
A Review of Barbed Sutures—Evolution, Applications and Clinical Significance



Abstract
1. Introduction
2. History of Barbed Sutures
2.1. Problems Associated with Conventional, Non-Barbed Sutures
2.2. Barbed Sutures
2.2.1. Evolution of Barbed Sutures—Patents Detailing History of Barbed Sutures
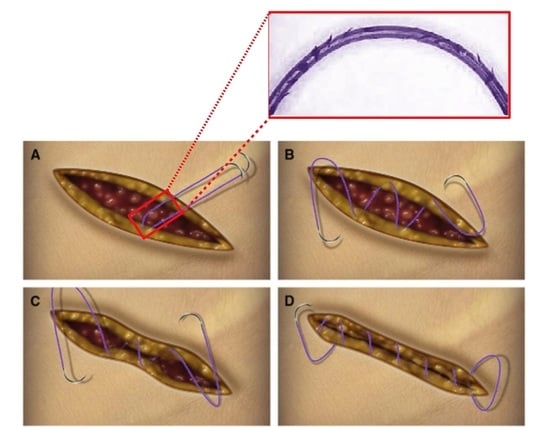
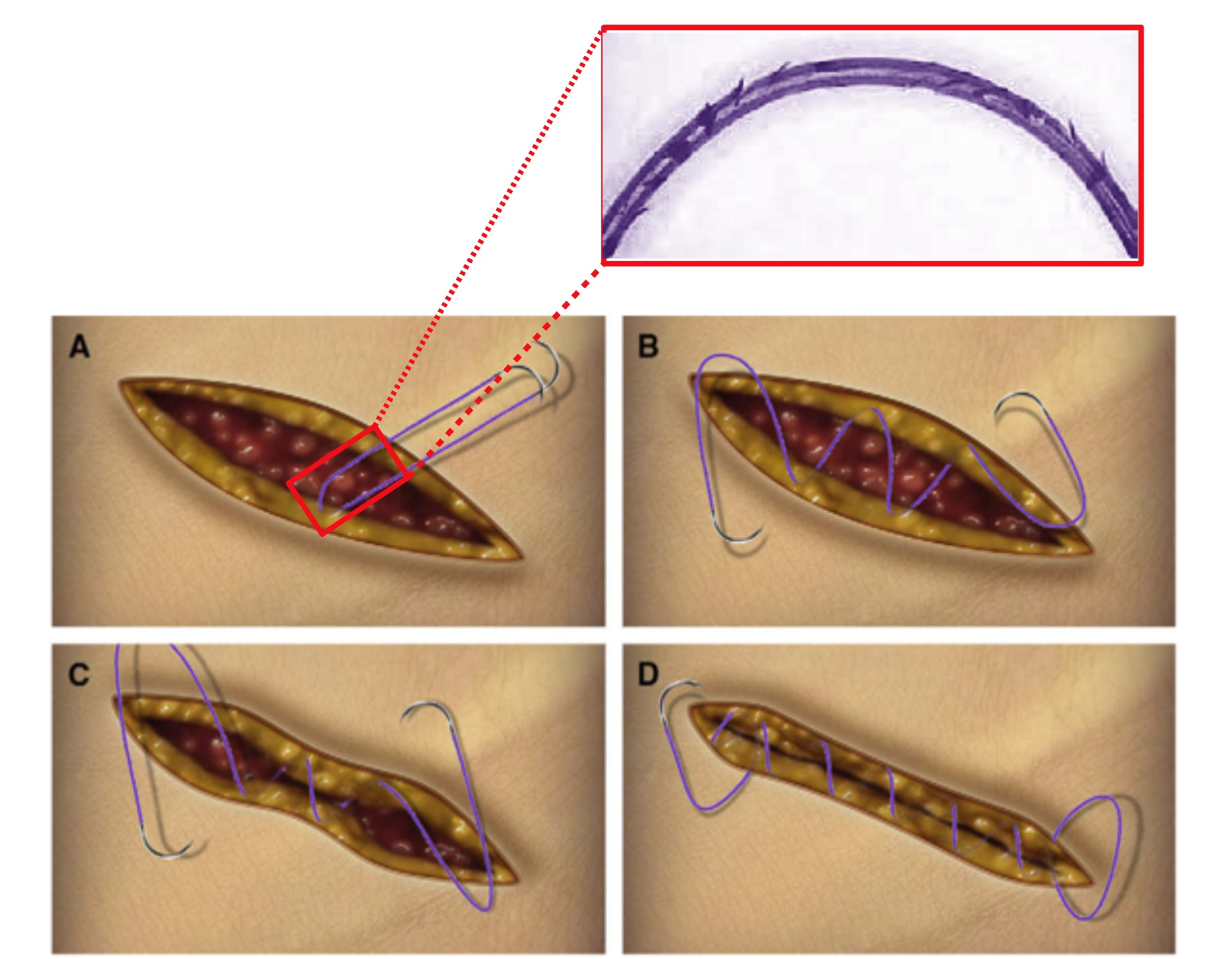
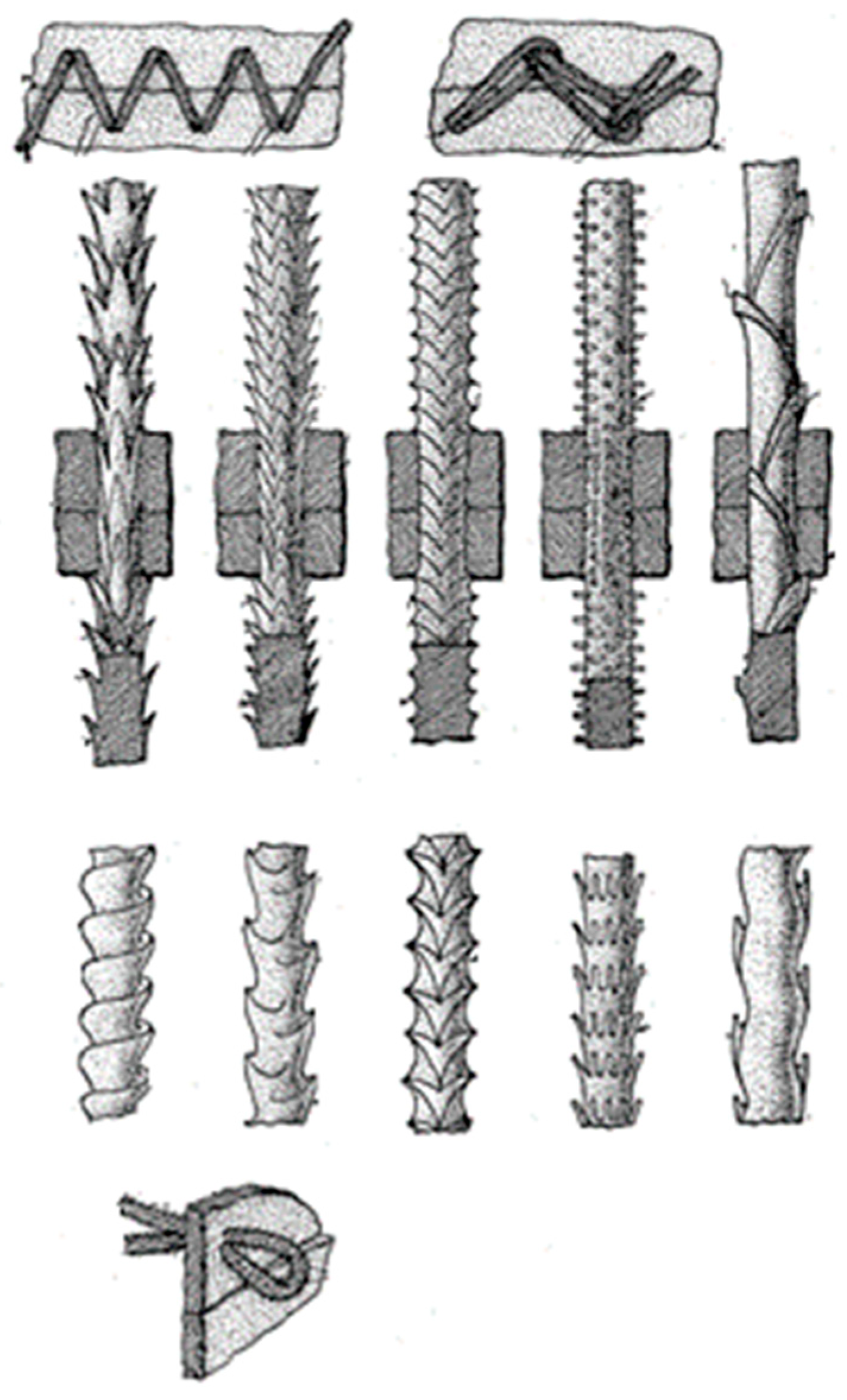
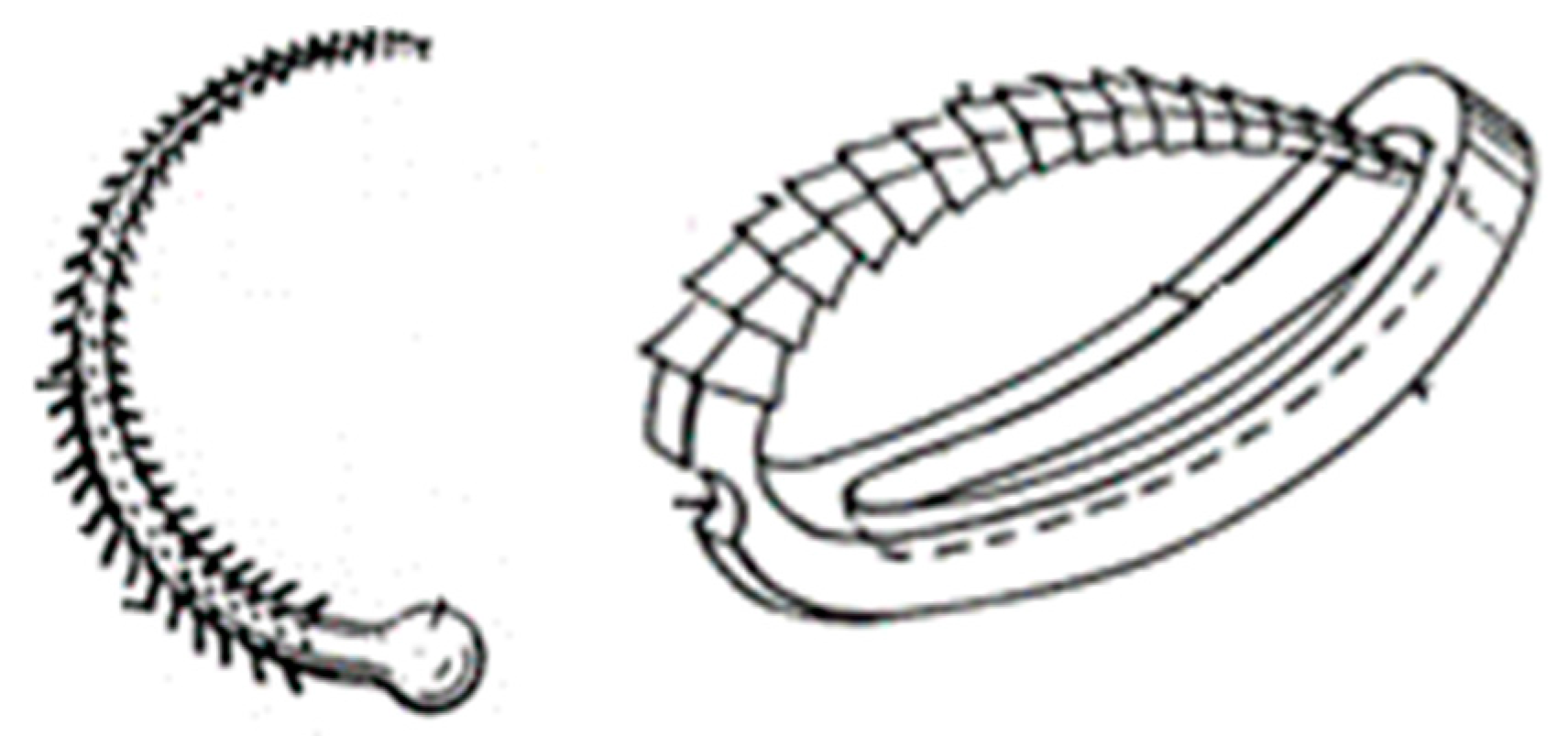
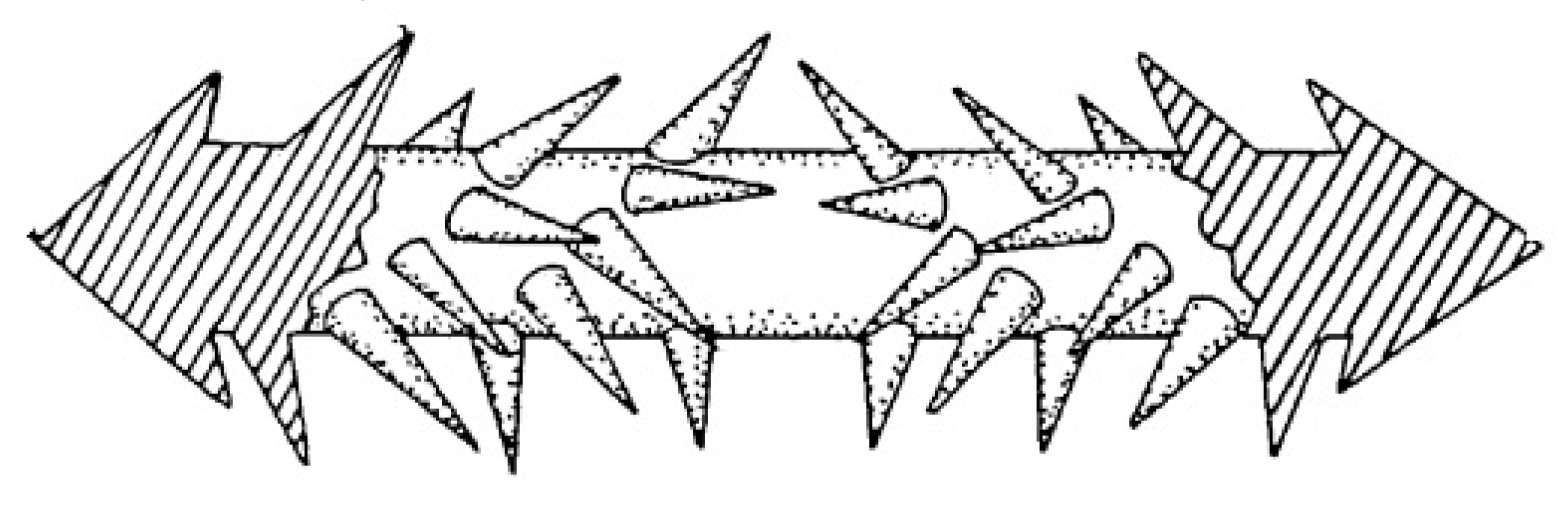
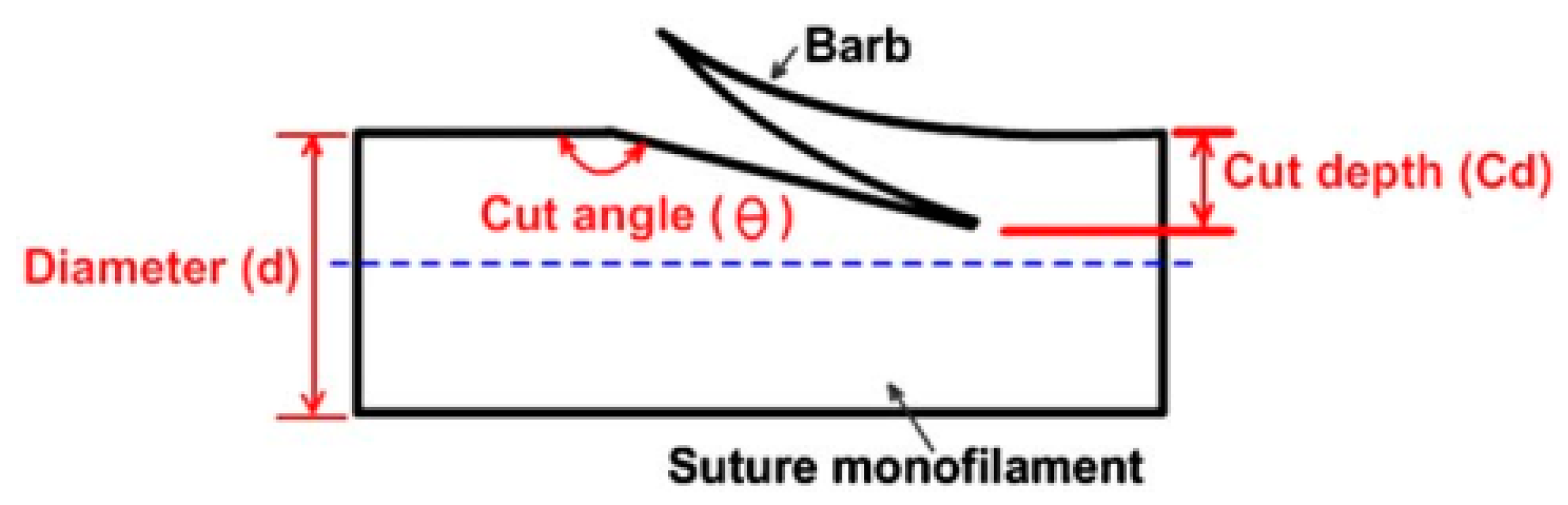
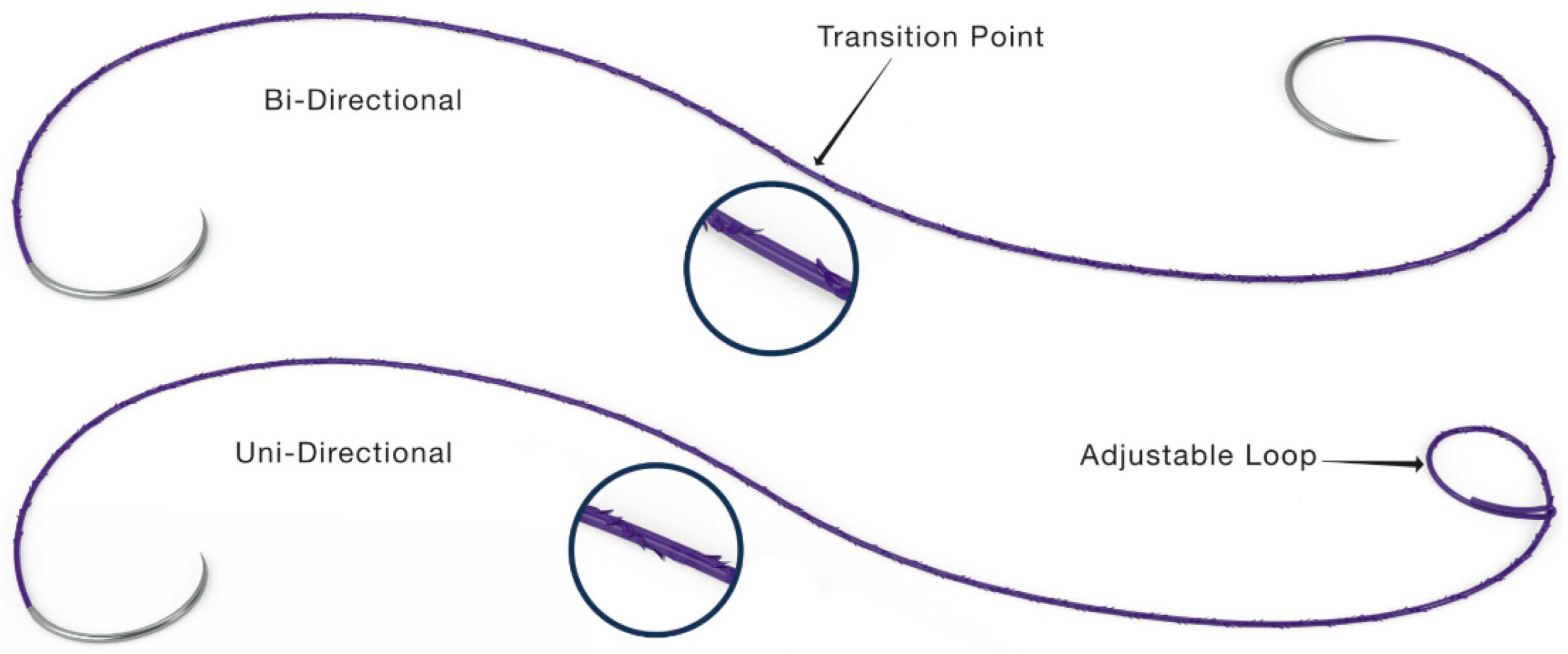
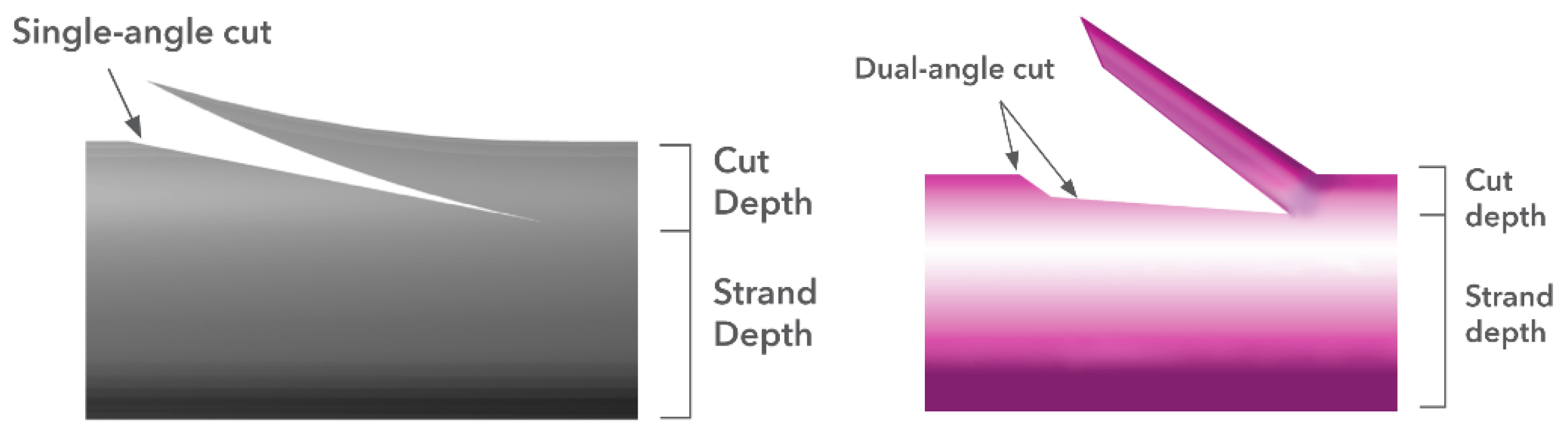
2.2.2. Geometric Design of Barbed Sutures
3. Commercial Barbed Sutures and Their Clinical Significance
3.1. Commercial Barbed Sutures
3.1.1. STRATAFIXTM Knotless Wound Closure Device
3.1.2. Quill SRSTM Bidirectional Barbed Sutures
3.1.3. V-LocTM Wound Closure Devices
3.2. The Role of Barbed Sutures in Cosmetic and Reconstructive Surgery: Benefits and Complications
3.2.1. Cosmetic and Plastic Surgery
3.2.2. Obstetric and Gynecological Procedures and Gastrointestinal Surgeries
3.2.3. Orthopedic Procedures
4. Conclusions
5. Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dattilo, P.P. Knotless Bi-Directional Barbed Absorbable Surgical Suture. Master’s Thesis, North Carolina State University, Raleigh, NC, USA, 2002. [Google Scholar]
- Edich, R.F.; Gubler, D.K.; Wallis, A.G.; Clark, J.J.; Dahlstrom, J.J.; Long, W.B. Wound Closure Sutures and Needles: A New Perspective. J. Environ. Pathol. Toxicol. Oncol. 2010, 29, 339–361. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y. A Comparison of the Properties and Performance of Polyvinylidene Fluoride and Polypropylene Barbed Sutures in Tendon Repair. Master’s Thesis, North Carolina State University, Raleigh, NC, USA, 2017. [Google Scholar]
- Danks, R.R.; Do, F.; Meyers, A.D. Wound Closure Technique: Overview, Indications, Contradictions. Available online: https://emedicine.medscape.com/article/1836438-overview (accessed on 22 June 2007).
- Buchanan, P.J.; Kung, T.A.; Cederna, P.S. Evidence-Based Medicine: Wound Closure. Plast. Reconstr. Surg. 2016, 138, 257S–270S. [Google Scholar] [CrossRef] [PubMed]
- Ruff, G.L. The History of Barbed Sutures. Aesthet. Surg. J. 2013, 33 (Suppl. S3), 12S–16S. [Google Scholar] [CrossRef] [PubMed]
- Holder, E.J. The Story of Catgut. Postgrad. Med. J. 1949, 25, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Cortez, R.; Lazcano, E.; Miller, T.; Hein, R.E.; Constantine, R.S.; Anigian, K.; Davis, K.E.; Kenkel, J.M. Barbed Sutures and Wound Complications in Plastic Surgery: An Analysis of Outcomes. Aesthet. Surg. J. 2015, 35, 178–188. [Google Scholar] [CrossRef] [PubMed]
- Dattilo, P.P.; King, M.W.; Leung, J.C. Tissue Holding Performance of Barbed Sutures. In Proceedings of the Society for Biomaterials 29th Annual Meeting Transactions, Reno, NV, USA, 24–29 April 2003. [Google Scholar]
- Matarasso, A.; Paul, M.D. Barbed Sutures in Aesthetic Plastic Surgery: Evolution of Thought and Process. Aesthet. Surg. J. 2013, 33 (Suppl. S3), 17S–31S. [Google Scholar] [CrossRef]
- Morency, S.D.; Jones, J.S. Barbed Surgical Suture. US 2003/0149447 A1, 7 August 2003. [Google Scholar]
- Murtha, A.P.; Kaplan, A.L.; Paglia, M.J.; Mills, B.B.; Feldstein, M.L.; Ruff, G.L. Evaluation of a Novel Technique for Wound Closure Using a Barbed Suture: Plast. Reconstr. Surg. 2006, 117, 1769–1780. [Google Scholar] [CrossRef]
- Paul, M.D. Complications of Barbed Sutures. Aesthet. Plast. Surg. 2008, 32, 149. [Google Scholar] [CrossRef]
- Wang, W.; Yan, S.; Liu, F.; Chai, W.; Zuo, J.; Xiao, J.; Niels-Derrek, S.; Zhu, Q.; Sanghita, B.; Bogdan, I.; et al. A Symmetric Anchor Designed Barbed Suture versus Conventional Interrupted Sutures in Total Knee Arthroplasty: A Multicenter, Randomized Controlled Trial. J. Orthop. Surg. 2020, 28, 1–10. [Google Scholar] [CrossRef]
- Cong, H. Studies of Barbed Surgical Sutures Associated with Materials, Anchoring Performance and Histology. Ph.D. Dissertation, North Carolina State University, Raleigh, NC, USA, 2018. [Google Scholar]
- Alcamo, J.H. Surgical Sutures. US 3123077, 3 March 1964. [Google Scholar]
- Akiyama, T. Surgical Thread and Cutting Apparatus for the Same. US 4069825, 24 January 1978. [Google Scholar]
- Yoon, I. Suture Devices Particularly Useful in Endoscopic Surgery. US 5222976A, 29 June 1993. [Google Scholar]
- Nilesh, I.; Martin, K. Tissue Holding Performance of Barbed Sutures. J. Donghua 2007, 24, 213–218. [Google Scholar]
- Ruff, G.L. Inserting Device for a Barbed Tissue Connector. US 5342376A, 30 August 1994. [Google Scholar]
- Ruff, G.L. Barbed Bodily Tissue Connector. US 7226468 B2, 5 June 2007. [Google Scholar]
- Buncke, H.J. Surgical Methods Using One-Way Suture. US 5931855, 3 August 1999. [Google Scholar]
- Rul, A.; Goraltchouk, A.; Herrmann, R.A.; Luscombe, B.H.; D’Agostino, W.L. Bidirectional Self-Retaining Sutures with Laser-Marked and/or Non-Laser Marked Indica and Methods. US 8961560 B2, 24 February 2015. [Google Scholar]
- Ingle, N.P.; King, M.W.; Zikry, M.A. Finite Element Analysis of Barbed Sutures in Skin and Tendon Tissues. J. Biomech. 2010, 43, 879–886. [Google Scholar] [CrossRef] [PubMed]
- Ingle, N.P.; King, M.W. Optimizing the Tissue Anchoring Performance of Barbed Sutures in Skin and Tendon Tissues. J. Biomech. 2010, 43, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Gregory, L.R.; Matthew, A.M.; Jeffrey, C.L. Barbed Suture in Combination with Surgical Needle. US 8721681 B2, 13 May 2014. [Google Scholar]
- Leung, J.C.; Ruff, G.L.; King, M.W.; Dattilo, P.P. Barbed, Bi-Directional Surgical Sutures. In Medical Textiles and Biomaterials for Healthcare; Elsevier: Amsterdam, The Netherlands, 2006; pp. 395–403. [Google Scholar] [CrossRef]
- Ruff, G. Technique and Uses for Absorbable Barbed Sutures. Aesthet. Surg. J. 2006, 26, 620–628. [Google Scholar] [CrossRef]
- Lin, Y.; Lai, S.; Huang, J.; Du, L. The Efficacy and Safety of Knotless Barbed Sutures in the Surgical Field: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Sci. Rep. 2016, 6, 23425. [Google Scholar] [CrossRef] [PubMed]
- Ethicon Inc. STRATAFIXTM Knotless Tissue Control Device Product Catalog. 2018. Available online: https://www.jnjmedtech.com/sites/default/files/user_uploaded_assets/pdf_assets/2019-10/115681-190531_WC_Suture_Catalog_2019_Update_297_7_CA.pdf (accessed on 22 June 2007).
- Corza Medical. QuillTM Barbed Suture Product Catalog. 2021. Available online: https://www.medtronic.com/content/dam/covidien/library/us/en/product/wound-closure/v-loc-wound-closure-device-product-catalog.pdf (accessed on 22 June 2007).
- Medtronic. V-LocTM Wound Closure Device Product Catalog. 2009. Available online: https://corza.com/wp-content/uploads/2021/10/COR-021-R12-US-Quill-Catalog_FINAL-1.pdf (accessed on 22 June 2007).
- Paul, M.D. Bidirectional Barbed Sutures for Wound Closure: Evolution and Applications. J. Am. Coll. Certif. Wound Spec. 2009, 1, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Choi, J. Cosmetic Surgery: Is It Science or Art? Arch. Plast. Surg. 2015, 42, 672–674. [Google Scholar] [CrossRef]
- 2020 Plastic Surgery Statistics Report; American Society of Plastic Surgeons: Chicago, IL, USA, 2020; Volume 26.
- Lee, M.; Sprague, N. Cosmetic Surgery: An Overview. 2016. Available online: https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/cosmetic-plastic-surgery-overview#:~:text=What%20is%20cosmetic%20plastic%20surgery,vein%20treatment%20or%20breast%20augmentation. (accessed on 22 June 2007).
- Jewell, M.L. Facial Rejuvenation with Loop Sutures, the MACS Lift and Its Derivatives. Plastic Surgery Key. Available online: https://plasticsurgerykey.com/facelift-5/ (accessed on 5 November 2022).
- Atiyeh, B.S.; Dibo, S.A.; Costagliola, M.; Hayek, S.N. Barbed Sutures “Lunch Time” Lifting: Evidence-Based Efficacy: “Lunch Time” Lifting. J. Cosmet. Dermatol. 2010, 9, 132–141. [Google Scholar] [CrossRef]
- Kaminer, M.S.; Bogart, M.; Choi, C.; Wee, S.A. Long-Term Efficacy of Anchored Barbed Sutures in the Face and Neck: Long-Term Efficacy of Anchored Barbed Sutures. Dermatol. Surg. 2008, 34, 1041–1047. [Google Scholar] [CrossRef]
- Giusto, G.; Iussich, S.; Tursi, M.; Perona, G.; Gandini, M. Comparison of Two Different Barbed Suture Materials for End-to-End Jejuno-Jejunal Anastomosis in Pigs. Acta Vet. Scand. 2019, 61, 3. [Google Scholar] [CrossRef]
- Greenberg, J.A.; Einarsson, J.I. The Use of Bidirectional Barbed Suture in Laparoscopic Myomectomy and Total Laparoscopic Hysterectomy. J. Minim. Invasive Gynecol. 2008, 15, 621–623. [Google Scholar] [CrossRef]
- Greenberg, J.A.; Goldman, R.H. Barbed Suture: A Review of the Technology and Clinical Uses in Obstetrics and Gynecology. Rev. Obstet. Gynecol. 2013, 6, 107–115. [Google Scholar]
- Selvest, N.; Subbaiah, M.; Maurya, D.K.; Dorairajan, G. Comparison of Unidirectional and Bidirectional Barbed Suture in Vaginal Cuff Closure during Total Laparoscopic Hysterectomy—A Randomised Controlled Trial. J. Clin. Diagn. Res. 2020, 14, QC12–QC15. [Google Scholar] [CrossRef]
- Demyttenaere, S.V.; Nau, P.; Henn, M.; Beck, C.; Zaruby, J.; Primavera, M.; Kirsch, D.; Miller, J.; Liu, J.J.; Bellizzi, A.; et al. Barbed Suture for Gastrointestinal Closure: A Randomized Control Trial. Surg. Innov. 2009, 16, 237–242. [Google Scholar] [CrossRef]
- Huang, P.; Tsai, M.; Ting, W.; Chen, H.; Lin, H.; Hsiao, S. Predictors of Surgical Outcomes of Laparoscopic Myomectomy with Barbed Sutures: Comparison of V-Loc and Quill Barbed Sutures. Int. J. Gynecol. Obstet. 2022, 158, 757–759. [Google Scholar] [CrossRef] [PubMed]
- Giampaolino, P.; De Rosa, N.; Tommaselli, G.A.; Santangelo, F.; Nappi, C.; Sansone, A.; Bifulco, G. Comparison of Bidirectional Barbed Suture Stratafix and Conventional Suture with Intracorporeal Knots in Laparoscopic Myomectomy by Office Transvaginal Hydrolaparoscopic Follow-up: A Preliminary Report. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 195, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Gutowski, K.A.; Warner, J.P. Incorporating Barbed Sutures in Abdominoplasty. Aesthet. Surg. J. 2013, 33 (Suppl. S3), 76S–81S. [Google Scholar] [CrossRef]
- Johnston, S.S.; Chen, B.P.-H.; Tommaselli, G.A.; Jain, S.; Pracyk, J.B. Barbed and Conventional Sutures in Spinal Surgery Patients: An Economic and Clinical Outcomes Comparison. J. Wound Care 2020, 29, S9–S20. [Google Scholar] [CrossRef]
- Shah, A.; Rowlands, M.; Au, A. Barbed Sutures and Tendon Repair—A Review. Hand 2015, 10, 6–15. [Google Scholar] [CrossRef]
- Ye, Z.; Zhu, W.; Xi, X.; Wu, Q. The Efficacy of Bidirectional Barbed Sutures for Incision Closure in Total Knee Replacement: A Protocol of Randomized Controlled Trial. Medicine 2020, 99, e21867. [Google Scholar] [CrossRef]
- Chowdhry, M.; Singh, S. Severe Scar Problems Following Use of a Locking Barbed Skin Closure System in the Foot. Foot Ankle Surg. 2013, 19, 131–134. [Google Scholar] [CrossRef]
- Mayet, Z.; Eshraghi, H.; Ferrao, P.N.F.; Saragas, N.P. Use of Locking Barbed Sutures in Foot and Ankle Surgery. A Case Series. Foot Ankle Surg. 2017, 23, 57–61. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Suture Name | Description | Suture Placement |
|---|---|---|
| Aptos Thread (Kolster Methods, Inc., Anahelm, CA, USA) | Bidirectional, nonabsorbable barbed suture | Free floating |
| Contour Thread (Surgical Specialities, Reading, PA, USA) | Unidirectional, nonabsorbable, looped or nonlooped barbed suture | Anchored proximally |
| Isse Endo Progressive Facelift Suture (Kolster Methods, Inc., Anahelm, CA, USA) | Unidirectional, nonabsorbable barbed suture | Anchored proximally |
| Silhouette Mid-Face Suture (Kolster Methods, Inc., Anahelm, CA, USA) | Nonabsorbable suture material with absorbable knots at 10 mm intervals | Anchored proximally |
| Woffles Thread (Kolster Methods, Inc., Anahelm, CA, USA) | Bidirectional, nonabsorbable barbed suture doubled in a sling format | Anchored proximally |
| V-Loc TM Wound Closure Device (Medtronic, New Haven, CT, USA) | Unidirectional, knotless, absorbable barbed suture | Anchored or not anchored |
| QuillTM Knotless Tissue-Closure Device (Corza Medical Inc., Westwood, MA, USA) | Absorbable and nonabsorbable, knotless, bidirectional barbed suture with central non-barbed segment | Anchored or not anchored |
| STRATAFIXTM (Ethicon Inc., Somerville, NJ, USA) | Bidirectional, absorbable barbed suture | Anchored or not anchored |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nambi Gowri, K.; King, M.W. A Review of Barbed Sutures—Evolution, Applications and Clinical Significance. Bioengineering 2023, 10, 419. https://doi.org/10.3390/bioengineering10040419
Nambi Gowri K, King MW. A Review of Barbed Sutures—Evolution, Applications and Clinical Significance. Bioengineering. 2023; 10(4):419. https://doi.org/10.3390/bioengineering10040419
Chicago/Turabian StyleNambi Gowri, Karuna, and Martin W. King. 2023. "A Review of Barbed Sutures—Evolution, Applications and Clinical Significance" Bioengineering 10, no. 4: 419. https://doi.org/10.3390/bioengineering10040419
APA StyleNambi Gowri, K., & King, M. W. (2023). A Review of Barbed Sutures—Evolution, Applications and Clinical Significance. Bioengineering, 10(4), 419. https://doi.org/10.3390/bioengineering10040419