


Breath-Holding as a Stimulus to Assess Peripheral Oxygenation Flow Using Near-Infrared Spectroscopic Imaging


Abstract
1. Introduction
1.1. Breath-Hold Stimulus
1.2. Objective
2. Materials and Methods
2.1. Instrumentation
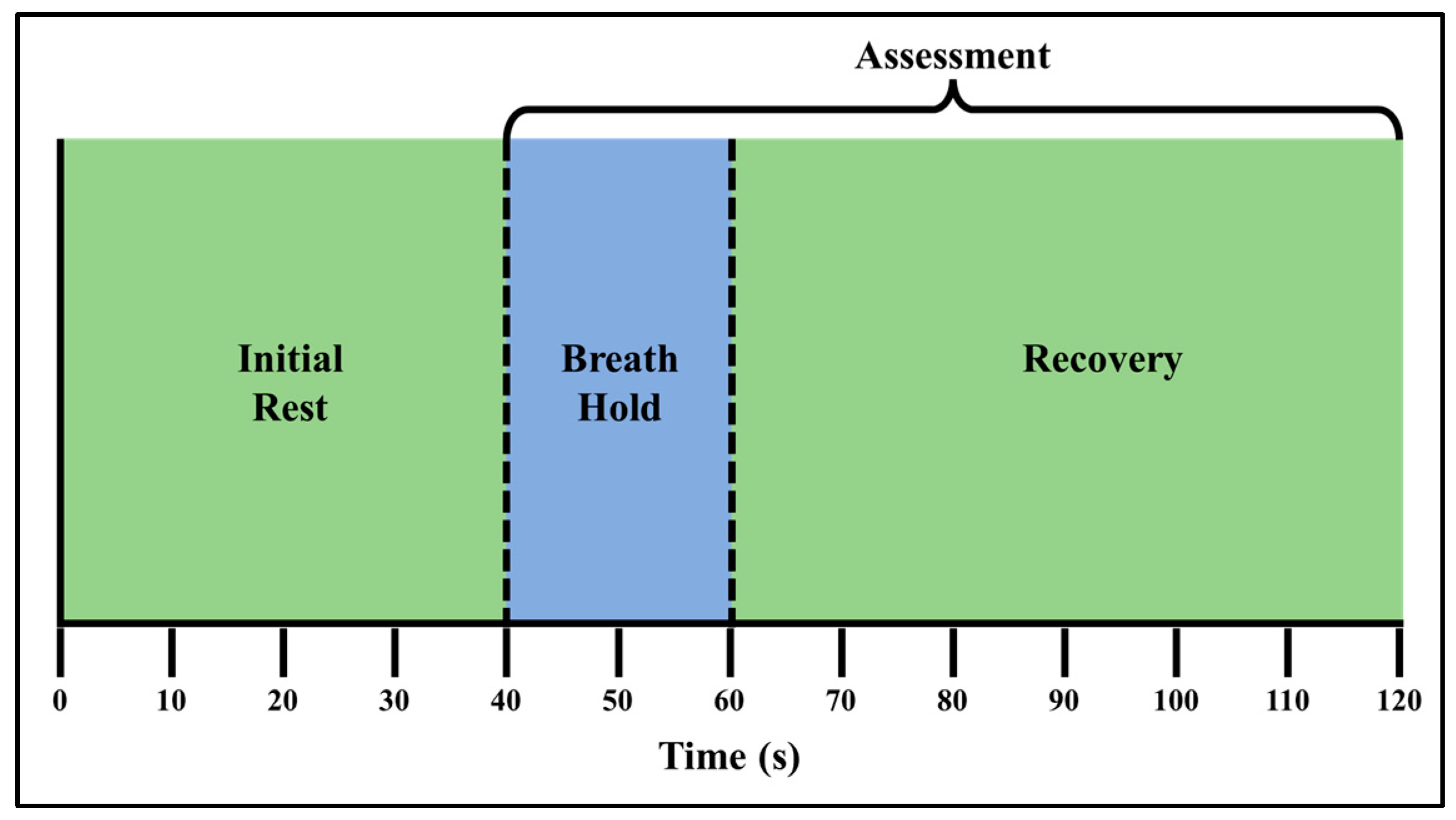
2.2. Subject Recruitment and Experimental Paradigm
2.3. Data Acquisition
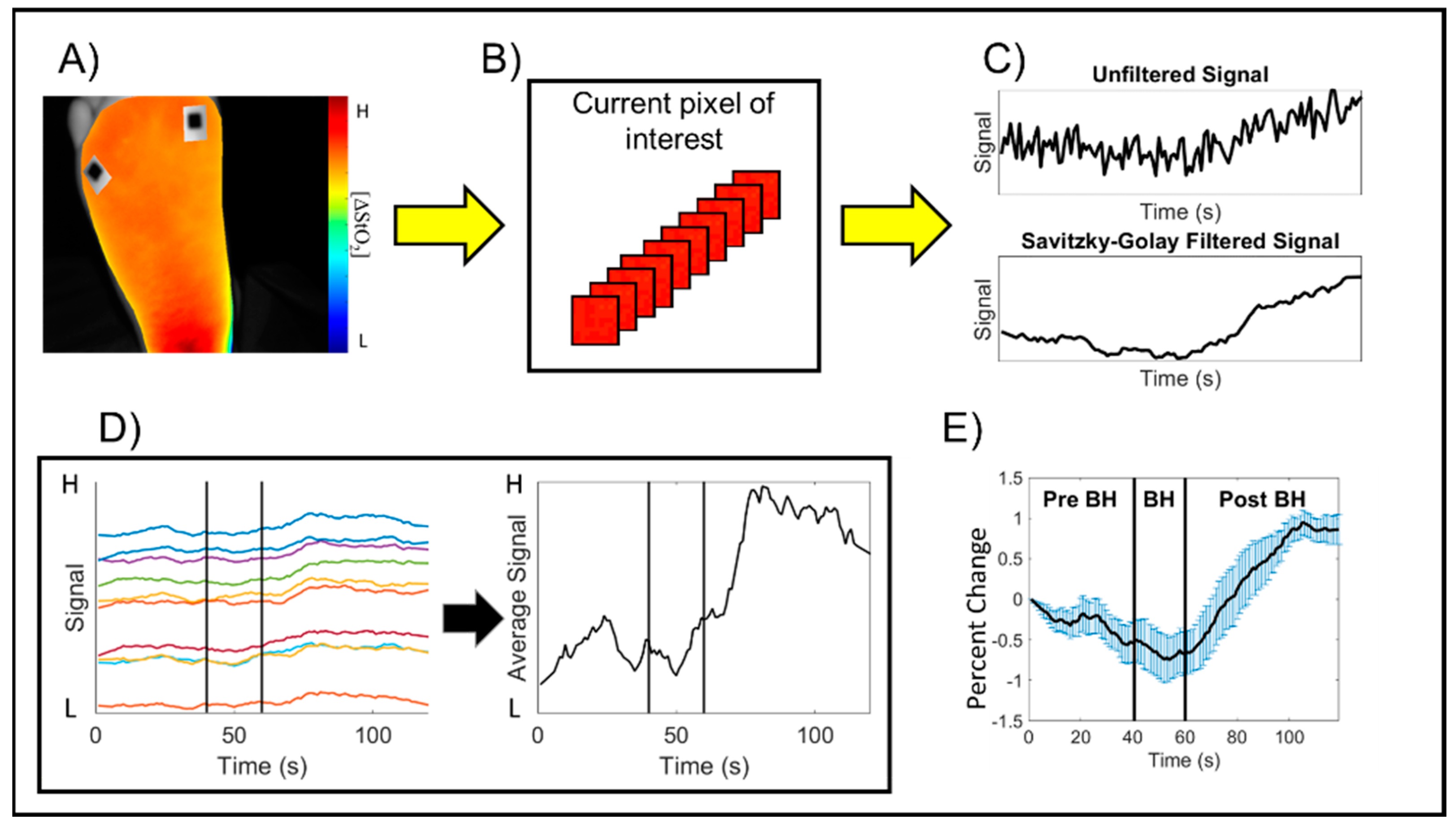
2.4. Image Analysis
3. Results
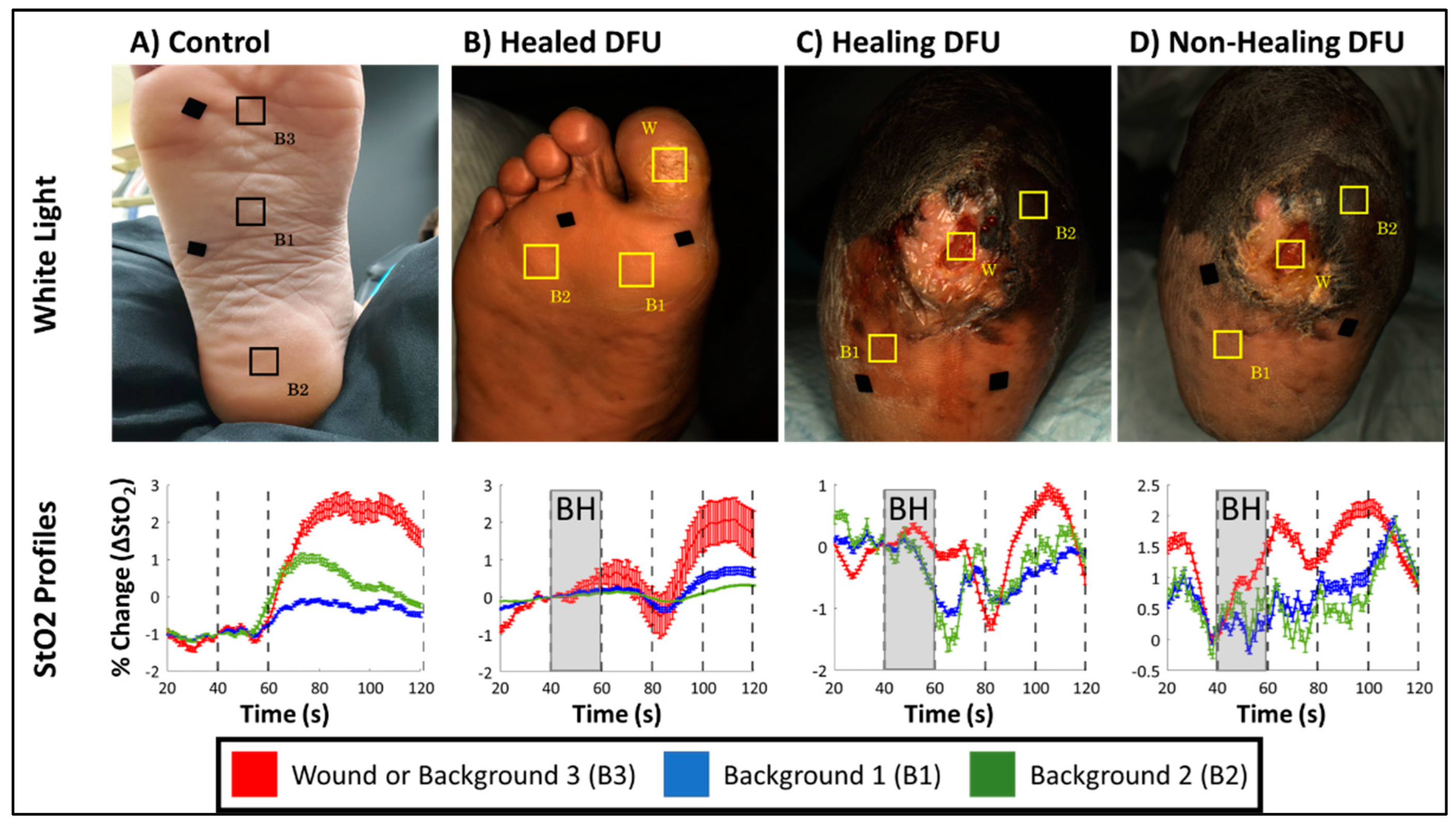
3.1. Time-Varying Hemoglobin Concentration Profiles of Control Subjects
3.2. Time-Varying Hemoglobin Concentration Profiles of DFU Subjects with Differing Skin Colors
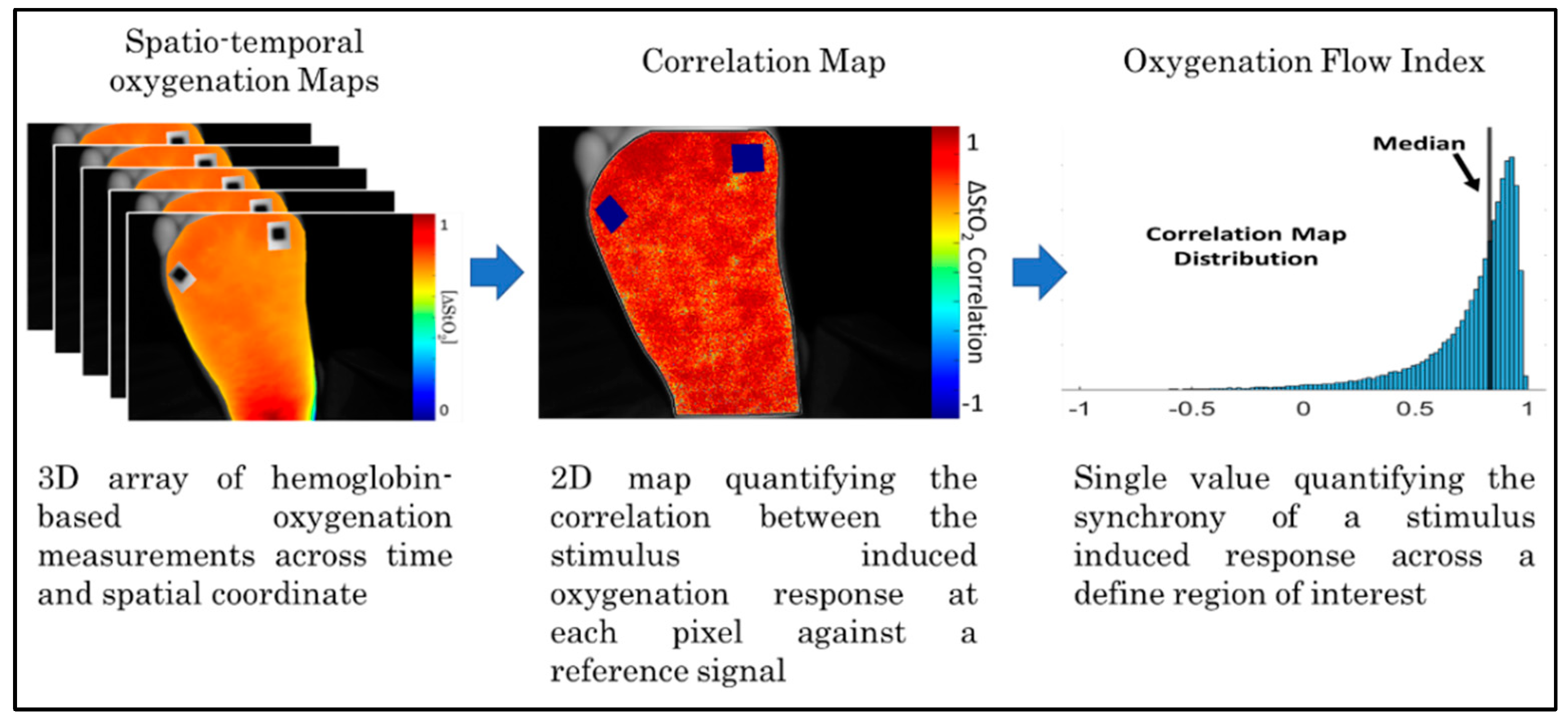
3.3. Flow Correlation Maps in Controls Vs. DFUs
4. Discussion
4.1. Effect of Breath-Holding on Peripheral Oxygenation in Controls
4.2. Hemoglobin Concentration Profiles of DFUs with Varying Skin Colors
4.3. Oxygenated Flow Response Differences Between Controls and DFUs
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Armstrong, D.G.; Boulton, A.J.M.; Bus, S.A. Diabetic Foot Ulcers and Their Recurrence. N. Engl. J. Med. 2017, 376, 2367–2375. [Google Scholar] [CrossRef] [PubMed]
- Everett, E.; Mathioudakis, N. Update on Management of Diabetic Foot Ulcers. Ann. N. Y. Acad. Sci. 2018, 1411, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Schreml, S.; Szeimies, R.M.; Prantl, L.; Karrer, S.; Landthaler, M.; Babilas, P. Oxygen in Acute and Chronic Wound Healing. Br. J. Dermatol. 2010, 163, 257–268. [Google Scholar] [CrossRef] [PubMed]
- Lavery, L.A.; Davis, K.E.; Berriman, S.J.; Braun, L.; Nichols, A.; Kim, P.J.; Margolis, D.; Peters, E.J.; Attinger, C. WHS Guidelines Update: Diabetic Foot Ulcer Treatment Guidelines. Wound Repair Regen. 2016, 24, 112–126. [Google Scholar] [CrossRef]
- Kolarsick, P.A.J.; Kolarsick, M.A.; Goodwin, C. Anatomy and Physiology of the Skin. J. Dermatol. Nurses Assoc. 2011, 3, 203–213. [Google Scholar] [CrossRef]
- Boulant, J.A. Role of the Preoptic-Anterior Hypothalamus in Thermoregulation and Fever. Clin. Infect. Dis. 2000, 31, S157–S161. [Google Scholar] [CrossRef]
- Bromley, I. Transcutaneous Monitoring–Understanding the Principles. Infant 2008, 4, 95–98. [Google Scholar]
- Serena, T.E.; Yaakov, R.; Serena, L.; Mayhugh, T.; Harrell, K. Comparing near Infrared Spectroscopy and Transcutaneous Oxygen Measurement in Hard-to-Heal Wounds: A Pilot Study. J. Wound Care 2020, 29, S4–S9. [Google Scholar] [CrossRef]
- Yudovsky, D.; Nouvong, A.; Schomacker, K.; Pilon, L. Monitoring Temporal Development and Healing of Diabetic Foot Ulceration Using Hyperspectral Imaging. J. Biophotonics 2011, 4, 565–576. [Google Scholar] [CrossRef]
- Khaodhiar, L.; Dinh, T.; Schomacker, K.T.; Panasyuk, S.V.; Freeman, J.E.; Lew, R.; Vo, T.; Panasyuk, A.A.; Lima, C.; Giurini, J.M.; et al. The Use of Medical Hyperspectral Technology to Evaluate Microcirculatory Changes in Diabetic Foot Ulcers and to Predict Clinical Outcomes. Diabetes Care 2007, 30, 903–910. [Google Scholar] [CrossRef]
- Nouvong, A.; Hoogwerf, B.; Mohler, E.; Davis, B.; Tajaddini, A.; Medenilla, E. Evaluation of Diabetic Foot Ulcer Healing With Hyperspectral Imaging of Oxyhemoglobin and Deoxyhemoglobin. Diabetes Care 2009, 32, 2056–2061. [Google Scholar] [CrossRef] [PubMed]
- López-Moral, M.; García-Álvarez, Y.; Molines-Barroso, R.J.; Tardáguila-García, A.; García-Madrid, M.; Lázaro-Martínez, J.L. A Comparison of Hyperspectral Imaging with Routine Vascular Noninvasive Techniques to Assess the Healing Prognosis in Patients with Diabetic Foot Ulcers. J. Vasc. Surg. 2022, 75, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Basiri, A.; Nabili, M.; Mathews, S.; Libin, A.; Groah, S.; Noordmans, H.J.; Ramella-Roman, J.C. Use of a Multi-Spectral Camera in the Characterization of Skin Wounds. Opt. Express 2010, 18, 3244. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Mey, L.; Szymanska, A.F.; Takhar, H.S.; Cuccia, D.J.; Mazhar, A.; Yu, K. SFDI Biomarkers Provide a Quantitative Ulcer Risk Metric and Can Be Used to Predict Diabetic Foot Ulcer Onset. J. Diabetes Complicat. 2020, 34, 107624. [Google Scholar] [CrossRef]
- Jayachandran, M.; Rodriguez, S.; Solis, E.; Lei, J.; Godavarty, A. Critical Review of Noninvasive Optical Technologies for Wound Imaging. Adv. Wound Care 2016, 5, 349–359. [Google Scholar] [CrossRef]
- Papazoglou, E.S.; Neidrauer, M.; Zubkov, L.; Weingarten, M.S.; Pourrezaei, K. Noninvasive Assessment of Diabetic Foot Ulcers with Diffuse Photon Density Wave Methodology: Pilot Human Study. J. Biomed. Opt. 2009, 14, 064032. [Google Scholar] [CrossRef]
- Neidrauer, M.; Zubkov, L.; Weingarten, M.S.; Pourrezaei, K.; Papazoglou, E.S. Near Infrared Wound Monitor Helps Clinical Assessment of Diabetic Foot Ulcers. J. Diabetes Sci. Technol. 2010, 4, 792–798. [Google Scholar] [CrossRef]
- Weingarten, M.S.; Neidrauer, M.; Mateo, A.; Mao, X.; McDaniel, J.E.; Jenkins, L.; Bouraee, S.; Zubkov, L.; Pourrezaei, K.; Papazoglou, E.S. Prediction of Wound Healing in Human Diabetic Foot Ulcers by Diffuse Near-Infrared Spectroscopy: A Pilot Study. Wound Repair Regen. 2010, 18, 180–185. [Google Scholar] [CrossRef]
- Leiva, K.; Mahadevan, J.; Kaile, K.; Schutzman, R.; Robledo, E.; Narayanan, S.; Muthukrishnan, V.; Mohan, V.; Wu, W.; Godavarty, A. Breath-Hold Paradigm to Assess Variations in Oxygen Flow in Diabetic Foot Ulcers Using a Noncontact Near-Infrared Optical Scanner. Adv. Wound Care 2019, 8, 386–402. [Google Scholar] [CrossRef]
- Ratnatunga, C.; Adiseshiah, M. Increase in Middle Cerebral Artery Velocity on Breath Holding: A Simplified Test of Cerebral Perfusion Reserve. Eur. J. Vasc. Surg. 1990, 4, 519–523. [Google Scholar] [CrossRef]
- Liu, H.-L.; Huang, J.-C.; Wu, C.-T.; Hsu, Y.-Y. Detectability of Blood Oxygenation Level-Dependent Signal Changes during Short Breath Hold Duration. Magn. Reson. Imaging 2002, 20, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Bain, A.R.; Drvis, I.; Dujic, Z.; MacLeod, D.B.; Ainslie, P.N. Physiology of Static Breath Holding in Elite Apneists. Exp. Physiol. 2018, 103, 635–651. [Google Scholar] [CrossRef] [PubMed]
- Andersson, J.; Schagatay, E. Undersea & Hyperbaric Medicine. Undersea Hyperb. Med. 1998, 25, 21–25. [Google Scholar] [PubMed]
- Bouten, J.; Bourgois, J.G.; Boone, J. Hold Your Breath: Peripheral and Cerebral Oxygenation during Dry Static Apnea. Eur. J. Appl. Physiol. 2020, 120, 2213–2222. [Google Scholar] [CrossRef]
- Fitzpatrick, T.B. The Validity and Practicality of Sun-Reactive Skin Types I Through VI. Arch. Dermatol. 1988, 124, 869. [Google Scholar] [CrossRef]
- Gussakovsky, E.; Jilkina, O.; Yang, Y.; Kupriyanov, V. Hemoglobin plus Myoglobin Concentrations and near Infrared Light Pathlength in Phantom and Pig Hearts Determined by Diffuse Reflectance Spectroscopy. Anal. Biochem. 2008, 382, 107–115. [Google Scholar] [CrossRef]
- Yudovsky, D.; Nouvong, A.; Schomacker, K.; Pilon, L. Assessing Diabetic Foot Ulcer Development Risk with Hyperspectral Tissue Oximetry. J. Biomed. Opt. 2011, 16, 026009. [Google Scholar] [CrossRef]
- Press, W.H.; Teukolsky, S.A. Savitzky-Golay Smoothing Filters. Comput. Phys. 1990, 4, 669–672. [Google Scholar] [CrossRef]
- Schafer, R. What Is a Savitzky-Golay Filter? [Lecture Notes]. IEEE Signal Process Mag. 2011, 28, 111–117. [Google Scholar] [CrossRef]
- Grunovas, A.; Trinkunas, E. Cardiovascular Response to Breath-Holding Explained by Changes of the Indices and Their Dynamic Interactions. Biol. Syst. Open Access 2015, 5, 152. [Google Scholar] [CrossRef]
- Leiva, K.; Trinidad, A.; Gonzalez, I.; Espinoza, A.; Zwick, T.; Levine, J.; Rodriguez, M.; Lev-Tov, H.; Kirsner, R.; Godavarty, A. Comparison of Oxygenated Flow Patterns in Diabetic Foot Ulcers Subjects and Controls in Response to Breath-Holding. In Optical Biopsy XX: Toward Real-Time Spectroscopic Imaging and Diagnosis; Alfano, R.R., Demos, S.G., Seddon, A.B., Eds.; SPIE: Bellingham, DC, USA, 2022; Volume 1195407. [Google Scholar] [CrossRef]
- Longobardi, P.; Hartwig, V.; Santarella, L.; Hoxha, K.; Campos, J.; Laurino, M.; Salvo, P.; Trivella, M.G.; Coceani, F.; Rocco, M.; et al. Potential Markers of Healing from near Infrared Spectroscopy Imaging of Venous Leg Ulcer. A Randomized Controlled Clinical Trial Comparing Conventional with Hyperbaric Oxygen Treatment. Wound Repair Regen. 2020, 28, 856–866. [Google Scholar] [CrossRef] [PubMed]
- Leiva, K.; Trinidad, A.; Gonzalez, I.; Espinosa, A.; Zwick, T.; Levine, J.E.; Rodriguez, M.A.; Lev-Tov, H.; Wu, W.; Kirsner, R.S.; et al. Development of a Tissue Oxygenation Flow-Based Index Toward Discerning the Healing Status in Diabetic Foot Ulcers. Adv. Wound Care 2024, 13, 22–33. [Google Scholar] [CrossRef] [PubMed]
- MacIntosh, B.J.; Klassen, L.M.; Menon, R.S. Transient Hemodynamics during a Breath Hold Challenge in a Two Part Functional Imaging Study with Simultaneous Near-Infrared Spectroscopy in Adult Humans. Neuroimage 2003, 20, 1246–1252. [Google Scholar] [CrossRef] [PubMed]
- DuBose, L.E.; Weng, T.B.; Pierce, G.L.; Wharff, C.; Reist, L.; Hamilton, C.; O’Deen, A.; Dubishar, K.; Lane-Cordova, A.; Voss, M.W. Association between Cardiorespiratory Fitness and Cerebrovascular Reactivity to a Breath-Hold Stimulus in Older Adults: Influence of Aerobic Exercise Training. J. Appl. Physiol. 2022, 132, 1468–1479. [Google Scholar] [CrossRef]
- Koep, J.L.; Barker, A.R.; Banks, R.; Banger, R.R.; Sansum, K.M.; Weston, M.E.; Bond, B. The Reliability of a Breath-hold Protocol to Determine Cerebrovascular Reactivity in Adolescents. J. Clin. Ultrasound 2020, 48, 544–552. [Google Scholar] [CrossRef]
- Ferretti, G. Extreme Human Breath-Hold Diving. Eur. J. Appl. Physiol. 2001, 84, 254–271. [Google Scholar] [CrossRef]
- Ferretti, G.; Costa, M. Diversity in and Adaptation to Breath-Hold Diving in Humans. Comp. Biochem. Physiol. A Mol. Integr. Physiol. 2003, 136, 205–213. [Google Scholar] [CrossRef]
- Keil, V.C.; Eichhorn, L.; Mutsaerts, H.J.M.M.; Träber, F.; Block, W.; Mädler, B.; van de Ven, K.; Siero, J.C.W.; MacIntosh, B.J.; Petr, J.; et al. Cerebrovascular Reactivity during Prolonged Breath-Hold in Experienced Freedivers. Am. J. Neuroradiol. 2018, 39, 1839–1847. [Google Scholar] [CrossRef]
- Palada, I.; Obad, A.; Bakovic, D.; Valic, Z.; Ivancev, V.; Dujic, Z. Cerebral and Peripheral Hemodynamics and Oxygenation during Maximal Dry Breath-Holds. Respir. Physiol. Neurobiol. 2007, 157, 374–381. [Google Scholar] [CrossRef]
- Bolton, B.; Carmichael, E.A.; Stürup, G. Vaso-constriction Following Deep Inspiration. J. Physiol. 1936, 86, 83–94. [Google Scholar] [CrossRef]
- Khoo, M.C.K.; Chalacheva, P. Respiratory Modulation of Peripheral Vasoconstriction: A Modeling Perspective. J. Appl. Physiol. 2019, 127, 1177–1186. [Google Scholar] [CrossRef] [PubMed]
- Roustit, M.; Loader, J.; Baltzis, D.; Zhao, W.; Veves, A. Microvascular Changes in the Diabetic Foot. In The Diabetic Foot. Contemporary Diabetes; Veves, A., Giurini, J., Guzman, R., Eds.; Humana: Cham, Switzerland, 2018; pp. 173–188. [Google Scholar] [CrossRef]
- Forsythe, R.O.; Brownrigg, J.; Hinchliffe, R.J. Peripheral Arterial Disease and Revascularization of the Diabetic Foot. Diabetes Obes. Metab. 2015, 17, 435–444. [Google Scholar] [CrossRef] [PubMed]
- Stirban, A. Microvascular Dysfunction in the Context of Diabetic Neuropathy. Curr. Diab Rep. 2014, 14, 541. [Google Scholar] [CrossRef] [PubMed]
- Kachlik, D.; Pechacek, V.; Baca, V.; Musil, V. The Superficial Venous System of the Lower Extremity: New Nomenclature. Phlebol. J. Venous Dis. 2010, 25, 113–123. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | DFU Subject | Status | Side | Week of Treatment | DFU Location | Fitzpatrick Grade |
|---|---|---|---|---|---|---|
| 1 | 1 | Healed | Right | 4 | Big Toe (Plantar) | 1 |
| 2 | 2 | Healing | Left | 1 | Midfoot (Post Transmetatarsal amputation) | 2 (Proximal) 5 (Distal) |
| 3 | 2 | Non-Healing | Left | 6 | Midfoot (Post Transmetatarsal amputation) | 2 (Proximal) 5 (Distal) |
| DFU Subject | Region | Pearson Correlation Coefficient |
|---|---|---|
| Control (Subject 1) | B1 vs. B2 | 95.42% |
| B1 vs. B3 | 95.2% | |
| B2 vs. B3 | 85.5% | |
| 1 (Healed DFU) | B1 vs. B2 | 93.9% |
| W vs. B1 | 95.5% | |
| W vs. B2 | 84.0% | |
| 2 (Week 1—Healing DFU) | B1 vs. B2 | 92.8% |
| W vs. B1 * | 26.1% | |
| W vs. B2 * | 31.5% | |
| 2 (Week 6—Non-Healing DFU) | B1 vs. B2 | 84.8% |
| W vs. B1 * | 57.2% | |
| W vs. B2 * | 34.3% |
| Controls | Dorsum OFI | Sole OFI |
|---|---|---|
| 1 | 36.6 ± 5.5% | 60.2 ± 25.0% |
| 2 | 45.0 ± 12.1% | 59.6 ± 20.5% |
| 3 | 45.0 ± 19.7% | 72.2 ± 22.0% |
| Grand Average | 42.2 ± 12.6% | 64.0 ± 20.5% |
| DFUs | OFI |
|---|---|
| Healed | 33.4% |
| Healing | 68.4% |
| Non-healing | 9.5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leiva, K.; Gonzalez, I.; Murillo, J.; Espinosa, A.; Kirsner, R.S.; Godavarty, A. Breath-Holding as a Stimulus to Assess Peripheral Oxygenation Flow Using Near-Infrared Spectroscopic Imaging. Bioengineering 2024, 11, 1221. https://doi.org/10.3390/bioengineering11121221
Leiva K, Gonzalez I, Murillo J, Espinosa A, Kirsner RS, Godavarty A. Breath-Holding as a Stimulus to Assess Peripheral Oxygenation Flow Using Near-Infrared Spectroscopic Imaging. Bioengineering. 2024; 11(12):1221. https://doi.org/10.3390/bioengineering11121221
Chicago/Turabian StyleLeiva, Kevin, Isabella Gonzalez, Juan Murillo, Aliette Espinosa, Robert S. Kirsner, and Anuradha Godavarty. 2024. "Breath-Holding as a Stimulus to Assess Peripheral Oxygenation Flow Using Near-Infrared Spectroscopic Imaging" Bioengineering 11, no. 12: 1221. https://doi.org/10.3390/bioengineering11121221
APA StyleLeiva, K., Gonzalez, I., Murillo, J., Espinosa, A., Kirsner, R. S., & Godavarty, A. (2024). Breath-Holding as a Stimulus to Assess Peripheral Oxygenation Flow Using Near-Infrared Spectroscopic Imaging. Bioengineering, 11(12), 1221. https://doi.org/10.3390/bioengineering11121221