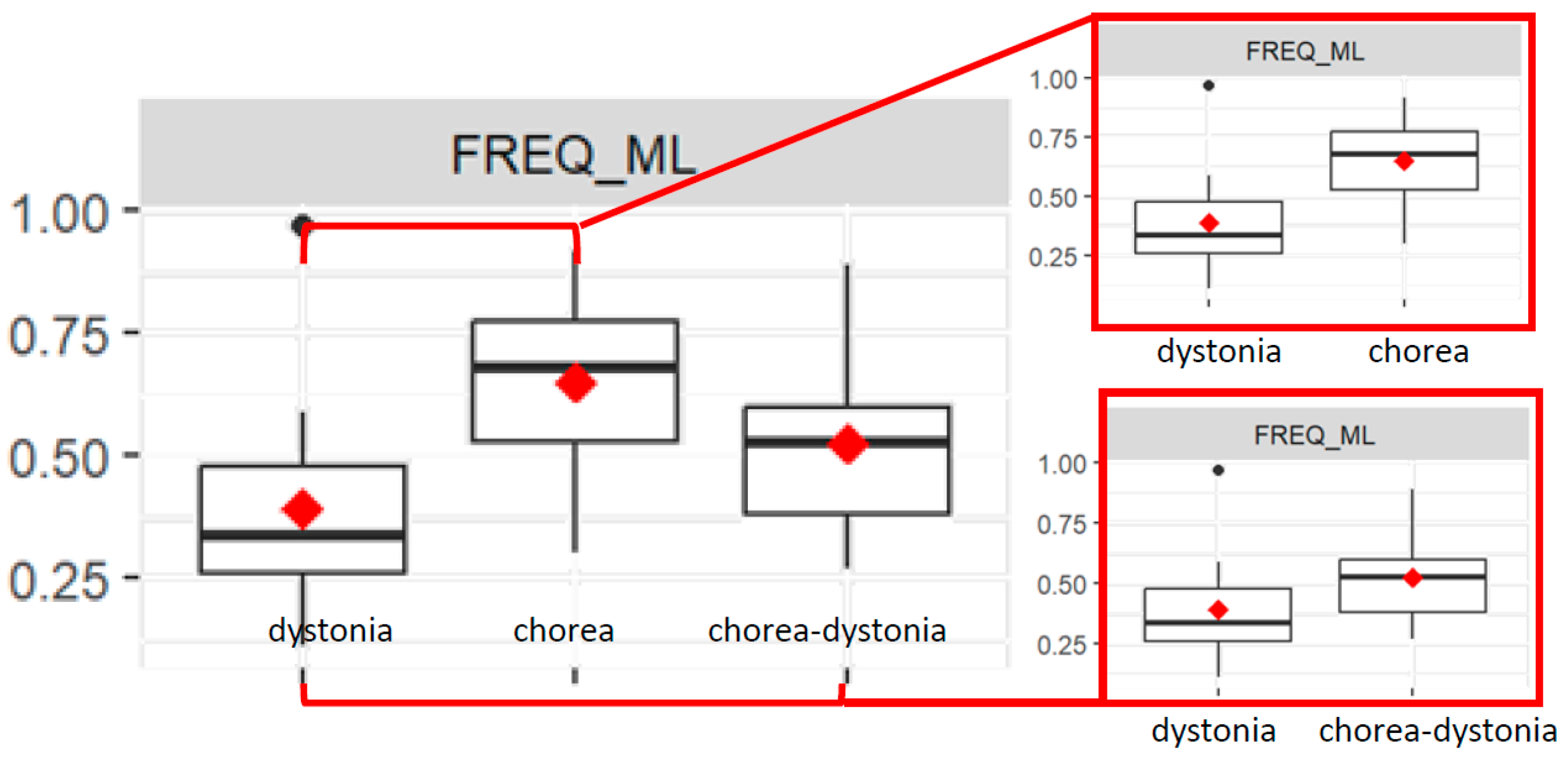
- Mean rotational frequency of the COP (FREQ_COP), AP (FREQ_AP) and ML (FREQ_ML) [Hz].
2.5. Statistical Analysis
3. Results
3.1. Participants
3.2. VRRS-Derived COP Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kurian, M.A.; Dale, R.C. Movement Disorders Presenting in Childhood. CONTINUUM Lifelong Learn. Neurol. 2016, 22, 1159–1185. [Google Scholar] [CrossRef] [PubMed]
- Singer, H.S.; Mink, J.W.; Gilbert, D.L.; Jankovic, J. Movement Disorders in Childhood, 2nd ed.; Academic Press: London, UK, 2016. [Google Scholar]
- Sanger, T.D.; Chen, D.; Fehlings, D.L.; Hallett, M.; Lang, A.E.; Mink, J.W.; Singer, H.S.; Alter, K.; Ben-Pazi, H.; Butler, E.E.; et al. Definition and Classification of Hyperkinetic Movements in Childhood. Mov. Disord. 2010, 25, 1538–1549. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Cazorla, A.; Duarte, S.T. Parkinsonism and Inborn Errors of Metabolism. J. Inherit. Metab. Dis. 2014, 37, 627–642. [Google Scholar] [CrossRef] [PubMed]
- Monbaliu, E.; Himmelmann, K.; Lin, J.-P.; Ortibus, E.; Bonouvrié, L.; Feys, H.; Vermeulen, R.J.; Dan, B. Clinical Presentation and Management of Dyskinetic Cerebral Palsy. Lancet Neurol. 2017, 16, 741–749. [Google Scholar] [CrossRef] [PubMed]
- Burke, R.E.; Fahn, S.; Marsden, C.D.; Bressman, S.B.; Moskowitz, C.; Friedman, J. Validity and Reliability of a Rating Scale for the Primary Torsion Dystonias. Neurology 1985, 35, 73. [Google Scholar] [CrossRef] [PubMed]
- Barry, M.J.; VanSwearingen, J.M.; Albright, A.L. Reliability and Responsiveness of the Barry–Albright Dystonia Scale. Dev. Med. Child Neurol. 1999, 41, 404–411. [Google Scholar] [CrossRef]
- Comella, C.L.; Leurgans, S.; Wuu, J.; Stebbins, G.T.; Chmura, T.; The Dystonia Study Group. Rating Scales for Dystonia: A Multicenter Assessment. Mov. Disord. 2003, 18, 303–312. [Google Scholar] [CrossRef]
- Simonin, C.; Delliaux, M.; Krystkowiak, P. [The UHDRS scale]. Rev. Neurol. 2009, 165 Spec No 3, F179–F187. [Google Scholar]
- Stewart, K.; Harvey, A.; Johnston, L.M. A Systematic Review of Scales to Measure Dystonia and Choreoathetosis in Children with Dyskinetic Cerebral Palsy. Develop. Med. Child Neuro. 2017, 59, 786–795. [Google Scholar] [CrossRef]
- MD-CRS Group; Battini, R.; Sgandurra, G.; Menici, V.; Scalise, R.; Olivieri, I.; Di Pietro, R.; Lucibello, S.; Giannini, M.T.; Cioni, G. Movement Disorders-Childhood Rating Scale 4-18 Revised in Children with Dyskinetic Cerebral Palsy. Eur. J. Phys. Rehabil. Med. 2020, 56, 272–278. [Google Scholar] [CrossRef]
- Griffiths, A.; Toovey, R.; Morgan, P.E.; Spittle, A.J. Psychometric Properties of Gross Motor Assessment Tools for Children: A Systematic Review. BMJ Open 2018, 8, e021734. [Google Scholar] [CrossRef] [PubMed]
- Berg, K.O.; Wood-Dauphinee, S.L.; Williams, J.I.; Maki, B. Measuring Balance in the Elderly: Validation of an Instrument. Can. J. Public Health 1992, 83 (Suppl. S2), S7–S11. [Google Scholar] [PubMed]
- Downs, S.; Marquez, J.; Chiarelli, P. The Berg Balance Scale Has High Intra- and Inter-Rater Reliability but Absolute Reliability Varies across the Scale: A Systematic Review. J. Physiother. 2013, 59, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Duncan, P.W.; Weiner, D.K.; Chandler, J.; Studenski, S. Functional Reach: A New Clinical Measure of Balance. J. Gerontol. 1990, 45, M192–M197. [Google Scholar] [CrossRef]
- Verbecque, E.; Schepens, K.; Theré, J.; Schepens, B.; Klingels, K.; Hallemans, A. The Timed Up and Go Test in Children: Does Protocol Choice Matter? A Systematic Review. Pediatr. Phys. Ther. 2019, 31, 22–31. [Google Scholar] [CrossRef]
- Paillard, T.; Noé, F. Techniques and Methods for Testing the Postural Function in Healthy and Pathological Subjects. BioMed Res. Int. 2015, 2015, 891390. [Google Scholar] [CrossRef]
- Ferhan, S. Technological Methods Used in Evaluating the Balance. Int. J. Spine Res. 2020, 60–63. [Google Scholar] [CrossRef]
- Baker, N.; Gough, C.; Gordon, S. Classification of Balance Assessment Technology: A Scoping Review of Systematic Reviews. Stud. Health Technol. Inf. 2020, 268, 45–59. [Google Scholar] [CrossRef]
- Chen, B.; Liu, P.; Xiao, F.; Liu, Z.; Wang, Y. Review of the Upright Balance Assessment Based on the Force Plate. IJERPH 2021, 18, 2696. [Google Scholar] [CrossRef]
- Boonstra, T.A.; Schouten, A.C.; Van Der Kooij, H. Identification of the Contribution of the Ankle and Hip Joints to Multi-Segmental Balance Control. J. NeuroEngineering Rehabil. 2013, 10, 23. [Google Scholar] [CrossRef]
- Robinson, J.; Dixon, J.; Macsween, A.; Van Schaik, P.; Martin, D. The Effects of Exergaming on Balance, Gait, Technology Acceptance and Flow Experience in People with Multiple Sclerosis: A Randomized Controlled Trial. BMC Sports Sci. Med. Rehabil. 2015, 7, 8. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.J.; Adair, B.S.; Pearce, A.J.; Said, C.M.; Ozanne, E.; Morris, M.M. Effectiveness and Feasibility of Virtual Reality and Gaming System Use at Home by Older Adults for Enabling Physical Activity to Improve Health-Related Domains: A Systematic Review. Age Ageing 2014, 43, 188–195. [Google Scholar] [CrossRef]
- Kim, J.H.; Jang, S.H.; Kim, C.S.; Jung, J.H.; You, J.H. Use of Virtual Reality to Enhance Balance and Ambulation in Chronic Stroke: A Double-Blind, Randomized Controlled Study. Am. J. Phys. Med. Rehabil. 2009, 88, 693–701. [Google Scholar] [CrossRef] [PubMed]
- Hung, J.-W.; Chou, C.-X.; Hsieh, Y.-W.; Wu, W.-C.; Yu, M.-Y.; Chen, P.-C.; Chang, H.-F.; Ding, S.-E. Randomized Comparison Trial of Balance Training by Using Exergaming and Conventional Weight-Shift Therapy in Patients with Chronic Stroke. Arch. Phys. Med. Rehabil. 2014, 95, 1629–1637. [Google Scholar] [CrossRef] [PubMed]
- Deutsch, J.E.; Borbely, M.; Filler, J.; Huhn, K.; Guarrera-Bowlby, P. Use of a Low-Cost, Commercially Available Gaming Console (Wii) for Rehabilitation of an Adolescent with Cerebral Palsy. Phys. Ther. 2008, 88, 1196–1207. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, L.; Esculier, J.; Vaudrin, J.; Bériault, P.; Gagnon, K. Home-Based Balance Training Programme Using Wii Fit with Balance Board for Parkinsons’s Disease: A Pilot Study. J. Rehabil. Med. 2012, 44, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Alves, M.L.M.; Mesquita, B.S.; Morais, W.S.; Leal, J.C.; Satler, C.E.; Dos Santos Mendes, F.A. Nintendo WiiTM Versus Xbox KinectTM for Assisting People with Parkinson’s Disease. Percept. Mot. Ski. 2018, 125, 003151251876920. [Google Scholar] [CrossRef]
- Betker, A.L.; Desai, A.; Nett, C.; Kapadia, N.; Szturm, T. Game-Based Exercises for Dynamic Short-Sitting Balance Rehabilitation of People with Chronic Spinal Cord and Traumatic Brain Injuries. Phys. Ther. 2007, 87, 1389–1398. [Google Scholar] [CrossRef]
- Heidt, C.; Vrankovic, M.; Mendoza, A.; Hollander, K.; Dreher, T.; Rueger, M. Simplified Digital Balance Assessment in Typically Developing School Children. Gait Posture 2021, 84, 389–394. [Google Scholar] [CrossRef]
- Dos Santos, L.R.A.; Carregosa, A.A.; Masruha, M.R.; Dos Santos, P.A.; Da Silveira Coêlho, M.L.; Ferraz, D.D.; Da Silva Ribeiro, N.M. The Use of Nintendo Wii in the Rehabilitation of Poststroke Patients: A Systematic Review. J. Stroke Cerebrovasc. Dis. 2015, 24, 2298–2305. [Google Scholar] [CrossRef]
- Bonnechère, B.; Jansen, B.; Omelina, L.; Van Sint Jan, S. The Use of Commercial Video Games in Rehabilitation: A Systematic Review. Int. J. Rehabil. Res. 2016, 39, 277–290. [Google Scholar] [CrossRef]
- Beani, E.; Filogna, S.; Martini, G.; Barzacchi, V.; Ferrari, A.; Guidi, E.; Menici, V.; Cioni, G.; Sgandurra, G. Application of Virtual Reality Rehabilitation System for the Assessment of Postural Control While Standing in Typical Children and Peers with Neurodevelopmental Disorders. Gait Posture 2022, 92, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Martini, G.; Beani, E.; Filogna, S.; Menici, V.; Cioni, G.; Battini, R.; Sgandurra, G. New Technological Approach for the Evaluation of Postural Control Abilities in Children with Developmental Coordination Disorder. Children 2022, 9, 957. [Google Scholar] [CrossRef] [PubMed]
- Menici, V.; Barzacchi, V.; Filogna, S.; Beani, E.; Tinelli, F.; Cioni, G.; Sgandurra, G. Tele-Rehabilitation for Postural Control by Means of Virtual Reality Rehabilitation System in an Adolescent with Motor Disorder: A Case Study. Front. Psychol. 2021, 12, 720677. [Google Scholar] [CrossRef]
- Olivieri, I.; Chiappedi, M.; Meriggi, P.; Mazzola, M.; Grandi, A.; Angelini, L. Rehabilitation of Children with Hemiparesis: A Pilot Study on the Use of Virtual Reality. BioMed Res. Int. 2013, 2013, 695935. [Google Scholar] [CrossRef] [PubMed]
- Luque-Moreno, C.; Oliva-Pascual-Vaca, A.; Kiper, P.; Rodríguez-Blanco, C.; Agostini, M.; Turolla, A. Virtual Reality to Assess and Treat Lower Extremity Disorders in Post-Stroke Patients. Methods Inf. Med. 2016, 55, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Cha, K.; Wang, J.; Li, Y.; Shen, L.; Chen, Z.; Long, J. A Novel Upper-Limb Tracking System in a Virtual Environment for Stroke Rehabilitation. J. NeuroEngineering Rehabil. 2021, 18, 166. [Google Scholar] [CrossRef] [PubMed]
- Manuli, A.; Maggio, M.G.; Tripoli, D.; Gullì, M.; Cannavò, A.; La Rosa, G.; Sciarrone, F.; Avena, G.; Calabrò, R.S. Patients’ Perspective and Usability of Innovation Technology in a New Rehabilitation Pathway: An Exploratory Study in Patients with Multiple Sclerosis. Mult. Scler. Relat. Disord. 2020, 44, 102312. [Google Scholar] [CrossRef]
- De Luca, R.; Maggio, M.G.; Naro, A.; Portaro, S.; Cannavò, A.; Calabrò, R.S. Can Patients with Severe Traumatic Brain Injury Be Trained with Cognitive Telerehabilitation? An Inpatient Feasibility and Usability Study. J. Clin. Neurosci. 2020, 79, 246–250. [Google Scholar] [CrossRef]
- Alemanno, F.; Houdayer, E.; Emedoli, D.; Locatelli, M.; Mortini, P.; Mandelli, C.; Raggi, A.; Iannaccone, S. Efficacy of Virtual Reality to Reduce Chronic Low Back Pain: Proof-of-Concept of a Non-Pharmacological Approach on Pain, Quality of Life, Neuropsychological and Functional Outcome. PLoS ONE 2019, 14, e0216858. [Google Scholar] [CrossRef]
- Kommalapati, R.; Michmizos, K.P. Virtual Reality for Pediatric Neuro-Rehabilitation: Adaptive Visual Feedback of Movement to Engage the Mirror Neuron System. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; IEEE: Piscataway, NJ, USA, 2016; pp. 5849–5852. [Google Scholar]
- Piron, L.; Turolla, A.; Agostini, M.; Zucconi, C.; Tonin, P.; Piccione, F.; Dam, M. Assessment and Treatment of the Upper Limb by Means of Virtual Reality in Post-Stroke Patients. Stud. Health Technol. Inform. 2009, 145, 55–62. [Google Scholar]
- Agostini, M.; Moja, L.; Banzi, R.; Pistotti, V.; Tonin, P.; Venneri, A.; Turolla, A. Telerehabilitation and Recovery of Motor Function: A Systematic Review and Meta-Analysis. J. Telemed. Telecare 2015, 21, 202–213. [Google Scholar] [CrossRef] [PubMed]
- Eysel-Gosepath, K.; McCrum, C.; Epro, G.; Brüggemann, G.-P.; Karamanidis, K. Visual and Proprioceptive Contributions to Postural Control of Upright Stance in Unilateral Vestibulopathy. Somatosens. Mot. Res. 2016, 33, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Scoppa, F.; Capra, R.; Gallamini, M.; Shiffer, R. Clinical Stabilometry Standardization. Gait Posture 2013, 37, 290–292. [Google Scholar] [CrossRef]
- Bloem, B.R.; Marinus, J.; Almeida, Q.; Dibble, L.; Nieuwboer, A.; Post, B.; Ruzicka, E.; Goetz, C.; Stebbins, G.; Martinez-Martin, P.; et al. Measurement Instruments to Assess Posture, Gait, and Balance in Parkinson’s Disease: Critique and Recommendations: Posture, Gait, and Balance Instruments in PD. Mov. Disord. 2016, 31, 1342–1355. [Google Scholar] [CrossRef] [PubMed]
- Verbecque, E.; Vereeck, L.; Hallemans, A. Postural Sway in Children: A Literature Review. Gait Posture 2016, 49, 402–410. [Google Scholar] [CrossRef]
- Geuze, R.H. Postural Control in Children with Developmental Coordination Disorder. Neural Plast. 2005, 12, 183–196. [Google Scholar] [CrossRef]
- Donker, S.F.; Ledebt, A.; Roerdink, M.; Savelsbergh, G.J.P.; Beek, P.J. Children with Cerebral Palsy Exhibit Greater and More Regular Postural Sway than Typically Developing Children. Exp. Brain Res. 2008, 184, 363–370. [Google Scholar] [CrossRef]
- Saxena, S.; Rao, B.K.; Kumaran, S. Analysis of Postural Stability in Children with Cerebral Palsy and Children with Typical Development: An Observational Study. Pediatr. Phys. Ther. 2014, 26, 325–330. [Google Scholar] [CrossRef]
- Pierret, J.; Caudron, S.; Paysant, J.; Beyaert, C. Impaired Postural Control of Axial Segments in Children with Cerebral Palsy. Gait Posture 2021, 86, 266–272. [Google Scholar] [CrossRef]
- Schoch, B.; Hogan, A.; Gizewski, E.R.; Timmann, D.; Konczak, J. Balance Control in Sitting and Standing in Children and Young Adults with Benign Cerebellar Tumors. Cerebellum 2010, 9, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Termsarasab, P. Chorea. CONTINUUM Lifelong Learn. Neurol. 2019, 25, 1001–1035. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A.; Cioni, G. Le Forme Discinetiche Delle Paralisi Cerebrali Infantili; Riabilitazione in età evolutiva, Nr. 5.; Edizioni Del Cerro: Pisa, Italy, 1996. [Google Scholar]
- Prieto, T.E.; Myklebust, J.B.; Hoffmann, R.G.; Lovett, E.G.; Myklebust, B.M. Measures of Postural Steadiness: Differences between Healthy Young and Elderly Adults. IEEE Trans. Biomed. Eng. 1996, 43, 956–966. [Google Scholar] [CrossRef] [PubMed]
- Clark, R.A.; Mentiplay, B.F.; Pua, Y.-H.; Bower, K.J. Reliability and Validity of the Wii Balance Board for Assessment of Standing Balance: A Systematic Review. Gait Posture 2018, 61, 40–54. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Chorea Group vs. Dystonia Group | Chorea–dystonia Group vs. Dystonia Group | Age | Therapy | |||||
|---|---|---|---|---|---|---|---|---|
| Estimate | p Value | Estimate | p Value | Estimate | p Value | Estimate | p Value | |
| MD_COP | −185.64 | 0.06 | −64.01 | 0.70 | −0.95 | 0.32 | 113.50 | 0.13 |
| MD_AP | −128.53 | 0.04 | −35.97 | 0.74 | −0.27 | 0.64 | 94.56 | 0.07 |
| MD_ML | −243.20 | 0.66 | 10.27 | 0.47 | −0.82 | 0.31 | 174.55 | 0.73 |
| RMS_COP | −246.07 | 0.73 | −9.02 | 0.65 | −1.11 | 0.30 | 156.30 | 0.81 |
| RMS_AP | −156.87 | 0.02 | 11.93 | 0.31 | −0.37 | 0.56 | 114.27 | 0.04 |
| RMS_ML | −322.04 | 0.63 | 19.23 | 0.28 | −1.01 | 0.30 | 232.18 | 0.70 |
| ESC_COP | −10,837.86 | 0.37 | 5549.68 | 0.06 | −66.60 | 0.62 | 9130.21 | 0.37 |
| ESC_AP | −5649.55 | 0.49 | 2479.81 | 0.17 | −47.00 | 0.61 | 5185.01 | 0.46 |
| ESC_ML | −7959.26 | 0.35 | −5361.34 | 0.75 | −33.52 | 0.72 | 6571.05 | 0.36 |
| VEL_COP | −249.00 | 0.34 | −132.86 | 0.80 | −1.15 | 0.69 | 159.26 | 0.46 |
| VEL_AP | −135.91 | 0.04 | 58.68 | <0.01 | −0.92 | 0.16 | 88.34 | 0.08 |
| VEL_ML | −179.70 | 0.28 | −103.75 | 0.75 | −0.41 | 0.82 | 115.30 | 0.40 |
| SWAY | −3886.73 | 0.22 | −1810.83 | 0.77 | −21.49 | 0.52 | 2411.99 | 0.35 |
| FREQ_COP | 2.53 | 0.02 | 0.32 | 0.11 | 0.01 | 0.39 | −1.62 | 0.05 |
| FREQ_AP | 3.62 | 0.10 | 0.20 | 0.61 | 0.01 | 0.97 | −2.78 | 0.13 |
| FREQ_ML | 2.38 | <0.01 | 0.38 | 0.02 | 0.01 | 0.30 | −1.17 | 0.05 |
| Interaction Chorea Group and Age | Interaction Chorea–Dystonia Group and Age | Interaction Chorea Group and Therapy | Interaction Chorea–Dystonia Group and Therapy | Interaction Age and Therapy | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Estimate | p Value | Estimate | p Value | Estimate | p Value | Estimate | p Value | Estimate | p Value | |
| MD_COP | 18.77 | 0.07 | 4.75 | 0.75 | 37.67 | 0.05 | 77.31 | 0.06 | −16.32 | 0.1 |
| MD_AP | 13.44 | 0.05 | 2.72 | 0.77 | 2.38 | 0.06 | 53.47 | 0.05 | −12.85 | 0.06 |
| MD_ML | 25.32 | 0.68 | −1.71 | 0.23 | 37.33 | 0.48 | 93.42 | 0.64 | −23.01 | 0.70 |
| RMS_COP | 25.16 | 0.75 | −0.41 | 0.82 | 46.34 | 0.51 | 102.15 | 0.69 | −22.04 | 0.78 |
| RMS_AP | 16.42 | 0.03 | −1.71 | 0.14 | 28.81 | 0.03 | 69.36 | 0.02 | −15.53 | 0.03 |
| RMS_ML | 33.73 | 0.64 | −2.71 | 0.12 | 47.70 | 0.45 | 122.87 | 0.68 | −30.60 | 0.67 |
| ESC_COP | 1474.87 | 0.27 | −531.97 | 0.05 | 737.91 | 0.75 | 5511.38 | 0.29 | −1261.76 | 0.34 |
| ESC_AP | 746.91 | 0.41 | −257.13 | 0.14 | 943.89 | 0.57 | 3302.50 | 0.36 | −717.16 | 0.43 |
| ESC_ML | 1075.80 | 0.25 | 472.77 | 0.76 | 347.31 | 0.83 | 3410.01 | 0.35 | −903.37 | 0.33 |
| VEL_COP | 27.05 | 0.34 | 11.40 | 0.81 | 47.27 | 0.37 | 89.76 | 0.43 | −22.06 | 0.43 |
| VEL_AP | 14.55 | 0.04 | −5.88 | <0.01 | 22.70 | 0.07 | 58.55 | 0.04 | −12.29 | 0.07 |
| VEL_ML | 19.71 | 0.28 | 9.14 | 0.76 | 29.04 | 0.38 | 59.95 | 0.40 | −15.84 | 0.37 |
| SWAY | 399.97 | 0.24 | 143.63 | 0.79 | 811.98 | 0.20 | 1517.56 | 0.26 | −341.25 | 0.31 |
| FREQ_COP | −0.25 | 0.03 | −0.02 | 0.36 | −0.52 | 0.02 | −1.15 | 0.02 | 0.23 | 0.04 |
| FREQ_AP | −0.38 | 0.11 | −0.01 | 0.74 | −0.65 | 0.14 | −1.73 | 0.08 | 0.38 | 0.11 |
| FREQ_ML | −0.21 | <0.01 | −0.01 | 0.38 | −0.51 | <0.01 | −1.00 | <0.01 | 0.18 | 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menici, V.; Scalise, R.; Fasano, A.; Falotico, E.; Dubbini, N.; Prencipe, G.; Sgandurra, G.; Filogna, S.; Battini, R. Assessment of Postural Control in Children with Movement Disorders by Means of a New Technological Tool: A Pilot Study. Bioengineering 2024, 11, 176. https://doi.org/10.3390/bioengineering11020176
Menici V, Scalise R, Fasano A, Falotico E, Dubbini N, Prencipe G, Sgandurra G, Filogna S, Battini R. Assessment of Postural Control in Children with Movement Disorders by Means of a New Technological Tool: A Pilot Study. Bioengineering. 2024; 11(2):176. https://doi.org/10.3390/bioengineering11020176
Chicago/Turabian StyleMenici, Valentina, Roberta Scalise, Alessio Fasano, Egidio Falotico, Nevio Dubbini, Giuseppe Prencipe, Giuseppina Sgandurra, Silvia Filogna, and Roberta Battini. 2024. "Assessment of Postural Control in Children with Movement Disorders by Means of a New Technological Tool: A Pilot Study" Bioengineering 11, no. 2: 176. https://doi.org/10.3390/bioengineering11020176
APA StyleMenici, V., Scalise, R., Fasano, A., Falotico, E., Dubbini, N., Prencipe, G., Sgandurra, G., Filogna, S., & Battini, R. (2024). Assessment of Postural Control in Children with Movement Disorders by Means of a New Technological Tool: A Pilot Study. Bioengineering, 11(2), 176. https://doi.org/10.3390/bioengineering11020176