

The Role of Augmented Reality in the Advancement of Minimally Invasive Surgery Procedures: A Scoping Review



Abstract
1. Introduction
1.1. Advantages and Disadvantages of Minimally Invasive Surgery (MIS)
1.2. The Basics of Augmented Reality (AR) and Its Impact on Healthcare
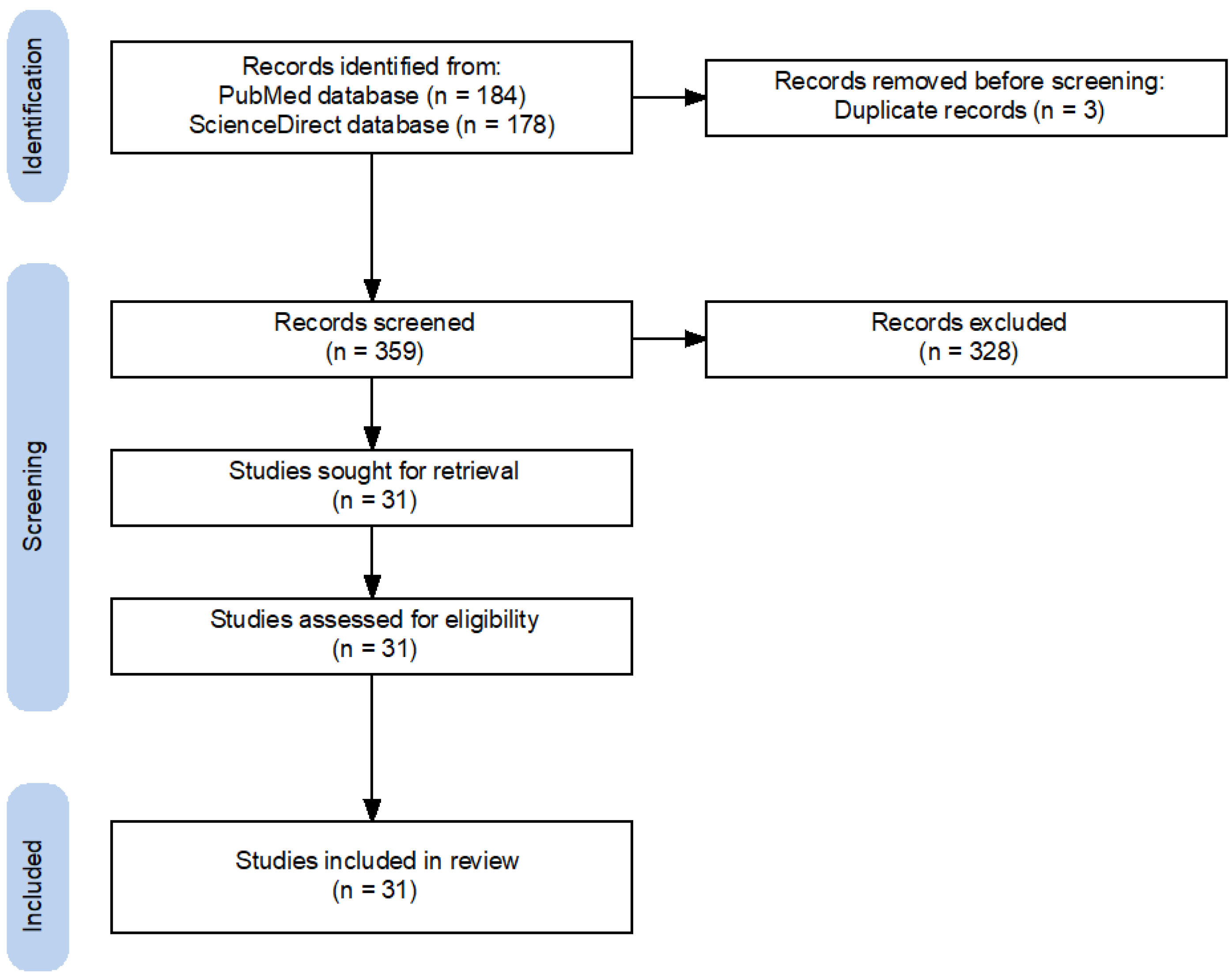
2. Materials and Methods
3. Results
3.1. AR-Guided Navigation
3.2. Improving Education and Training
3.3. Building Improved User-Environment Interfaces

{kind=link}
| Citation | Research Topic | Methodology | Outcome Parameter | Findings | Conclusions |
|---|---|---|---|---|---|
| Navigation | |||||
| Zadeh et al. [28] | AI system for laparoscopic AR-guided uterine surgery | Experimental N = 3800 (images) | Semiquantitative | Segmentation scores: (The higher, the better): 94.6% (training dataset) 84.9% (test dataset) Contour error on training: (The lower, the better): 19.5% (training dataset) 47.3% (test dataset) | System is useful for all surgical steps |
| Xu et al. [29] | Advantages and disadvantages of various surgical tracking systems | Review Specified search strategy N = 174 (included) | Objective evaluation | Overview of surgical navigation systems, tracking technologies, and preoperative planning procedures | Information loss is a major problem |
| Butler et al. [30] | In vivo percutaneously inserted pedicle screws with AR guidance | Prospective multicenter clinical trial N = 164 (patients) | Quantitative | Time from registration/percutaneous approach to screw placement: 3.54 min/screw Time per screw placement in first 20 cases: 4.1 min Time per screw placement in last 20 cases: 3.52 min (No difference, p = 0.48) | Confirmed efficiency/safety of screw placement with the benefits of AR technology |
| Zhu et al. [31] | Dual-mode AR-navigated neuroendoscopy for target localization and hematoma removal | Proof-of-concept Experimental N = 24 | Quantitative | Root Mean Square Error (RMSE) Between medical images and patients: 0.784 mm Variance: 0.1426 mm Pixel mismatching degrees: <1% in different AR modes Error of distance in catheter implantation experiments: 1.28 mm Variance: 0.43 mm Average error angle: 1.34° Variance 0.45° | High accuracy and feasibility of the system to provide stereo images with depth information fused to the patient |
| Lecointre et al. [32] | AR-based robotic assistance system for laparoscopic detection of target lymph nodes (TLN) in pelvic lymphadenectomy | Proof-of-concept Animal study N = 2 (pigs) | Quantitative and semiquantitative | CT overlay accuracy: >90% Overflow rates: <6% Significant higher scores: TLN: AR score 3.9 ± 0.32 vs. direct vision; DV, 2.1 ± 0.74 (p < 0.001) Ureter: AR score 3.7 ± 0.48 vs. DV 2.5 ± 0.84 (p = 0.003) Vessels: AR score 3.4 ± 0.51 vs. DV 1.7 ± 0.67 (p < 0.001) | AR approach with rigid registration is a first step in simplifying complex procedures and improving surgical safety |
| Guo et al. [33] | AR-guided MIS approach for scapula fractures | Retrospective clinical trial N = 21 (patients) | Quantitative | Virtual simulation time: 44.42 ± 15.54 min Time required for pre-operative plate contouring: 16.08 ± 5.09 min AR-guided MIS: Shorter operation time (−28.75 min, p = 0.0007) Less blood loss (−81.94 mL, p = 0.0052) Similar follow up outcome (p > 0.05) | Effective and reliable method for treating scapula fractures |
| Felix et al. [34] | AR-guided (VisAR) implantation of thoracolumbar pedicle screws | Experimental N = 7 (cadavers) | Quantitative | 124 pedicle screws in total Accuracy: 96% (Gertzbein-Robbins grades A and B) Combined angle of error: 2.4° Distance error: 1.9 mm | High-precision, emerging technology for navigating open surgery and MIS techniques with off-the-shelf headset hardware |
| Yuk et al. [35] | Advances/Applications of AR in spine surgery | Review Specified search strategy N = 41 (included) | Objective evaluation | No randomized controlled trials to date to evaluate accuracy, cost-effectiveness, and patient outcomes. VR training is an effective way to teach traditional/new methods of spine surgery | The use of VR/AR will increase in spine surgery |
| Chen et al. [36] | In-situ AR navigation system with enhanced arthroscopic information for MIS knee surgery | Experimental N = 2 (knee phantom, swine knee) | Quantitative | Mean targeting error Knee phantom: Traditional 2D arthroscopy navigation: 4.11 ± 0.80 mm AR navigation: 2.01 ± 0.65 mm (Significant difference, p < 0.01) In vitro swine knee: Traditional 2D arthroscopy navigation: 5.67 ± 0.97 mm AR navigation: 2.97 ± 0.79 mm (Significant difference, p < 0.01) | Suggested AR navigation is helpful in MIS knee surgeries |
| Benmahdjoub et al. [37] | AR in craniomaxillofacial surgery | Systematic Review Specified search strategy N = 7067 (reviewed) N = 39 (included) | Objective evaluation | Classification of study types, surgery types, equipment used, metrics reported, and benefits | Difficult to aggregate metrics. Difficult to obtain statistical value. Lack of user evaluation studies |
| Hussain et al. [38] | AR technology in cranial base surgery | Systematic review Specified search strategy N = 210 (reviewed) N = 45 (included) | Objective evaluation | Evaluate the benefits/challenges/solutions of AR systems in cranial base surgery | Growing interest in AR systems that can lead to safer and more cost-effective procedures, but issues need to be addressed |
| Hussain et al. [39] | Navigation in MIS and its evolution over time | Review Unspecified search strategy N = 54 (included) | Objective evaluation | Overview of the characteristics of navigation in MIS over time and key features for surgical advancement | New developments will further enhance the value of 3D navigation in MIS |
| Hu et al. [40] | Percutaneous Vertebroplasty (PVP) with the ARCASS AR System | Prospective case-control study N = 18 (patients) | Quantitative | ARCASS group/control group: Less frequency of fluoroscopy (6 vs. 18, p < 0.001) Shorter operation time (78 s vs. 205 s, p < 0.001) Higher proportion of ‘good’ entry point on lateral views (81.8% vs. 30.0%, p = 0.028) and anteroposterior views (72.7% vs. 20.0%, p = 0.020) | The ARCASS system provides a more precise bone entry point with less surgical time and unnecessary radiation exposure |
| Gribaudo et al. [41] | Development of AR-guided robotic surgery | Experimental N = not specified | Objective evaluation | Modular approach to the tracking problem. Segmentation of the entire process into several stages | May be helpful in surgical implementation |
| Chauvet et al. [42] | AR and magnetic resonance diffusion tensor imaging (DTI) for uterine fiber visualization and tracking | Case series N = 2 (patients) | Clinical evaluation | Localization of myomas Visualization and overlay of uterine muscle fibers | Can help surgeons identify and determine the starting point for laparoscopic myomectomies |
| Brebant et al. [43] | AR-guided supermicrosurgical lymphovenous anastomosis (LVA) | Clinical trial N = 32 (patients) | PROMs | 63 LVAs in total 27 upper extremities 5 lower extremities Mean operation time: 60–150 min Patency was confirmed by intraoperative AR-ICG No postoperative complications | AR-ICG enables a robust validation of LVA |
| Education and training | |||||
| Balla et al. [44] | Knowledge and prevalence of AR in surgical training in Italy | Web-based survey N = 217 (participants) | Quantitative | Participants: University hospital (41%), general hospital (35%), national health system (6%), general surgery (86%), abdominal surgery (72.8%) Knowledge of technology: Mean perceived knowledge (4.9 ± 2.4, out of max. 10), no experience (56.2%), primarily used for training (31.3%), didactic (29%) and intraoperatively (12.4%), Never used before (48.4%) Interest in technology: Should be used for teaching, training, and clinical use (80.3%), significant contribution in training (84.3%) and didactic (71.9%) Limits of technology: Insufficient knowledge (83.9%) and costs (80.6%) | Knowledge and dissemination still limited |
| Wild et al. [45] | AR-telestration for laparoscopic MIS training | Randomized controlled trial N = 60 (participants) Global Operative Assessment of Laparoscopic Skills (GOALS) Objective Structured assessment of Technical Skills (OSATS) Subjective workload (NASA-TLX questionnaire) | Quantitative | Faster training time (AR vs. verbal guidance) (1163 ± 275 vs. 1658 ± 375 s, p < 0.001) Reduced error rates Better laparoscopic cholecystectomy (GOALS 21 ± 5 vs. 18 ± 4, p < 0.007 and OSATS 67 ± 11 vs. 61 ± 8, p < 0.015) Less complications (13.3% vs. 40%, p < 0.020) Reduced subjective workload and stress (33.6 ± 12.0 vs. 30.6 ± 12.9, p < 0.022) | AR-telestration improves training success and MIS-safety |
| Gholizadeh et al. [46] | Overview of MIS and conventional liver surgery based on AR training | Review Specified search strategy N = 135 (review) N = 31 (included) | Quantitative | Inconsistency between algorithms used and claimed registration accuracy (mean 5.38 mm, range 0.93–10.3 mm) Any AR system (manual, semi-automatic, or automatic) requires human input/knowledge. Methods for determining accuracy are inconsistent. Measurements include pixel-based or spatial 3D registration error. Registration accuracy is difficult to determine. Few patients have undergone AR surgery. AR in soft tissue surgery cannot accurately register the virtual model | Further clinical studies are needed to evaluate AR as a tool to reduce postoperative morbidity and mortality |
| Godzik et al. [47] | VR and AR interfaces in spine surgery and education | Review and case report Unspecified search strategy N = 38 (included) | Objective evaluation | Overview of potential future applications and demonstration of the feasibility of a VR program for neurosurgical spine training using a case study | VR/AR is easy to implement. Further prospective studies through multi-institutional and industry-academic partnerships are needed to solidify the future of VR/AR in spine surgery education and clinical practice |
| Benčurik et al. [48] | New procedures and technologies for total mesorectal excision (TME) | Clinical trial N = 200 (patients) | Semiquantitative | In fifteen patients (15%), resection was postponed due to inadequate perfusion detected by AR. The incidence of anastomotic leakage was lower in the group with AR than in the group without AR (9% vs. 19%, p = 0.042) | The use of AR in rectal resections with TME for cancer may lead to a reduction in the incidence of anastomotic leakage |
| Pratt et al. [49] | Image guidance and AR in transsoral robotic surgery | Literature Overview and recent appraisals N = 10 (included) | Objective evaluation | Preoperative imaging guidance Intraoperative fluorescence imaging. Deformable registration using CBCT imaging. Image guided cochlear implantation | Ability to expand the surgical field with navigational cues and visualization of important anatomical structures |
| User-environment interface | |||||
| Thabit et al. [50] | AR with electromagnetic tracking system for MIS craniosynostosis | Experimental N = 120 (sutures on two skull phantoms) System Usability Scale (SUS) | Quantitative | Distance of the marked sutures from planning reference: 2.4 ± 1.2 mm Time per suture: 13 ± 5 s SUS value: 73 | Good accuracy Helpful in pre-planning MIS craniosynostosis surgery |
| Stewart et al. [51] | AR system for bedside surgical assistance | Proof-of-concept N = unspecified Different bedside tasks with da Vinci Xi surgical system on mock abdominal cavity | Semiquantitative | Improved times for ring path task with better resolution: lower resolution 23 ± 11 s vs. higher resolution 14 ± 4 s (p = 0.002) | High-resolution AR reduces time and improves accuracy during more complex laparoscopic procedures |
| Rush III et al. [52] | Advantages/disadvantages of AR in spine surgery | Review Unspecified search strategy N = 20 (included) | Objective evaluation | Different AR systems: Augmedics and Holosurgical ARAI navigation system | Accurate anatomical information with minimal to no radiation exposure |
| Forte et al. [53] | Voice-activated system for displaying live video on da Vinci Si surgical robot | Experimental N = 8 (surgeons) Phantom model Utility and usability questionnaire Four voice-controlled AR functions: Viewing live video Viewing 2D pre-op images Measuring 3D distances Warning about out-of-view instruments | Quantitative and semiquantitative | Average time for surgeons to become familiar with the technology: 8.47 min Accuracy of voice commands: 100% Voice command sensitivity: 89.8% | Support for further exploration |
| Wendler et al. [54] | Evaluate new technologies at various stages of the surgical workflow | Review Unspecified search strategy N = 226 (included) | Objective evaluation | Artificial intelligence. Computational visualization. Innovative molecular imaging modalities. Surgical navigation | Integrating molecular imaging could be the key to a new level of precision surgery |
| Li et al. [55] | Dense feature point description and matching method in endoscopic video | Experimental N = 3 (video segments) | Quantitative | True Positive Matching Result (TPM): 142.33 False Positive Matching Results (FPM): 10 | New approach has great potential for 2D/3D reconstruction in endoscopy |
| Jia et al. [56] | 6DoF method to improve motion tracking in AR systems | Experimental N = unspecified Ex-vivo tissue phantoms (kidney) and clinical datasets Root Mean Squared Error (RMSE) | Quantitative | RMSE: 2.31 mm (without disctraction) RMSE: 3.43 mm (middle-level distraction) RMSE: 3.56 mm (high-level distraction) | Robust and long-term tracking in highly dynamic operating environments |
| Wang et al. [57] | Robust tracking algorithm in an endoscopic AR system | Experimental N = unspecified Experiments with synthetic and simulation datasets | Quantitative | Average Contour Distance: 1.2398 pixels Frame Rates: 38.46 fps | The effectiveness and robustness of the method represents a novel tracking strategy for medical AR |
| Chen et al. [58] | Robotic algorithm (SLAM) in monocular surgical MIS scenes for reliable endoscopic camera tracking | Experimental Simulated laparoscopic scene image sequences and clinical data (N = 877) Root Mean Square Distance (RMSD) | Quantitative | RMSD: 2.54 mm Other monocular MIS scene reconstruction method (RMSD: 7.21 mm) State-of-the-art stereo reconstruction method (RMSD: 2.04/2.57 mm) | High accuracy of the developed algorithm |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Golder, H.J.; Papalois, V. Enhanced Recovery after Surgery: History, Key Advancements and Developments in Transplant Surgery. J. Clin. Med. 2021, 10, 1634. [Google Scholar] [CrossRef] [PubMed]
- Baek, H.; Cho, M.; Kim, S.; Hwang, H.; Song, M.; Yoo, S. Analysis of length of hospital stay using electronic health records: A statistical and data mining approach. PLoS ONE 2018, 13, e0195901. [Google Scholar] [CrossRef]
- Liu, C.; Pan, L.K. Advances in minimally invasive surgery and clinical measurement. Comput. Assist. Surg. 2019, 24, 1–4. [Google Scholar] [CrossRef]
- Hirst, A.; Philippou, Y.; Blazeby, J.; Campbell, B.; Campbell, M.; Feinberg, J.; Rovers, M.; Blencowe, N.; Pennell, C.; Quinn, T.; et al. No Surgical Innovation Without Evaluation: Evolution and Further Development of the IDEAL Framework and Recommendations. Ann. Surg. 2019, 269, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Jaffray, B. Minimally invasive surgery. Arch. Dis. Child. 2005, 90, 537–542. [Google Scholar] [CrossRef]
- Prete, F.P.; Pezzolla, A.; Prete, F.; Testini, M.; Marzaioli, R.; Patriti, A.; Jimenez-Rodriguez, R.M.; Gurrado, A.; Strippoli, G.F.M. Robotic Versus Laparoscopic Minimally Invasive Surgery for Rectal Cancer: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Ann. Surg. 2018, 267, 1034–1046. [Google Scholar] [CrossRef] [PubMed]
- Karayiannakis, A.J.; Makri, G.G.; Mantzioka, A.; Karousos, D.; Karatzas, G. Postoperative pulmonary function after laparoscopic and open cholecystectomy. Br. J. Anaesth. 1996, 77, 448–452. [Google Scholar] [CrossRef] [PubMed]
- Zureikat, A.H.; Beane, J.D.; Zenati, M.S.; Al Abbas, A.I.; Boone, B.A.; Moser, A.J.; Bartlett, D.L.; Hogg, M.E.; Zeh, H.J., 3rd. 500 Minimally Invasive Robotic Pancreatoduodenectomies: One Decade of Optimizing Performance. Ann. Surg. 2021, 273, 966–972. [Google Scholar] [CrossRef]
- de Rooij, T.; Lu, M.Z.; Steen, M.W.; Gerhards, M.F.; Dijkgraaf, M.G.; Busch, O.R.; Lips, D.J.; Festen, S.; Besselink, M.G. Minimally Invasive Versus Open Pancreatoduodenectomy: Systematic Review and Meta-analysis of Comparative Cohort and Registry Studies. Ann. Surg. 2016, 264, 257–267. [Google Scholar] [CrossRef]
- Chadi, S.A.; Guidolin, K.; Caycedo-Marulanda, A.; Sharkawy, A.; Spinelli, A.; Quereshy, F.A.; Okrainec, A. Current Evidence for Minimally Invasive Surgery During the COVID-19 Pandemic and Risk Mitigation Strategies: A Narrative Review. Ann. Surg. 2020, 272, e118–e124. [Google Scholar] [CrossRef]
- Chen, M.K.; Schropp, K.P.; Lobe, T.E. Complications of minimal-access surgery in children. J. Pediatr. Surg. 1996, 31, 1161–1165. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.I.; Baigrie, R.J.; Jamieson, G.G. A learning curve for laparoscopic fundoplication. Definable, avoidable, or a waste of time? Ann. Surg. 1996, 224, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Chandra, M.; Kumar, K.; Thakur, P.; Chattopadhyaya, S.; Alam, F.; Kumar, S. Digital technologies, healthcare and COVID-19: Insights from developing and emerging nations. Health Technol. 2022, 12, 547–568. [Google Scholar] [CrossRef]
- Milgram, P.; Kishino, F. A Taxonomy of Mixed Reality Visual Displays. IEICE Trans. Inf. Syst. 1994, E77-D, 1321–1329. [Google Scholar]
- Wedel, M.; Bigné, E.; Zhang, J. Virtual and augmented reality: Advancing research in consumer marketing. Int. J. Res. Mark. 2020, 37, 443–465. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, Q.; Chen, H.; Song, X.; Tang, H.; Tian, M. An overview of augmented reality technology. J. Phys. Conf. Ser. 2019, 1237, 022082. [Google Scholar] [CrossRef]
- Munzer, B.W.; Khan, M.M.; Shipman, B.; Mahajan, P. Augmented reality in emergency medicine: A scoping review. J. Med. Internet Res. 2019, 21, e12368. [Google Scholar] [CrossRef] [PubMed]
- Naziri, Q.; Mixa, P.J.; Murray, D.P.; Abraham, R.; Zikria, B.A.; Sastry, A.; Patel, P.D. Robotic-Assisted and Computer-Navigated Unicompartmental Knee Arthroplasties: A Systematic Review. Surg. Technol. Int. 2018, 32, 271–278. [Google Scholar] [PubMed]
- Vavra, P.; Roman, J.; Zonca, P.; Ihnat, P.; Nemec, M.; Kumar, J.; Habib, N.; El-Gendi, A. Recent Development of Augmented Reality in Surgery: A Review. J. Healthc. Eng. 2017, 2017, 4574172. [Google Scholar] [CrossRef]
- Herron, J. Augmented reality in medical education and training. J. Electron. Resour. Med. Libr. 2016, 13, 51–55. [Google Scholar] [CrossRef]
- Basoglu, N.A.; Goken, M.; Dabic, M.; Ozdemir Gungor, D.; Daim, T.U. Exploring adoption of augmented reality smart glasses: Applications in the medical industry. Front. Eng. 2018, 5, 167–181. [Google Scholar] [CrossRef]
- Gallos, P.; Georgiadis, C.; Liaskos, J.; Mantas, J. Augmented reality glasses and head-mounted display devices in healthcare. In Data, Informatics and Technology: An Inspiration for Improved Healthcare; IOS Press: Amsterdam, The Netherlands, 2018; pp. 82–85. [Google Scholar]
- Moro, C.; Štromberga, Z.; Raikos, A.; Stirling, A. The effectiveness of virtual and augmented reality in health sciences and medical anatomy. Anat. Sci. Educ. 2017, 10, 549–559. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Day, T.W.; Tang, W.; John, N.W. Recent developments and future challenges in medical mixed reality. In Proceedings of the 2017 IEEE International Symposium on Mixed and Augmented Reality (ISMAR), Nantes, France, 9–13 October 2017; pp. 123–135. [Google Scholar]
- Tong, A.; Flemming, K.; McInnes, E.; Oliver, S.; Craig, J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med. Res. Methodol. 2012, 12, 181. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J. Clin. Epidemiol. 2021, 134, 178–189. [Google Scholar] [CrossRef]
- Haddaway, N.R.; Page, M.J.; Pritchard, C.C.; McGuinness, L.A. PRISMA2020: An R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis. Campbell Syst. Rev. 2022, 18, e1230. [Google Scholar] [CrossRef] [PubMed]
- Zadeh, S.M.; François, T.; Comptour, A.; Canis, M.; Bourdel, N.; Bartoli, A. SurgAI3.8K: A labelled dataset of gynaecologic organs in laparoscopy, with application to automatic augmented reality surgical guidance. J. Minim. Invasive Gynecol. 2023. [Google Scholar] [CrossRef]
- Xu, L.; Zhang, H.; Wang, J.; Li, A.; Song, S.; Ren, H.; Qi, L.; Gu, J.J.; Meng, M.Q.H. Information loss challenges in surgical navigation systems: From information fusion to AI-based approaches. Inf. Fusion 2023, 92, 13–36. [Google Scholar] [CrossRef]
- Butler, A.J.; Colman, M.W.; Lynch, J.; Phillips, F.M. Augmented reality in minimally invasive spine surgery: Early efficiency and complications of percutaneous pedicle screw instrumentation. Spine J. 2023, 23, 27–33. [Google Scholar] [CrossRef]
- Zhu, T.; Jiang, S.; Yang, Z.; Zhou, Z.; Li, Y.; Ma, S.; Zhuo, J. A neuroendoscopic navigation system based on dual-mode augmented reality for minimally invasive surgical treatment of hypertensive intracerebral hemorrhage. Comput. Biol. Med. 2022, 140, 105091. [Google Scholar] [CrossRef]
- Lecointre, L.; Verde, J.; Goffin, L.; Venkatasamy, A.; Seeliger, B.; Lodi, M.; Swanström, L.L.; Akladios, C.; Gallix, B. Robotically assisted augmented reality system for identification of targeted lymph nodes in laparoscopic gynecological surgery: A first step toward the identification of sentinel node: Augmented reality in gynecological surgery. Surg. Endosc. 2022, 36, 9224–9233. [Google Scholar] [CrossRef]
- Guo, Q.; Li, X.; Tang, Y.; Huang, Y.; Luo, L. Augmented reality and three-dimensional plate library-assisted posterior minimally invasive surgery for scapula fracture. Int. Orthop. 2022, 46, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Felix, B.; Kalatar, S.B.; Moatz, B.; Hofstetter, C.; Karsy, M.; Parr, R.; Gibby, W. Augmented Reality Spine Surgery Navigation: Increasing Pedicle Screw Insertion Accuracy for Both Open and Minimally Invasive Spine Surgeries. Spine 2022, 47, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Yuk, F.J.; Maragkos, G.A.; Sato, K.; Steinberger, J. Current innovation in virtual and augmented reality in spine surgery. Ann. Transl. Med. 2021, 9, 94. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Cui, X.; Han, B.; Liu, J.; Zhang, X.; Liao, H. Augmented reality navigation for minimally invasive knee surgery using enhanced arthroscopy. Comput. Methods Programs Biomed. 2021, 201, 105952. [Google Scholar] [CrossRef] [PubMed]
- Benmahdjoub, M.; van Walsum, T.; van Twisk, P.; Wolvius, E.B. Augmented reality in craniomaxillofacial surgery: Added value and proposed recommendations through a systematic review of the literature. Int. J. Oral Maxillofac. Surg. 2021, 50, 969–978. [Google Scholar] [CrossRef]
- Hussain, R.; Lalande, A.; Guigou, C.; Bozorg-Grayeli, A. Contribution of Augmented Reality to Minimally Invasive Computer-Assisted Cranial Base Surgery. IEEE J. Biomed. Health Inform. 2020, 24, 2093–2106. [Google Scholar] [CrossRef] [PubMed]
- Hussain, I.; Cosar, M.; Kirnaz, S.; Schmidt, F.A.; Wipplinger, C.; Wong, T.; Härtl, R. Evolving Navigation, Robotics, and Augmented Reality in Minimally Invasive Spine Surgery. Glob. Spine J. 2020, 10, 22s–33s. [Google Scholar] [CrossRef]
- Hu, M.H.; Chiang, C.C.; Wang, M.L.; Wu, N.Y.; Lee, P.Y. Clinical feasibility of the augmented reality computer-assisted spine surgery system for percutaneous vertebroplasty. Eur. Spine J. 2020, 29, 1590–1596. [Google Scholar] [CrossRef]
- Gribaudo, M.; Piazzolla, P.; Porpiglia, F.; Vezzetti, E.; Violante, M.G. 3D augmentation of the surgical video stream: Toward a modular approach. Comput. Methods Programs Biomed. 2020, 191, 105505. [Google Scholar] [CrossRef]
- Chauvet, P.; Bourdel, N.; Calvet, L.; Magnin, B.; Teluob, G.; Canis, M.; Bartoli, A. Augmented Reality with Diffusion Tensor Imaging and Tractography during Laparoscopic Myomectomies. J. Minim. Invasive Gynecol. 2020, 27, 973–976. [Google Scholar] [CrossRef]
- Brebant, V.; Heine, N.; Lamby, P.; Heidekrueger, P.I.; Forte, A.J.; Prantl, L.; Aung, T. Augmented reality of indocyanine green fluorescence in simplified lymphovenous anastomosis in lymphatic surgery. Clin. Hemorheol. Microcirc. 2019, 73, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Balla, A.; Sartori, A.; Botteri, E.; Podda, M.; Ortenzi, M.; Silecchia, G.; Guerrieri, M.; Agresta, F. Augmented reality (AR) in minimally invasive surgery (MIS) training: Where are we now in Italy? The Italian Society of Endoscopic Surgery (SICE) ARMIS survey. Updates Surg. 2023, 75, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Wild, C.; Lang, F.; Gerhäuser, A.S.; Schmidt, M.W.; Kowalewski, K.F.; Petersen, J.; Kenngott, H.G.; Müller-Stich, B.P.; Nickel, F. Telestration with augmented reality for visual presentation of intraoperative target structures in minimally invasive surgery: A randomized controlled study. Surg. Endosc. 2022, 36, 7453–7461. [Google Scholar] [CrossRef] [PubMed]
- Gholizadeh, M.; Bakhshali, M.A.; Mazlooman, S.R.; Aliakbarian, M.; Gholizadeh, F.; Eslami, S.; Modrzejewski, A. Minimally invasive and invasive liver surgery based on augmented reality training: A review of the literature. J. Robot. Surg. 2022. [Google Scholar] [CrossRef] [PubMed]
- Godzik, J.; Farber, S.H.; Urakov, T.; Steinberger, J.; Knipscher, L.J.; Ehredt, R.B.; Tumialán, L.M.; Uribe, J.S. “Disruptive Technology” in Spine Surgery and Education: Virtual and Augmented Reality. Oper. Neurosurg. 2021, 21, S85–S93. [Google Scholar] [CrossRef]
- Benčurik, V.; Skrovina, M.; Martínek, L.; Bartoš, J.; Macháčková, M.; Dosoudil, M.; Štěpánová, E.; Přibylová, L.; Briš, R.; Anděl, P.; et al. Fluorescent angiography in colorectal surgery, the influence of augmented reality in the operating room on the anastomotic leakage after low rectal resection. Rozhl. Chir. 2021, 100, 543–551. [Google Scholar] [CrossRef]
- Pratt, P.; Arora, A. Transoral Robotic Surgery: Image Guidance and Augmented Reality. ORL J. Otorhinolaryngol. Relat. Spec. 2018, 80, 204–212. [Google Scholar] [CrossRef]
- Thabit, A.; Benmahdjoub, M.; van Veelen, M.C.; Niessen, W.J.; Wolvius, E.B.; van Walsum, T. Augmented reality navigation for minimally invasive craniosynostosis surgery: A phantom study. Int. J. Comput. Assist. Radiol. Surg. 2022, 17, 1453–1460. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.L.; Fong, A.; Payyavula, G.; DiMaio, S.; Lafaro, K.; Tallmon, K.; Wren, S.; Sorger, J.; Fong, Y. Study on augmented reality for robotic surgery bedside assistants. J. Robot. Surg. 2022, 16, 1019–1026. [Google Scholar] [CrossRef]
- Rush, A.J., 3rd; Shepard, N.; Nolte, M.; Siemionow, K.; Phillips, F. Augmented Reality in Spine Surgery: Current State of the Art. Int. J. Spine Surg. 2022, 16, S22–S27. [Google Scholar] [CrossRef]
- Forte, M.P.; Gourishetti, R.; Javot, B.; Engler, T.; Gomez, E.D.; Kuchenbecker, K.J. Design of interactive augmented reality functions for robotic surgery and evaluation in dry-lab lymphadenectomy. Int. J. Med. Robot. 2022, 18, e2351. [Google Scholar] [CrossRef] [PubMed]
- Wendler, T.; van Leeuwen, F.W.B.; Navab, N.; van Oosterom, M.N. How molecular imaging will enable robotic precision surgery: The role of artificial intelligence, augmented reality, and navigation. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4201–4224. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Pan, J.; Yang, Y.; Wei, N.; Yan, B.; Liu, H.; Yang, Y.; Qin, H. Accurate and robust feature description and dense point-wise matching based on feature fusion for endoscopic images. Comput. Med. Imaging Graph. 2021, 94, 102007. [Google Scholar] [CrossRef]
- Jia, T.; Taylor, Z.A.; Chen, X. Long term and robust 6DoF motion tracking for highly dynamic stereo endoscopy videos. Comput. Med. Imaging Graph. 2021, 94, 101995. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Zhang, M.; Meng, X.; Geng, Z.; Wang, F.Y. 3-D Tracking for Augmented Reality Using Combined Region and Dense Cues in Endoscopic Surgery. IEEE J. Biomed. Health Inform. 2018, 22, 1540–1551. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Tang, W.; John, N.W.; Wan, T.R.; Zhang, J.J. SLAM-based dense surface reconstruction in monocular Minimally Invasive Surgery and its application to Augmented Reality. Comput. Methods Programs Biomed. 2018, 158, 135–146. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brockmeyer, P.; Wiechens, B.; Schliephake, H. The Role of Augmented Reality in the Advancement of Minimally Invasive Surgery Procedures: A Scoping Review. Bioengineering 2023, 10, 501. https://doi.org/10.3390/bioengineering10040501
Brockmeyer P, Wiechens B, Schliephake H. The Role of Augmented Reality in the Advancement of Minimally Invasive Surgery Procedures: A Scoping Review. Bioengineering. 2023; 10(4):501. https://doi.org/10.3390/bioengineering10040501
Chicago/Turabian StyleBrockmeyer, Phillipp, Bernhard Wiechens, and Henning Schliephake. 2023. "The Role of Augmented Reality in the Advancement of Minimally Invasive Surgery Procedures: A Scoping Review" Bioengineering 10, no. 4: 501. https://doi.org/10.3390/bioengineering10040501
APA StyleBrockmeyer, P., Wiechens, B., & Schliephake, H. (2023). The Role of Augmented Reality in the Advancement of Minimally Invasive Surgery Procedures: A Scoping Review. Bioengineering, 10(4), 501. https://doi.org/10.3390/bioengineering10040501