

A New Conformal Penetrating Heating Strategy for Atherosclerotic Plaque


Abstract
1. Introduction
2. Materials and Methods
2.1. Tissue-Mimicking Phantom Heating Experiment
2.1.1. Experimental Setup
2.1.2. Heating Conditions
2.2. Numerical Simulation
2.2.1. Model Geometry
2.2.2. Mathematical Modeling
2.3. Optimal Heating Strategy
3. Results
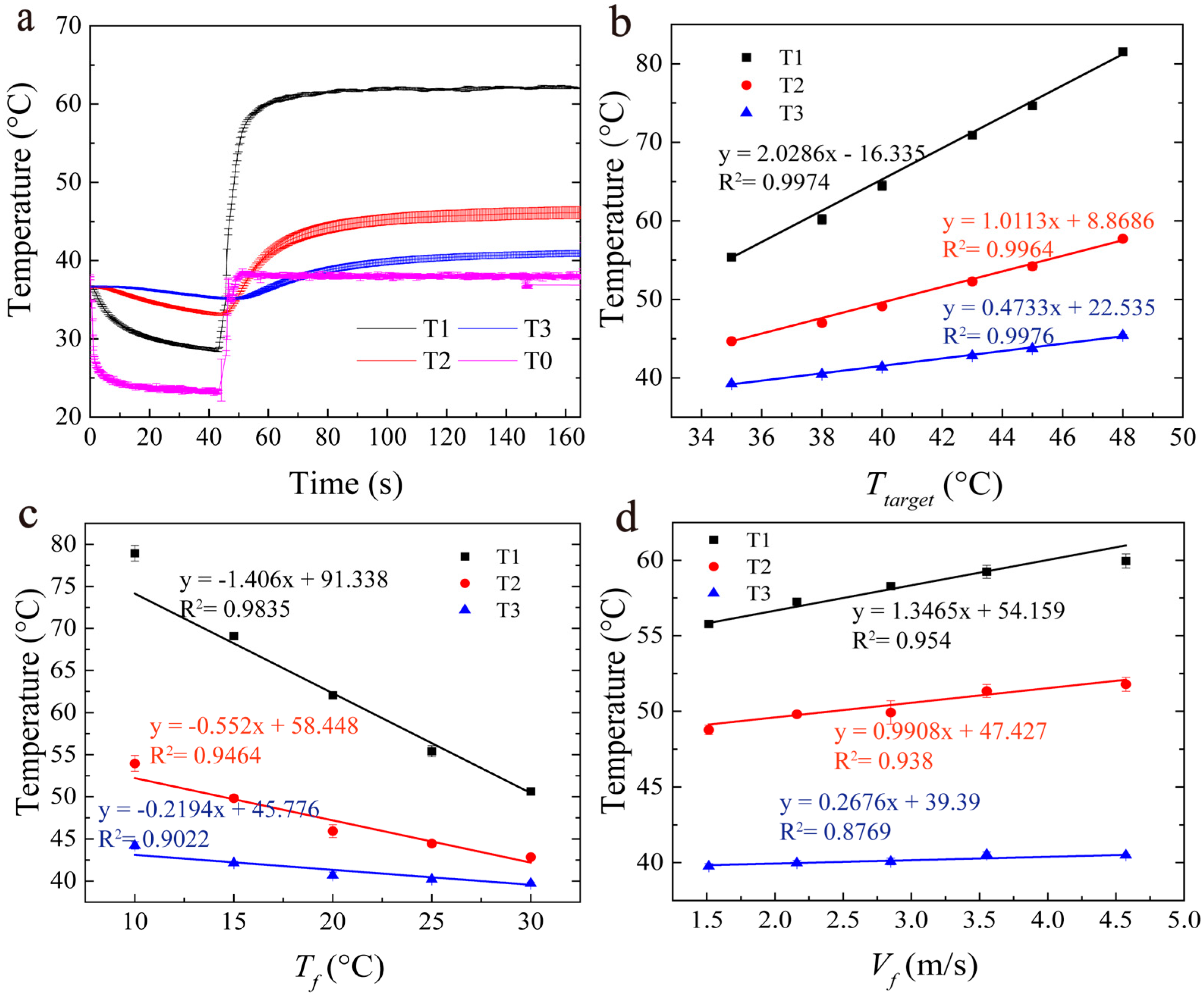
3.1. Influence of Parameters Based on Experiments
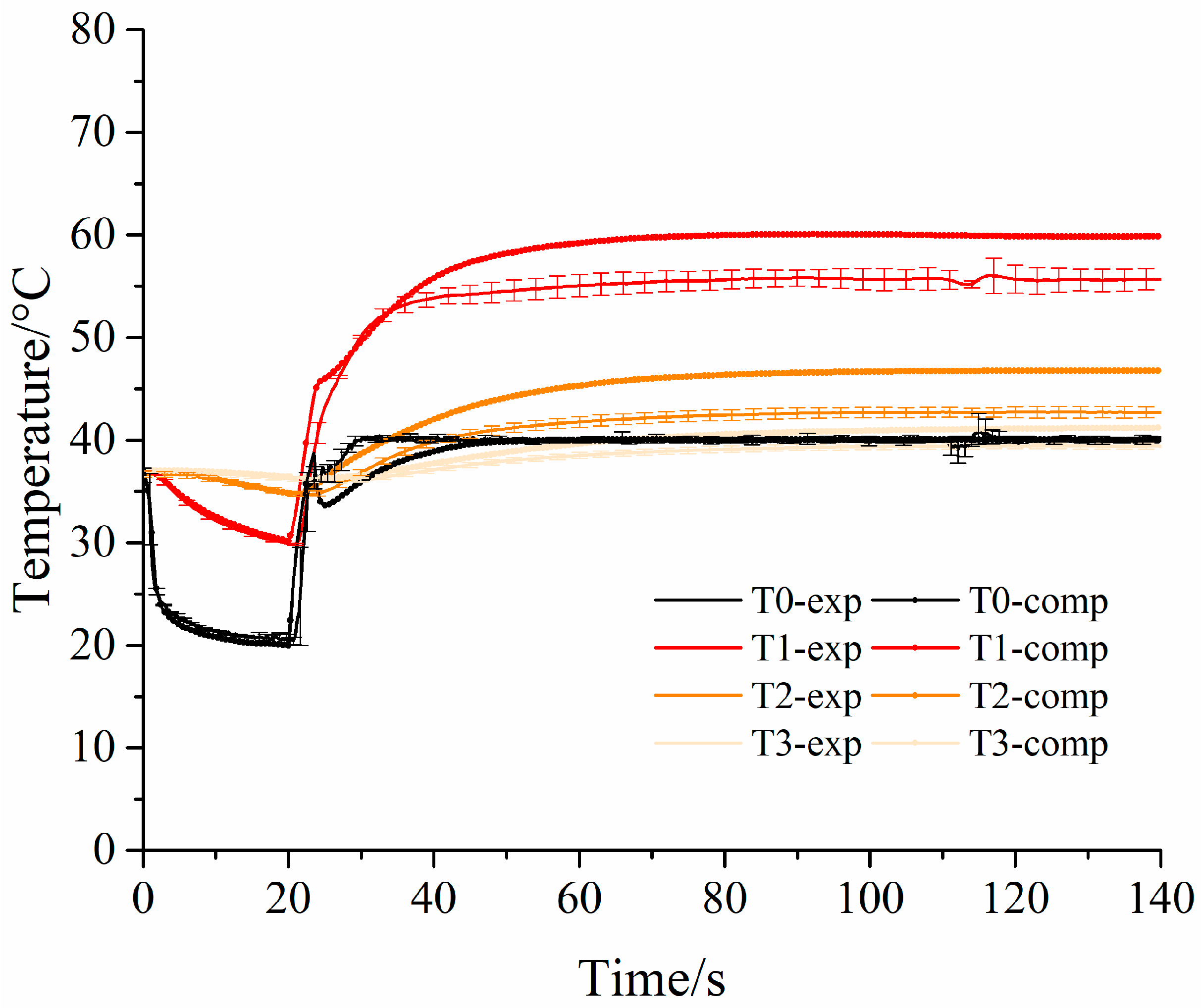
3.2. Numerical Modeling
Numerical Results
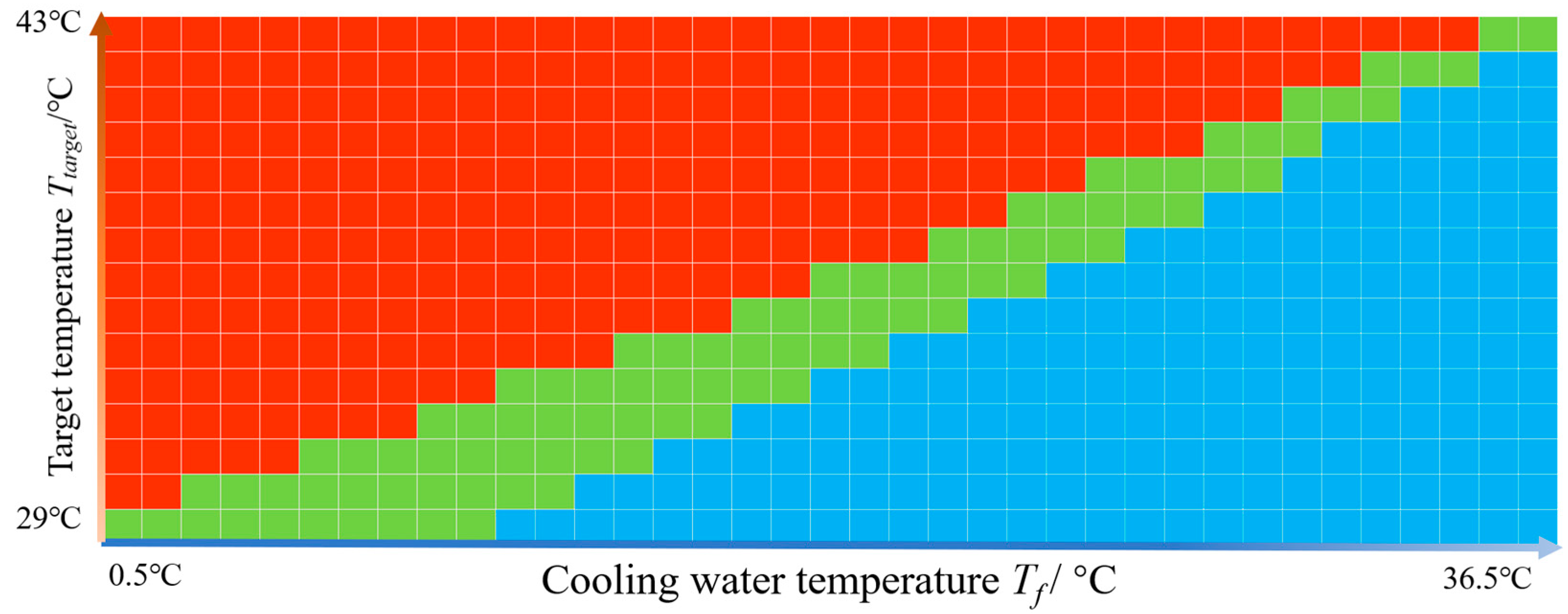
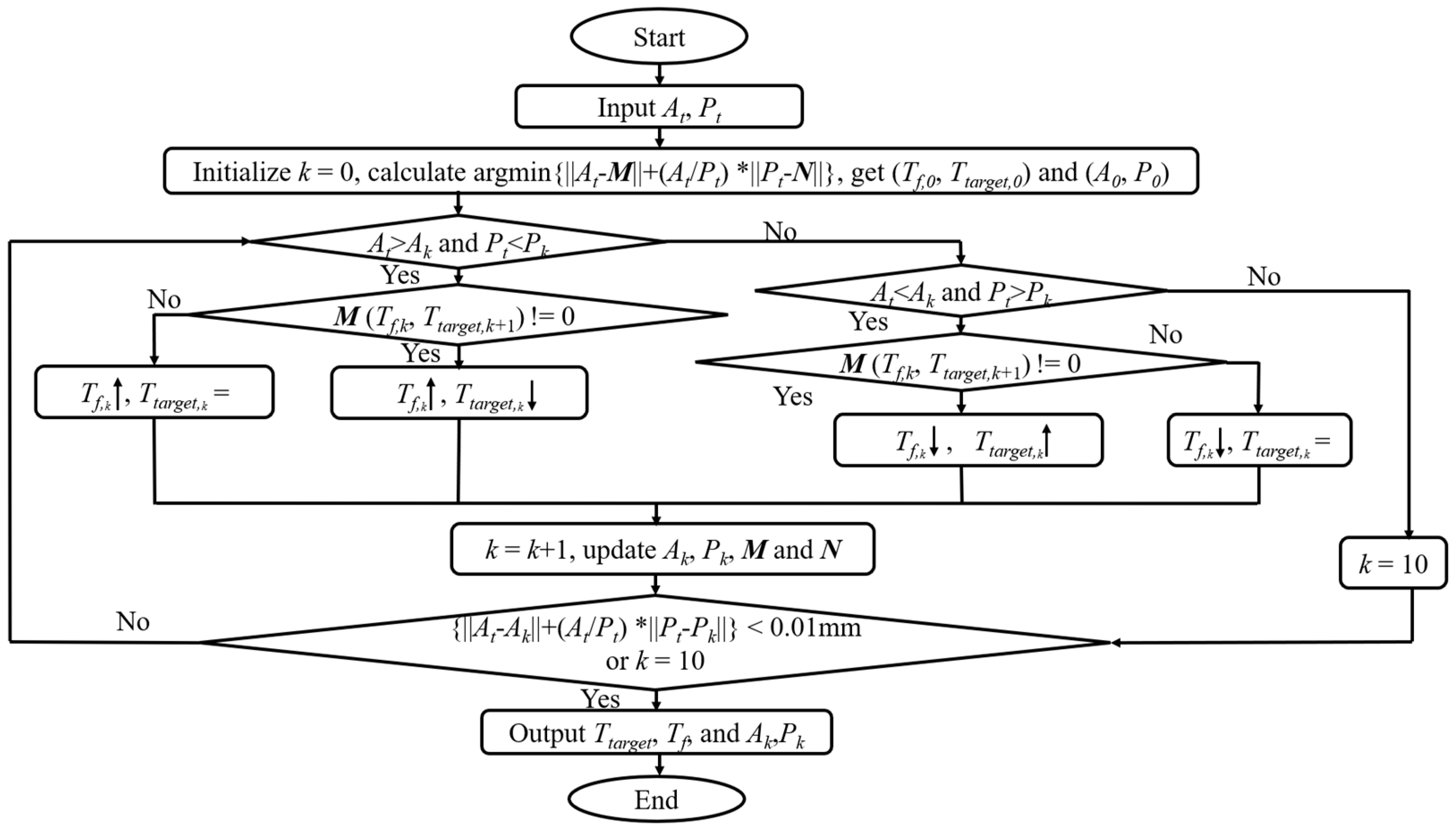
3.3. Algorithm of Optimal Heating Strategy
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| RF | radiofrequency |
| PID | proportional-integral-derivative |
| Ttarget | the target temperature |
| Tf | the temperature of cooling water |
| Vf | the velocity of cooling water |
| PTA | percutaneous transluminal angioplasty |
| SMCs | smooth muscle cells |
| IMT | intima–media thickness |
| DAQ | data acquisition card |
| TC0, TC1, TC2, and TC3 | thermocouples on points TC0, TC1, TC2, and TC3 |
| T0, T1, T2, and T3 | temperatures measured by thermocouples TC0, TC1, TC2, and TC3 |
| SAR | specific absorption rate |
| A | ablation depth, unit: millimeter |
| P | protection depth, unit: millimeter |
| Ak | calculated ablation depth, unit: millimeter |
| Pk | calculated protection depth, unit: millimeter |
Appendix A




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Domain | Dimensions | Number of Elements or Nodes | Size of Elements (Unit: mm) | ||
|---|---|---|---|---|---|
| Elements | Nodes | Minimum | Maximum | ||
| Copper electrodes | 3 | 44,458 | 15,355 | 0.005 | 0.02 |
| Polyimide catheter | 3 | 141,974 | 32,726 | 0.2 | 2.75 |
| Refined region (Phantom) | 3 | 162,247 | 32,143 | 0.075 | 1 |
| Coarse region (Phantom) | 3 | 32,146 | 7463 | 2.7 | 15 |


References
- Bauters, C.; Meurice, T.; Hamon, M.; McFadde, E.; Lablanche, J.-M.; Bertrand, M.E. Mechanisms and prevention of restenosis: From experimental models to clinical practice. Cardiovasc. Res. 1996, 31, 835–846. [Google Scholar] [CrossRef] [PubMed]
- Byrne, R.A.; Joner, M.; Kastrati, A. Stent thrombosis and restenosis: What have we learned and where are we going? The Andreas Gruntzig Lecture ESC 2014. Eur. Heart J. 2015, 36, 3320–3331. [Google Scholar] [CrossRef]
- Libby, P.; Buring, J.E.; Badimon, L.; Hansson, G.K.; Deanfield, J.; Bittencourt, M.S.; Tokgozoglu, L.; Lewis, E.F. Atherosclerosis. Nat. Rev. Dis. Prim. 2019, 5, 56. [Google Scholar] [CrossRef]
- Perkins, L.E.L.; Rippy, M.K. Balloons and Stents and Scaffolds: Preclinical Evaluation of Interventional Devices for Occlusive Arterial Disease. Toxicol. Pathol. 2019, 47, 297–310. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, F.; Finn, A.V.; Yazdani, S.K.; Nakano, M.; Kolodgie, F.D.; Virmani, R. The importance of the endothelium in atherothrombosis and coronary stenting. Nat. Rev. Cardiol. 2012, 9, 439–453. [Google Scholar]
- Cosedis Nielsen, J.; Johannessen, A.; Raatikainen, P.; Hindricks, G.; Walfridsson, H.; Kongstad, O.; Pehrson, S.; Englund, A.; Hartikainen, J.; Mortensen, L.S.; et al. Radiofrequency ablation as initial therapy in paroxysmal atrial fibrillation. N. Engl. J. Med. 2012, 367, 1587–1595. [Google Scholar] [CrossRef] [PubMed]
- Chu, K.F.; Dupuy, D.E. Thermal ablation of tumours: Biological mechanisms and advances in therapy. Nat. Rev. Cancer 2014, 14, 199–208. [Google Scholar] [CrossRef]
- Becker, G.J.; Lee, B.I.; Waller, B.F.; Barry, K.J.; Kaplan, J.; Connolly, R.; Dreesen, R.G.; Nardella, P. Radiofrequency balloon angioplasty. Rationale and proof of principle. Investig. Radiol. 1988, 23, 810–817. [Google Scholar] [CrossRef]
- Grundfest, W.S.; Litvack, F.; Forrester, J.S.; Goldenberg, T.; Swan, H.J.; Morgenstern, L.; Fishbein, M.; McDermid, I.S.; Rider, D.M.; Pacala, T.J. Laser ablation of human atherosclerotic plaque without adjacent tissue injury. J. Am. Coll Cardiol. 1985, 5, 929–933. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, K.; Satake, S.; Ohira, H.; Ohtomo, K. Radiofrequency thermal balloon coronary angioplasty: A new device for successful percutaneous transluminal coronary angioplasty. J. Am. Coll. Cardiol. 1994, 23, 336–340. [Google Scholar] [CrossRef]
- Lee, B.I.; Becker, G.J.; Waller, B.F.; Barry, K.J.; Connolly, R.J.; Kaplan, J.; Shapiro, A.R.; Nardella, P.C. Thermal compression and molding of atherosclerotic vascular tissue with use of radiofrequency energy: Implications for radiofrequency balloon angioplasty. J. Am. Coll. Cardiol. 1989, 13, 1167–1175. [Google Scholar] [CrossRef] [PubMed]
- Steinkamp, H.J.; Wissgott, C.; Rademaker, J.; Scheinert, D.; Werk, M.; Settmacher, U.; Felix, R. Short (1–10 cm) superficial femoral artery occlusions: Results of treatment with excimer laser angioplasty. Cardiovasc. Interv.. Radiol. 2002, 25, 388–396. [Google Scholar] [CrossRef]
- Zhao, S.; Zou, J.; Wang, H.; Qin, J.; Lu, X.; Zhang, A.; Xu, L.X. A new radiofrequency balloon angioplasty device for atherosclerosis treatment. Biomed. Eng. Online 2020, 19, 44. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.; Zhang, K.; Zhao, S.; Zou, J.; Zhang, A.; Xu, L.X. An RF device for effective thermal treatment of atherosclerosis. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015. [Google Scholar]
- Buccheri, D.; Piraino, D.; Andolina, G.; Cortese, B. Understanding and managing in-stent restenosis: A review of clinical data, from pathogenesis to treatment. J. Thorac. Dis. 2016, 8, E1150–E1162. [Google Scholar] [CrossRef]
- Wang, Z.; Luo, H.; Coleman, S.; Cuschieri, A. Bicomponent Conformal Electrode for Radiofrequency Sequential Ablation and Circumferential Separation of Large Tumors in Solid Organs: Development and In Vitro Evaluation. IEEE Trans. Biomed. Eng. 2017, 64, 699–705. [Google Scholar]
- Audigier, C.; Kim, Y.; Ziegle, J.; Friebe, M.; Boctor, E.M.; Fei, B.; Linte, C.A. Conformal radiofrequency ablation to validate ultrasound thermometry. In Medical Imaging 2019: Image-Guided Procedures, Robotic Interventions, and Modeling; SPIE: Washington, DC, USA, 2019. [Google Scholar]
- Wendelhag, I.; Wiklund, O.; Wikstrand, J. Atherosclerotic changes in the femoral and carotid arteries in familial hypercholesterolemia. Ultrasonographic assessment of intima-media thickness and plaque occurrence. Arterioscler. Thromb. A J. Vasc. Biol. 1993, 13, 1404–1411. [Google Scholar] [CrossRef]
- Enderle, M.D.; Schroeder, S.; Ossen, R.; Meisner, C.; Baumbach, A.; Haering, H.U.; Karsch, K.R.; Pfohl, M. Comparison of peripheral endothelial dysfunction and intimal media thickness in patients with suspected coronary artery disease. Heart 1998, 80, 349–354. [Google Scholar] [CrossRef]
- Meng, L.B.; Yu, Z.M.; Guo, P.; Wang, Q.Q.; Qi, R.M.; Shan, M.J.; Lv, J.; Gong, T. Neutrophils and neutrophil-lymphocyte ratio: Inflammatory markers associated with intimal-media thickness of atherosclerosis. Thromb. Res. 2018, 170, 45–52. [Google Scholar] [CrossRef]
- Tarkin, J.M.; Dweck, M.R.; Evans, N.R.; Takx, R.A.; Brown, A.J.; Tawakol, A.; Fayad, Z.A.; Rudd, J.H. Imaging Atherosclerosis. Circ. Res. 2016, 118, 750–769. [Google Scholar] [CrossRef]
- de Groot, E.; van Leuven, S.I.; Duivenvoorden, R.; Meuwese, M.C.; Akdim, F.; Bots, M.L.; Kastelein, J.J. Measurement of carotid intima-media thickness to assess progression and regression of atherosclerosis. Nat. Clin. Pract. Cardiovasc. Med. 2008, 5, 280–288. [Google Scholar] [CrossRef] [PubMed]
- Mohler, E.R.; Sibley, A.A., 3rd; Schultz, S.M.; Zhang, Z.; Sehgal, C.M. High-frequency ultrasound for evaluation of intimal thickness. J. Am. Soc. Echocardiogr. 2009, 22, 1129–1133. [Google Scholar] [CrossRef]
- Shinozuka, M.; Shimazaki, N.; Ogawa, E.; Machida, N.; Arai, T. Acute cell death rate of vascular smooth muscle cells during or after short heating up to 20 s ranging 50 to 60 degrees C as a basic study of thermal angioplasty. In Optical Interactions with Tissue and Cells Xxv; and Terahertz for Biomedical Applications; Jansen, E.D., Thomas, R.J., Wilmink, G.J., Ibey, B.L., Eds.; SPIE: Washington, DC, USA.
- Brasselet, C.; Durand, E.; Addad, F.; Vitry, F.; Chatellier, G.; Demerens, C.; Lemitre, M.; Garnotel, R.; Urbain, D.; Bruneval, P.; et al. Effect of local heating on restenosis and in-stent neointimal hyperplasia in the atherosclerotic rabbit model: A dose-ranging study. Eur. Heart J. 2008, 29, 402–412. [Google Scholar] [CrossRef]
- Zhu, L.; Xu, L.X. Evaluation of the effectiveness of transurethral radio frequency hyperthermia in the canine prostate: Temperature distribution analysis. J. Biomech. Eng.-Trans. ASME 1999, 121, 584–590. [Google Scholar] [CrossRef]
- Zou, K.; Zou, J.; Wang, Y.; Zhang, A. Design of Real-Time Temperature Monitoring and Control System for Multimodal Ablation. J. Shanghai Jiaotong Univ. (Sci.) 2022, 27, 535–542. [Google Scholar] [CrossRef]
- Hodges, T.C.; Detmer, P.R.; Dawson, D.L.; Bergelin, R.O.; Beach, K.W.; Hatsukami, T.S.; Zierler, B.K.; Isaacson, J.A.; Strandness, D.E., Jr. Ultrasound determination of total arterial wall thickness. J. Vasc. Surg. 1994, 19, 745–753. [Google Scholar] [CrossRef]
- Bergman, T.L.; Lavine, A.S.; Incropera, F.P.; DeWitt, D.P. Fundamentals of Heat and Mass Transfer, 8th ed.; Wiley: New York, NY, USA, 2018. [Google Scholar]
- van Erven, L.; Velema, E.; Bos, A.N.; Post, M.J.; Borst, C. Thrombogenicity and intimal hyperplasia after conventional and thermal balloon dilation in normal rabbit iliac arteries. J. Vasc. Res. 1992, 29, 426–434. [Google Scholar] [CrossRef]
- Iasiello, M.; Andreozzi, A.; Bianco, N.; Vafai, K. The porous media theory applied to radiofrequency catheter ablation. Int. J. Numer. Methods Heat Fluid Flow 2020, 30, 2669–2681. [Google Scholar] [CrossRef]
- Iasiello, M.; Vafai, K.; Andreozzi, A.; Bianco, N. Hypo-and hyperthermia effects on LDL deposition in a curved artery. Comput. Therm. Sci. Int. J. 2019, 11, 95–103. [Google Scholar] [CrossRef]
- Ortega-Palacios, R.; Trujillo-Romero, C.J.; Cepeda-Rubio, M.F.J.; Leija, L.; Vera Hernández, A. Heat Transfer Study in Breast Tumor Phantom during Microwave Ablation: Modeling and Experimental Results for Three Different Antennas. Electronics 2020, 9, 535. [Google Scholar] [CrossRef]
- Slager, C.J.; Phaff, A.C.; Essed, C.E.; Bom, N.; Schuurbiers, J.C.; Serruys, P.W. Electrical impedance of layered atherosclerotic plaques on human aortas. IEEE Trans. Bio-Med. Eng. 1992, 39, 411–419. [Google Scholar]
- Boulanger, L. Observations on variations in electrical conductivity of pure demineralized water: Modification (“activation”) of conductivity by low-frequency, low-level alternativing electric fields. Int. J. Biometeorol. 1998, 41, 137–140. [Google Scholar] [CrossRef]
- Kurabayashi, K.; Asheghi, M.; Touzelbaev, M.; Goodson, K.E. Measurement of the thermal conductivity anisotropy in polyimide films. J. Microelectromech. Syst. 1999, 8, 180–191. [Google Scholar] [CrossRef]
- Chen, R.K.; Than, K.D.; Park, P.; Shih, A.J. Thermoelectrical modeling of bipolar coagulation on posterior spinal artery in a porcine spinal surgery model. IEEE Trans. Biomed. Eng. 2014, 61, 182–188. [Google Scholar]
- Edgerton, R.H. Radial conductivity of arterial walls. Med. Biol. Eng. 1975, 13, 531–534. [Google Scholar] [CrossRef]
- Gentilal, N.; Miranda, P.C. Heat transfer during TTFields treatment: Influence of the uncertainty of the electric and thermal parameters on the predicted temperature distribution. Comput. Methods Programs Biomed. 2020, 196, 105706. [Google Scholar] [CrossRef]
- Skilton, M.R.; Boussel, L.; Bonnet, F.; Bernard, S.; Douek, P.C.; Moulin, P.; Serusclat, A. Carotid intima-media and adventitial thickening: Comparison of new and established ultrasound and magnetic resonance imaging techniques. Atherosclerosis 2011, 215, 405–410. [Google Scholar] [CrossRef]
- van den Munckhof, I.; Scholten, R.; Cable, N.T.; Hopman, M.T.E.; Green, D.J.; Thijssen, D.H.J. Impact of age and sex on carotid and peripheral arterial wall thickness in humans. Acta Physiol. 2012, 206, 220–228. [Google Scholar] [CrossRef]
- Li, Y.; Zeng, D.; Tan, J. Reconstruction of thermal field in target tissue during the therapy of high intensity focused ultrasound. Int. Commun. Heat Mass Transf. 2019, 108, 104352. [Google Scholar] [CrossRef]
- Paruch, M. Identification of the degree of tumor destruction on the basis of the Arrhenius integral using the evolutionary algorithm. Int. J. Therm. Sci. 2018, 130, 507–517. [Google Scholar] [CrossRef]
- Utsunomiya, M.; Hara, H.; Moroi, M.; Sugi, K.; Nakamura, M. Relationship between tissue characterization with 40 MHz intravascular ultrasound imaging and 64-slice computed tomography. J. Cardiol. 2011, 57, 297–302. [Google Scholar] [CrossRef]
- Helft, G.; Worthley, S.G.; Fuster, V.; Fayad, Z.A.; Zaman, A.G.; Corti, R.; Fallon, J.T.; Badimon, J.J. Progression and regression of atherosclerotic lesions: Monitoring with serial noninvasive magnetic resonance imaging. Circulation 2002, 105, 993–998. [Google Scholar] [CrossRef] [PubMed]











| Parameter | Tissue | Polyimide | Copper |
|---|---|---|---|
| Thermal conductivity, k (W/(mK)) | 0.60 + 0.0014(T − Tref) [13] | 0.25 [36] | 386.47 |
| Density, (kg/m3) | 998.2 | 2200 | 8935.4 |
| Specific heat capacity, (J/(kgK)) | 4183 | 1050 | 383.9 |
| Electrical conductivity, (S/m) | 0.33 + 0.0035(T − Tref)) [37,38] | 0 | 5.76 × 107 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.; Zhao, S.; Zou, J.; Zhang, A. A New Conformal Penetrating Heating Strategy for Atherosclerotic Plaque. Bioengineering 2023, 10, 162. https://doi.org/10.3390/bioengineering10020162
Wang H, Zhao S, Zou J, Zhang A. A New Conformal Penetrating Heating Strategy for Atherosclerotic Plaque. Bioengineering. 2023; 10(2):162. https://doi.org/10.3390/bioengineering10020162
Chicago/Turabian StyleWang, Hongying, Shiqing Zhao, Jincheng Zou, and Aili Zhang. 2023. "A New Conformal Penetrating Heating Strategy for Atherosclerotic Plaque" Bioengineering 10, no. 2: 162. https://doi.org/10.3390/bioengineering10020162
APA StyleWang, H., Zhao, S., Zou, J., & Zhang, A. (2023). A New Conformal Penetrating Heating Strategy for Atherosclerotic Plaque. Bioengineering, 10(2), 162. https://doi.org/10.3390/bioengineering10020162