



Tissue Integration of Calcium Phosphate Compound after Subchondroplasty: 4-Year Follow-Up in a 76-Year-Old Female Patient



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
3. Results
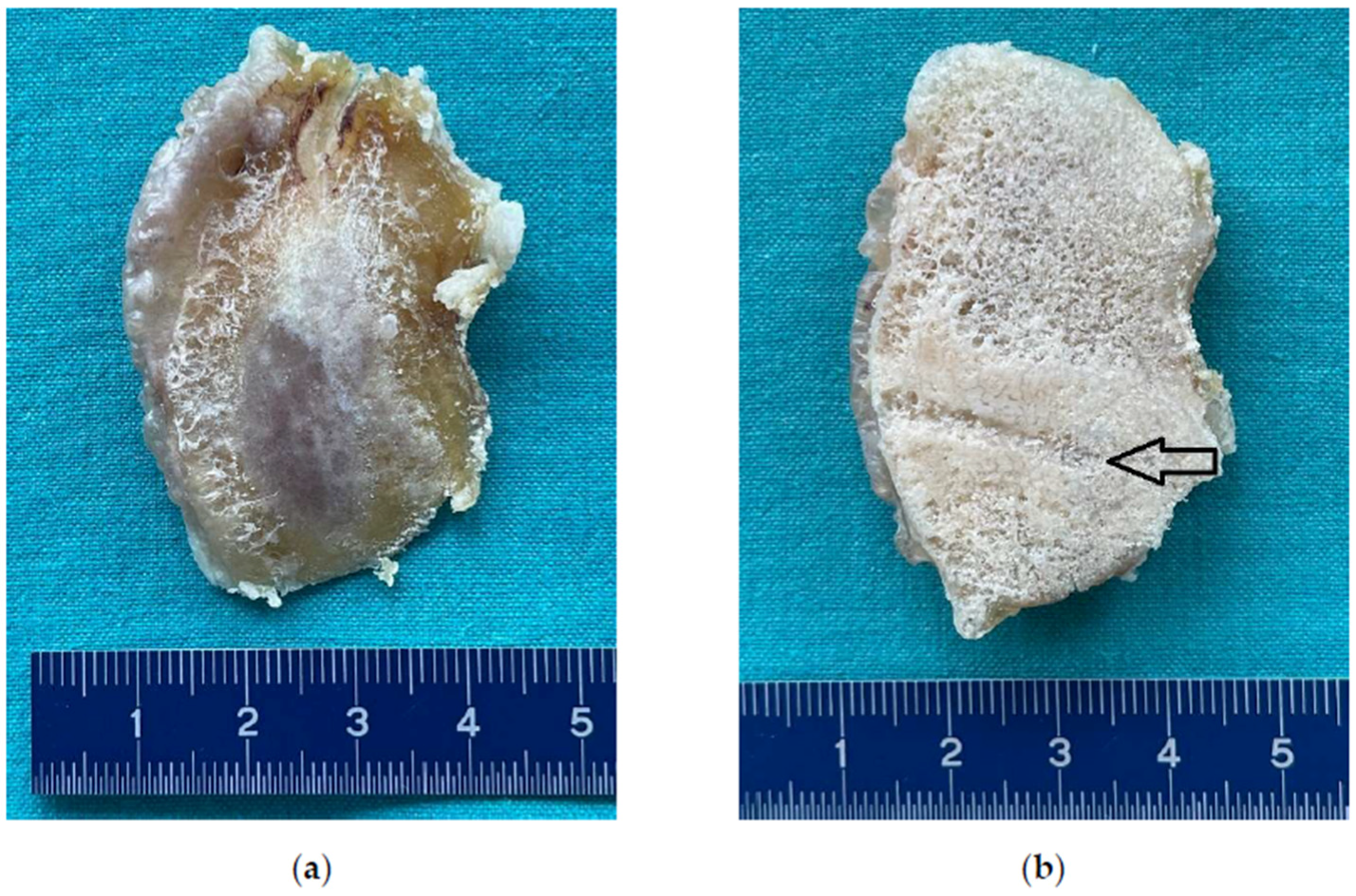
3.1. Surgical Examination
3.2. Histologic Examination
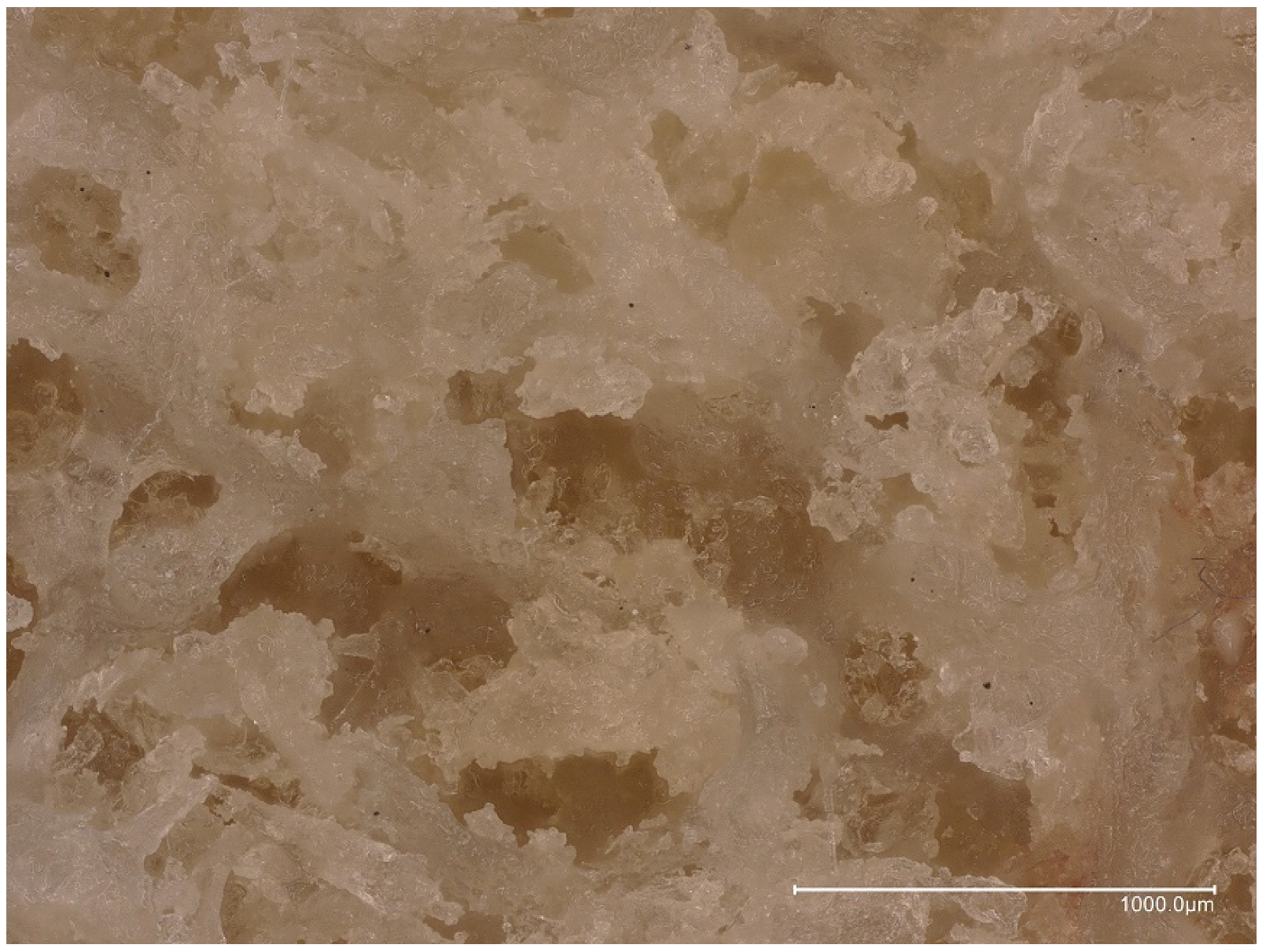
3.3. Microphotography and Stereomicroscopic Examination
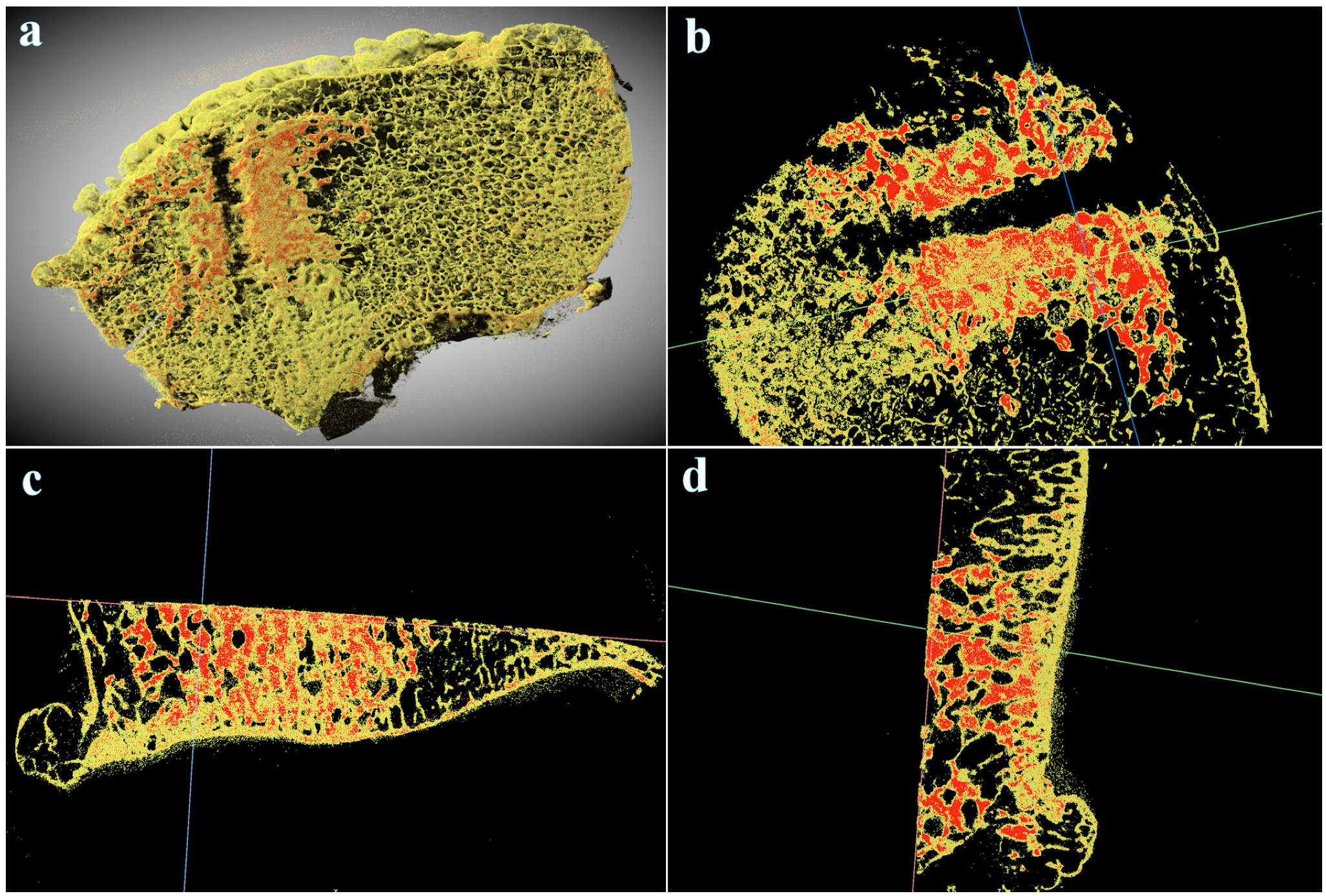
3.4. Micro-CT Examination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pasqualotto, S.; Sgroi, A.V.; Causero, A.; Di Benedetto, P.; Zorzi, C. Subchondroplasty in the Treatment of Bone Marrow Lesions of the Knee: Preliminary Experience on First 15 Patients. Joints 2021, 7, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.B.; Sharkey, P.F. Subchondroplasty for Treating Bone Marrow Lesions. J. Knee Surg. 2016, 29, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Zeng, G.J.; Foong, W.S.; Lie, T.T.D. Knee subchondroplasty for management of subchondral bone cysts: A novel treatment method. Singap. Med. J. 2021, 62, 492–496. [Google Scholar] [CrossRef] [PubMed]
- Bonadio, M.B.; Giglio, P.N.; Helito, C.P.; Pécora, J.R.; Camanho, G.L.; Demange, M.K. Subchondroplasty for treating bone marrow lesions in the knee-initial experience. Rev. Bras. Ortop. 2017, 52, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Levy, A.S.; Cousins, K. The rational for and efficacy of subchondroplasty in the injured worker. J. Orthop. 2020, 22, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef]
- Cross, M.; Smith, E.; Hoy, D.; Nolte, S.; Ackerman, I.; Fransen, M.; Bridgett, L.; Williams, S.; Guillemin, F.; Hill, C.L.; et al. The global burden of hip and knee osteoarthritis: Estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1323–1330. [Google Scholar] [CrossRef]
- Kohn, M.D.; Sassoon, A.A.; Fernando, N.D. Classifications in Brief: Kellgren-Lawrence Classification of Osteoarthritis. Clin. Orthop. Relat. Res. 2016, 474, 1886–1893. [Google Scholar] [CrossRef]
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone Jt. Surg. 2007, 89, 780–785. [Google Scholar] [CrossRef]
- Krakowski, P.; Karpiński, R.; Jojczuk, M.; Nogalska, A.; Jonak, J. Knee MRI Underestimates the Grade of Cartilage Lesions. Appl. Sci. 2021, 11, 1552. [Google Scholar] [CrossRef]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef]
- Krakowski, P.; Karpiński, R.; Maciejewski, R.; Jonak, J.; Jurkiewicz, A. Short-Term Effects of Arthroscopic Microfracturation of Knee Chondral Defects in Osteoarthritis. Appl. Sci. 2020, 10, 8312. [Google Scholar] [CrossRef]
- Alliston, T.; Hernandez, C.J.; Findlay, D.M.; Felson, D.T.; Kennedy, O.D. Bone marrow lesions in osteoarthritis: What lies beneath. J. Orthop. Res. 2018, 36, 1818–1825. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Hayashi, D.; Roemer, F.W.; Felson, D.T.; Guermazi, A. Magnetic resonance imaging of subchondral bone marrow lesions in association with osteoarthritis. Semin. Arthritis Rheum. 2012, 42, 105–118. [Google Scholar] [CrossRef] [PubMed]
- Roemer, F.W.; Guermazi, A.; Javaid, M.K.; Lynch, J.A.; Niu, J.; Zhang, Y.; Felson, D.T.; Lewis, C.E.; Torner, J.; Nevitt, M.C.; et al. Change in MRI-detected subchondral bone marrow lesions is associated with cartilage loss: The MOST Study. A longitudinal multicentre study of knee osteoarthritis. Ann. Rheum. Dis. 2009, 68, 1461–1465. [Google Scholar] [CrossRef]
- Hunter, D.J.; Zhang, Y.; Niu, J.; Goggins, J.; Amin, S.; LaValley, M.P.; Guermazi, A.; Genant, H.; Gale, D.; Felson, D.T. Increase in bone marrow lesions associated with cartilage loss: A longitudinal magnetic resonance imaging study of knee osteoarthritis. Arthritis Rheum. 2006, 54, 1529–1535. [Google Scholar] [CrossRef]
- Yusuf, E.; Kortekaas, M.C.; Watt, I.; Huizinga, T.W.; Kloppenburg, M. Do knee abnormalities visualised on MRI explain knee pain in knee osteoarthritis? A systematic review. Ann. Rheum. Dis. 2011, 70, 60–67. [Google Scholar] [CrossRef]
- Felson, D.T.; Chaisson, C.E.; Hill, C.L.; Totterman, S.M.; Gale, M.E.; Skinner, K.M.; Kazis, L.; Gale, D.R. The association of bone marrow lesions with pain in knee osteoarthritis. Ann. Intern. Med. 2001, 134, 541–549. [Google Scholar] [CrossRef]
- Felson, D.T.; Niu, J.; Guermazi, A.; Roemer, F.; Aliabadi, P.; Clancy, M.; Torner, J.; Lewis, C.E.; Nevitt, M.C. Correlation of the development of knee pain with enlarging bone marrow lesions on magnetic resonance imaging. Arthritis Rheum. 2007, 56, 2986–2992. [Google Scholar] [CrossRef]
- Hunter, D.J.; Gerstenfeld, L.; Bishop, G.; Davis, A.D.; Mason, Z.D.; Einhorn, T.A.; Maciewicz, R.A.; Newham, P.; Foster, M.; Jackson, S.; et al. Bone marrow lesions from osteoarthritis knees are characterized by sclerotic bone that is less well mineralized. Arthritis Res. Ther. 2009, 11, R11. [Google Scholar] [CrossRef]
- Sowers, M.; Karvonen-Gutierrez, C.A.; Jacobson, J.A.; Jiang, Y.; Yosef, M. Associations of anatomical measures from MRI with radiographically defined knee osteoarthritis score, pain, and physical functioning. J. Bone Jt. Surgery. 2011, 93, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Mastbergen, S.C.; Lafeber, F.P. Changes in subchondral bone early in the development of osteoarthritis. Arthritis Rheum. 2011, 63, 2561–2563. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, E.F.; Ringe, J.D. Bone marrow lesions: A universal bone response to injury? Rheumatol. Int. 2012, 32, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Tarantino, U.; Greggi, C.; Cariati, I.; Caldora, P.; Capanna, R.; Capone, A.; Civinini, R.; Colagrande, S.; De Biase, P.; Falez, F.; et al. Bone Marrow Edema: Overview of Etiology and Treatment Strategies. J. Bone Jt. Surgery. 2022, 104, 189–200. [Google Scholar] [CrossRef]
- Sugano, N.; Kubo, T.; Takaoka, K.; Ohzono, K.; Hotokebuchi, T.; Matsumoto, T.; Igarashi, H.; Ninomiya, S. Diagnostic criteria for non-traumatic osteonecrosis of the femoral head. A multicentre study. J. Bone Jt. Surg. 1999, 81, 590–595. [Google Scholar] [CrossRef]
- Boutry, N.; Paul, C.; Leroy, X.; Fredoux, D.; Migaud, H.; Cotten, A. Rapidly destructive osteoarthritis of the hip: MR imaging findings. AJR. Am. J. Roentgenol. 2002, 179, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, W.; Itoi, E.; Yamada, S. Early MRI findings of rapidly destructive coxarthrosis. Skelet. Radiol. 2002, 31, 35–38. [Google Scholar] [CrossRef]
- Vande Berg, B.C.; Lecouvet, F.E.; Koutaissoff, S.; Simoni, P.; Malghem, J. Bone marrow edema of the femoral head and transient osteoporosis of the hip. Eur. J. Radiol. 2008, 67, 68–77. [Google Scholar] [CrossRef]
- Taljanovic, M.S.; Graham, A.R.; Benjamin, J.B.; Gmitro, A.F.; Krupinski, E.A.; Schwartz, S.A.; Hunter, T.B.; Resnick, D.L. Bone marrow edema pattern in advanced hip osteoarthritis: Quantitative assessment with magnetic resonance imaging and correlation with clinical examination, radiographic findings, and histopathology. Skelet. Radiol. 2008, 37, 423–431. [Google Scholar] [CrossRef]
- Brimmo, O.A.; Bozynski, C.C.; Cook, C.R.; Kuroki, K.; Sherman, S.L.; Pfeiffer, F.M.; Stoker, A.M.; Cook, J.L. Subchondroplasty for the treatment of post-traumatic bone marrow lesions of the medial femoral condyle in a pre-clinical canine model. J. Orthop. Res. 2018, 36, 2709–2717. [Google Scholar] [CrossRef]
- Bajammal, S.S.; Zlowodzki, M.; Lelwica, A.; Tornetta, P., III; Einhorn, T.A.; Buckley, R.; Leighton, R.; Russell, T.A.; Larsson, S.; Bhandari, M. The use of calcium phosphate bone cement in fracture treatment. A meta-analysis of randomized trials. J. Bone Jt. Surg. 2008, 90, 1186–1196. [Google Scholar] [CrossRef]
- Kim, J.K.; Kim, N.K. Curettage and calcium phosphate bone cement injection for the treatment of enchondroma of the finger. Hand Surg. 2012, 17, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Evaniew, N.; Tan, V.; Parasu, N.; Jurriaans, E.; Finlay, K.; Deheshi, B.; Ghert, M. Use of a calcium sulfate-calcium phosphate synthetic bone graft composite in the surgical management of primary bone tumors. Orthopedics 2013, 36, e216–e222. [Google Scholar] [CrossRef] [PubMed]
- Winge, M.I.; Reikerås, O.; Røkkum, M. Calcium phosphate bone cement: A possible alternative to autologous bone graft. A radiological and biomechanical comparison in rat tibial bone. Arch. Orthop. Trauma Surg. 2011, 131, 1035–1041. [Google Scholar] [CrossRef] [PubMed]
- Akhavan, S.; Martinkovich, S.C.; Kasik, C.; DeMeo, P.J. Bone Marrow Edema, Clinical Significance, and Treatment Options: A Review. J. Am. Acad. Orthop. Surg. 2020, 28, e888–e899. [Google Scholar] [CrossRef]
- Welch, R.D.; Zhang, H.; Bronson, D.G. Experimental tibial plateau fractures augmented with calcium phosphate cement or autologous bone graft. J. Bone Jt. Surg. 2003, 85, 222–231. [Google Scholar] [CrossRef]
- Oliver, H.A.; Bozynski, C.C.; Cook, C.R.; Kuroki, K.; Sherman, S.L.; Stoker, A.M.; Cook, J.L. Enhanced Subchondroplasty Treatment for Post-Traumatic Cartilage and Subchondral Bone Marrow Lesions in a Canine Model. J. Orthop. Res. 2020, 38, 740–746. [Google Scholar] [CrossRef]
- Chua, K.; Kang, J.Y.B.; Ng, F.D.J.; Pang, H.N.; Lie, D.T.T.; Silva, A.; Chang, P.C.C. Subchondroplasty for Bone Marrow Lesions in the Arthritic Knee Results in Pain Relief and Improvement in Function. J. Knee Surg. 2021, 34, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Nairn, L.N.; Subramaniam, M.; Ekhtiari, S.; Axelrod, D.E.; Grant, J.A.; Khan, M. Safety and early results of Subchondroplasty® for the treatment of bone marrow lesions in osteoarthritis: A systematic review. Knee Surg. Sport. Traumatol. Arthrosc. 2021, 29, 3599–3607. [Google Scholar] [CrossRef]
- Krebs, N.M.; Kehoe, J.L.; Van Wagner, M.J.; Rios-Bedoya, C. The Efficacy of Subchondroplasty for the Treatment of Knee Pain Associated with Bone Marrow Lesions. Spartan Med. Res. J. 2020, 4, 11767. [Google Scholar] [CrossRef]
- Previtali, D.; Merli, G.; Di Laura Frattura, G.; Candrian, C.; Zaffagnini, S.; Filardo, G. The Long-Lasting Effects of “Placebo Injections” in Knee Osteoarthritis: A Meta-Analysis. Cartilage 2021, 13 (Suppl. S1), 185S–196S. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, D.; McGee, A.; Strauss, E.; Youm, T.; Jazrawi, L. Subchondral Calcium Phosphate is Ineffective for Bone Marrow Edema Lesions in Adults With Advanced Osteoarthritis. Clin. Orthop. Relat. Res. 2015, 473, 2334–2342. [Google Scholar] [CrossRef] [PubMed]
- Nevalainen, M.T.; Sharkey, P.F.; Cohen, S.B.; Roedl, J.B.; Zoga, A.C.; Morrison, W.B. MRI findings of subchondroplasty of the knee: A two-case report. Clin. Imaging 2016, 40, 241–243. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.Y.; O’Malley, M.J.; Matsen Ko, L.J.; Cohen, S.B.; Sharkey, P.F. Knee Arthroplasty After Subchondroplasty: Early Results, Complications, and Technical Challenges. J. Arthroplast. 2016, 31, 2188–2192. [Google Scholar] [CrossRef]
- Dold, A.; Perretta, D.; Youm, T. Osteomyelitis After Calcium Phosphate Subchondroplasty A Case Report. Bull. Hosp. Jt. Dis. 2017, 75, 282–285. [Google Scholar]
- Betzler, B.K.; Chee, Y.J.; Bin Abd Razak, H.R. Intraosseous Injections Are Safe And Effective in Knee Osteoarthritis: A Systematic Review. Arthrosc. Sport. Med. Rehabil. 2021, 3, e1557–e1567. [Google Scholar] [CrossRef] [PubMed]
- Colon, D.A.; Yoon, B.V.; Russell, T.A.; Cammisa, F.P.; Abjornson, C. Assessment of the injection behavior of commercially available bone BSMs for Subchondroplasty® procedures. Knee 2015, 22, 597–603. [Google Scholar] [CrossRef]









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fokter, S.K.; Kuhta, M.; Hojnik, M.; Ledinek, Ž.; Kostanjšek, R. Tissue Integration of Calcium Phosphate Compound after Subchondroplasty: 4-Year Follow-Up in a 76-Year-Old Female Patient. Bioengineering 2023, 10, 208. https://doi.org/10.3390/bioengineering10020208
Fokter SK, Kuhta M, Hojnik M, Ledinek Ž, Kostanjšek R. Tissue Integration of Calcium Phosphate Compound after Subchondroplasty: 4-Year Follow-Up in a 76-Year-Old Female Patient. Bioengineering. 2023; 10(2):208. https://doi.org/10.3390/bioengineering10020208
Chicago/Turabian StyleFokter, Samo K., Matevž Kuhta, Marko Hojnik, Živa Ledinek, and Rok Kostanjšek. 2023. "Tissue Integration of Calcium Phosphate Compound after Subchondroplasty: 4-Year Follow-Up in a 76-Year-Old Female Patient" Bioengineering 10, no. 2: 208. https://doi.org/10.3390/bioengineering10020208
APA StyleFokter, S. K., Kuhta, M., Hojnik, M., Ledinek, Ž., & Kostanjšek, R. (2023). Tissue Integration of Calcium Phosphate Compound after Subchondroplasty: 4-Year Follow-Up in a 76-Year-Old Female Patient. Bioengineering, 10(2), 208. https://doi.org/10.3390/bioengineering10020208