
Validation of an Automated Optical Scanner for a Comprehensive Anthropometric Analysis of the Foot and Ankle


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
- -
- The first metatarsal and fifth metatarsal ground support points (“toe 1 inside”, “toe 5 outside”, “Toe 1 Med to Pternion”, and “Toe 5 Lat to Pternion”) had, overall, the highest variances for length and width measurements, with a variance percentage ranging from 2% to 4%. During the data acquisition, the load appeared to be evenly distributed on the two feet, thanks to a platform that supported the contralateral foot at the same height as the foot undergoing the examination. The slightly higher variance could have resulted from asymmetric weight distribution applied by the subject on both feet.
- -
- The set of malleolar height points (“sphyrion”, “sphyrion fibulare”, “medial malleolus”, and “lateral malleolus”) also showed higher variance percentages, ranging from 1% to 8%. A possible explanation for a higher variance percentage is that the bony prominences of the malleolar points mentioned above appear more salient when scanned from the back. On the other hand, when they are scanned from the front, the transition between the proximal and distal areas of the anterior aspect of the foot shows a more arcuate shape, with a gentle slope, causing detection issues for the scanner, related to a mismatch of the measurements from the front and the back.
- -
- The measurements of the circumference had the highest variances compared to length, width, and height, but they also had the highest absolute values. The variance percentage reached 2.3% for those measurements with absolute values greater than 250 mm. The less reproducible circumference measurement was “long heel”; we suppose that the rotation of the leg in the scanner could have slightly affected the angle measurements at points of anatomical continuity between the foot and ankle, the so-called “junction points”. On the other hand, the reproducibility of circumferences outside the junction points was excellent, with a mean absolute error of around 1 mm.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kouchi, M.; Mochimaru, M.; Tsuzuki, K.; Yokoi, T. Interobserver errors in anthropometry. J. Hum. Ergol. 1999, 28, 15–24. [Google Scholar]
- Kouchi, M.; Mochimaru, M. Errors in landmarking and the evaluation of the accuracy of traditional and 3D anthropometry. Appl. Ergon. 2011, 42, 518–527. [Google Scholar] [CrossRef]
- Sharkey, A.R.; King, S.W.; Kuo, R.Y.; Bickerton, S.B.; Ramsden, A.J.; Furniss, D. Measuring Limb Volume: Accuracy and Reliability of Tape Measurement Versus Perimeter Measurement. Lymphat. Res. Biol. 2018, 16, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.C.; Lin, G.; Wang, M.J.J. Comparing 3D foot scanning with conventional measurement methods. J. Foot Ankle Res. 2014, 7, 44. [Google Scholar] [CrossRef]
- Razeghi, M.; Batt, M.E. Foot type classification: A critical review of current methods. Gait Posture 2002, 15, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, M.C.; Zhu, A.; Lee, Y.C. Stature estimation from various three-dimensional anthropometric foot measurements of Taiwanese female population. Leg. Med. Tokyo Jpn. 2022, 54, 102000. [Google Scholar] [CrossRef]
- Jurca, A.; Žabkar, J.; Džeroski, S. Analysis of 1.2 million foot scans from North America, Europe and Asia. Sci. Rep. 2019, 9, 19155. [Google Scholar] [CrossRef] [PubMed]
- Istook, C. 3D scanning systems with application to the apparel industry. J. Fash. Market. Manag. 2000, 5, 120–132. [Google Scholar] [CrossRef]
- Zhao, J.; Xiong, S.; Bu, Y.; Goonetilleke, R. Computerized girth determination for custom footwear manufacture. Comput. Ind. Eng. 2008, 54, 359–373. [Google Scholar] [CrossRef]
- Cheng, F.T.; Perng, D.B. A systematic approach for developing a foot size information system for shoe last design. Int. J. Ind. Ergon. 2000, 25, 171–185. [Google Scholar] [CrossRef]
- Dickerson, L.C.; Queen, R.M. The Design and Validation of a Low-Cost Foot Measurement System. J. Biomech. Eng. 2021, 143, 084502. [Google Scholar] [CrossRef] [PubMed]
- Krauss, I.; Grau, S.; Mauch, M.; Maiwald, C.; Horstmann, T. Sex-related differences in foot shape. Ergonomics 2008, 51, 1693–1709. [Google Scholar] [CrossRef] [PubMed]
- Mauch, M.; Grau, S.; Krauss, I.; Maiwald, C.; Horstmann, T. A new approach to children’s footwear based on foot type classification. Ergonomics 2009, 52, 999–1008. [Google Scholar] [CrossRef] [PubMed]
- Luo, G.; Houston, V.L.; Mussman, M.; Garbarini, M.; Beattie, A.C.; Thongpop, C. Comparison of male and female foot shape. J. Am. Podiatr. Med. Assoc. 2009, 99, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Guldemond, N.A.; Leffers, P.; Sanders, A.P.; Emmen, H.; Schaper, N.C.; Walenkamp, G.H.I.M. Casting methods and plantar pressure: Effects of custom-made foot orthoses on dynamic plantar pressure distribution. J. Am. Podiatr. Med. Assoc. 2006, 96, 9–18. [Google Scholar] [CrossRef]
- Bamber, Z.A.; Wheeler, P.C.; He, X.; Ling, S.K.K.; Yung, P.S.H.; Fong, D.T.P. Screening for laterally deviated plantar pressure during stance using the Cumberland ankle instability tool and anthropometric measures. Res. Sports Med. 2021, 29, 323–335. [Google Scholar] [CrossRef]
- Beldame, J.; Sacco, R.; Munoz, M.A.; Masse, M.; Lalevée, M. Assessment of the Efficiency of Measuring Foot and Ankle Edema with a 3D Portable Scanner. Bioengineering 2023, 10, 549. [Google Scholar] [CrossRef]
- Agudelo-Varela, Ó.; Vargas-Riaño, J.; Valera, Á. Turmell-Meter: A Device for Estimating the Subtalar and Talocrural Axes of the Human Ankle Joint by Applying the Product of Exponentials Formula. Bioengineering 2022, 9, 199. [Google Scholar] [CrossRef]
- Ma, R.; Lam, W.K.; Ding, R.; Yang, F.; Qu, F. Effects of Shoe Midfoot Bending Stiffness on Multi-Segment Foot Kinematics and Ground Reaction Force during Heel-Toe Running. Bioengineering 2022, 9, 520. [Google Scholar] [CrossRef]
- Peng, H.T.; Liu, L.W.; Chen, C.J.; Chen, Z.R. The Soft Prefabricated Orthopedic Insole Decreases Plantar Pressure during Uphill Walking with Heavy Load Carriage. Bioengineering 2023, 10, 353. [Google Scholar] [CrossRef]
- Williams, D.S., 3rd; McClay, I.S.; Hamill, J. Arch structure and injury patterns in runners. Clin. Biomech. 2001, 16, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Isman, R.E.; Inman, V.T.; Poor, P.M. Anthropometric studies of the human foot and ankle. Bull. Prosthet. Res. 1969, 11, 97–129. [Google Scholar]
- Mootanah, R.; Song, J.; Lenhoff, M.W.; Hafer, J.F.; Backus, S.I.; Gagnon, D.; Deland, J.T., 3rd; Hillstrom, H.J. Foot Type Biomechanics Part 2: Are structure and anthropometrics related to function? Gait Posture 2013, 37, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Rogati, G.; Leardini, A.; Ortolani, M.; Caravaggi, P. Validation of a novel Kinect-based device for 3D scanning of the foot plantar surface in weight-bearing. J. Foot Ankle Res. 2019, 12, 46. [Google Scholar] [CrossRef]
- Bao, H.P.; Soundar, P.; Yang, T. Integrated approach to design and manufacture of shoe lasts for orthopaedic use. Comput. Ind. Eng. 1994, 26, 411–421. [Google Scholar] [CrossRef]
- Bogdab, S.; Costea, M.; Liute, D. Anthropometric study of the foot using 3D scanning method and statistical analysis. In Proceedings of the International symposium in Knitting an Apparel-ISKA 2013, Iasi, Romania, 21–22 June 2013. [Google Scholar]
- Hu, C.W.; Baca, A.; Groeber, M.; Dabnichki, P. Geometrical Model for Characterization of foot deformity using 3D imaging. IFAC-PapersOnLine 2018, 51, 373–378. [Google Scholar] [CrossRef]
- Rogati, G.; Leardini, A.; Ortolani, M.; Caravaggi, P. Semi-automatic measurements of foot morphological parameters from 3D plantar foot scans. J. Foot Ankle Res. 2021, 14, 18. [Google Scholar] [CrossRef]
- Telfer, S.; Woodburn, J. The use of 3D surface scanning for the measurement and assessment of the human foot. J. Foot Ankle Res. 2010, 3, 19. [Google Scholar] [CrossRef]
- Witana, C.P.; Xiong, S.; Zhao, J.; Goonetilleke, R.S. Foot measurements from three-dimensional scans: A comparison and evaluation of different methods. Int. J. Ind. Ergon. 2006, 36, 789–807. [Google Scholar] [CrossRef]
- Flannelly, K.J.; Jankowski, K.R.; Flannelly, L.T. Measures of variability in chaplaincy, health care, and related research. J. Health Care Chaplain. 2015, 21, 122–130. [Google Scholar] [CrossRef]
- Laštovička, O.; Cuberek, R.; Janura, M.; Klein, T. Evaluation of the Usability of the Tiger Full-Foot Three-Dimensional Scanner for the Measurements of Basic Foot Dimensions in Clinical Practice. J. Am. Podiatr. Med. Assoc. 2022, 112, 20-019. [Google Scholar] [CrossRef] [PubMed]
- Saltzman, C.L.; Nawoczenski, D.A.; Talbot, K.D. Measurement of the medial longitudinal arch. Arch. Phys. Med. Rehabil. 1995, 76, 45–49. [Google Scholar] [CrossRef] [PubMed]
- De Mits, S.; Coorevits, P.; De Clercq, D.; Elewaut, D.; Woodburn, J.; Roosen, P. Reliability and validity of the INFOOT three-dimensional foot digitizer for patients with rheumatoid arthritis. J. Am. Podiatr. Med. Assoc. 2011, 101, 198–207. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
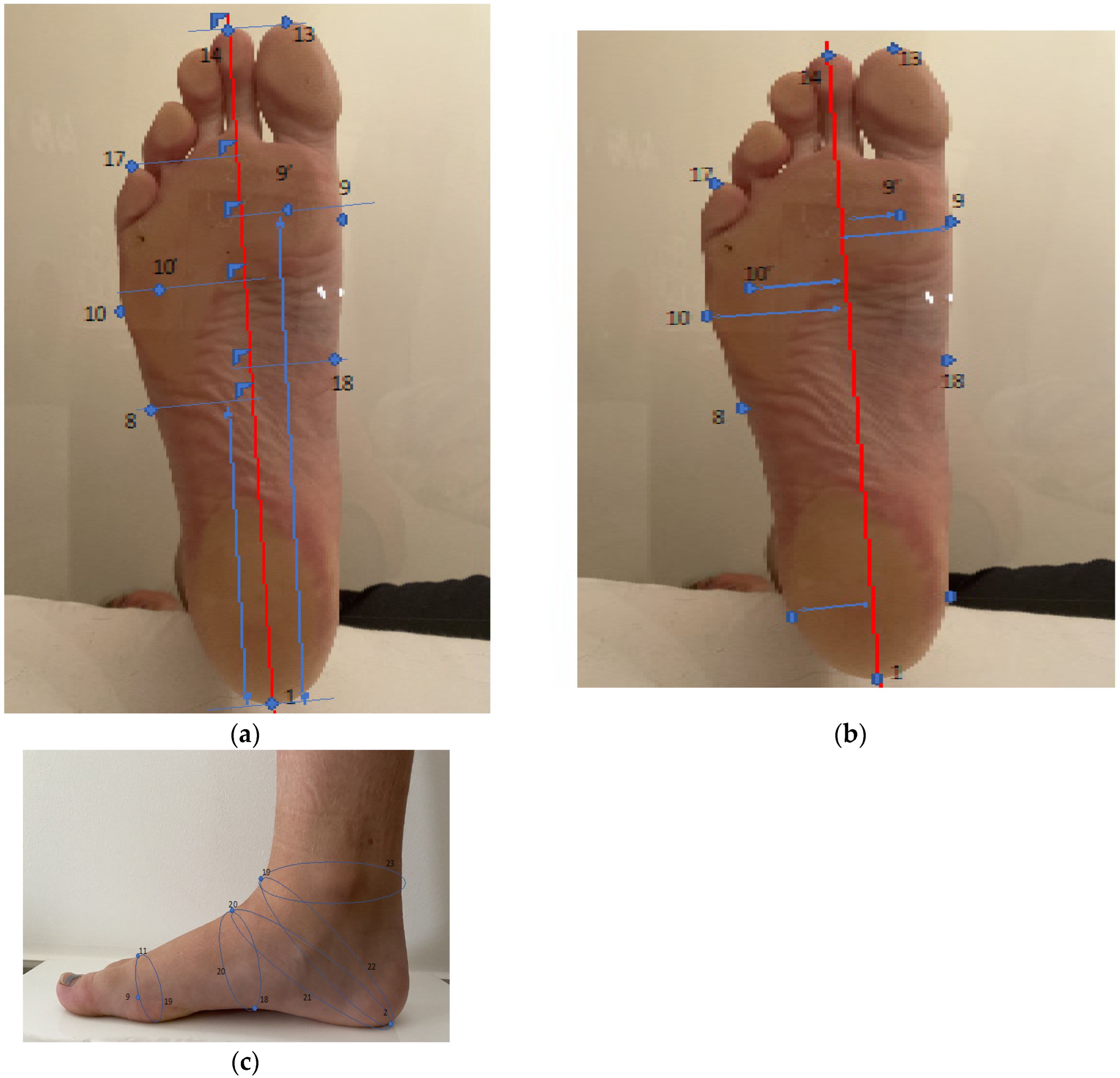
| Number | Name of Point |
|---|---|
| 1 | Pternion |
| 2 | Landing points |
| 3 | The most medial point of medial malleolus |
| 4 | Sphyrion |
| 5 | The most lateral point of lateral malleolus |
| 6 | Sphyrion fibulare |
| 7 | Navicular (the most medial point of navicular landmark) |
| 8 | Tuberosity of 5th metatarsal |
| 9 | Metatarsal tibiale |
| 10 | Metatarsal fibulare |
| 11 | Highest point of 1st metatarsal head |
| 12 | Toe 1 joint |
| 13 | Tip of 1 toe |
| 14 | Tip of 2 toe |
| 15 | Tip of 3 toe |
| 16 | Tip of 4 toe |
| 17 | Tip of 5 toe |
| 18 | Highest point of medial arch |
| 9′ | Ground support of M1 |
| 10′ | Ground support of M5 |
| 19 | Junction point |
| 20 | Highest point of Instep without the case of 50% of foot length |
| (a) | |||
| Length in mm | Foot length | Distance along the axis from pternion to the tip of the longest toe | |
| Arch length | Distance along the axis from pternion to the most medially prominent point on the first metatarsal head | ||
| Medial malleolus | Distance along the axis of the most medial point of medial malleolus | ||
| Lateral malleolus | Distance along the axis of the most lateral point of lateral malleolus | ||
| Fibulare instep | Distance along the axis of the most lateral point of instep | ||
| 1met to pternion | Distance from contact point of M1 to pternion | ||
| 5met to pternion | Distance from contact point of M5 to pternion | ||
| HC to pternion | (Horizontal) distance between center point of lateral and medial malleolus to pternion | ||
| Lat arch to pternion | Distance along the axis of the most lateral point of the arch | ||
| Med arch to pternion | Distance perpendicular to axis of the most lateral point of the arch | ||
| Toe 1 med to pternion | Distance from the most medial point of M1 to pternion | ||
| Toe 5 lat to pternion | Distance from the most lateral point of M5 to pternion | ||
| Waist point to pternion | Distance along the axis of the highest point mid foot, at 50% of foot length from pternion | ||
| (b) | |||
| Width in mm | Forefoot width | Distance between horizontal breadth, across the foot axis in the region in front of the most laterally prominent point on the fifth metatarsal head | |
| Heel width | Breath of the heel, 40 mm forward of the pternion | ||
| Bimalleolar | Distance between the most medially protruding point on the medial malleolus and the most laterally protruding point on the lateral malleolus, measured perpendicular to axis | ||
| Width mid-foot | Maximum horizontal breath, across the foot perpendicular to axis, at 50% of foot length from the pternion | ||
| 1–5 toe met | Maximum horizontal breath across the foot, perpendicular to axis, passing by toe 1 inside and toe 5 outside | ||
| Toe 1 inside | Toe 1 (big toe) contact point | ||
| Toe 5 outside | Toe 5 (little toe) contact point | ||
| Metatarsale tibiale | Width of the most medial point of M1 to axis | ||
| Metatarsale fibulare | Width of the most lateral point of M5 to axis | ||
| Waist point outside | The most lateral point relief, across the foot perpendicular to axis, at 50% of foot length from the pternion | ||
| (c) | |||
| Height * in mm | Ball girth | Height of the highest point of ball girth circumference | |
| Instep | Height of the highest point at the level of 50% of foot length | ||
| Toe 1 | Height of the highest point of M1 | ||
| Toe 5 | Height of the highest point of M5 | ||
| Navicular | Height of navicular point | ||
| Sphyrion | Height of sphyrion point | ||
| Lateral malleolus | Vertical distance from the floor to the most prominent point on the lateral malleolus | ||
| Medial malleolus | Vertical distance from the floor to the most prominent point on the medial malleolus | ||
| Mid-foot | Maximum height of the vertical cross-section at 50% of foot length from the pternion | ||
| (d) | |||
| Girth in mm | Metatarsal girth | Circumference of foot, measured with a tape touching the medial margin of the head of the first metatarsal bone, top of the first metatarsal bone and the lateral margin of the head of the fifth metatarsal bone | |
| Instep girth | Circumference at the level of midfoot, at 50% of foot length | ||
| Long heel girth | Girth from instep point around back heel point | ||
| Short heel girth | Maximum girth around back heel point and dorsal foot surface | ||
| Ankle girth | Horizontal girth at the foot and leg intersection | ||
| Waist | Smallest girth over middle cuneiform prominence | ||
| Population | n = 20 |
| Gender (Male/female) | 5/15 |
| Age (years) average +/− standard deviation | 35.62 +/− 9.54 |
| Minimum age (years) | 9 |
| Maximum age (years) | 75 |
| European shoe size (average +/− standard deviation) Range | 38.17 +/− 3.23 32–45 |
| Mean Variance * | Mean Difference (in mm) ** | Mean Measurement (in mm) *** | Mean % of Variance **** | ||
|---|---|---|---|---|---|
| Length measurements | Foot | 0.537 | 0.126 | 250.39 | 0.21 |
| Arch | 0.266 | 0.07 | 180.29 | 0.15 | |
| Medial Malleolus | 0.619 | 0.151 | 60.67 | 1.02 | |
| Lateral Malleolus | 0.693 | 0.201 | 54.02 | 1.29 | |
| Fibulare instep | 0.206 | 0.083 | 157.73 | 0.13 | |
| 1 Met to Pternion | 0.477 | 0.134 | 180.29 | 0.27 | |
| 5 Met to Pternion | 0.376 | 0.171 | 157.73 | 0.24 | |
| HC to Pternion | 0.144 | 0.138 | 32.51 | 0.44 | |
| Lat Arch to Pternion | 0.236 | 0.062 | 95.51 | 0.25 | |
| Med Arch to Pternion | 0.638 | 0.137 | 106.72 | 0.6 | |
| Toe 1 Med to Pternion | 3.538 | 0.791 | 222.61 | 1.59 | |
| Toe 5 Lat to Pternion | 8.006 | 0.283 | 189.95 | 4.22 | |
| Waist Point to Pternion | 0.095 | 0.05 | 105.91 | 0.09 | |
| Width measurements | Fore foot | 0.222 | 0.277 | 98.35 | 0.23 |
| Heel | 0.159 | 0.104 | 61.18 | 0.26 | |
| Bimalleolar | 0.242 | 0.111 | 71.51 | 0.34 | |
| Mid-Foot | 0.27 | 0.171 | 85.10 | 0.32 | |
| 1–5 Met | 0.0646 | 0.316 | 65.71 | 0.98 | |
| Toe 1 inside | 1.012 | 0.127 | 45.77 | 2.13 | |
| Toe 5 Outside | 0.598 | 0.081 | 44.57 | 1.34 | |
| Metatarsale Tibiale | 0.086 | 0.16 | 47.78 | 0.18 | |
| Metatarsale Fibulare | 0.073 | 0.109 | 47.93 | 0.15 | |
| Waist Point Outside | 0.128 | 0.04 | 41.13 | 0.31 | |
| Height measurements | Ball girth | 0.286 | 0.116 | 41.99 | 0.68 |
| Instep | 0.374 | 0.183 | 70.15 | 0.53 | |
| Toe 1 | 0.535 | 0.141 | 25.90 | 2.07 | |
| Toe 5 | 0.52 | 0.14 | 21.21 | 2.45 | |
| Navicular | 0.668 | 0.194 | 41.56 | 1.62 | |
| Sphyrion Fibulare | 5.068 | 0.633 | 62.01 | 8.28 | |
| Sphyrion | 1.727 | 0.562 | 71.29 | 2.42 | |
| Lateral Malleolus | 4.225 | 0.619 | 72.29 | 5.89 | |
| Medial Malleolus | 1.156 | 0.416 | 87.29 | 1.33 | |
| Mid-foot | 0.368 | 0.15 | 70.61 | 0.52 | |
| Girth Measurements | Ball | 1.514 | 0.256 | 243.10 | 0.62 |
| Instep | 1.592 | 0.612 | 245.42 | 0.65 | |
| Short Heel | 2.445 | 1.013 | 342.38 | 0.71 | |
| Long Heel | 7.059 | 1.955 | 330.14 | 2.14 | |
| Ankle | 5.941 | 1.102 | 253.60 | 2.34 | |
| Waist | 1.485 | 0.223 | 245.41 | 0.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sacco, R.; Munoz, M.-A.; Billuart, F.; Lalevée, M.; Beldame, J. Validation of an Automated Optical Scanner for a Comprehensive Anthropometric Analysis of the Foot and Ankle. Bioengineering 2023, 10, 968. https://doi.org/10.3390/bioengineering10080968
Sacco R, Munoz M-A, Billuart F, Lalevée M, Beldame J. Validation of an Automated Optical Scanner for a Comprehensive Anthropometric Analysis of the Foot and Ankle. Bioengineering. 2023; 10(8):968. https://doi.org/10.3390/bioengineering10080968
Chicago/Turabian StyleSacco, Riccardo, Marie-Aude Munoz, Fabien Billuart, Matthieu Lalevée, and Julien Beldame. 2023. "Validation of an Automated Optical Scanner for a Comprehensive Anthropometric Analysis of the Foot and Ankle" Bioengineering 10, no. 8: 968. https://doi.org/10.3390/bioengineering10080968
APA StyleSacco, R., Munoz, M.-A., Billuart, F., Lalevée, M., & Beldame, J. (2023). Validation of an Automated Optical Scanner for a Comprehensive Anthropometric Analysis of the Foot and Ankle. Bioengineering, 10(8), 968. https://doi.org/10.3390/bioengineering10080968