


Walking Stability and Risk of Falls



Abstract

1. Introduction
2. Materials and Methods
2.1. Secondary Data Analysis
2.2. Movement Synergy Extraction
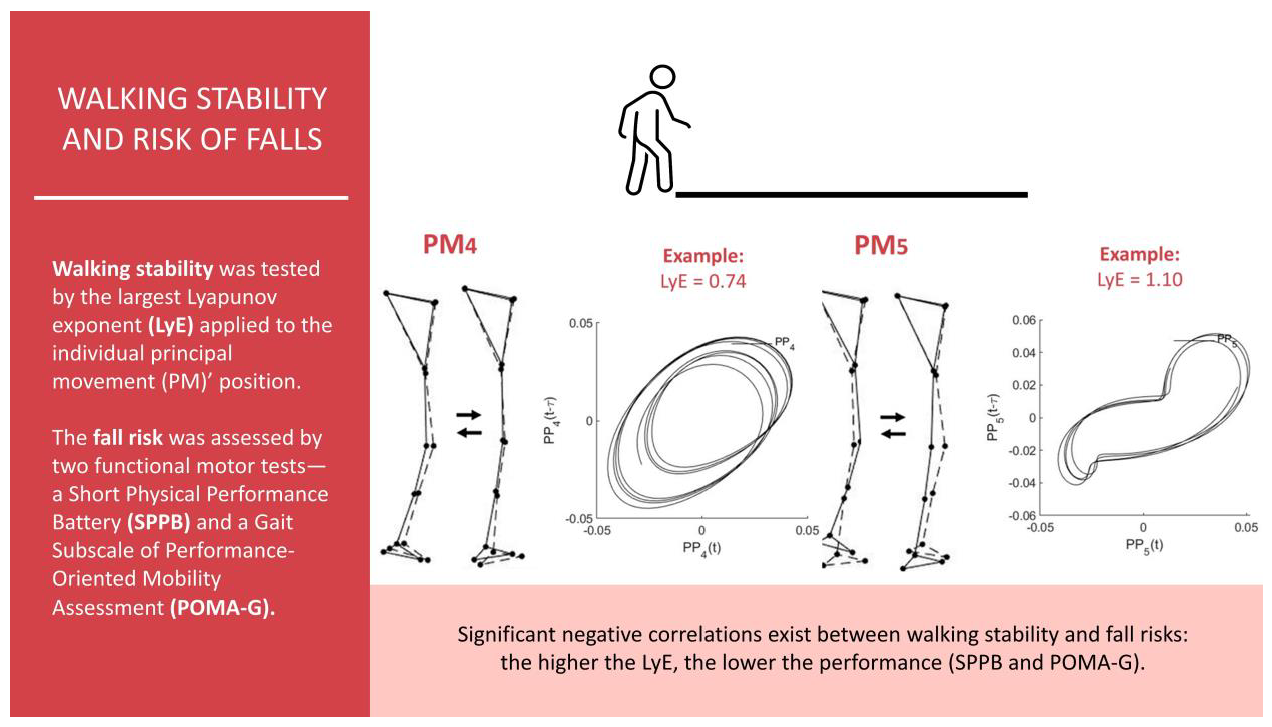
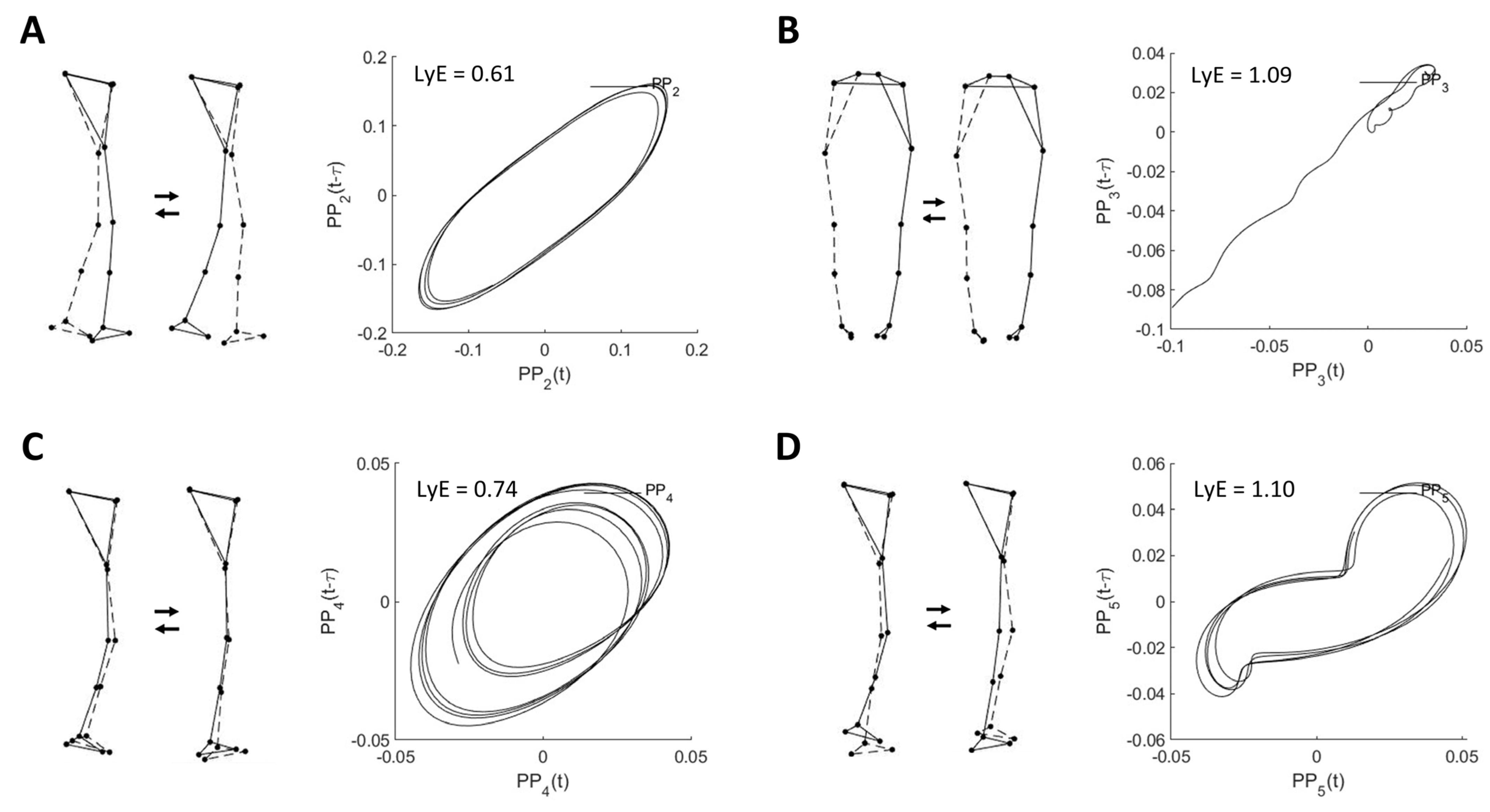
2.3. Investigating Walking Stability
2.4. Statistical Analysis
3. Results
3.1. Movement Synergies
3.2. Relationship between Walking Stability and Risk of Falls
4. Discussion
Limitations and Future Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sturnieks, D.L.; St George, R.; Lord, S.R. Balance Disorders in the Elderly. Neurophysiol. Clin. 2008, 38, 467–478. [Google Scholar] [CrossRef] [PubMed]
- Khalaf, S.; Morris, C. Falls in the Elderly. Psychiatr. Bull. 1996, 20, 501. [Google Scholar] [CrossRef]
- Gillespie, L. Preventing Falls in Elderly People. Br. Med. J. 2004, 328, 653–654. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, M.K.; Vonschewelov, T.; Karlsson, C.; CÃster, M.; Rosengen, B.E. Prevention of Falls in the Elderly: A Review. Scand. J. Public Health 2013, 41, 442–454. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Kumar, C. The Patient Who Falls: “It’s Always a Trade-Off”. JAMA-J. Am. Med. Assoc. 2010, 303, 258–266. [Google Scholar] [CrossRef]
- Tinetti, M.E. Preventing Falls in Elderly Persons. N. Engl. J. Med. 2003, 348, 42–49. [Google Scholar] [CrossRef]
- Callisaya, M.L.; Blizzard, L.; Schmidt, M.D.; McGinley, J.L.; Srikanth, V.K. Ageing and Gait Variability—A Population-Based Study of Older People. Age Ageing 2010, 39, 191–197. [Google Scholar] [CrossRef]
- Hamacher, D.; Singh, N.B.; Van Dieën, J.H.; Heller, M.O.; Taylor, W.R. Kinematic Measures for Assessing Gait Stability in Elderly Individuals: A Systematic Review. J. R. Soc. Interface 2011, 8, 1682–1698. [Google Scholar] [CrossRef]
- Bruijn, S.M.; Meijer, O.G.; Beek, P.J.; Van Dieen, J.H.; van Dieën, J.H. Assessing the Stability of Human Locomotion: A Review of Current Measures. J. R. Soc. Interface 2013, 10, 20120999. [Google Scholar] [CrossRef]
- Federolf, P.; Tecante, K.; Nigg, B. A Holistic Approach to Study the Temporal Variability in Gait. J. Biomech. 2012, 45, 1127–1132. [Google Scholar] [CrossRef]
- Cavanaugh, J.T.; Guskiewicz, K.M.; Stergiou, N. A Nonlinear Dynamic Approach for Evaluating Postural Control: New Directions for the Management of Sport-Related Cerebral Concussion. Sport. Med. 2005, 35, 935–950. [Google Scholar] [CrossRef] [PubMed]
- Dingwell, J.B.; Cusumano, J.P.; Cavanagh, P.R.; Sternad, D. Local Dynamic Stability Versus Kinematic Variability of Continuous Overground and Treadmill Walking. J. Biomech. Eng. 2001, 123, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Dingwell, J.B.; Marin, L.C. Kinematic Variability and Local Dynamic Stability of Upper Body Motions When Walking at Different Speeds. J. Biomech. 2006, 39, 444–452. [Google Scholar] [CrossRef] [PubMed]
- England, S.A.; Granata, K.P. The Influence of Gait Speed on Local Dynamic Stability of Walking. Gait Posture 2007, 25, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Haid, T.H.; Zago, M.; Promsri, A.; Doix, A.-C.M.; Federolf, P.A. PManalyzer: A Software Facilitating the Study of Sensorimotor Control of Whole-Body Movements. Front. Neuroinformat. 2019, 13, 24. [Google Scholar] [CrossRef] [PubMed]
- Promsri, A. Assessing Walking Stability Based on Whole-Body Movement Derived from a Depth-Sensing Camera. Sensors 2022, 22, 7542. [Google Scholar] [CrossRef]
- Federolf, P.A. A Novel Approach to Study Human Posture Control: “Principal Movements” Obtained from a Principal Component Analysis of Kinematic Marker Data. J. Biomech. 2016, 49, 364–370. [Google Scholar] [CrossRef]
- Troje, N.F. Decomposing Biological Motion: A Framework for Analysis and Synthesis of Human Gait Patterns. J. Vis. 2002, 2, 371–387. [Google Scholar] [CrossRef]
- Daffertshofer, A.; Lamoth, C.J.C.; Meijer, O.G.; Beek, P.J. PCA in Studying Coordination and Variability: A Tutorial. Clin. Biomech. 2004, 19, 415–428. [Google Scholar] [CrossRef]
- Promsri, A.; Mohr, M.; Federolf, P. Principal Postural Acceleration and Myoelectric Activity: Interrelationship and Relevance for Characterizing Neuromuscular Function in Postural Control. Hum. Mov. Sci. 2021, 77, 102792. [Google Scholar] [CrossRef]
- Promsri, A.; Haid, T.; Federolf, P. Complexity, Composition, and Control of Bipedal Balancing Movements as the Postural Control System Adapts to Unstable Support Surfaces or Altered Feet Positions. Neuroscience 2020, 430, 113–124. [Google Scholar] [CrossRef]
- Promsri, A.; Longo, A.; Haid, T.; Doix, A.-C.M.; Federolf, P. Leg Dominance as a Risk Factor for Lower-Limb Injuries in Downhill Skiers—A Pilot Study into Possible Mechanisms. Int. J. Environ. Res. Public Health 2019, 16, 3399. [Google Scholar] [CrossRef]
- Promsri, A. Sex Difference in Running Stability Analyzed Based on a Whole-Body Movement: A Pilot Study. Sports 2022, 10, 138. [Google Scholar] [CrossRef] [PubMed]
- Enderlin, C.; Rooker, J.; Ball, S.; Hippensteel, D.; Alderman, J.; Fisher, S.J.; McLeskey, N.; Jordan, K. Summary of Factors Contributing to Falls in Older Adults and Nursing Implications. Geriatr. Nurs. 2015, 36, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A Short Physical Performance Battery Assessing Lower Extremity Function: Association with Self-Reported Disability and Prediction of Mortality and Nursing Home Admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Abbruzzese, L.D. The Tinetti Performance-Oriented Mobility Assessment Tool. Am. J. Nurs. 1998, 98, 16J. [Google Scholar] [CrossRef]
- Lauretani, F.; Ticinesi, A.; Gionti, L.; Prati, B.; Nouvenne, A.; Tana, C.; Meschi, T.; Maggio, M. Short-Physical Performance Battery (SPPB) Score Is Associated with Falls in Older Outpatients. Aging Clin. Exp. Res. 2019, 31, 1435–1442. [Google Scholar] [CrossRef] [PubMed]
- Perell, K.L.; Nelson, A.; Goldman, R.L.; Luter, S.L.; Prieto-Lewis, N.; Rubenstein, L.Z. Fall Risk Assessment Measures: An Analytic Review. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, 761–766. [Google Scholar] [CrossRef]
- Veronese, N.; Bolzetta, F.; Toffanello, E.D.; Zambon, S.; De Rui, M.; Perissinotto, E.; Coin, A.; Corti, M.C.; Baggio, G.; Crepaldi, G.; et al. Association between Short Physical Performance Battery and Falls in Older People: The Progetto Veneto Anziani Study. Rejuvenation Res. 2014, 17, 276–284. [Google Scholar] [CrossRef]
- Faber, M.J.; Bosscher, R.J.; Van Wieringen, P.C.W. Clinimetric Properties of the Performance-Oriented Mobility Assessment. Phys. Ther. 2006, 86, 944–954. [Google Scholar] [CrossRef]
- Menz, H.B.; Lord, S.R.; Fitzpatrick, R.C. Age-Related Differences in Walking Stability. Age Ageing 2003, 32, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Caicedo, P.E.; Rengifo, C.F.; Rodriguez, L.E.; Sierra, W.A.; Gómez, M.C. Dataset for Gait Analysis and Assessment of Fall Risk for Older Adults. Data Br. 2020, 33, 106550. [Google Scholar] [CrossRef] [PubMed]
- Promsri, A.; Haid, T.; Federolf, P. How Does Lower Limb Dominance Influence Postural Control Movements during Single Leg Stance? Hum. Mov. Sci. 2018, 58, 165–174. [Google Scholar] [CrossRef]
- Promsri, A.; Haid, T.; Werner, I.; Federolf, P. Leg Dominance Effects on Postural Control When Performing Challenging Balance Exercises. Brain Sci. 2020, 10, 128. [Google Scholar] [CrossRef] [PubMed]
- Promsri, A.; Federolf, P. Analysis of Postural Control Using Principal Component Analysis: The Relevance of Postural Accelerations and of Their Frequency Dependency for Selecting the Number of Movement Components. Front. Bioeng. Biotechnol. 2020, 8, 480. [Google Scholar] [CrossRef]
- Longo, A.; Haid, T.; Meulenbroek, R.; Federolf, P. Biomechanics in Posture Space: Properties and Relevance of Principal Accelerations for Characterizing Movement Control. J. Biomech. 2019, 82, 397–403. [Google Scholar] [CrossRef]
- Ó’Reilly, D.; Federolf, P. Identifying Differences in Gait Adaptability across Various Speeds Using Movement Synergy Analysis. PLoS ONE 2021, 16, e0244582. [Google Scholar] [CrossRef]
- Longo, A.; Federolf, P.; Haid, T.; Meulenbroek, R. Effects of a Cognitive Dual Task on Variability and Local Dynamic Stability in Sustained Repetitive Arm Movements Using Principal Component Analysis: A Pilot Study. Exp. Brain Res. 2018, 236, 1611–1619. [Google Scholar] [CrossRef]
- Wolf, A.; Swift, J.B.; Swinney, H.L.; Vastano, J.A. Determining Lyapunov Exponents from a Time Series. Phys. D Nonlinear Phenom. 1985, 16, 285–317. [Google Scholar] [CrossRef]
- Kantz, H. A Robust Method to Estimate the Maximal Lyapunov Exponent of a Time Series. Phys. Lett. A 1994, 185, 77–87. [Google Scholar] [CrossRef]
- Akoglu, H. User’s Guide to Correlation Coefficients. Turk. J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef] [PubMed]
- Cappellini, G.; Ivanenko, Y.P.; Poppele, R.E.; Lacquaniti, F. Motor Patterns in Human Walking and Running. J. Neurophysiol. 2006, 95, 3426–3437. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, T.; Ota, S.; Yamashita, S.; Tsukamoto, Y.; Onishi, E. Association of Preoperative Variables of Ipsilateral Hip Abductor Muscles with Gait Function after Total Hip Arthroplasty: A Retrospective Study. Arthroplasty 2022, 4, 23. [Google Scholar] [CrossRef]
- Krupenevich, R.L.; Beck, O.N.; Sawicki, G.S.; Franz, J.R. Reduced Achilles Tendon Stiffness Disrupts Calf Muscle Neuromechanics in Elderly Gait. Gerontology 2022, 68, 241–251. [Google Scholar] [CrossRef]
- Keller, K.; Coldewey, M.; Engelhardt, M. Muscle Mass and Strength Loss with Aging. Gazz. Med. Ital. Arch. Sci. Med. 2014, 173, 477–483. [Google Scholar]
- Fredericson, M.; Moore, W.; Guillet, M.; Beaulieu, C. High Hamstring Tendinopathy in Runners Meeting the Challenges of Diagnosis, Treatment, and Rehabilitation. Physician Sportsmed. 2005, 33, 32–43. [Google Scholar] [CrossRef]
- Pavasini, R.; Guralnik, J.; Brown, J.C.; di Bari, M.; Cesari, M.; Landi, F.; Vaes, B.; Legrand, D.; Verghese, J.; Wang, C.; et al. Short Physical Performance Battery and All-Cause Mortality: Systematic Review and Meta-Analysis. BMC Med. 2016, 14, 215. [Google Scholar] [CrossRef]
- Creavin, S.T.; Wisniewski, S.; Noel-Storr, A.H.; Trevelyan, C.M.; Hampton, T.; Rayment, D.; Thom, V.M.; Nash, K.J.E.; Elhamoui, H.; Milligan, R.; et al. Mini-Mental State Examination (MMSE) for the Detection of Dementia in Clinically Unevaluated People Aged 65 and over in Community and Primary Care Populations. Cochrane Database Syst. Rev. 2016, 2016, CD011145. [Google Scholar] [CrossRef]
- Pijnappels, M.; van der Burg, J.C.E.; Reeves, N.D.; van Dieën, J.H. Identification of Elderly Fallers by Muscle Strength Measures. Eur. J. Appl. Physiol. 2008, 102, 585–592. [Google Scholar] [CrossRef]
- Pijnappels, M.; Reeves, N.D.; Maganaris, C.N.; van Dieën, J.H. Tripping without Falling; Lower Limb Strength, a Limitation for Balance Recovery and a Target for Training in the Elderly. J. Electromyogr. Kinesiol. 2008, 18, 188–196. [Google Scholar] [CrossRef]
- Torpy, J.M.; Lynm, C.; Glass, R.M. Frailty in Older Adults. JAMA 2006, 296, 2280. [Google Scholar] [CrossRef] [PubMed]
- Larson, S.T.; Wilbur, J. Muscle Weakness in Adults: Evaluation and Differential Diagnosis. Am. Fam. Physician 2020, 101, 95–108. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
| Min | Max | Mean | SD | |
|---|---|---|---|---|
| Age (years) | 54.0 | 87.0 | 69.8 | 8.5 |
| Mass (kg) | 41.8 | 104.4 | 67.6 | 11.2 |
| Height (m) | 1.4 | 1.7 | 1.6 | 0.1 |
| Body Mass Index (kg/m2) | 17.4 | 40.3 | 27.8 | 4.5 |
| MMSE | 22.0 | 30.0 | 26.6 | 2.5 |
| SPPB | 5.0 | 12.0 | 9.8 | 1.7 |
| POMA-G | 8.0 | 12.0 | 10.2 | 0.8 |
| Walking speed (m/s) | 0.6 | 1.2 | 0.8 | 0.2 |
| Number of falls in the last month (time) | 0 | 1 | 0.1 | 0.3 |
| PMk | Descriptive Characteristics | PPk_rVAR | PAk_rVAR |
|---|---|---|---|
| 1 | Movements of the lower extremities in the direction of walking | 98.91 ± 0.33 | 4.90 ± 1.12 |
| 2 | Resemble swing phase movement of the gait cycle: the anti-phase lower-limb movements in the anteroposterior direction | 0.90 ± 0.25 | 31.67 ± 2.94 |
| 3 | Movements of the lower extremities in the mediolateral direction (i.e., mediolateral sway) combined with anti-phase knee flexion and extension movements in the vertical direction | 0.07 ± 0.12 | 0.43 ± 0.17 |
| 4 | Both ankle and knee flexion and extension movements in the vertical direction | 0.05 ± 0.01 | 24.65 ± 1.95 |
| 5 | Resemble the mid-stance phase movement of the gait cycle: the anti-phase lower-limb movements in the vertical direction | 0.04 ± 0.01 | 9.22 ± 1.95 |
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Age | 1 | ||||||||||
| 2. BMI | −0.063 | 1 | |||||||||
| 3. MMSE | −0.449 ** | −0.290 | 1 | ||||||||
| 4. WS | 0.242 | 0.206 | −0.122 | 1 | |||||||
| 5. SPPB | −0.205 | −0.355 * | 0.142 | −0.556 *** | 1 | ||||||
| 6. POMA-G | −0.450 ** | −0.051 | 0.379 * | −0.356 * | 0.146 | 1 | |||||
| 7. PP1_LyE | 0.178 | 0.173 | −0.086 | −0.001 | −0.100 | 0.043 | 1 | ||||
| 8. PP2_LyE | 0.102 | 0.343 * | −0.145 | 0.516 *** | −0.164 | −0.249 | 0.032 | 1 | |||
| 9. PP3_LyE | −0.306 * | 0.145 | 0.030 | 0.099 | −0.097 | 0.003 | 0.066 | 0.075 | 1 | ||
| 10. PP4_LyE | 0.145 | 0.506 *** | −0.186 | 0.635 *** | −0.402 ** | −0.417 ** | 0.160 | 0.718 *** | 0.050 | 1 | |
| 11. PP5_LyE | 0.266 | 0.091 | −0.097 | 0.428 ** | −0.046 | −0.396 ** | 0.021 | 0.443 ** | −0.056 | 0.386 * | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Promsri, A.; Cholamjiak, P.; Federolf, P. Walking Stability and Risk of Falls. Bioengineering 2023, 10, 471. https://doi.org/10.3390/bioengineering10040471
Promsri A, Cholamjiak P, Federolf P. Walking Stability and Risk of Falls. Bioengineering. 2023; 10(4):471. https://doi.org/10.3390/bioengineering10040471
Chicago/Turabian StylePromsri, Arunee, Prasit Cholamjiak, and Peter Federolf. 2023. "Walking Stability and Risk of Falls" Bioengineering 10, no. 4: 471. https://doi.org/10.3390/bioengineering10040471
APA StylePromsri, A., Cholamjiak, P., & Federolf, P. (2023). Walking Stability and Risk of Falls. Bioengineering, 10(4), 471. https://doi.org/10.3390/bioengineering10040471