Association between Prurigo Nodularis and Etiologies of Peripheral Neuropathy: Suggesting a Role for Neural Dysregulation in Pathogenesis


Abstract
1. Introduction
2. Materials and Methods
3. Results
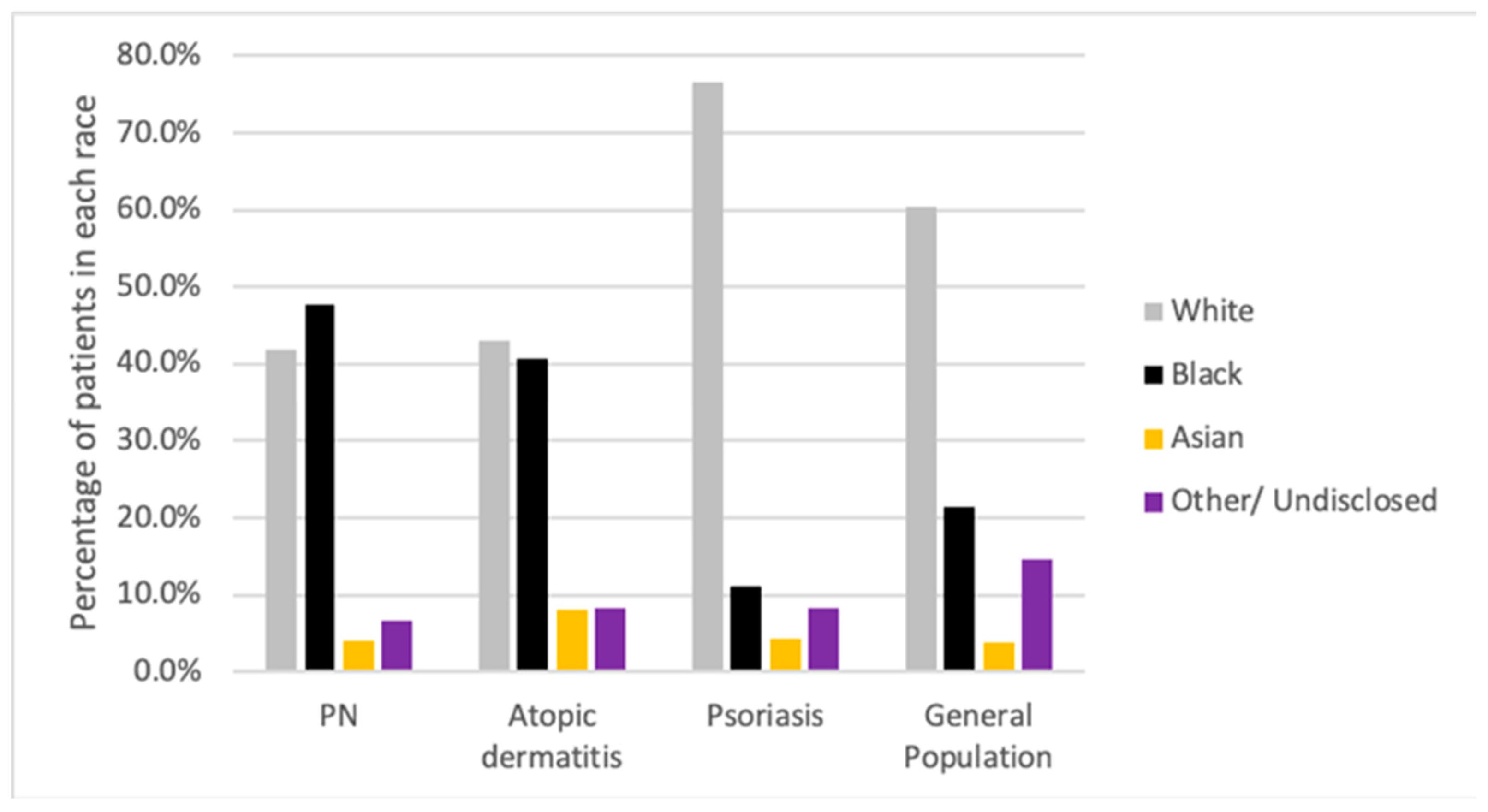
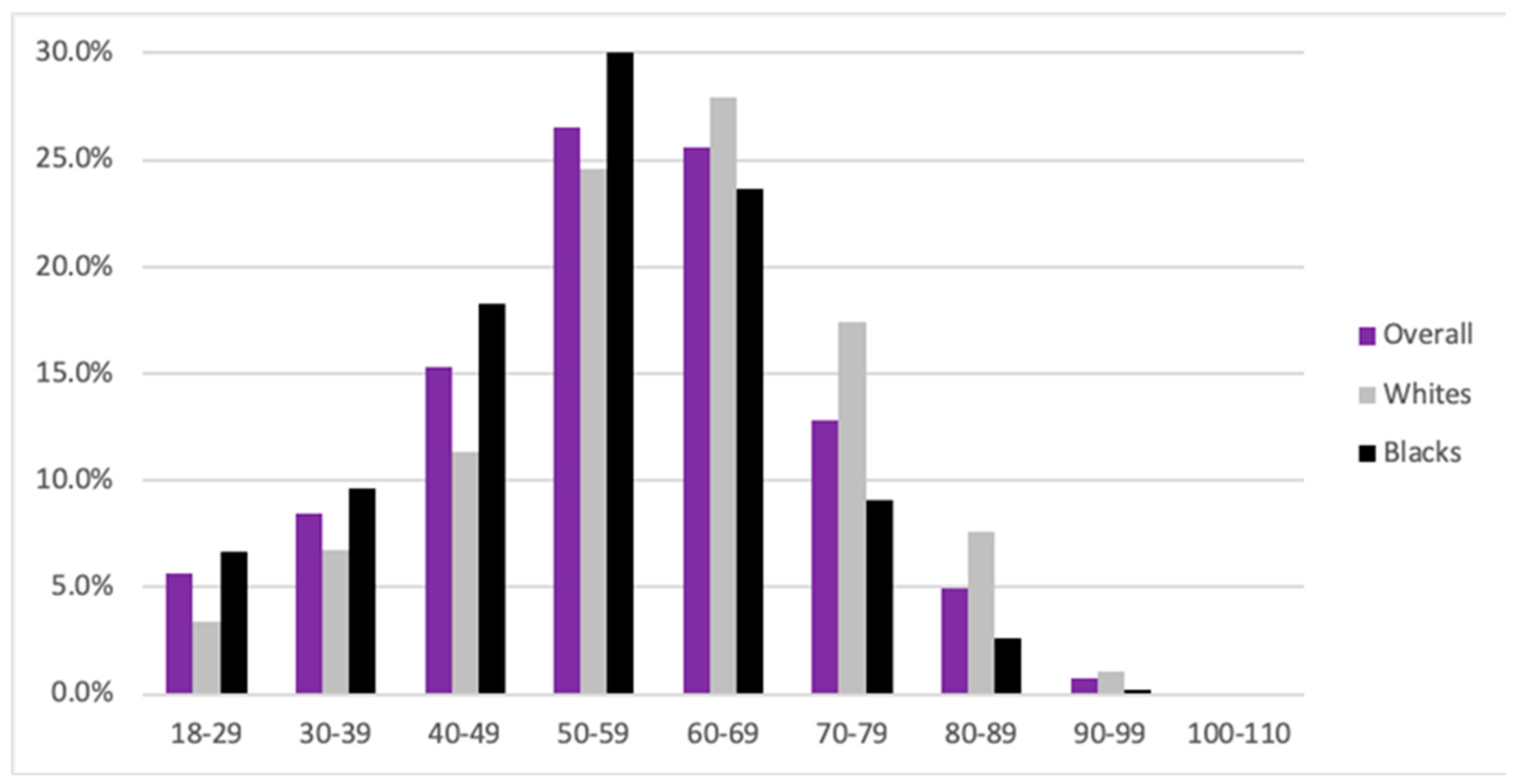
3.1. Patient Demographics
3.2. Association of Prurigo Nodularis with Conditions Known to Feature Peripheral Neuropathies
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kwon, C.D.; Khanna, R.; Williams, K.A.; Kwatra, M.M.; Kwatra, S.G. Diagnostic Workup and Evaluation of Patients with Prurigo Nodularis. Medicines 2019, 6, 97. [Google Scholar] [CrossRef]
- Huang, A.H.; Canner, J.K.; Khanna, R.; Kang, S.; Kwatra, S.G. Real-world prevalence of prurigo nodularis and burden of associated diseases. J. Investig. Dermatol. 2019. [Google Scholar] [CrossRef]
- Székely, H.; Pónyai, G.; Temesvári, E.; Berczi, L.; Hársing, J.; Kárpáti, S.; Herszényi, L.; Tulassay, Z.; Juhasz, M. Association of collagenous colitis with prurigo nodularis. Eur. J. Gastroenterol. Hepatol. 2009, 21, 946–951. [Google Scholar] [CrossRef] [PubMed]
- Payne, R.; Wilkinson, J.D.; Mckee, P.H.; Jurecka, W.; Black, M.M. Nodular prurigo—A clinicopathological study of 46 patients. Br. J. Dermatol. 1985, 113, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Dazzi, C.; Erma, D.; Piccinno, R.; Veraldi, S.; Caccialanza, M. Psychological factors involved in prurigo nodularis: A pilot study. J. Dermatolog Treat. 2011, 22, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Bobko, S.; Zeidler, C.; Osada, N.; Riepe, C.; Pfleiderer, B.; Pogatzki-Zahn, E.; Lvov, A.; Ständer, S. Intraepidermal Nerve Fibre Density is Decreased in Lesional and Inter-lesional Prurigo Nodularis and Reconstitutes on Healing of Lesions. Acta Derm. Venereol. 2016, 96, 404–406. [Google Scholar] [CrossRef] [PubMed]
- Schuhknecht, B.; Marziniak, M.; Wissel, A.; Phan, N.; Pappai, D.; Dangelmaier, J.; Metze, D.; Ständer, S. Reduced intraepidermal nerve fibre density in lesional and nonlesional prurigo nodularis skin as a potential sign of subclinical cutaneous neuropathy. Br. J. Dermatol. 2011, 165, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Vaalasti, A.; Suomalainen, H.; Rechardt, L. Calcitonin gene-related peptide immunoreactivity in prurigo nodularis: A comparative study with neurodermatitis circumscripta. Br. J. Dermatol. 1989, 120, 619–623. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.P.; Pogatzki-Zahn, E.; Snels, C.; Vu, T.H.; Üçeyler, N.; Loser, K.; Sommer, C.; Evers, A.W.M.; Van Laarhoven, A.I.M.; Agelopoulos, K.; et al. There is no functional small-fibre neuropathy in prurigo nodularis despite neuroanatomical alterations. Exp. Dermatol. 2017, 26, 969–971. [Google Scholar] [CrossRef]
- Bharati, A.; Wilson, N.J.E. Peripheral neuropathy associated with nodular prurigo. Clin. Exp. Dermatol. 2017, 26, 969–971. [Google Scholar] [CrossRef]
- Mazza, M.; Guerriero, G.; Marano, G.; Janiri, L.; Bria, P.; Mazza, S. Treatment of prurigo nodularis with pregabalin. J. Clin. Pharm Ther. 2013, 38, 16–18. [Google Scholar] [CrossRef] [PubMed]
- Huang, A.H.; Canner, J.K.; Kang, S.; Kwatra, S.G. Analysis of real-world treatment patterns in patients with prurigo nodularis. J. Am. Acad. Dermatol. 2019, 82, 34–36. [Google Scholar] [CrossRef] [PubMed]
- Aguh, C.; Kwatra, S.G.; He, A.; Okoye, G.A. Thalidomide for the Treatment of Chronic Refractory Prurigo Nodularis. Dermatol. Online J. 2018, 24, 1–6. [Google Scholar] [CrossRef]
- Sharma, D.; Kwatra, S.G. Thalidomide for the treatment of chronic refractory pruritus. J. Am. Acad. Dermatol. 2016, 74, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Tarikci, N.; Kocatürk, E.; Güngör, Ş.; Topal, I.O.; Can, P.Ü.; Singer, R. Pruritus in Systemic Diseases: A Review of Etiological Factors and New Treatment Modalities. Sci. World J. 2015. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, K.M.; Egeberg, A.; Gislason, G.H.; Skov, L.; Thyssen, J.P. Anxiety, depression and suicide in patients with prurigo nodularis. J. Eur. Acad. Dermatol. Venereol. 2017, 31, e106–e107. [Google Scholar] [CrossRef]
- Boozalis, E.; Tang, O.; Patel, S.; Semenov, Y.R.; Pereira, M.P.; Stander, S.; Kang, S.; Kwatra, S.G. Ethnic differences and comorbidities of 909 prurigo nodularis patients. J. Am. Acad. Dermatol. 2018, 79, 714–719.e3. [Google Scholar] [CrossRef]
- Matthews, S.N.; Cockerell, C.J. Prurigo nodularis in, H.I.V-infected individuals. Int J. Dermatol. 1998, 37, 401–409. [Google Scholar] [CrossRef]
- Reich, A.; Ständer, S.; Szepietowski, J.C. Drug-induced pruritus: A review. Acta Derm.-Venereol. 2009, 89, 236–244. [Google Scholar] [CrossRef]
- Tierney, E.F.; Thurman, D.J.; Beckles, G.L.; Cadwell, B.L. Association of statin use with peripheral neuropathy in the, U.S. population 40 years of age or older. J. Diabetes 2012, 5, 207–215. [Google Scholar] [CrossRef]
- Waldinger, T.P.; Siegle, R.J.; Weber, W.; Voorhees, J.J. Dapsone-Induced Peripheral Neuropathy. Arch. Dermatol. 1984, 120, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Goolsby, T.A.; Jakeman, B.; Gaynes, R.P. Clinical relevance of metronidazole and peripheral neuropathy: A systematic review of the literature. Int J. Antimicrob. Agents 2018, 51, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Spring, P.; Gschwind, I.; Gilliet, M. Prurigo nodularis: Retrospective study of 13 cases managed with methotrexate. Clin. Exp. Dermatol. 2014, 39, 468–473. [Google Scholar] [CrossRef] [PubMed]
- Schneider, G.; Hockmann, J.; Ständer, S.; Luger, T.A.; Heuft, G. Psychological factors in prurigo nodularis in comparison with psoriasis vulgaris: Results of a case-control study. Br. J. Dermatol. 2006, 154, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Steinke, S.; Zeidler, C.; Riepe, C.; Bruland, P.; Soto-Rey, I.; Storck, M.; Augustin, M.; Bobko, S.; Garcovich, S.; Legat, F.J.; et al. Humanistic burden of chronic pruritus in patients with inflammatory dermatoses: Results of the European Academy of Dermatology and Venereology Network on Assessment of Severity and Burden of Pruritus (PruNet) cross-sectional trial. J. Am. Acad. Dermatol. 2018, 79, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Iking, A.; Grundmann, S.; Chatzigeorgakidis, E.; Phan, N.Q.; Klein, D.; Ständer, S. Prurigo as a symptom of atopic and non-atopic diseases: Aetiological survey in a consecutive cohort of 108 patients. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 550–557. [Google Scholar] [CrossRef]
- Baykal, C.; Ozkaya-Bayazit, E.; Gökdemir, G.; Diz Küçükkaya, R. The combined occurrence of macular amyloidosis and prurigo nodularis. Eur. J. Dermatol. 2000, 10, 297–299. Available online: http://www.ncbi.nlm.nih.gov/pubmed/10846258 (accessed on 22 October 2018).
- Larson, V.A.; Tang, O.; Stander, S.; Miller, L.S.; Kang, S.; Kwatra, S.G. Association between prurigo nodularis and malignancy in middle-aged adults. J. Am. Acad. Dermatol. 2019, 81, 1198–1201. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Comorbidity | PN, n (%) | AD, n (%) | OR (95% CI) | p-Value | Psoriasis, n (%) | OR (95% CI) | p-Value | Gen Pop, n (%) | OR (95% CI) | p-Value |
|---|---|---|---|---|---|---|---|---|---|---|
| Peripheral neuropathies | 308(27.45) | 1673(16.1) | 1.97(1.71–2.27) | <0.002 | 2759(18.32) | 1.69(1.47–1.94) | <0.002 | 150,325(3.04) | 12.08(10.59–13.77) | <0.002 |
| Focal–multifocal neuropathies | ||||||||||
| Amyloidosis | 12(1.07) | 31(0.3) | 3.61(1.85–7.05) | <0.002 | 32(0.21) | 5.08(2.61–9.88) | <0.002 | 2234(0.05) | 23.94(13.53–42.35) | <0.002 |
| Carpal tunnel syndrome | 54(4.81) | 397(3.82) | 1.27(0.95–1.7) | 0.10377 | 522(3.47) | 1.41(1.06–1.88) | 0.01893 | 22,079(0.45) | 11.28(8.58–14.83) | <0.002 |
| DM | 296(26.38) | 1167(11.23) | 2.83(2.45–3.28) | <0.002 | 2648(17.59) | 1.68(1.46–1.93) | <0.002 | 177,323(3.58) | 9.64(8.44–11.01) | <0.002 |
| Hyperpituitarism | 6(0.53) | 37(0.36) | 1.5(0.63–3.57) | 0.35138 | 38(0.25) | 2.12(0.9–5.04) | 0.07978 | 3268(0.07) | 8.14(3.64–18.16) | <0.002 |
| Myxedema | 5(0.45) | 15(0.14) | 3.1(1.12–8.53) | 0.02133 | 27(0.18) | 2.49(0.96–6.48) | 0.05277 | 1169(0.02) | 18.95(7.86–45.69) | <0.002 |
| Phlebitis | 26(2.32) | 122(1.17) | 2(1.3–3.06) | <0.002 | 168(1.12) | 2.1(1.38–3.19) | <0.002 | 7395(0.15) | 15.85(10.74–23.4) | <0.002 |
| Ulnar nerve entrapment | 17(1.52) | 74(0.71) | 2.14(1.26–3.65) | 0.00391 | 76(0.5) | 3.03(1.79–5.15) | <0.002 | 3546(0.07) | 21.46(13.27–34.68) | <0.002 |
| Vasculitis | 38(3.39) | 208(2) | 1.72(1.21–2.44) | 0.00231 | 302(2.01) | 1.71(1.22–2.41) | <0.002 | 13,241(0.27) | 13.07(9.45–18.07) | <0.002 |
| Chronic axonal neuropathies | ||||||||||
| Alcohol abuse | 69(6.15) | 202(1.94) | 3.3(2.5–4.38) | <0.002 | 462(3.07) | 2.07(1.6–2.69) | <0.002 | 33,073(0.67) | 9.74(7.63–12.43) | <0.002 |
| Borreliosis | 5(0.45) | 63(0.61) | 0.73(0.29–1.83) | 0.50450 | 141(0.94) | 0.47(0.19–1.16) | 0.09351 | 62,20(0.13) | 3.56(1.48–8.57) | 0.00250 |
| CKD | 180(16.04) | 446(4.29) | 4.26(3.54–5.13) | <0.002 | 950(6.31) | 2.84(2.39–3.37) | <0.002 | 57,268(1.16) | 16.32(13.91–19.15) | <0.002 |
| Cobalamin deficiency | 31(2.76) | 204(1.96) | 1.42(0.97–2.08) | 0.07200 | 383(2.54) | 1.09(0.75–1.58) | 0.65366 | 13,782(0.28) | 10.17(7.12–14.55) | <0.002 |
| Dapsone | 48(4.28) | 132(1.27) | 3.47(2.48–4.86) | <0.002 | 96(0.64) | 6.97(4.9–9.9) | <0.002 | 5420(0.11) | 40.76(30.49–54.5) | <0.002 |
| Folic acid deficiency | 5(0.45) | 14(0.13) | 3.32(1.19–9.23) | 0.01480 | 30(0.2) | 2.24(0.87–5.79) | 0.08659 | 930(0.02) | 23.82(9.87–57.47) | <0.002 |
| HIV infection | 150(13.37) | 185(1.78) | 8.51(6.8–10.66) | <0.002 | 144(0.96) | 15.98(12.6–20.27) | <0.002 | 13,137(0.27) | 57.98(48.78–68.92) | <0.002 |
| Hypothyroidism | 124(11.05) | 844(8.12) | 1.41(1.15–1.72) | <0.002 | 2066(13.72) | 0.78(0.64–0.95) | 0.01169 | 113,182(2.29) | 5.31(4.4–6.4) | <0.002 |
| Metronidazole | 139(12.39) | 1216(11.7) | 1.07(0.88–1.29) | 0.49875 | 1098(7.29) | 1.8(1.49–2.17) | <0.002 | 69,631(1.41) | 9.91(8.3–11.84) | <0.002 |
| NSCLC | 3(0.27) | 9(0.09) | 3.09(0.84–11.44) | 0.07466 | 33(0.22) | 1.22(0.37–3.99) | 0.74091 | 2234(0.05) | 5.94(1.91–18.45) | <0.002 |
| Phenytoin | 2(0.18) | 1(0.01) | 18.55(1.68–204.76) | <0.002 | 2(0.01) | 13.44(1.89–95.52) | <0.002 | 1039(0.02) | 8.5(2.12–34.09) | <0.002 |
| PMN | 94(8.38) | 432(4.16) | 2.11(1.67–2.66) | <0.002 | 894(5.94) | 1.45(1.16–1.81) | <0.002 | 73,237(1.48) | 6.09(4.93–7.52) | <0.002 |
| PMN of Lung | 6(0.53) | 30(0.29) | 1.86(0.77–4.47) | 0.16086 | 83(0.55) | 0.97(0.42–2.23) | 0.94261 | 7227(0.15) | 3.68(1.65–8.2) | <0.002 |
| PMN of Ovary | 2(0.18) | 4(0.04) | 4.64(0.85–25.34) | 0.05135 | 4(0.03) | 6.72(1.23–36.73) | 0.01090 | 481(0.01) | 18.37(4.58–73.76) | <0.002 |
| Small-cell carcinoma | 1(0.09) | 4(0.04) | 2.32(0.26–20.74) | 0.43939 | 14(0.09) | 0.96(0.13–7.3) | 0.96736 | 948(0.02) | 4.66(0.65–33.12) | 0.09051 |
| Statins | 419(37.34) | 1999(19.24) | 2.5(2.2–2.85) | <0.002 | 4748(31.54) | 1.29(1.14–1.47) | <0.002 | 361,855(7.31) | 7.56(6.69–8.53) | <0.002 |
| Waldenstrom’s disease | 1(0.09) | 3(0.03) | 3.09(0.32–29.72) | 0.30358 | 5(0.03) | 2.69(0.31–23.01) | 0.34799 | 293(0.01) | 15.07(2.11–107.42) | <0.002 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hughes, J.-D.M.; Woo, T.E.; Belzberg, M.; Khanna, R.; Williams, K.A.; Kwatra, M.M.; Hassan, S.; Kwatra, S.G. Association between Prurigo Nodularis and Etiologies of Peripheral Neuropathy: Suggesting a Role for Neural Dysregulation in Pathogenesis. Medicines 2020, 7, 4. https://doi.org/10.3390/medicines7010004
Hughes J-DM, Woo TE, Belzberg M, Khanna R, Williams KA, Kwatra MM, Hassan S, Kwatra SG. Association between Prurigo Nodularis and Etiologies of Peripheral Neuropathy: Suggesting a Role for Neural Dysregulation in Pathogenesis. Medicines. 2020; 7(1):4. https://doi.org/10.3390/medicines7010004
Chicago/Turabian StyleHughes, John-Douglas Matthew, Taylor E. Woo, Micah Belzberg, Raveena Khanna, Kyle A. Williams, Madan M. Kwatra, Shahzeb Hassan, and Shawn G. Kwatra. 2020. "Association between Prurigo Nodularis and Etiologies of Peripheral Neuropathy: Suggesting a Role for Neural Dysregulation in Pathogenesis" Medicines 7, no. 1: 4. https://doi.org/10.3390/medicines7010004
APA StyleHughes, J.-D. M., Woo, T. E., Belzberg, M., Khanna, R., Williams, K. A., Kwatra, M. M., Hassan, S., & Kwatra, S. G. (2020). Association between Prurigo Nodularis and Etiologies of Peripheral Neuropathy: Suggesting a Role for Neural Dysregulation in Pathogenesis. Medicines, 7(1), 4. https://doi.org/10.3390/medicines7010004