
A Randomized Controlled Trial of the Efficacy of Systemic Enzymes and Probiotics in the Resolution of Post-COVID Fatigue


Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Ethics and Informed Consent
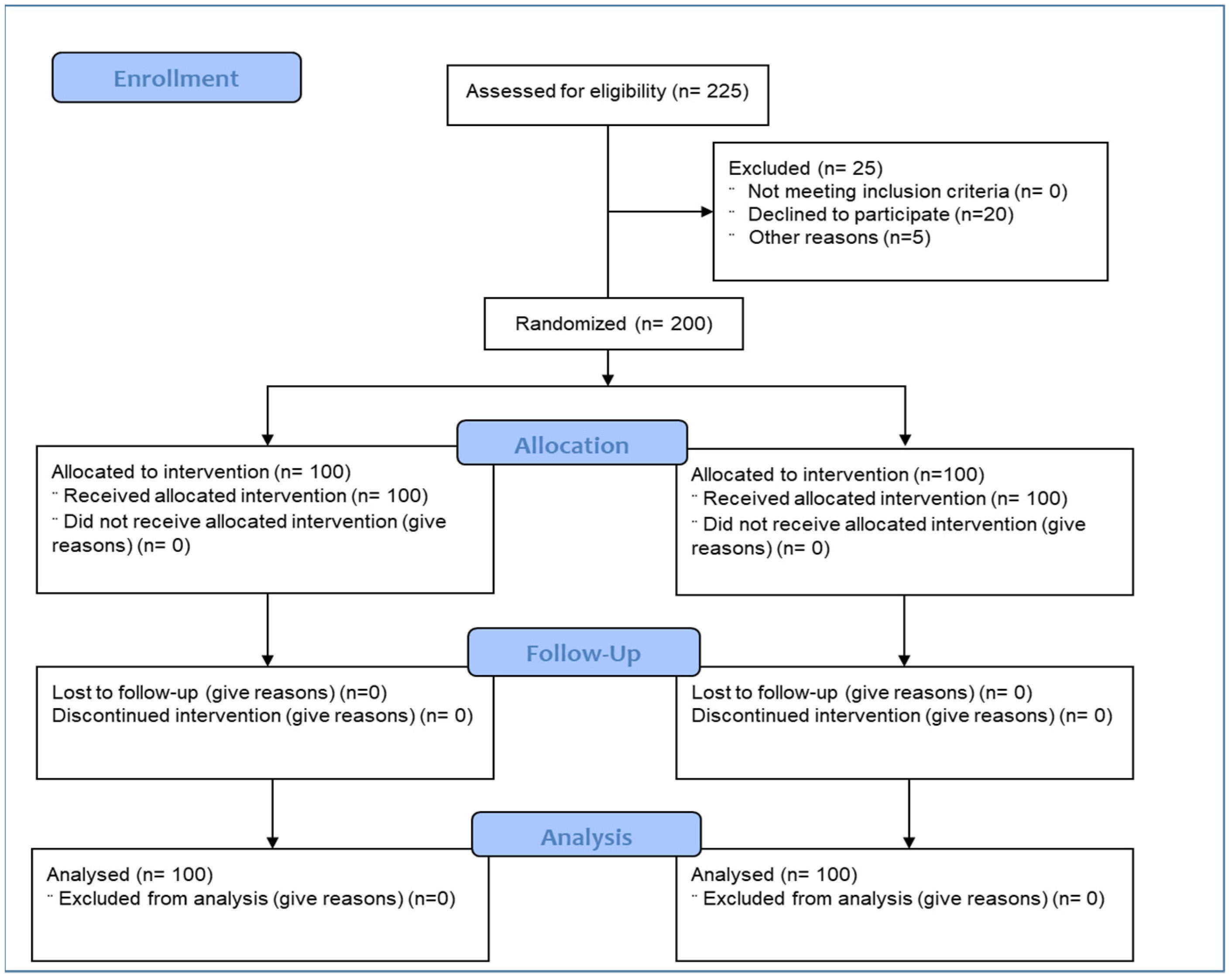
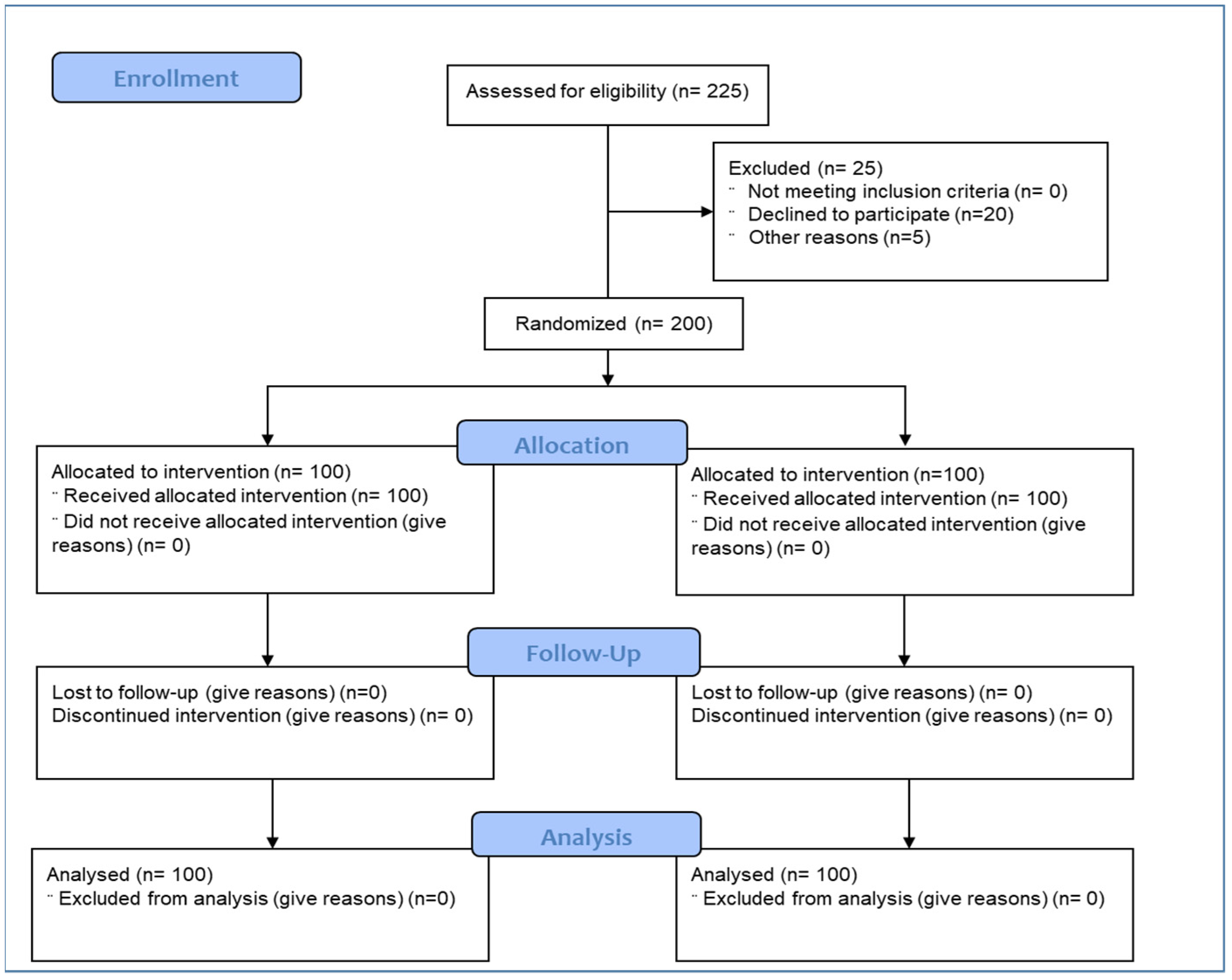
2.3. Selection of Study Subjects
2.3.1. Inclusion Criteria
2.3.2. Exclusion Criteria
2.4. Study Design, Randomization and Treatments
2.5. Endpoints: Efficacy and Safety Variables
2.6. Statistical Analysis
3. Results
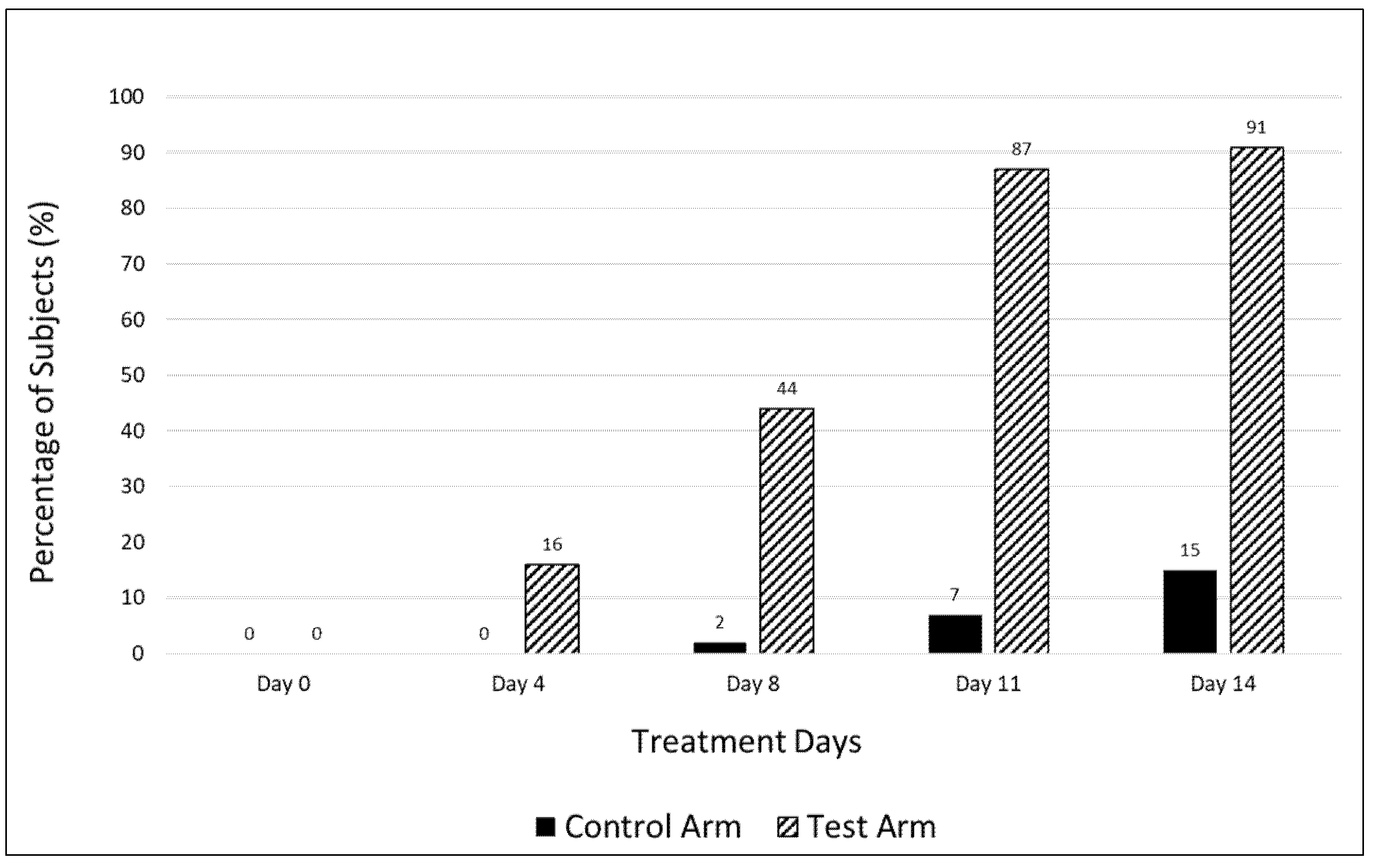
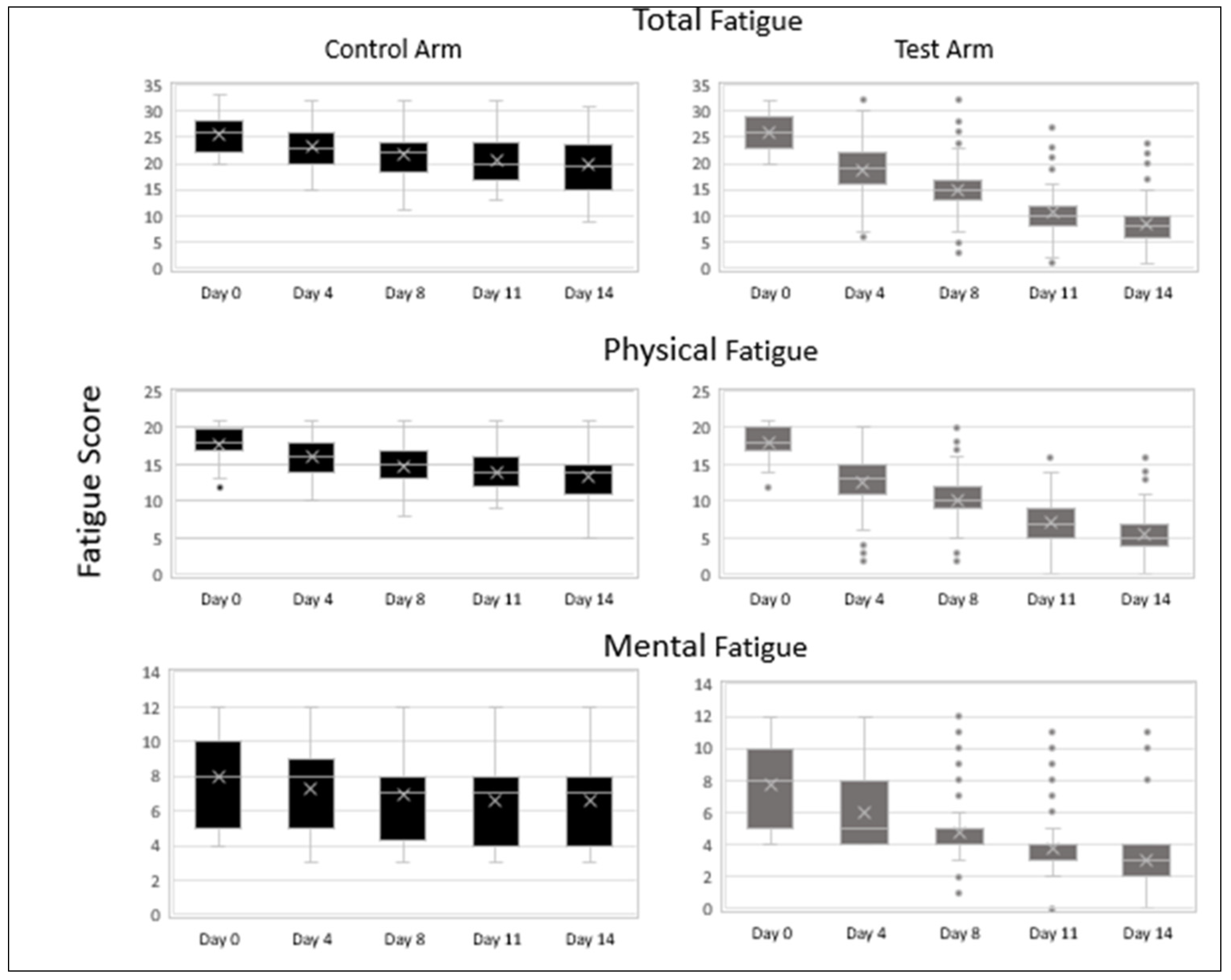
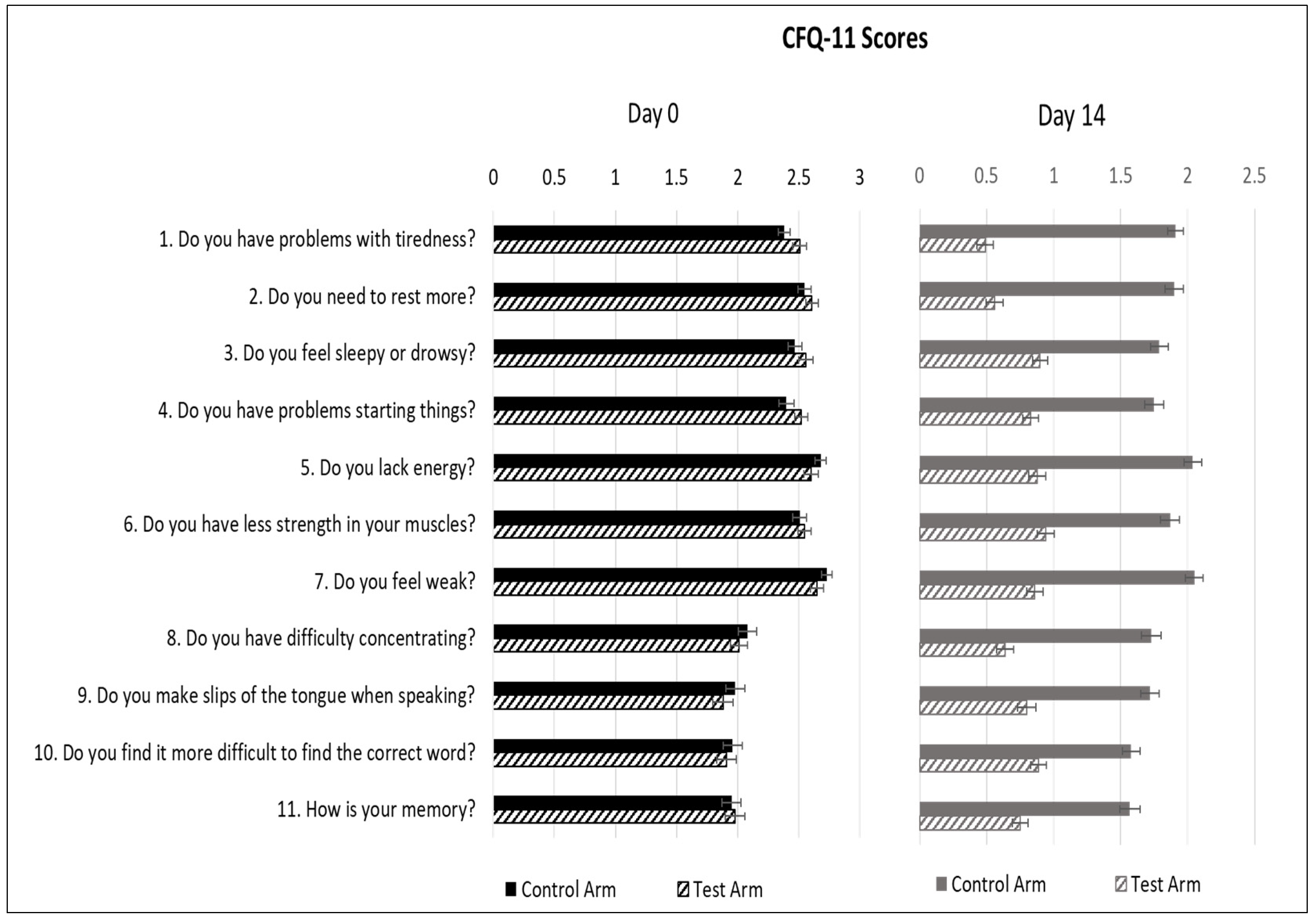
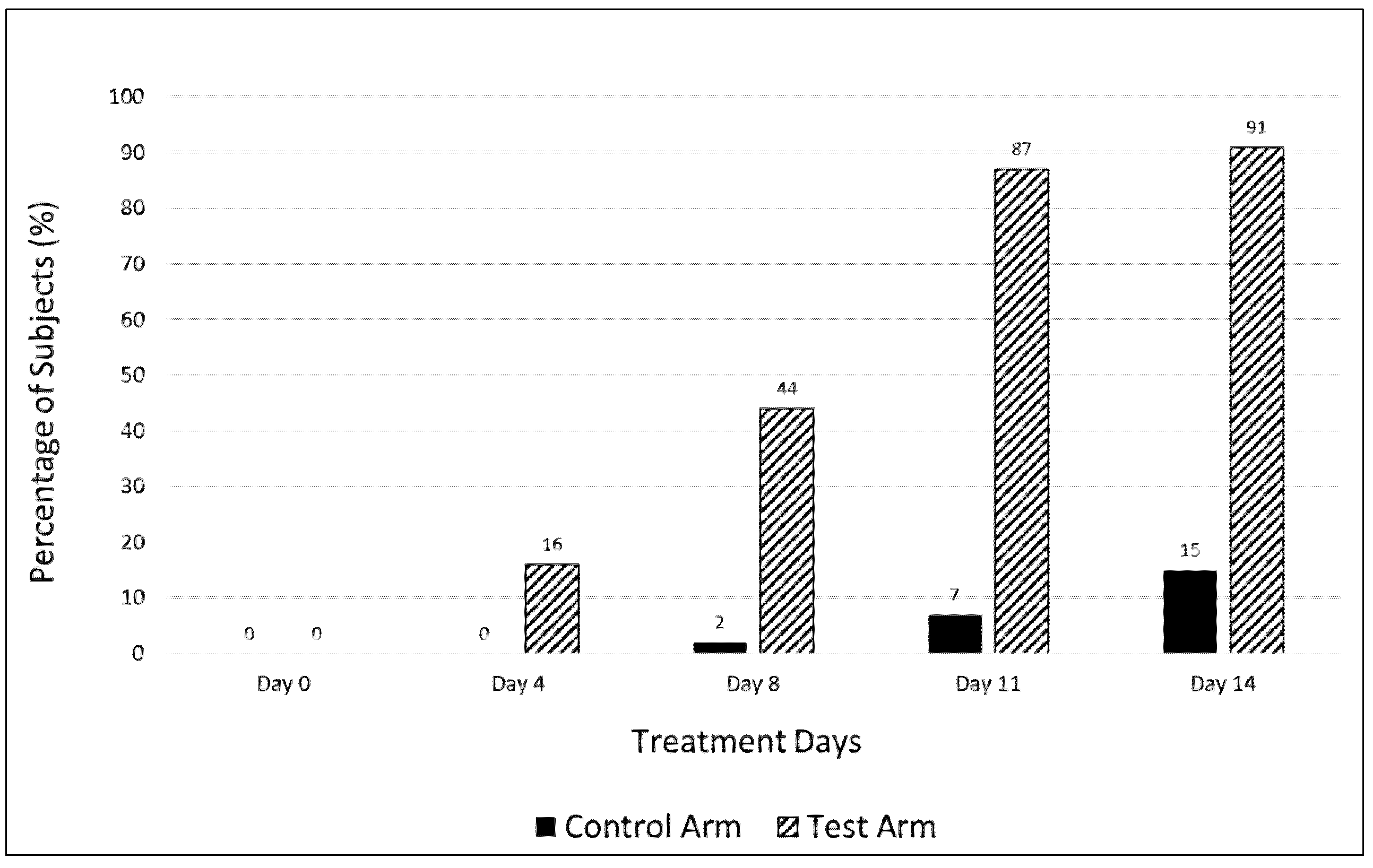
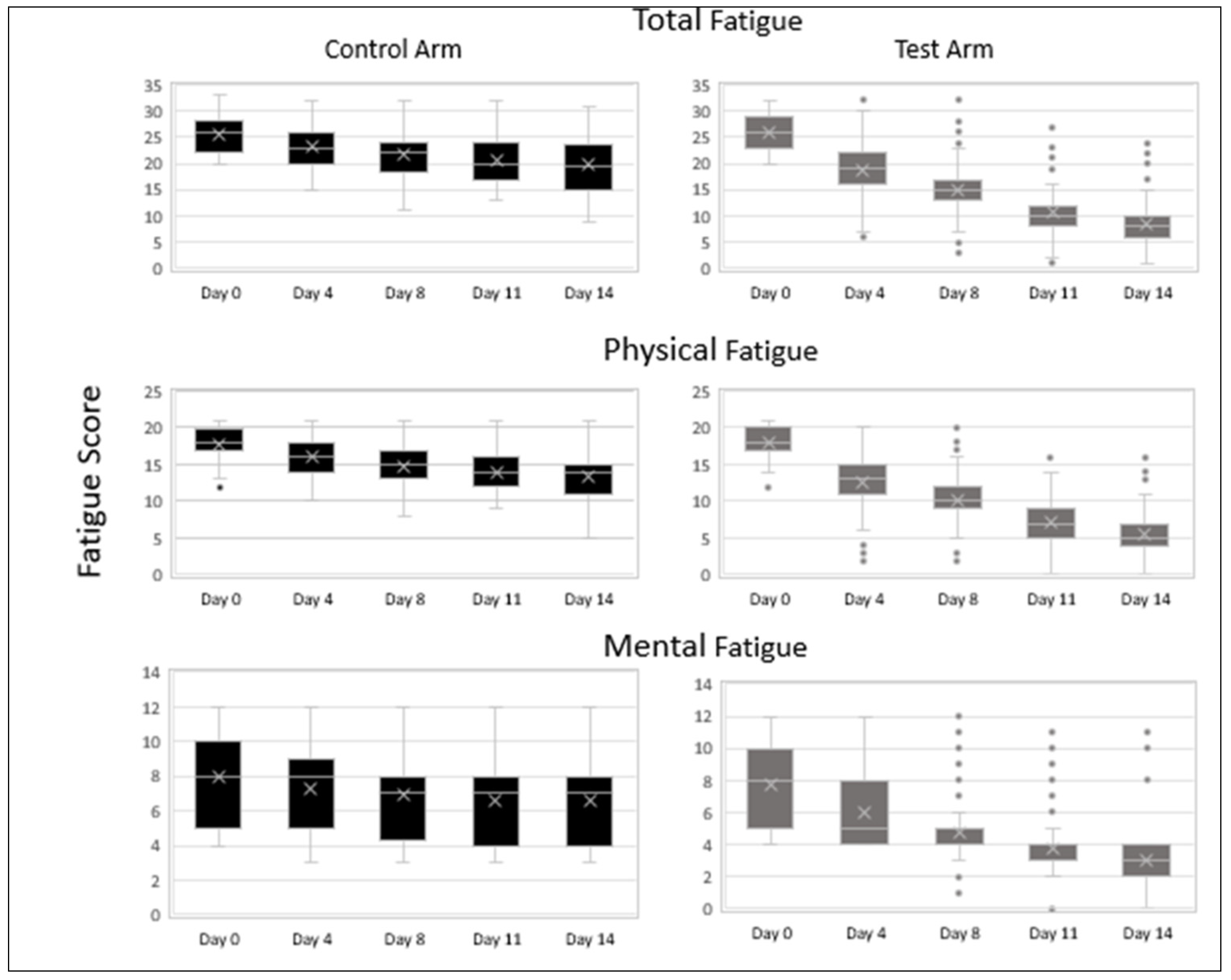
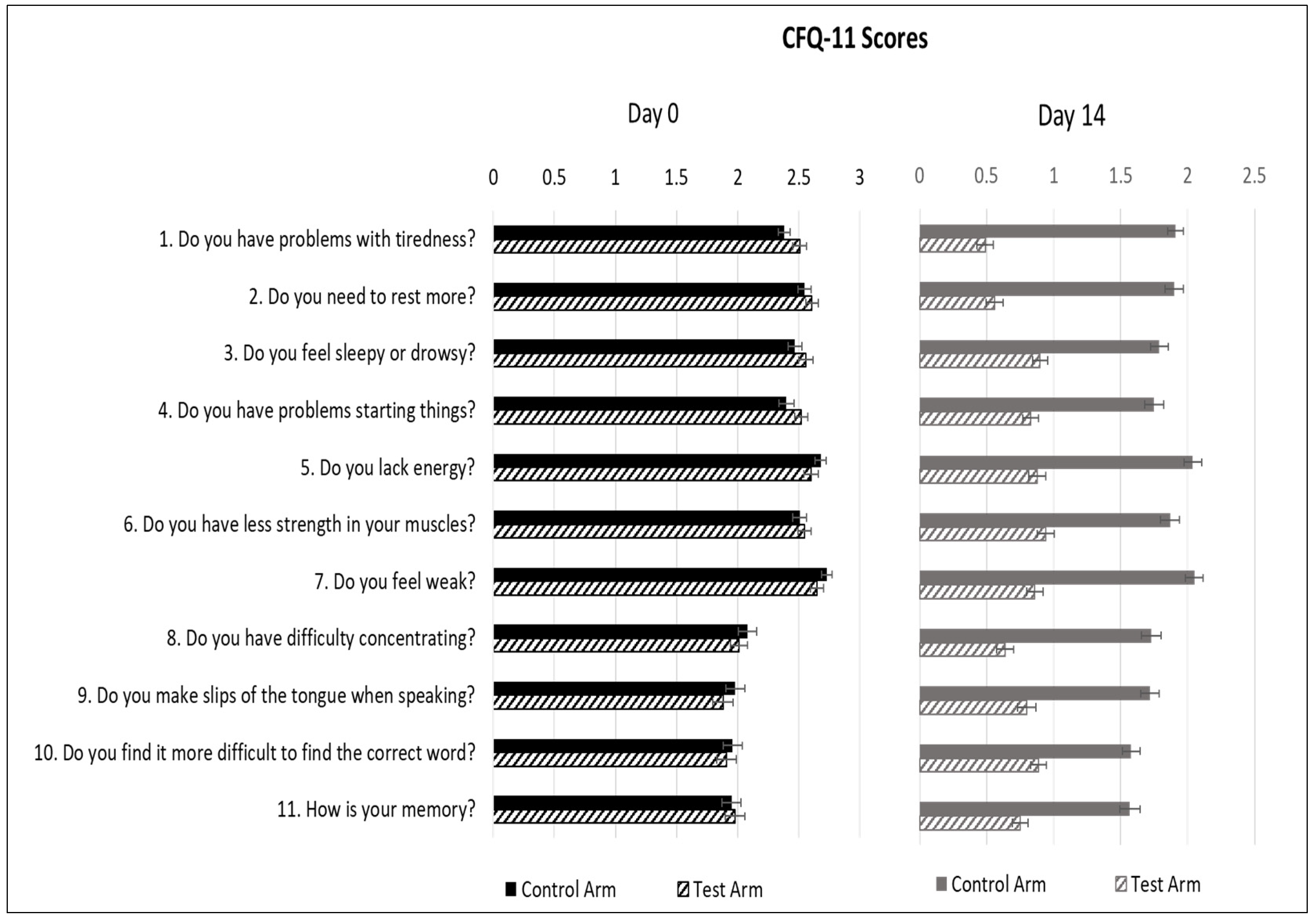
3.1. Analysis of Efficacy
3.2. Analysis of Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raveendran, A.V.; Jayadevan, R.; Sashidharan, S. Long COVID: An overview, diabetes & metabolic syndrome. Clin. Res. Rev. 2021, 15, 869–875. [Google Scholar]
- Rudroff, T.; Fietsam, A.C.; Deters, J.R.; Bryant, A.D.; Kamholz, J. Post-COVID-19 fatigue: Potential contributing factors. Brain Sci. 2020, 10, 1012. [Google Scholar] [CrossRef]
- Xu, X.W.; Wu, X.X.; Jiang, X.G.; Xu, K.J.; Ying, L.J.; Ma, C.L.; Li, S.B.; Wang, H.Y.; Zhang, S.; Gao, H.N.; et al. Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-Cov-2) outside of Wuhan, China: Retrospective case series. BMJ 2020, 368, 606. [Google Scholar] [CrossRef] [Green Version]
- Townsend, L.; Dyer, A.H.; Jones, K.; Dunne, J.; Mooney, A.; Gaffney, F.; O’Connor, L.; Leavy, D.; O’Brien, K.; Dowds, J.; et al. Persistent fatigue following SARS-CoV-2 infection is common and independent of severity of initial infection. PLoS ONE 2020, 15, e0240784. [Google Scholar] [CrossRef]
- ONS WEBSITE. Available online: https://www.ons.gov.uk/news/statementsandletters/theprevalenceoflongcovidsymptomsandcovid19complications (accessed on 16 August 2021).
- O’Connor, C.M. COVID-19 Fatigue. JACC Heart Fail. 2020, 8, 592–594. [Google Scholar] [CrossRef] [PubMed]
- Kedor, C.; Freitag, H.; Meyer-Arndt, L.A.; Wittke, K.; Steinbeis, F.; Haffke, M.; Gordon, R.; Heidecker, B.; Volk, H.D.; Skurk, C.; et al. Chronic COVID-19 syndrome and chronic fatigue syndrome (ME/CFS) following the first pandemic wave in Germany—A first analysis of a prospective observational study. medRxiv 2021. [Google Scholar] [CrossRef]
- Poenaru, S.; Abdallah, S.J.; Corrales-Medina, V.; Cowan, J. COVID-19 and post-infectious myalgic encephalomyelitis/chronic fatigue syndrome: A narrative review. Ther. Adv. Infect. Dis. 2021, 8, 20499361211009385. [Google Scholar]
- Perrin, R.; Riste, L.; Hann, M. Into the looking glass: Post-viral syndrome post COVID-19. Med. Hypotheses 2020, 144, 110055. [Google Scholar] [CrossRef] [PubMed]
- Toogood, P.L.; Clauw, D.J.; Phadke, S.; Hoffman, D. Myalgic encephalomyelitis/ chronic fatigue syndrome (ME/CFS): Where will the drugs come from? Pharmacol. Res. 2021, 165, 105465. [Google Scholar] [CrossRef]
- Maccarone, M.C.; Magro, G.; Tognolo, L.; Masiero, S. Post COVID-19 persistent fatigue: A proposal for rehabilitative interventions in the spa setting. Intern. J. Biometeorol. 2021, 1–3. [Google Scholar]
- Rao, A.V.; Bested, A.C.; Beaulne, T.M.; Katzman, M.A.; Iorio, C.; Berardi, J.M.; Logan, A. A randomized, double-blind, placebo-controlled pilot study of a probiotic in emotional symptoms of chronic fatigue syndrome. Gut. Pathogens 2009, 1, 6. [Google Scholar] [CrossRef] [Green Version]
- Venturini, L.; Bacchi, S.; Capelli, E.; Lorusso, L.; Ricevuti, G.; Cusa1, C. Modification of immunological parameters, oxidative stress markers, mood symptoms, and well-being status in CFS patients after probiotic intake: Observations from a pilot study. Oxid. Med. Cel. Longev. 2019, 2019, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.; Naidu, P.S.; Gupta, S.; Kulkarni, S.K. Effect of natural and synthetic antioxidants in a mouse model of chronic fatigue syndrome. J. Med. Food 2002, 5, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Vi, G.; Sharma, S.; Tirkey, N.; Rishi, P.; Chopra, K. Curcumin, a polyphenolic antioxidant, attenuates chronic fatigue syndrome in murine water immersion stress model. Immunobiology 2009, 214, 33–39. [Google Scholar] [CrossRef]
- Nipate, S.S.; Tiwari, A.H. Antioxidant and immunomodulatory properties of Spilanthes oleracea with potential effect in chronic fatigue syndrome infirmity. J. Ayurv. Int. Med. 2020, 11, 130. [Google Scholar] [CrossRef] [PubMed]
- Rose, B.; Herder, C.; Löffler, H.; Meierhoff, G.; Schloot, N.C.; Walz, M.; Martin, S. Dose-dependent induction of IL-6 by plant-derived proteases in vitro. Clin. Exp. Immunol. 2006, 143, 85–92. [Google Scholar] [CrossRef]
- Rosa, G.; De, Y.; Tewary, P.; Varadhachary, A.; Oppenheim, J.J. Lactoferrin acts as an alarmin to promote the recruitment and activation of antigen-presenting cells and antigen-specific immune responses. J. Immunol. 2008, 180, 6868–6876. [Google Scholar] [CrossRef] [PubMed]
- Murakami, F.; Sasaki, T.; Sugahara, T. Lysozyme stimulates immunoglobulin production by human-human hybridoma and human peripheral blood lymphocytes. Cytotechnology 1997, 24, 177–182. [Google Scholar] [CrossRef]
- Shi, X.L.; Shi, Z.H.; Feng, M.Q.; Ye, L.; Zhu, H.Y.; Li, J.Y.; Ju, D.W.; Zhou, P. High expression of recombinant human catalase and its immunomodulatory effects on H1N1 influenza virus infection. Process. Biochem. 2013, 48, 588–592. [Google Scholar] [CrossRef]
- Liu, H.; Zheng, F.; Cao, Q.; Ren, B.; Zhu, L.; Striker, G.; Vlassara, H. Amelioration of oxidant stress by the defensin lysozyme. Am. J. Physiol. Endocrinol. Metab. 2006, 290, E824–E832. [Google Scholar] [CrossRef] [PubMed]
- Jadhav, S.B.; Shah, N.; Rathi, A.; Rathi, V.; Rathi, A. Serratiopeptidase: Insights into the therapeutic applications. Biotechnol. Rep. 2020, 28, 544. [Google Scholar] [CrossRef]
- Parate, R.; Shah, N. Management of post COVID-19 fatigue using systemic enzymes and probiotics—Case series. Med. J. Clin. Trials Case Stud. 2021, 5, 281. [Google Scholar]
- Butler, S.; Chalder, T.; Ron, M.; Wessely, S. Cognitive behaviour therapy in chronic fatigue syndrome. J. Neurol. Neurosurg. Psychiatry. 1991, 54, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Chalder, T.; Berelowitz, G.; Pawlikowska, T.; Watts, L.; Wessely, S.; Wright, D.; Wallace, E.P. Development of a fatigue scale. J. Psychosom. Res. 1993, 37, 147–153. [Google Scholar] [CrossRef] [Green Version]
- Mahase, E. Covid-19: What do we know about “long covid”? BMJ 2020, 370, m2815. [Google Scholar] [CrossRef]
- Yelin, D.; Wirtheim, E.; Vetter, P.; Kalil, A.C.; Bruchfeld, J.; Runold, M.; Guaraldi, G.; Mussini, C.; Gudiol, C.; Pujol, M.; et al. Long-term consequences of COVID-19: Research needs. Lancet. infect. Dis. 2020, 20, 1115–1117. [Google Scholar] [CrossRef]
- Wilson, C. Concern coronavirus may trigger post-viral fatigue syndromes. New Sci. 2020, 246, 10–11. [Google Scholar] [CrossRef]
- Marshall, M. The lasting misery of coronavirus long-haulers. Nature 2020, 585, 339–341. [Google Scholar] [CrossRef] [PubMed]
- Tansey, C.M.; Louie, M.; Loeb, M.; Gold, W.L.; Muller, M.P.; de Jager, J.; Cameron, J.I.; Tomlinson, G.; Mazzulli, T.; Walmsley, S.L.; et al. One-year outcomes and health care utilization in survivors of severe acute respiratory syndrome. Arch. Intern. Med. 2007, 167, 1312–1320. [Google Scholar] [CrossRef] [Green Version]
- O’Sullivan, O. Long-term sequelae following previous coronavirus epidemics. Clin. Med. 2021, 21, e68–e70. [Google Scholar] [CrossRef]
- Lee, S.H.; Shin, H.S.; Park, H.Y.; Kim, J.L.; Lee, J.J.; Lee, H.; Won, S.D.; Han, W. Depression as a mediator of chronic fatigue and post-traumatic stress symptoms in middle east respiratory syndrome survivors. Psychiatry. Investig. 2019, 16, 59–64. [Google Scholar] [CrossRef] [Green Version]
- Jackson, C. The general health questionnaire. Occup. Med. 2007, 57, 79. [Google Scholar] [CrossRef] [Green Version]
- Morriss, R.; Wearden, A.; Mullis, R. Exploring the validity of the Chalder Fatigue scale in chronic fatigue syndrome. J. Psychosom. Res. 1998, 45, 411–417. [Google Scholar] [CrossRef]
- Loge, J.H.; Ekeberg, Ø.; Kaasa, S. Fatigue in the general Norwegian population: Normative data and associations. J. Psychosom. Res. 1998, 45, 53–65. [Google Scholar] [CrossRef]
- Jackson, C. The Chalder fatigue scale (CFQ 11). Occup. Med. 2015, 65, 86. [Google Scholar] [CrossRef] [Green Version]
- Vollbracht, C.; Kraft, K. Feasibility of vitamin C in the treatment of post viral fatigue with focus on long COVID, based on a systematic review of IV vitamin C on fatigue. Nutrients 2021, 13, 1154. [Google Scholar] [CrossRef] [PubMed]
- Gerwyn, M.; Maes, M. Mechanisms explaining muscle fatigue and muscle pain in patients with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): A Review of recent findings. Curr. Rheumatol. Rep. 2017, 19, 1. [Google Scholar] [CrossRef]
- Sullivan, A.; Nord, C.E.; Evengard, B. Effect of supplement with lactic-acid producing bacteria on fatigue and physical activity in patients with chronic fatigue syndrome. Nutr. J. 2009, 8, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Carabotti, M.; Scirocco, A.; Maselli, M.A.; Severi, C. The gut-brain axis: Interactions between enteric microbiota, central and enteric nervous systems. Ann. Gastroenterol. 2015, 28, 203–209. [Google Scholar] [PubMed]
- Rajinikanth, B.; Venkatachalam, V.V.; Manavalan, R. Investigations on the potential of serratiopeptidase– a proteolytic enzyme, on acetic acid induced ulcerative colitis in mice. Int. J. Pharm. Pharmaceut. Sci. 2014, 6, 525–531. [Google Scholar]
- Gaspani, L.; Limiroli, E.; Ferrario, P.; Bianchi, M. In vivo and in vitro effects of bromelain on PGE2 and SP concentrations in the inflammatory exudate in rats. Pharmacology 2002, 65, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Ando, T.; Mimura, K.; Johansson, C.; Hanson, M.G.; Mougiakakos, D.; Larsson, C.; Palma, T.M.; Sakurai, D.; Norell, H.; Li, M.; et al. Transduction with the antioxidant enzyme catalase protects human T cells against oxidative stress. J. Immunol. 2008, 181, 8382–8390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farhadi, S.A.; Bracho-Sanchez, E.; Freeman, S.L.; Keselowsky, B.G.; Hudalla, G.A. Enzymes as immunotherapeutics. Bioconjugate Chem. 2018, 29, 649–656. [Google Scholar] [CrossRef]
- Malaczewska, J.; Kaczorek-Lukowska, E.; Wojcik, R.; Siwicki, A.K. Antiviral effects of nisin, lysozyme, lactoferrin and their mixtures against bovine viral diarrhoea virus. BMC Veter. Res. 2019, 15, 318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sagar, S.; Rathinavel, A.K.; Lutz, W.E.; Struble, L.R.; Khurana, S.; Schnaubelt, A.T.; Mishra, N.K.; Guda, C.; Broadhurst, M.J.; Reid, S.P.M.; et al. Bromelain inhibits SARS-CoV-2 infection in VeroE6 cells. bioRxiv 2020. [Google Scholar] [CrossRef]
- Chitnis, A.V.; Rathi, A.K. In-vitro virucidal activity of commercial enzyme preparations against SARS-CoV-2 virus. Preprint 2020. [Google Scholar] [CrossRef]
- Qin, M.; Cao, Z.; Wen, J.; Qingsong, Y.; Chaoyong, L. An antioxidant enzyme therapeutic for COVID-19. Adv. Mater. 2020, 32, 1–9. [Google Scholar] [CrossRef]
- Azad, M.A.K.; Sarker, M.; Wan, D. Immunomodulatory effects of probiotics on cytokine profiles. Biomed. Res. Int. 2018, 2018, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morshedi, M.; Hashemi, R.; Moazzen, S. Immunomodulatory and anti-inflammatory effects of probiotics in multiple sclerosis: A systematic review. J. Neuroinflam. 2019, 16, 231. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Wu, Y.; Wang, Y. Antioxidant properties of probiotic bacteria. Nutrients 2017, 9, 521. [Google Scholar] [CrossRef]
- Eguchi, K.; Fujitani, N.; Nakagawa, H. Prevention of respiratory syncytial virus infection with probiotic lactic acid bacterium Lactobacillus gasseri SBT2055. Sci. Rep. 2019, 9, 4812. [Google Scholar] [CrossRef]
- Kim, N.; Yun, M.; Oh, Y.J.; Choi, H.J. Mind-altering with the gut: Modulation of the gut-brain axis with probiotics. J. Microbiol. 2018, 56, 172–182. [Google Scholar] [CrossRef]
- Marotta, A.; Sarno, E.; Del Casale, A.; Pane, M.; Mogna, L.; Amoruso, A.; Felis, G.E.; Fiorio, M. Effects of probiotics on cognitive reactivity, mood, and sleep quality. Front. Psychiatry 2019, 10, 164. [Google Scholar] [CrossRef] [PubMed]
- Williamson, C.B.; Pizano, J.M.; Gasta, M.G. Probiotics and disease: A comprehensive summary—Part 3, Cardiometabolic disease and fatigue syndromes. Integr. Med. 2017, 16, 30. [Google Scholar]
- Ng, Q.X.; Peters, C.; Ho, C.Y.X.; Lim, D.Y.; Yeo, W.S. A meta-analysis of the use of probiotics to alleviate depressive symptoms. J. Affect. Disord. 2018, 228, 13–19. [Google Scholar] [CrossRef]
- Shah, N.; Parate, R.; Vispute, A. Potential of the Combination of a systemic enzyme complex and probiotics administration to combat COVID-19: A randomized open label prospective analysis. Adv. Clin. Toxicol. 2021, 6, 205. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Screening | Treatment | EOT | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Visits | 1 | 2 | 3 | |||||||||||||
| Day (±days) | 24–48 h | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 |
| Written Informed Consent | X | |||||||||||||||
| Inclusion/Exclusion Criteria | X | |||||||||||||||
| Medical and surgical History | X | |||||||||||||||
| Physical Examination | X | |||||||||||||||
| Vital signs | X | X | X | X | X | |||||||||||
| Demographic Information | X | |||||||||||||||
| IP administration | X | X | X | X | X | X | X | X | X | X | X | X | X | X | ||
| Urine pregnancy test (In case of a female subject) | X | |||||||||||||||
| Chalder Fatigue Scale | X | X | X | X | X | X 1 | ||||||||||
| Patient Diary | X | X | X | X | X | X | X | X | X | X | X | X | X | X | ||
| Adverse events | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | |
| Concomitant Medications | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | |
| Control Arm | Test Arm | * p Value | |
|---|---|---|---|
| Age (years); SD; Range | 41.29 ± 13.0 (20–75) | 41.17 ± 12.9 (20–75) | 0.11 |
| Males: Females (%) | 65:35 | 62:38 | - |
| Subjects with co-morbidities (%) | 17 | 12 | - |
| Days to enrolment post negative COVID test; Range | 18.5 (2–48) | 20.6 (4–87) | 0.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rathi, A.; Jadhav, S.B.; Shah, N. A Randomized Controlled Trial of the Efficacy of Systemic Enzymes and Probiotics in the Resolution of Post-COVID Fatigue. Medicines 2021, 8, 47. https://doi.org/10.3390/medicines8090047
Rathi A, Jadhav SB, Shah N. A Randomized Controlled Trial of the Efficacy of Systemic Enzymes and Probiotics in the Resolution of Post-COVID Fatigue. Medicines. 2021; 8(9):47. https://doi.org/10.3390/medicines8090047
Chicago/Turabian StyleRathi, Abhijit, Swati B. Jadhav, and Neha Shah. 2021. "A Randomized Controlled Trial of the Efficacy of Systemic Enzymes and Probiotics in the Resolution of Post-COVID Fatigue" Medicines 8, no. 9: 47. https://doi.org/10.3390/medicines8090047
APA StyleRathi, A., Jadhav, S. B., & Shah, N. (2021). A Randomized Controlled Trial of the Efficacy of Systemic Enzymes and Probiotics in the Resolution of Post-COVID Fatigue. Medicines, 8(9), 47. https://doi.org/10.3390/medicines8090047