
Wearable Online Freezing of Gait Detection and Cueing System


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Materials
2.1.1. Vibrational Stimulation Actuators
2.1.2. Real-Time Gait Analysis Module
2.2. Methods
- machine learning algorithm,
- implementation of the ML algorithm in an online environment, and
- the dataset recording protocol.
2.2.1. Machine Learning Algorithm
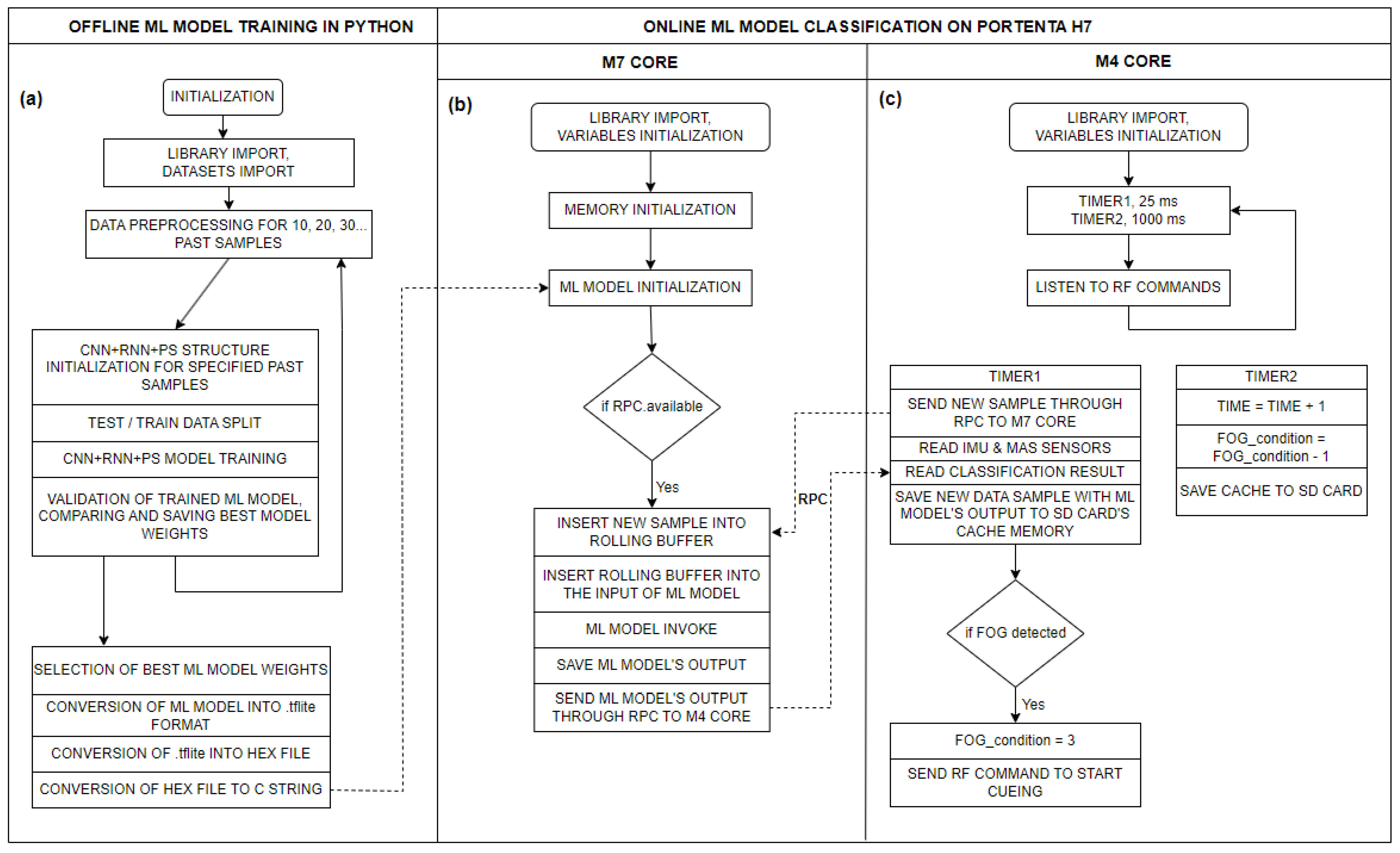
2.2.2. Implementation of the ML Algorithm in an Online Environment
2.2.3. Participants and the Dataset Recording Protocol
3. Results
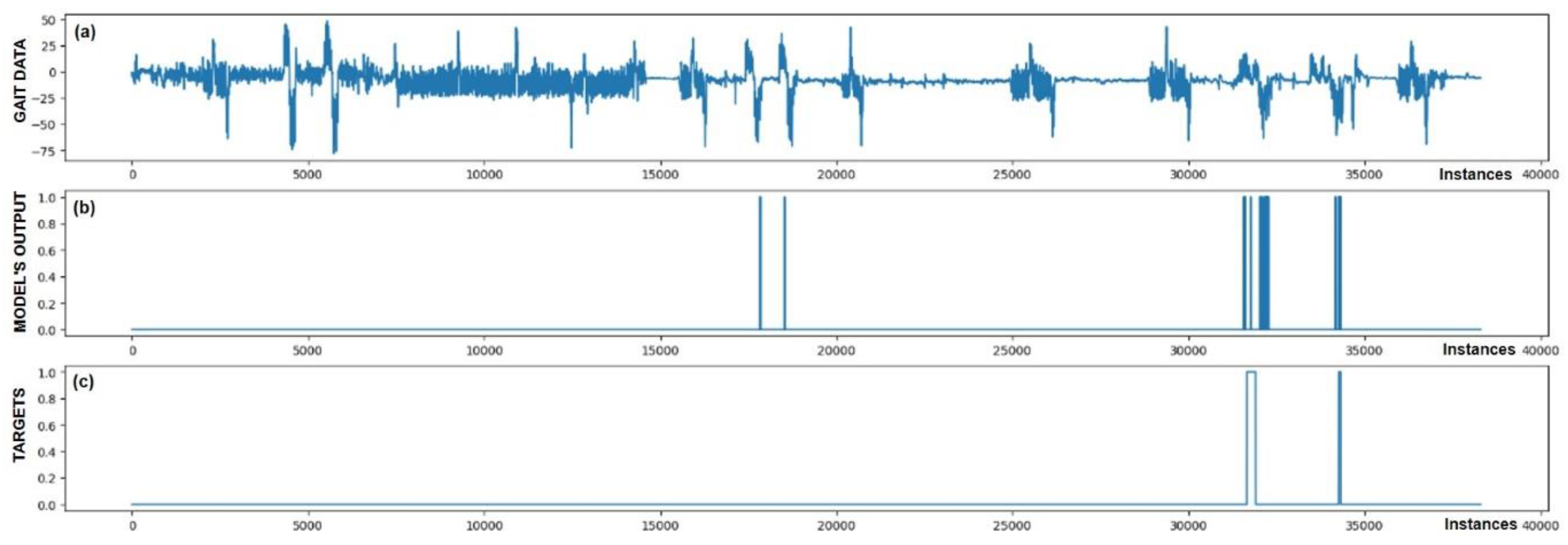
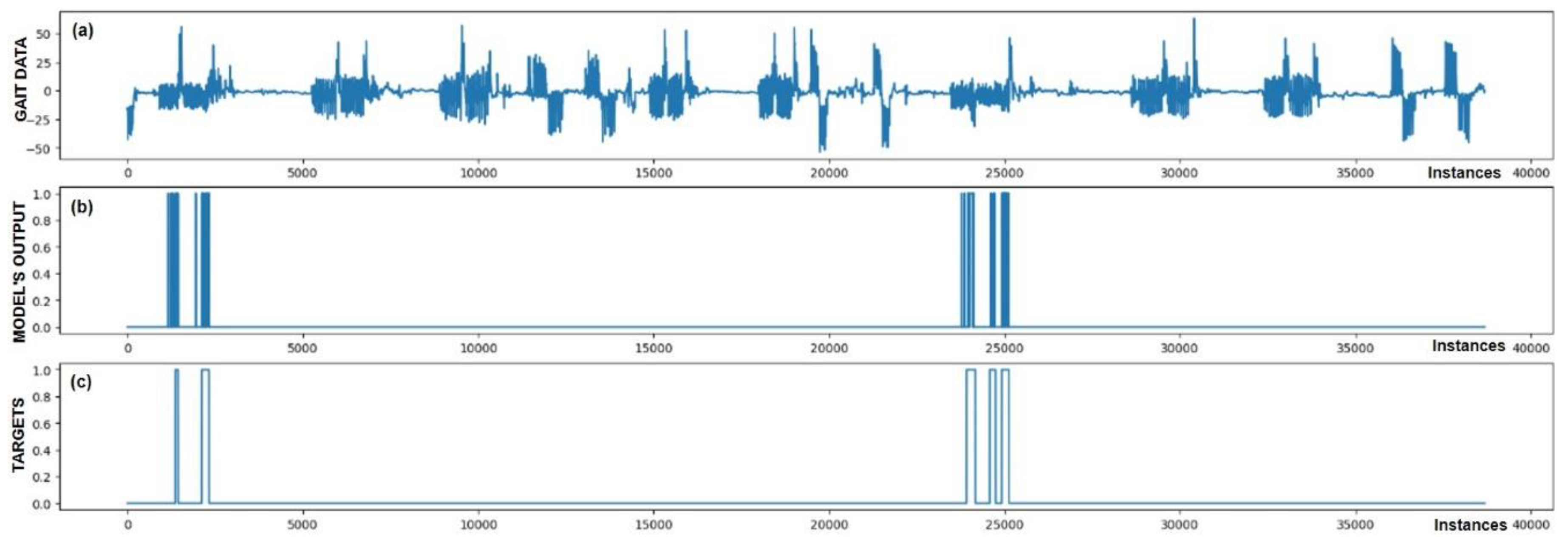
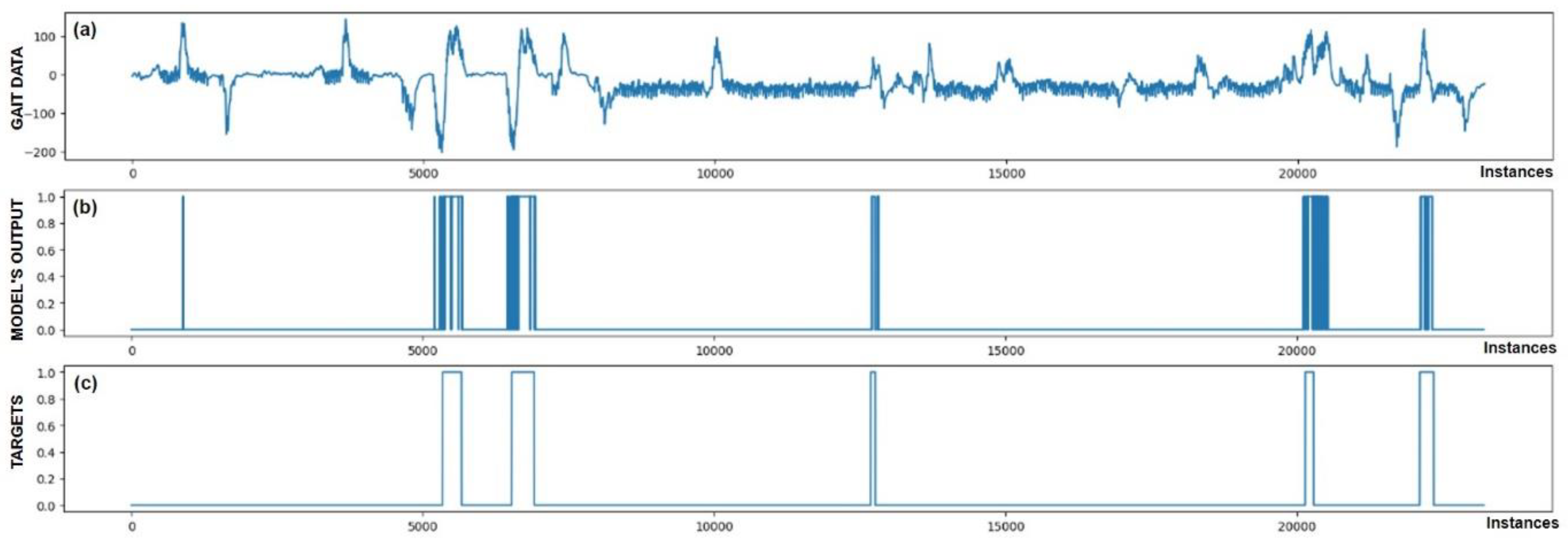
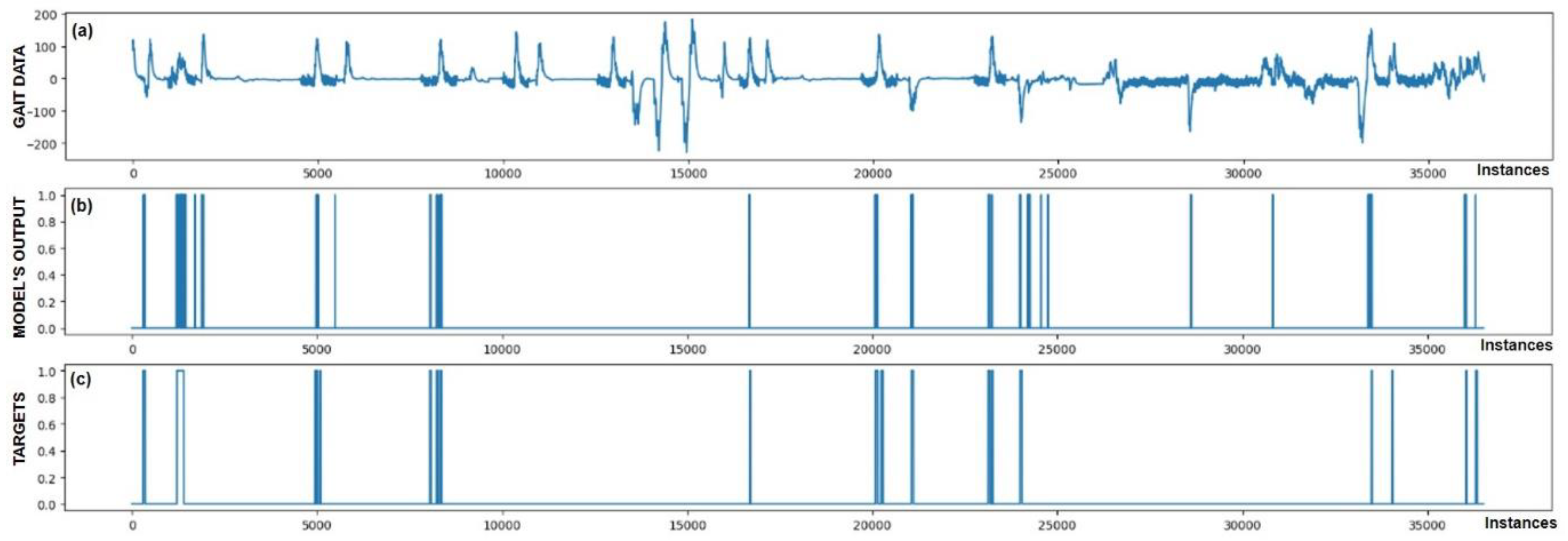
3.1. Offline Detection of Freezing of Gait Episodes
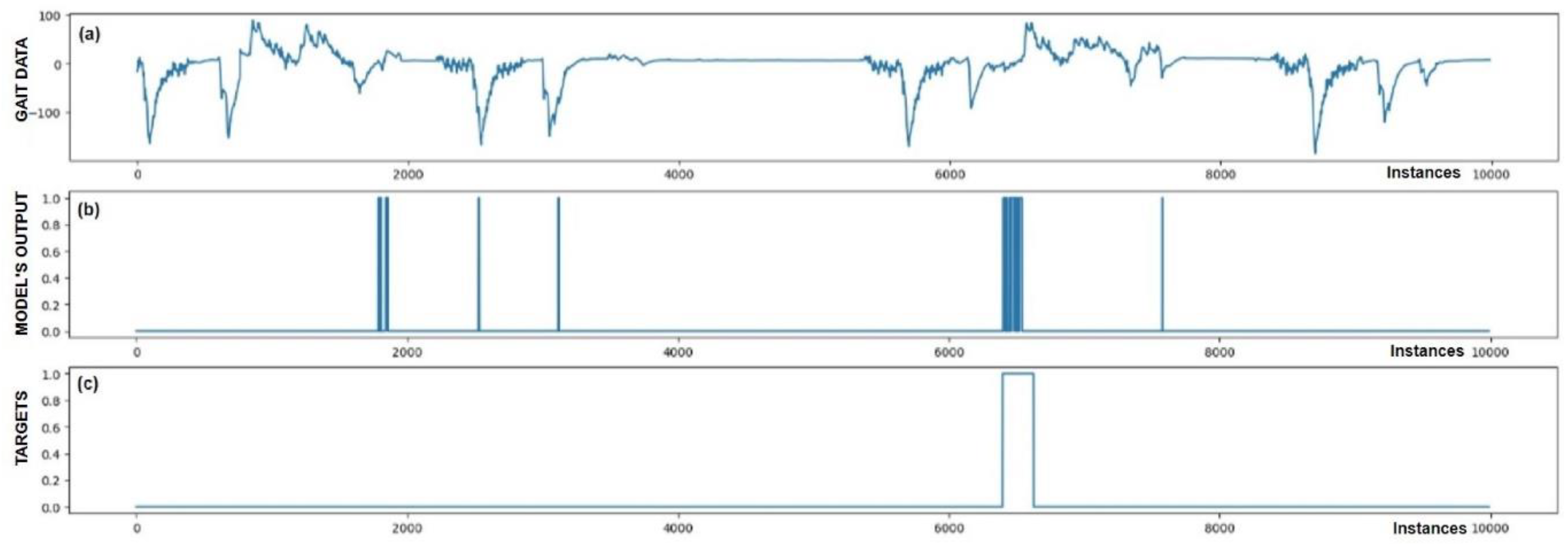
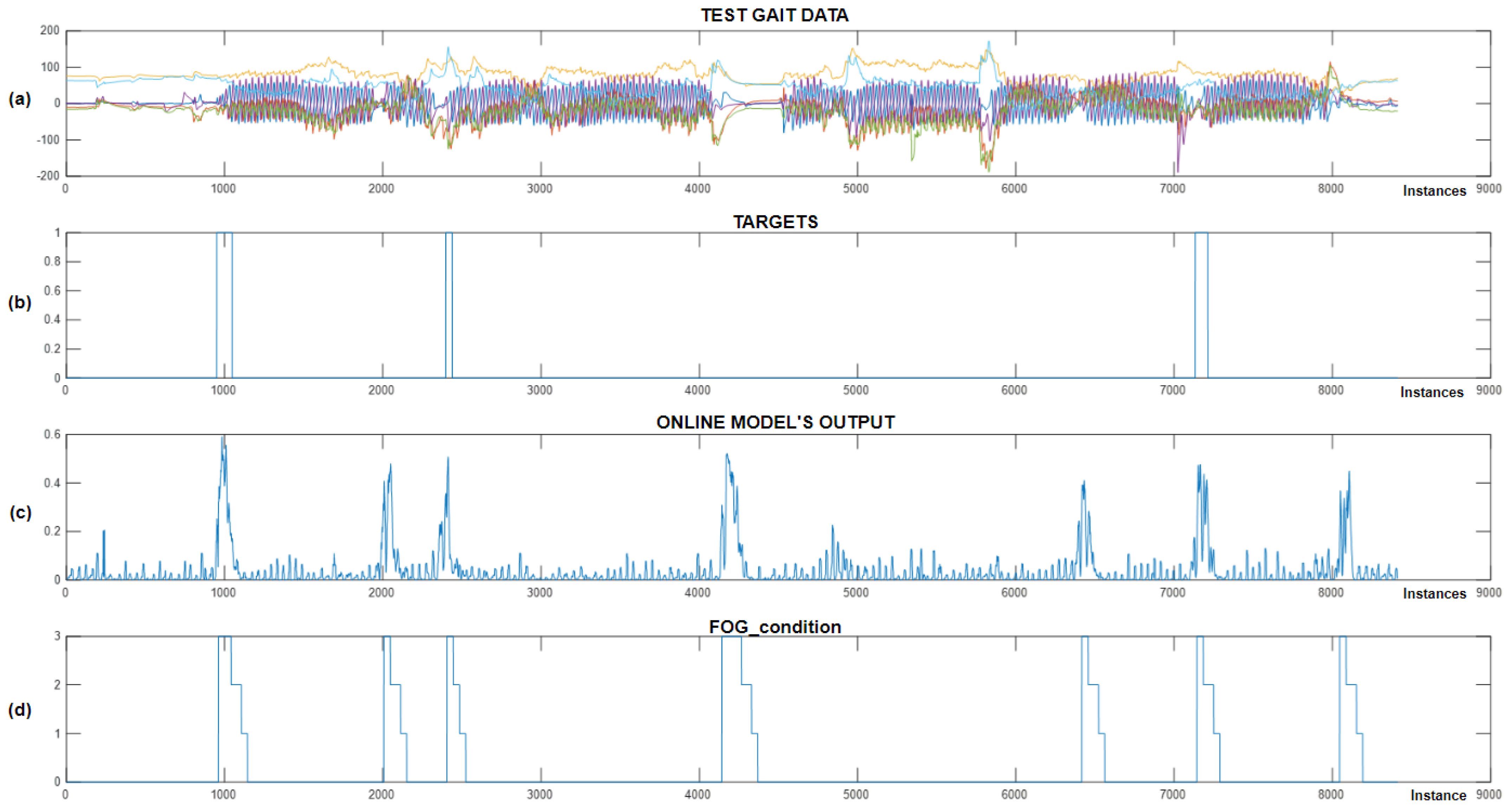
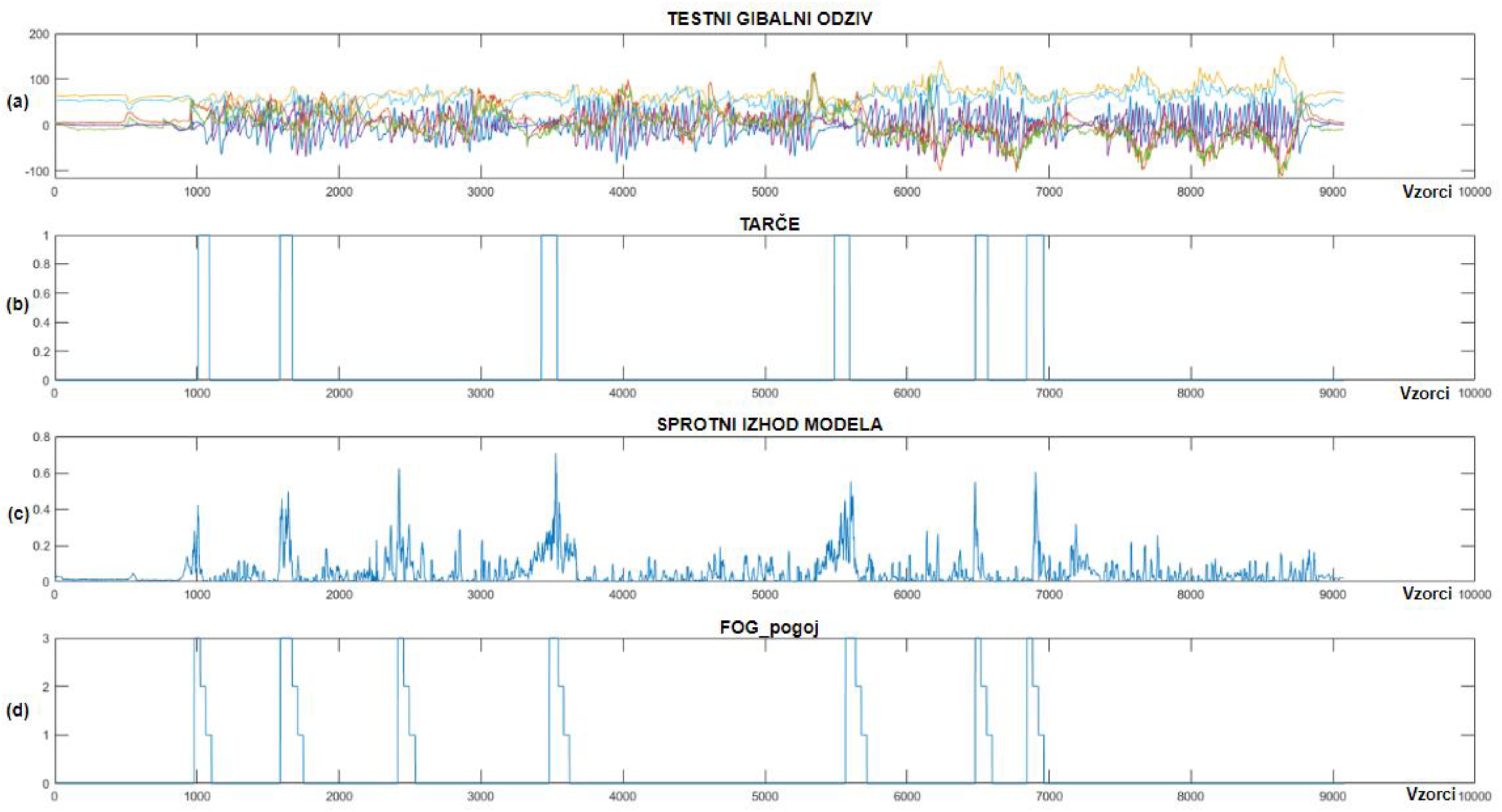
3.2. Online Detection of Simulated Freezing of Gait Episodes
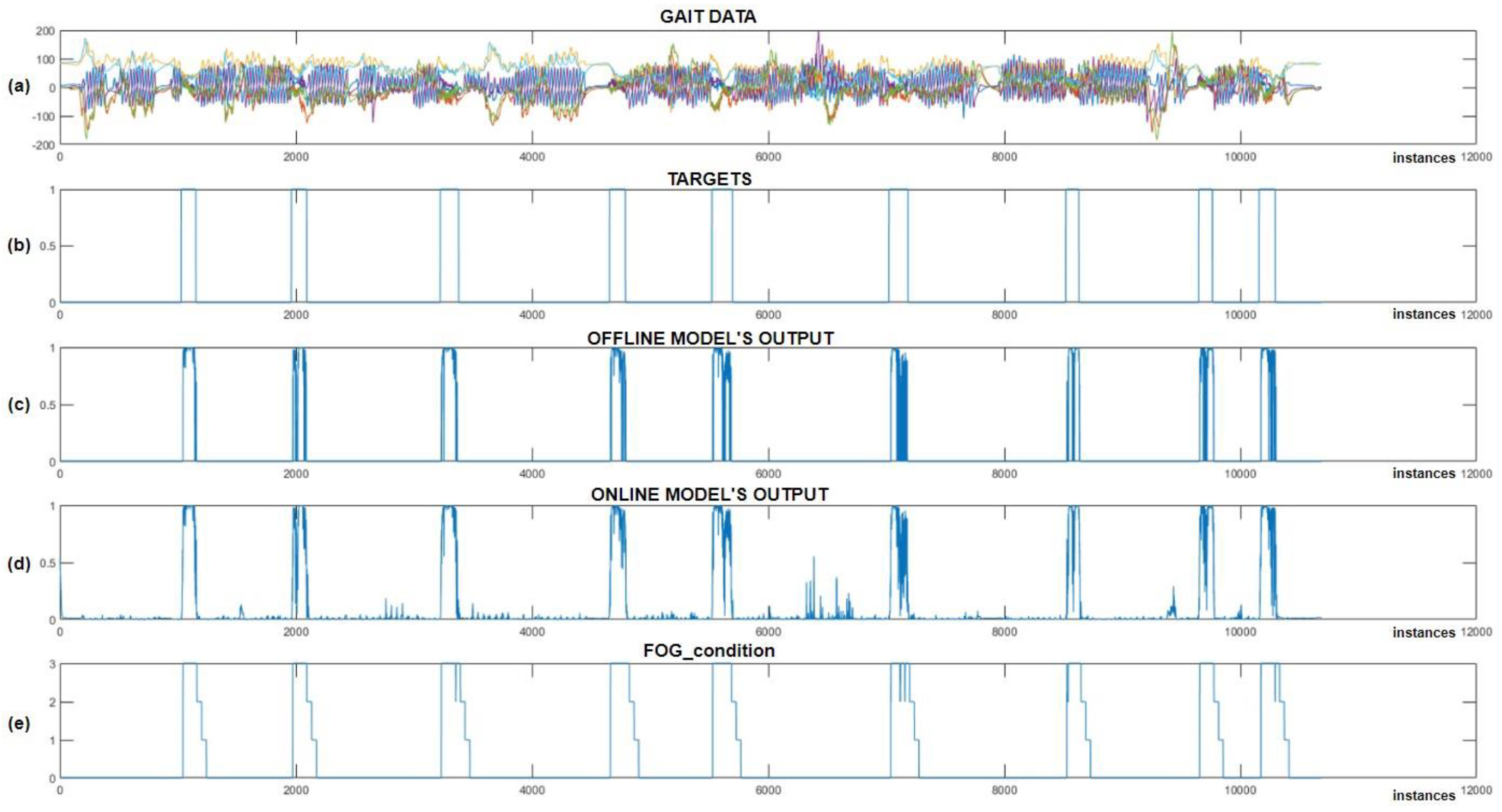
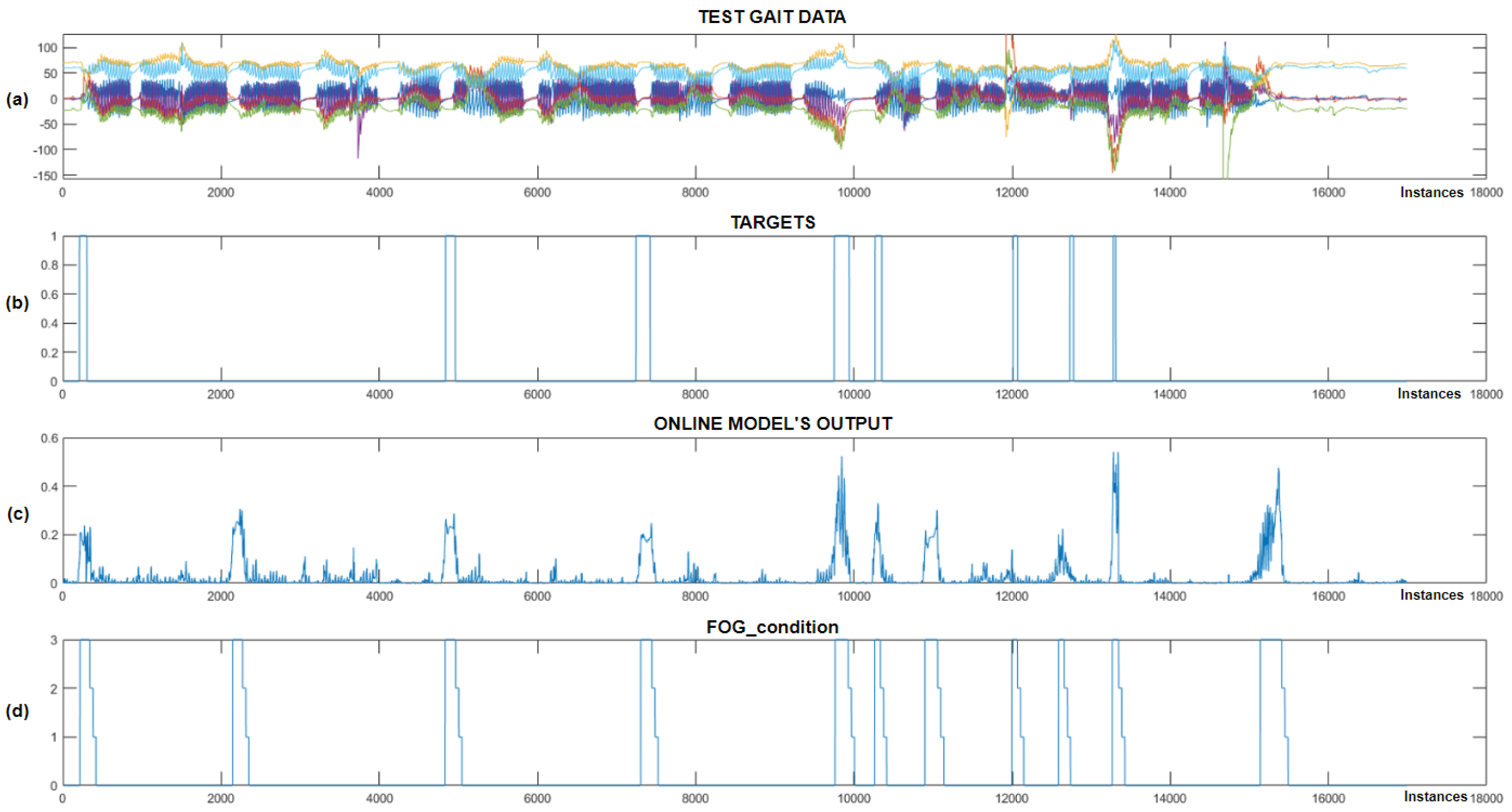
3.3. Online Detection of Freezing of Gait Episodes
3.4. Preliminary Statistical Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Giladi, N.; Nieuwboer, A. Understanding and treating freezing of gait in parkinsonism, proposed working definition, and setting the stage. Mov. Disord. 2008, 23 (Suppl. S2), S423–S425. [Google Scholar] [CrossRef] [PubMed]
- Nutt, J.G.; Bloem, B.R.; Giladi, N.; Hallett, M.; Horak, F.B.; Nieuwboer, A. Freezing of gait: Moving forward on a mysterious clinical phenomenon. Lancet Neurol. 2011, 10, 734–744. [Google Scholar] [CrossRef] [PubMed]
- Tysnes, O.B.; Storstein, A. Epidemiology of Parkinson’s disease. J. Neural. Transm. 2017, 124, 901–905. [Google Scholar] [CrossRef] [PubMed]
- Ben-Shlomo, Y.; Darweesh, S.; Llibre-Guerra, J.; Marras, C.; San Luciano, M.; Tanner, C. The epidemiology of Parkinson’s disease. Lancet 2024, 403, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Dietz, V.; Leenders, K.L.; Colombo, G. Leg muscle activation during gait in Parkinson’s disease: Influence of body unloading. Electroencephalogr. Clin. Neurophysiol. 1997, 105, 400–405. [Google Scholar] [CrossRef]
- Jankovic, J. Atomoxetine for freezing of gait in Parkinson disease. J. Neurol. Sci. 2009, 284, 177–178. [Google Scholar] [CrossRef]
- Giladi, N.; McMahon, D.; Przedborski, S.; Flaster, E.; Guillory, S.; Kostic, V.; Fahn, S. Motor blocks in Parkinson’s disease. Neurology 1992, 42, 333–339. [Google Scholar] [CrossRef]
- Schaafsma, J.D.; Balash, Y.; Gurevich, T.; Bartels, A.L.; Hausdorff, J.M.; Giladi, N. Characterization of freezing of gait subtypes and the response of each to levodopa in Parkinson’s disease. Eur. J. Neurol. 2003, 10, 391–398. [Google Scholar] [CrossRef]
- Bonanno, M.; De Nunzio, A.M.; Quartarone, A.; Militi, A.; Petralito, F.; Calabrò, R.S. Gait Analysis in Neurorehabilitation: From Research to Clinical Practice. Bioengineering 2023, 10, 785. [Google Scholar] [CrossRef]
- Marimon, X.; Mengual, I.; Lopez-de-Celis, C.; Portela, A.; Rodriguez-Sanz, J.; Herraez, I.A.; Perez-Bellmunt, A. Kinematic Analysis of Human Gait in Healthy Young Adults Using IMU Sensors: Exploring Relevant Machine Learning Features for Clinical Applications. Bioengineering 2024, 11, 105. [Google Scholar] [CrossRef]
- Huang, D.; Wu, C.; Wang, Y.; Zhang, Z.; Chen, C.; Li, L.; Zhang, W.; Zhang, Z.; Li, J.; Guo, Y.; et al. Episode-level prediction of freezing of gait based on wearable inertial signals using a deep neural network model. Biomed. Signal Process. Control 2024, 88, 105613. [Google Scholar] [CrossRef]
- Benson, L.C.; Clermont, C.A.; Bošnjak, E.; Ferber, R. The use of wearable devices for walking and running gait analysis outside of the lab: A systematic review. Gait Posture 2018, 63, 124–138. [Google Scholar] [CrossRef] [PubMed]
- Ion, C.; Henri, G.C. Low Cost Sensor-based Gait Monitoring System. In Proceedings of the IEEE 15th International Conference on Electronics, Computers and Artificial Intelligence, Bucharest, Romania, 29–30 June 2023. [Google Scholar] [CrossRef]
- Huang, T.; Li, M.; Huang, J. Recent trends in wearable device used to detect freezing of gait and falls in people with Parkinson’s disease: A systematic review. Front. Aging Neurosci. 2023, 15, 1119956. [Google Scholar] [CrossRef] [PubMed]
- Takeda, R.; Tadano, S.; Natorigawa, A.; Todoh, M.; Yoshinari, S. Gait posture estimation using wearable acceleration and gyro sensors. J. Biomech. 2009, 42, 2486–2494. [Google Scholar] [CrossRef]
- Prado, A.; Kwei, S.K.; Vanegas-Arroyave, N.; Agrawal, S.K. Continuous Identification of Freezing of Gait in Parkinson’s Patients Using Artificial Neural Networks and Instrumented Shoes. IEEE Trans. Med. Robot. Bionics 2021, 3, 554–562. [Google Scholar] [CrossRef]
- Slemensek, J.; Fister, I.; Gersak, J.; Bratina, B.; van Midden, V.M.; Pirtosek, Z.; Safaric, R. Human Gait Activity Recognition Machine Learning Methods. Sensors 2023, 23, 745. [Google Scholar] [CrossRef]
- Zhang, W.; Sun, H.; Huang, D.; Zhang, Z.; Li, J.; Wu, C.; Sun, Y.; Gong, M.; Wang, Z.; Sun, C.; et al. Detection and prediction of freezing of gait with wearable sensors in Parkinson’s disease. Neurol. Sci. 2023, 45, 431–453. [Google Scholar] [CrossRef]
- Prado, A.; Cao, X.; Robert, M.T.; Gordon, A.M.; Agrawal, S.K. Gait Segmentation of Data Collected by Instrumented Shoes Using a Recurrent Neural Network Classifier. Phys. Med. Rehabil. Clin. N. Am. 2019, 30, 355–366. [Google Scholar] [CrossRef]
- Mo, L.F.; Zeng, L.J. Running gait pattern recognition based on cross-correlation analysis of single acceleration sensor. Math. Biosci. Eng. 2019, 16, 6242–6256. [Google Scholar] [CrossRef]
- Dvorani, A.; Waldheim, V.; Jochner, M.C.E.; Salchow-Hommen, C.; Meyer-Ohle, J.; Kuhn, A.A.; Wenger, N.; Schauer, T. Real-Time Detection of Freezing Motions in Parkinson’s Patients for Adaptive Gait Phase Synchronous Cueing. Front. Neurol. 2021, 12, 720516. [Google Scholar] [CrossRef]
- Marcante, A.; Di Marco, R.; Gentile, G.; Pellicano, C.; Assogna, F.; Pontieri, F.E.; Spalletta, G.; Macchiusi, L.; Gatsios, D.; Giannakis, A.; et al. Foot Pressure Wearable Sensors for Freezing of Gait Detection in Parkinson’s Disease. Sensors 2020, 21, 128. [Google Scholar] [CrossRef] [PubMed]
- Borzi, L.; Mazzetta, I.; Zampogna, A.; Suppa, A.; Olmo, G.; Irrera, F. Prediction of Freezing of Gait in Parkinson’s Disease Using Wearables and Machine Learning. Sensors 2021, 21, 614. [Google Scholar] [CrossRef]
- Aich, S.; Pradhan, P.M.; Park, J.; Sethi, N.; Vathsa, V.S.S.; Kim, H.C. A Validation Study of Freezing of Gait (FoG) Detection and Machine-Learning-Based FoG Prediction Using Estimated Gait Characteristics with a Wearable Accelerometer. Sensors 2018, 18, 3287. [Google Scholar] [CrossRef] [PubMed]
- Camps, J.; Samà, A.; Martín, M.; Rodríguez-Martín, D.; Pérez-López, C.; Moreno Arostegui, J.M.; Cabestany, J.; Català, A.; Alcaine, S.; Mestre, B.; et al. Deep learning for freezing of gait detection in Parkinson’s disease patients in their homes using a waist-worn inertial measurement unit. Knowl.-Based Syst. 2018, 139, 119–131. [Google Scholar] [CrossRef]
- Pierleoni, P.; Belli, A.; Bazgir, O.; Maurizi, L.; Paniccia, M.; Palma, L. A Smart Inertial System for 24h Monitoring and Classification of Tremor and Freezing of Gait in Parkinson’s Disease. IEEE Sens. J. 2019, 19, 11612–11623. [Google Scholar] [CrossRef]
- Ren, K.; Chen, Z.; Ling, Y.; Zhao, J. Recognition of freezing of gait in Parkinson’s disease based on combined wearable sensors. BMC Neurol. 2022, 22, 229. [Google Scholar] [CrossRef]
- Bachlin, M.; Plotnik, M.; Roggen, D.; Maidan, I.; Hausdorff, J.M.; Giladi, N.; Troster, G. Wearable assistant for Parkinson’s disease patients with the freezing of gait symptom. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 436–446. [Google Scholar] [CrossRef]
- Kita, A.; Lorenzi, P.; Rao, R.; Irrera, F. Reliable and Robust Detection of Freezing of Gait Episodes With Wearable Electronic Devices. IEEE Sens. J. 2017, 17, 1899–1908. [Google Scholar] [CrossRef]
- Mazzetta, I.; Zampogna, A.; Suppa, A.; Gumiero, A.; Pessione, M.; Irrera, F. Wearable Sensors System for an Improved Analysis of Freezing of Gait in Parkinson’s Disease Using Electromyography and Inertial Signals. Sensors 2019, 19, 948. [Google Scholar] [CrossRef]
- Rodriguez-Martin, D.; Perez-Lopez, C.; Sama, A.; Catala, A.; Moreno Arostegui, J.M.; Cabestany, J.; Mestre, B.; Alcaine, S.; Prats, A.; Cruz Crespo, M.; et al. A Waist-Worn Inertial Measurement Unit for Long-Term Monitoring of Parkinson’s Disease Patients. Sensors 2017, 17, 827. [Google Scholar] [CrossRef]
- Suppa, A.; Kita, A.; Leodori, G.; Zampogna, A.; Nicolini, E.; Lorenzi, P.; Rao, R.; Irrera, F. l-DOPA and Freezing of Gait in Parkinson’s Disease: Objective Assessment through a Wearable Wireless System. Front. Neurol. 2017, 8, 406. [Google Scholar] [CrossRef] [PubMed]
- Jahangir, F.; Khan, M.A.; Alhaisoni, M.; Alqahtani, A.; Alsubai, S.; Sha, M.; Al Hejaili, A.; Cha, J.H. A Fusion-Assisted Multi-Stream Deep Learning and ESO-Controlled Newton-Raphson-Based Feature Selection Approach for Human Gait Recognition. Sensors 2023, 23, 2754. [Google Scholar] [CrossRef] [PubMed]
- Ginis, P.; Nackaerts, E.; Nieuwboer, A.; Heremans, E. Cueing for people with Parkinson’s disease with freezing of gait: A narrative review of the state-of-the-art and novel perspectives. Ann. Phys. Rehabil. Med. 2018, 61, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Hammerla, N.Y.; Halloran, S.; Ploetz, T. Deep, Convolutional, and Recurrent Models for Human Activity Recognition using Wearables. arXiv 2016. [Google Scholar] [CrossRef]
- Bohan, S.; Shih, C.Y.; Tay, A. Convolutional Neural Network for Freezing of Gait Detection Leveraging the Continuous Wavelet Transform on Lower Extremities Wearable Sensors Data. In Proceedings of the 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020. [Google Scholar] [CrossRef]
- Spaulding, S.J.; Barber, B.; Colby, M.; Cormack, B.; Mick, T.; Jenkins, M.E. Cueing and gait improvement among people with Parkinson’s disease: A meta-analysis. Arch. Phys. Med. Rehabil. 2013, 94, 562–570. [Google Scholar] [CrossRef]
- Young, W. AmbuloSonus: Wearable Auditory Cueing for Gait Improvement in Parkinson’s Disease. J. NeuroEng. Rehabil. 2016, 43, 50–55. [Google Scholar]
- Bartolo, M.; Castelli, A.; Calabrese, M.; Buttacchio, G.; Zucchella, C.; Tamburin, S.; Fontana, A.; Copetti, M.; Fasano, A.; Intiso, D. A wearable system for visual cueing gait rehabilitation in Parkinson’s disease: A randomized non-inferiority trial. Eur. J. Phys. Rehabil. Med. 2024, 60, 245–256. [Google Scholar] [CrossRef]
- Rocha, P.A.; Porfirio, G.M.; Ferraz, H.B.; Trevisani, V.F. Effects of external cues on gait parameters of Parkinson’s disease patients: A systematic review. Clin. Neurol. Neurosurg. 2014, 124, 127–134. [Google Scholar] [CrossRef]
- Caldas, R.; Mundt, M.; Potthast, W.; Buarque de Lima Neto, F.; Markert, B. A systematic review of gait analysis methods based on inertial sensors and adaptive algorithms. Gait Posture 2017, 57, 204–210. [Google Scholar] [CrossRef]
- Arias, P.; Cudeiro, J. Effect of rhythmic auditory stimulation on gait in Parkinsonian patients with and without freezing of gait. PLoS ONE 2010, 5, e9675. [Google Scholar] [CrossRef]
- Behari, M.; Aggarwal, R.; Pretzer-Aboff, I.; Winfree, K.; Agrawal, S. Clinical outcomes of step-synchronized vibration training in patients of Parkinson’s disease with freezing of gait. Ann. Mov. Disord. 2019, 2, 15–20. [Google Scholar] [CrossRef]
- Delval, A.; Moreau, C.; Bleuse, S.; Tard, C.; Ryckewaert, G.; Devos, D.; Defebvre, L. Auditory cueing of gait initiation in Parkinson’s disease patients with freezing of gait. Clin. Neurophysiol. 2014, 125, 1675–1681. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Chu, H.; Zhang, Y.; Wang, X. Deep Brain Stimulation to Alleviate Freezing of Gait and Cognitive Dysfunction in Parkinson’s Disease: Update on Current Research and Future Perspectives. Front. Neurosci. 2018, 12, 29. [Google Scholar] [CrossRef] [PubMed]
- Donovan, S.; Lim, C.; Diaz, N.; Browner, N.; Rose, P.; Sudarsky, L.R.; Tarsy, D.; Fahn, S.; Simon, D.K. Laserlight cues for gait freezing in Parkinson’s disease: An open-label study. Park. Relat. Disord. 2011, 17, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Brigham, L.K. The influence of Visual Cueing on Freezing of Gait Among Individuals with Parkinson’s Disease. Master’s Thesis, The University of Western Ontario, London, ON, Canada, 2014. Available online: https://ir.lib.uwo.ca/etd/2016 (accessed on 23 September 2024).
- Lee, A.; Hellmers, N.; Vo, M.; Wang, F.; Popa, P.; Barkan, S.; Patel, D.; Campbell, C.; Henchcliffe, C.; Sarva, H. Can google glass technology improve freezing of gait in parkinsonism? A pilot study. Disabil. Rehabil. Assist. Technol. 2023, 18, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Bachlin, M.; Plotnik, M.; Roggen, D.; Giladi, N.; Hausdorff, J.M.; Troster, G. A wearable system to assist walking of Parkinson s disease patients. Methods Inf. Med. 2010, 49, 88–95. [Google Scholar] [CrossRef]
- Punin, C.; Barzallo, B.; Clotet, R.; Bermeo, A.; Bravo, M.; Bermeo, J.P.; Llumiguano, C. A Non-Invasive Medical Device for Parkinson’s Patients with Episodes of Freezing of Gait. Sensors 2019, 19, 737. [Google Scholar] [CrossRef]
- Rossi, S.; Lisini Baldi, T.; Aggravi, M.; Ulivelli, M.; Cioncoloni, D.; Niccolini, V.; Donati, L.; Prattichizzo, D. Wearable haptic anklets for gait and freezing improvement in Parkinson’s disease: A proof-of-concept study. Neurol. Sci. 2020, 41, 3643–3651. [Google Scholar] [CrossRef]
- Bowman, T.; Pergolini, A.; Carrozza, M.C.; Lencioni, T.; Marzegan, A.; Meloni, M.; Vitiello, N.; Crea, S.; Cattaneo, D. Wearable biofeedback device to assess gait features and improve gait pattern in people with parkinson’s disease: A case series. J. Neuroeng. Rehabil. 2024, 21, 110. [Google Scholar] [CrossRef]
- Samotus, O. Exploring the Effects of Spinal Cord Stimulation for Freezing of Gait in Parkinsonian Patients. Ph.D. Thesis, The University of Western Ontario, London, ON, Canada, 2022. Available online: https://ir.lib.uwo.ca/etd/8377 (accessed on 23 September 2024).
- Sijobert, B.; Azevedo, C.; Andreu, D.; Verna, C.; Geny, C. Effects of Sensitive Electrical Stimulation-Based Somatosensory Cueing in Parkinson’s Disease Gait and Freezing of Gait Assessment. Artif. Organs 2017, 41, E222–E232. [Google Scholar] [CrossRef]
- Patel, M. A Technology for Prediction and Prevention of Freezing of Gait (FOG) in Individuals with Parkinson Disease. In Proceedings of the 16th IFIP Conference on Human-Computer Interaction (INTERACT), Mumbai, India, 25–29 September 2017. [Google Scholar] [CrossRef]
- Mancini, M.; Bloem, B.R.; Horak, F.B.; Lewis, S.J.G.; Nieuwboer, A.; Nonnekes, J. Clinical and methodological challenges for assessing freezing of gait: Future perspectives. Mov. Disord. 2019, 34, 783–790. [Google Scholar] [CrossRef] [PubMed]
- Pardoel, S.; Kofman, J.; Nantel, J.; Lemaire, E.D. Wearable-Sensor-based Detection and Prediction of Freezing of Gait in Parkinson’s Disease: A Review. Sensors 2019, 19, 5141. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.; Watson, A.; Zhou, G. Wearable computing of Freezing of Gait in Parkinson’s disease: A survey. Smart Health 2020, 18, 100143. [Google Scholar] [CrossRef]
- Sweeney, D.; Quinlan, L.R.; Browne, P.; Richardson, M.; Meskell, P.; ÓLaighin, G. A Technological Review of Wearable Cueing Devices Addressing Freezing of Gait in Parkinson’s Disease. Sensors 2019, 19, 1277. [Google Scholar] [CrossRef] [PubMed]
- Mohd-Yasin, F.; Nagel, D.J.; Korman, C.E. Noise in MEMS. Meas. Sci. Technol. 2010, 21, 012001. [Google Scholar] [CrossRef]
- Narkhede, P.; Poddar, S.; Walambe, R.; Ghinea, G.; Kotecha, K. Cascaded Complementary Filter Architecture for Sensor Fusion in Attitude Estimation. Sensors 2021, 21, 1937. [Google Scholar] [CrossRef]
- Kubat, M. An Introduction to Machine Learning. Elsevier Scopus 2017. [Google Scholar] [CrossRef]
- Kiranyaz, S.; Avci, O.; Abdeljaber, O.; Ince, T.; Gabbouj, M.; Inman, D.J. 1D convolutional neural networks and applications: A survey. Mech. Syst. Signal Process. 2021, 151, 107398. [Google Scholar] [CrossRef]
- Ordóñez, F.J.; Roggen, D. Deep convolutional and LSTM recurrent neural networks for multimodal wearable activity recognition. Sensors 2016, 1, 115. [Google Scholar] [CrossRef]
- Su, B.; Smith, C.; Gutierrez Farewik, E. Gait Phase Recognition Using Deep Convolutional Neural Network with Inertial Measurement Units. Biosensors 2020, 10, 109. [Google Scholar] [CrossRef]
- Tajbakhsh, N.; Shin, J.Y.; Gurudu, S.R.; Hurst, R.T.; Kendall, C.B.; Gotway, M.B.; Jianming, L. Convolutional Neural Networks for Medical Image Analysis: Full Training or Fine Tuning? IEEE Trans. Med. Imaging 2016, 35, 1299–1312. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; He, J.; Zhang, L. Attention-Based Convolutional Neural Network for Weakly Labeled Human Activities’ Recognition With Wearable Sensors. IEEE Sens. J. 2019, 19, 7598–7604. [Google Scholar] [CrossRef]
- Yang, J.N.M.; San, P. Deep Convolutional Neural Networks on Multichannel Time Series for Human Activity Recognition. Conf. Artif. Intell. 2015. Available online: https://www.ijcai.org/Proceedings/15/Papers/561.pdf (accessed on 23 September 2024).
- Albahra, S.; Gorbett, T.; Robertson, S.; D’Aleo, G.; Kumar, S.V.S.; Ockunzzi, S.; Lallo, D.; Hu, B.; Rashidi, H.H. Artificial intelligence and machine learning overview in pathology & laboratory medicine: A general review of data preprocessing and basic supervised concepts. Semin. Diagn. Pathol. 2023, 40, 71–87. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, T. Hyperparameter Optimization in Machine Learning: Make Your Machine Learning and Deep Learning Models More Efficient; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar] [CrossRef]
- Kaur, H.; Pannu, H.S.; Malhi, A.K. A Systematic Review on Imbalanced Data Challenges in Machine Learning. ACM Comput. Surv. 2019, 52, 1–36. [Google Scholar] [CrossRef]
- Hossin, M.; Sulaiman, M.N. A Review on Evaluation Metrics for Data Classification Evaluations. Int. J. Data Min. Knowl. Manag. Process 2015, 5, 1–11. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PD Patients | Distribution [%] | Data Characteristics | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Subject | UPDRS | Hoehn and Yahr | Gender | Medicine? | Age | FoG | Other | Num. FoG | Num. Samples |
| 1 | 71 | 3 | M | Yes | 90 | 4.7 | 95.3 | 54.030 | |
| 2 | 49 | 3 | F | Yes | 75 | 1.5 | 98.5 | 8 | 97.227 |
| 3 | 44 | 2 | M | Yes | 70 | 1.9 | 98.1 | 10 | 99.175 |
| 4 | 57 | 3 | M | Yes | 81 | 8.6 | 91.4 | 16 | 58.620 |
| 5 | 44 | 2 | M | Yes | 56 | 7.6 | 92.4 | 86 | 92.987 |
| 6 | 29 | 3 | F | Yes | 59 | 3.0 | 97.0 | 6 | 25.313 |
| 7 | 62 | 3 | M | Yes | 73 | 6.2 | 93.8 | 7 | 9.480 |
| 8 | 49 | 3 | F | Yes | 51 | 4.8 | 95.2 | 4 | 12.309 |
| 9 | 47 | 3 | M | Yes | 52 | 15.4 | 84.6 | 13 | 14.055 |
| Average | 67 | 5.9 | 94.1 | 17 | 51.466 | ||||
| Raw Dataset | CWT Dataset | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Person | Accuracy | Precision | Sensitivity | Specificity | F1 | Num. PS | Accuracy | Precision | Sensitivity | Specificity | F1 |
| 1 | 0.941 | 0.010 | 0.006 | 0.951 | 0.016 | 30 | 0.960 | 0.009 | 0.030 | 0.969 | 0.014 |
| 2 | 0.986 | 0.008 | 0.005 | 0.994 | 0.007 | 60 | 0.987 | 0.008 | 0.005 | 0.995 | 0.006 |
| 3 | 0.959 | 0.024 | 0.018 | 0.982 | 0.020 | 15 | 0.953 | 0.023 | 0.024 | 0.976 | 0.024 |
| 4 | 0.913 | 0.050 | 0.067 | 0.934 | 0.057 | 30 | 0.884 | 0.050 | 0.072 | 0.928 | 0.059 |
| 5 | 0.947 | 0.024 | 0.031 | 0.971 | 0.026 | 40 | 0.949 | 0.023 | 0.027 | 0.972 | 0.026 |
| 6 | 0.958 | 0.023 | 0.022 | 0.980 | 0.021 | 30 | 0.969 | 0.024 | 0.007 | 0.992 | 0.011 |
| Mean | 0.951 | 0.023 | 0.024 | 0.968 | 0.024 | 34 | 0.950 | 0.022 | 0.027 | 0.972 | 0.023 |
| Sensor Combination | Accuracy | Precision | Sensitivity | Specificity | F1 |
|---|---|---|---|---|---|
| CF | 0.910 | 0.051 | 0.057 | 0.943 | 0.053 |
| ACC | 0.911 | 0.050 | 0.062 | 0.937 | 0.056 |
| GYRO | 0.914 | 0.050 | 0.056 | 0.942 | 0.052 |
| MA | 0.912 | 0.051 | 0.057 | 0.943 | 0.054 |
| ACC, GYRO | 0.914 | 0.050 | 0.063 | 0.938 | 0.056 |
| ACC, CF | 0.915 | 0.050 | 0.059 | 0.940 | 0.054 |
| ACC, MA | 0.915 | 0.051 | 0.051 | 0.949 | 0.050 |
| GYRO, CF | 0.914 | 0.050 | 0.057 | 0.943 | 0.054 |
| GYRO, MA | 0.912 | 0.050 | 0.056 | 0.943 | 0.053 |
| CF, MA | 0.911 | 0.050 | 0.057 | 0.943 | 0.054 |
| CF, MA, GYRO | 0.913 | 0.050 | 0.063 | 0.937 | 0.056 |
| CF, MA, ACC | 0.912 | 0.050 | 0.064 | 0.936 | 0.056 |
| MA, ACC, GYRO | 0.912 | 0.050 | 0.065 | 0.935 | 0.057 |
| CF, ACC, GYRO | 0.913 | 0.050 | 0.069 | 0.931 | 0.058 |
| CF, ACC, GYRO, MA | 0.912 | 0.050 | 0.067 | 0.934 | 0.057 |
| PD Patient | Vibratory Stimulation | Total Samples | FoG Samples | FoG Probability | FoG Reduction | Z-Value | p-Value |
|---|---|---|---|---|---|---|---|
| 7 | With Without | 9480 16,991 | 586 720 | 0.0618 0.0424 | 32% | −6.47 | |
| 8 | With Without | 12,309 8412 | 562 217 | 0.0457 0.0258 | 44% | −7.63 | |
| 9 | With Without | 14,055 9077 | 2168 593 | 0.1542 0.0653 | 58% | −22.18 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Slemenšek, J.; Geršak, J.; Bratina, B.; van Midden, V.M.; Pirtošek, Z.; Šafarič, R. Wearable Online Freezing of Gait Detection and Cueing System. Bioengineering 2024, 11, 1048. https://doi.org/10.3390/bioengineering11101048
Slemenšek J, Geršak J, Bratina B, van Midden VM, Pirtošek Z, Šafarič R. Wearable Online Freezing of Gait Detection and Cueing System. Bioengineering. 2024; 11(10):1048. https://doi.org/10.3390/bioengineering11101048
Chicago/Turabian StyleSlemenšek, Jan, Jelka Geršak, Božidar Bratina, Vesna Marija van Midden, Zvezdan Pirtošek, and Riko Šafarič. 2024. "Wearable Online Freezing of Gait Detection and Cueing System" Bioengineering 11, no. 10: 1048. https://doi.org/10.3390/bioengineering11101048
APA StyleSlemenšek, J., Geršak, J., Bratina, B., van Midden, V. M., Pirtošek, Z., & Šafarič, R. (2024). Wearable Online Freezing of Gait Detection and Cueing System. Bioengineering, 11(10), 1048. https://doi.org/10.3390/bioengineering11101048