
Obesity: Clinical Impact, Pathophysiology, Complications, and Modern Innovations in Therapeutic Strategies

Abstract
1. Introduction
2. Definition and Classification of Obesity
3. Limitations of Current Definitions
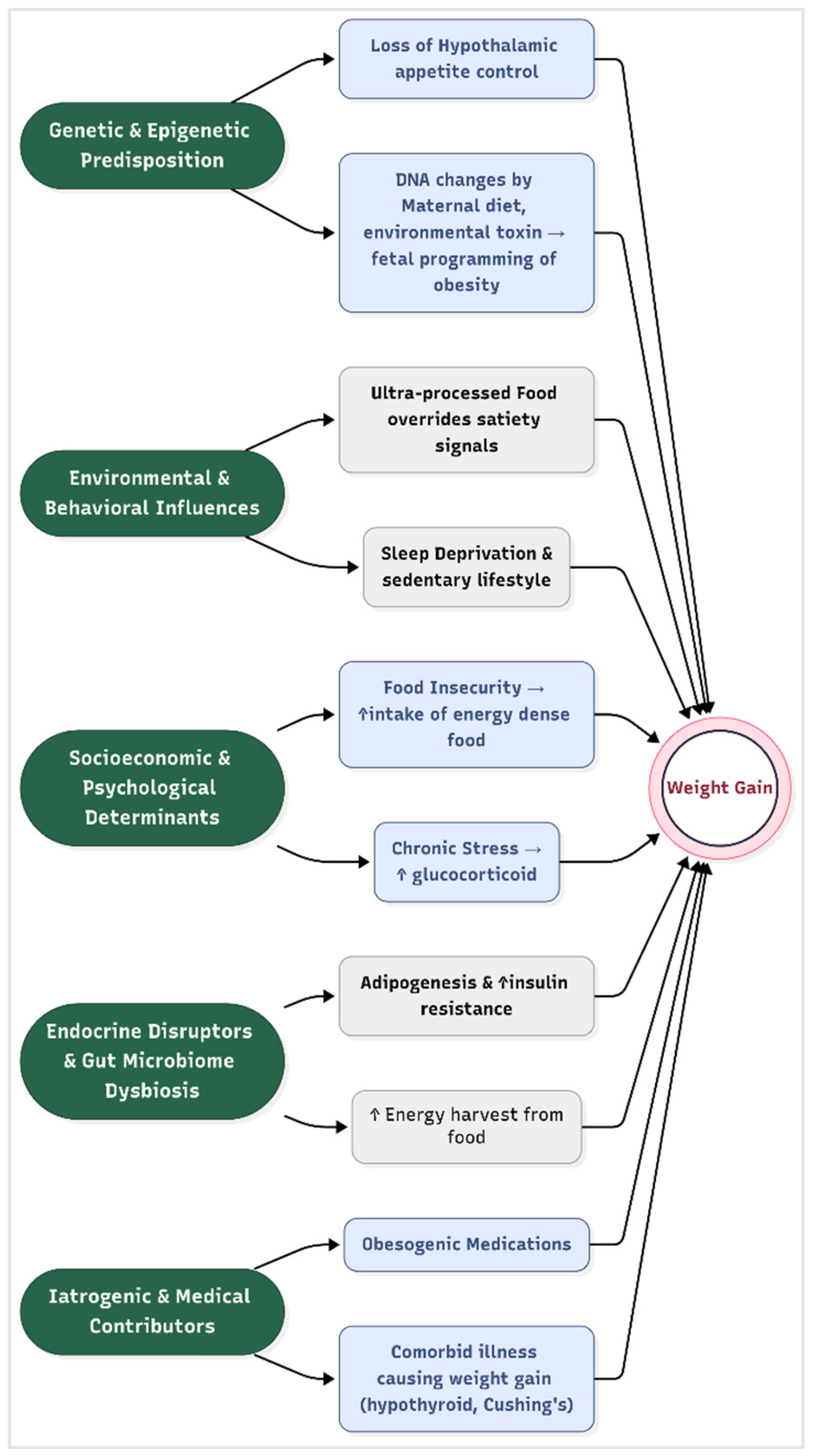
4. Risk Factors for Obesity
- Genetic and Epigenetic Predisposition
- Environmental and Behavioral Influences
- Socioeconomic and Psychological Determinants
- Endocrine Disruptors and Gut Microbiome Dysbiosis
- Iatrogenic and Medical Contributors
5. Pathological Impact of Obesity on Human Health
- Metabolic Dysfunction and Insulin Resistance
- Cardiovascular Disease (CVD)
- Respiratory Complications
- Chronic kidney disease
- Musculoskeletal Degeneration
- Cancer Pathogenesis
- Neuroendocrine and Mental Health Disorders
- Reproductive Dysfunction
- Immune System Impairment
6. Historical Treatment Options for Obesity
- Pharmacological Interventions
- ○
- Amphetamines and stimulants (1930s–1970s): Amphetamines were first marketed in the 1930s as Benzedrine in an over-the-counter inhaler to treat nasal congestion. By 1937, amphetamines were available by prescription in tablet form and were used in the treatment of the sleeping disorder narcolepsy and ADHD. They were widely prescribed for weight loss in the mid-20th century due to their appetite-suppressing effects. However, their addictive potential, cardiovascular risks (e.g., hypertension, arrhythmias), and misuse led to strict regulation under the U.S. Controlled Substances Act in 1971 [56].
- ○
- Fenfluramine/phentermine (1990s): This combination therapy enhanced serotonin release (fenfluramine) and norepinephrine reuptake inhibition (phentermine) to suppress appetite. While effective (average 10–15% weight loss), fenfluramine was withdrawn in 1997 after studies linked it to valvular heart disease and pulmonary hypertension [3].
- ○
- Sibutramine (1997–2010): A serotonin–norepinephrine reuptake inhibitor, sibutramine reduced hunger and increased satiety. Despite 5–10% weight loss in trials, it was discontinued in 2010 after the SCOUT trial showed elevated cardiovascular events (e.g., stroke) in high-risk patients [4].
- ○
- Orlistat (1999–present): A pancreatic lipase inhibitor, orlistat blocks dietary fat absorption, resulting in ~3–5% weight loss. It is still available, but its use is limited by gastrointestinal side effects (e.g., steatorrhea, fecal incontinence) and poor long-term adherence [57].
- Surgical Interventions
- ○
- Jejunoileal bypass (1950s–1970s): This malabsorptive procedure involved bypassing most of the small intestine. While effective (~30% weight loss), it caused severe complications, including liver failure, renal stones, and malnutrition, leading to its abandonment [58].
- ○
- Vertical banded gastroplasty (1980s): This restrictive surgery partitioned the stomach with staples and a band. Initial weight loss (20–25%) was often reversed due to staple-line breakdown and pouch dilation, with high reoperation rates [59].
- ○
- Adjustable gastric banding (1990s–2010s): The Lap-Band® restricted stomach capacity via an inflatable band. While safer than bypass surgeries, it resulted in only 15–20% weight loss, with frequent complications (band slippage, erosion) and a 40% long-term failure rate [60].
- ○
- Roux-en-Y gastric bypass (RYGB, 1960s–present): Combining restriction and malabsorption, RYGB reduces stomach size and reroutes the small intestine. It remains the gold standard, with 25–30% sustained weight loss and remission of diabetes in 60–80% of patients. However, risks include dumping syndrome, micronutrient deficiencies, and rare but severe complications (e.g., anastomotic leaks) [5].
7. Emerging Medical Therapies for Obesity
7.1. Semaglutide
- Route of administration: It can be administered in both injectable (subcuteneous) and oral form as described above.
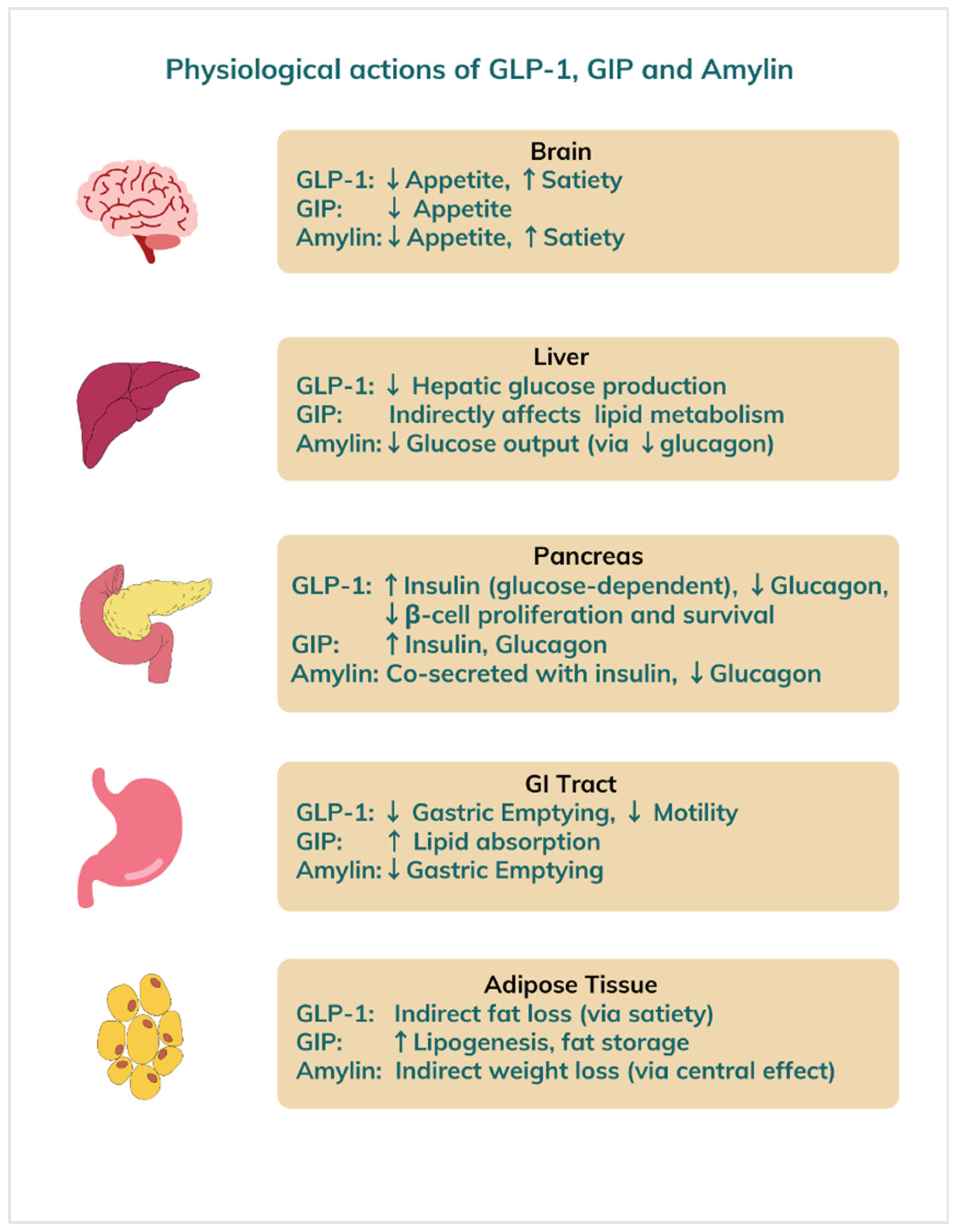
- Mechanism of action: Semaglutide mimics the effects of endogenous GLP-1, a gut-derived incretin hormone. It acts centrally on hypothalamic GLP-1 receptors to suppress appetite, enhance satiety, and reduce food intake. Peripherally, it slows gastric emptying and improves insulin secretion in a glucose-dependent manner, indirectly promoting weight loss [6].
- Rybelsus is an oral form of semaglutide, a modified GLP-1 analog in which the native peptide has been engineered for both enzymatic stability and albumin binding: specifically, an Aib (α-aminoisobutyric acid) substitution at position 8 to resist DPP-4 degradation and an attached C18 fatty diacid chain at lysine 26 (via a spacer) to promote reversible albumin binding and extend half-life [63]. Crucially, it is co-formulated with the small-molecule absorption enhancer SNAC (sodium N-[8-(2-hydroxybenzoyl)amino]caprylate), which transiently raises local gastric pH and facilitates transcellular uptake of semaglutide across the gastric epithelium [64]. Once absorbed, it mimics the similar action of endogenous GLP-1. For optimum absorption, Rybelsus should be taken first thing in the morning on an empty stomach, with no more than 4 ounces of water. At least 30 min should be allowed to pass before eating, drinking anything else, or taking other medications.
- Efficacy: In the semaglutide treatment effect in people (STEP) with obesity trials, semaglutide 2.4 mg weekly produced a mean placebo-adjusted weight loss of 14.9% over 68 weeks in STEP 1, and up to 16.0% in STEP 4 with continued use [6,8]. These outcomes are substantially superior to older therapies such as orlistat or phentermine/topiramate [65].
- Side effects: The most common adverse events are gastrointestinal, such as nausea (up to 44%), vomiting, diarrhea, and constipation. These effects are dose-dependent and occur primarily during dose escalation [65]. Rare but serious adverse events may include acute pancreatitis, gallbladder disease, and renal impairment. An FDA boxed warning exists for thyroid C-cell tumors based on rodent studies, contraindicating its use in patients with personal or family history of medullary thyroid carcinoma.
7.2. Tirzepatide
- Route of administration: Tirzepatide is administered as a once-weekly subcutaneous injection.
- Mechanism of action: Tirzepatide is a 39–amino-acid peptide engineered as a dual agonist of the glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptors, combining both incretin activities within a single molecule to achieve prolonged plasma half-life [67]. By co-activating GIP and GLP-1 receptors on pancreatic β-cells, it amplifies cyclic AMP signaling and enhances glucose-dependent insulin secretion while concurrently suppressing glucagon release from α-cells, leading to improved glycemic control [68]. Activation of its GLP-1 component also delays gastric emptying, blunting postprandial glucose excursions and contributing to steadier overall glucose profiles [69]. In addition to these peripheral actions, its dual receptor engagement in hypothalamic feeding centers reduces appetite and caloric intake, resulting in substantial weight loss that surpasses effects seen with selective GLP-1 agonists [67].
- Efficacy: In the SURMOUNT-1 trial, tirzepatide 15 mg weekly achieved mean weight reductions of 20.9% over 72 weeks, with 50–57% of participants losing ≥20% of their body weight [7]. It also included regular lifestyle counselling sessions to reinforce a ~500 kcal/day deficit and ≥150 min/week of exercise during the trial. This surpasses all previously approved pharmacotherapies, including semaglutide.
- Side effects: Similar to GLP-1 agonists, it commonly causes gastrointestinal effects, including nausea (31%), diarrhea (22%), and constipation. Injection-site reactions and fatigue also occur. As with semaglutide, rare events include pancreatitis and gallbladder disease. There is a class effect boxed warning by the FDA for medullary thyroid carcinoma.
7.3. Retatrutide
- Route of administration: It is administered as a weekly subcutaneous injection.
- Mechanism of action: Retatrutide combines appetite suppression (GLP-1, GIP) with increased energy expenditure via glucagon receptor stimulation. This multifaceted mechanism targets both caloric intake and energy metabolism and enhances insulin secretion, optimizes glucose homeostasis, and effectively regulates appetite [70].
- Efficacy: Findings from phase 1 to phase 3 clinical trials highlight retatrutide’s significant therapeutic efficacy, with marked reductions in body weight (up to 24.2% over 48 weeks) and improved glycemic control, underscoring its potential as a treatment for obesity and type 2 diabetes mellitus. In addition to its effects on weight and glucose regulation, retatrutide demonstrates potential benefits in reducing cardiovascular risk factors and managing non-alcoholic fatty liver disease, suggesting a broader role in the management of metabolic disorders [71].
- Side effects: Similar to other incretin-based agents, nausea, vomiting, and diarrhea are common. Glucagon activity may cause transient elevations in heart rate and hepatic transaminases.
7.4. Cagrilintide
- Route of administration: It is administered as a weekly subcutaneous injection.
- Mechanism of action: Cagrilintide acts on amylin and calcitonin receptors within the area of the postrema and nucleus tractus solitarius, lowering food intake through both homeostatic and hedonic mechanisms. It slows gastric emptying, suppresses postprandial glucagon secretion, and reduces appetite via central hypothalamic pathways [63]. Its extended half-life enables convenient once-weekly dosing and a stable pharmacodynamic profile. When co-administered with the GLP-1 receptor agonist semaglutide (CagriSema®), they act synergistically to produce greater weight loss and improved glycemic control than either agent alone, without significantly increasing the incidence or severity of gastrointestinal adverse events [72,73]. In combination with GLP-1 receptor activation from semaglutide, this dual approach enhances anorectic effects.
- Efficacy: In a phase 2 study, the combination achieved mean body weight reductions of 15.6% at 32 weeks, compared to 5.1% with semaglutide alone [72].
- Side effects: The most common side effects of cagrilintide are gastrointestinal—mild-to-moderate nausea, vomiting, and constipation—which are generally transient and can be managed through gradual dose escalation and adequate hydration [74].
7.5. Orforglipron
- Route of administration: It is taken once a day as an oral pill.
- Mechanism of action: It binds to and activates the GLP-1 receptor to stimulate glucose-dependent insulin secretion, inhibit glucagon release, delay gastric emptying, and suppress appetite—mechanisms that contribute to improved glycemic control and substantial weight loss [76]. Preclinical studies demonstrated that orforglipron has a high oral bioavailability and favorable pharmacokinetics, supporting once-daily dosing [77].
- Efficacy: In a phase 2 clinical trial, orforglipron led to mean weight reductions of up to 12.6% over 36 weeks in people with obesity, a result comparable to injectable GLP-1 analogues [76].
- Side effects: Common side effects included nausea, vomiting, and diarrhea, which were dose-dependent and tended to decline over time. Importantly, no cases of severe hypoglycemia were reported, supporting its favorable safety profile when used without concomitant insulin or sulfonylureas [77].
7.6. Setmelanotide
- Route of administration: It is administered as a weekly subcutaneous injection.
- Mechanism of action: It is a melanocortin-4 receptor (MC4R) agonist that restores signaling disrupted in genetic obesity disorders. Unlike GLP-1 therapies, setmelanotide acts directly on hypothalamic satiety pathways.
- Efficacy: In trials, 80% of patients with POMC deficiency and 45% with LEPR deficiency achieved ≥10% weight loss over one year. Hunger scores also improved dramatically.
- Side effects: Injection site reactions, hyperpigmentation, and nausea are common. Skin darkening occurred in ~60% of trial participants. No serious long-term safety concerns have been observed [78].
7.7. Tesofensine
- Route of administration: It is administered as a once-daily oral capsule.
- Mechanism of action: Tesofensine inhibits the presynaptic reuptake of dopamine, norepinephrine, and serotonin in appetite-regulating centers of the brain, thereby suppressing hunger and enhancing satiety [79].
- Efficacy: In the pivotal phase IIb “TIPO-1” trial, obese patients treated with 1.0 mg of tesofensine daily for 24 weeks experienced a mean weight loss of 12.8 kg (≈11% of body weight), compared with a 2.2 kg loss in the placebo group.
- Side effects: The most commonly reported adverse events included dry mouth, nausea, insomnia, headache, diarrhea, and constipation. Dose-dependent increases in heart rate (up to 8 bpm) and blood pressure (1–3 mmHg) were noted, with an overall withdrawal rate of 13% versus 6% for placebo.
7.8. Bimagrumab
- Route of administration: It is administered as a monthly intravenous injection.
- Mechanism of action: Bimagrumab is a fully human monoclonal antibody that exerts its anabolic effects on skeletal muscle by dual blockade of activin type II receptors, thereby neutralizing multiple negative regulators of muscle growth [81,82]. It acts via several pathways as follows:
- ○
- High-affinity binding to ActRIIA and ActRIIB: Bimagrumab binds both activin receptor type IIA (ActRIIA) and type IIB (ActRIIB) with high affinity, preventing endogenous ligands—principally myostatin (GDF-8), activin A, activin B, and growth differentiation factor 11 (GDF-11)—from engaging the receptor complex.
- ○
- Inhibition of Smad2/3 signaling: Ligand-activated ActRII receptors normally recruit and phosphorylate Smad2/3 transcription factors, which then translocate to the nucleus to upregulate atrophy-associated genes (e.g., atrogin-1, MuRF-1) and suppress protein synthesis pathways. Bimagrumab’s receptor blockade abolishes Smad2/3 phosphorylation, shifting the balance toward muscle protein accretion.
- ○
- Promotion of myoblast differentiation and hypertrophy: By neutralizing multiple TGF-β family ligands simultaneously, bimagrumab not only counteracts myostatin’s anti-anabolic signal, but also blocks activin-mediated inhibition of myogenic differentiation. The result is enhanced myoblast fusion, increased fiber cross-sectional area, and a more than two-fold greater hypertrophic response than myostatin inhibition alone.
- ○
- Reversible endocrine modulation: Activin signaling in the anterior pituitary regulates follicle-stimulating hormone (FSH) secretion. In healthy adults, bimagrumab transiently suppresses FSH and subtly alters luteinizing hormone (LH) responses without impacting downstream sex steroid levels; these effects fully reverse after drug clearance.
- ○
- Net clinical effect: Through these combined actions—pan ligand blockade at ActRIIA/B, inhibition of catabolic Smad signaling, and potentiation of anabolic myogenic pathways—bimagrumab consistently increases lean body mass, strength, and functional outcomes in sarcopenic and muscle-wasting populations. By blocking activin IIA and IIB receptors, bimagrumab inhibits myostatin and related ligands, promoting skeletal muscle hypertrophy and enhancing adipose tissue loss through increased energy expenditure.
- Efficacy: In a 48-week phase II randomized trial of adults with type 2 diabetes and obesity, intravenous bimagrumab (10 mg/kg every 4 weeks) led to a 20.5% reduction in fat mass and a 3.6% increase in lean mass versus placebo, with an overall weight loss of 6.5% compared to 0.8% for placebo.
- Side effects: Bimagrumab was generally well-tolerated; reported adverse events included transient gastrointestinal symptoms, muscle cramps, and mild elevations in liver enzymes. No serious cardiovascular signals were observed.
8. Limitations of New Obesity Pharmacotherapy
9. New Therapeutic Approaches on the Horizon
9.1. Epigenetic Modulation
- DNA methyltransferase inhibitors, such as low-dose 5-azacytidine, improved lipid oxidation and insulin sensitivity in animal models by demethylating promoters of metabolism related genes [87].
- Histone deacetylase modulators, including selective HDAC3 inhibitors, increase expression of genes involved in mitochondrial growth and activation of brown fat, leading to higher resting energy use [88].
- Natural products such as resveratrol, curcumin, and omega 3 fatty acids are under study for their capacity to induce beneficial chromatin changes in liver and fat tissue, with early data showing modest improvements in body composition [89].
9.2. Fecal Microbiota Transplantation
- Single-dose transplantation has temporarily improved insulin sensitivity and reduced liver fat, though sustained weight loss has been small without repeat procedures [90].
- Combining transplantation with low fermentable fiber intake enhances donor microbe growth, supports production of beneficial fatty acids, and yields larger reductions in abdominal fat over six months [91].
- Future studies use defined bacterial mixtures rather than whole stool to create standardized, safe, and scalable therapies aimed at specific metabolic pathways.
9.3. Noncoding RNA-Based Therapeutics
- MicroRNA inhibitors (antagomirs) targeting miR-103 and miR-107 improve insulin sensitivity and reduce adiposity in diet-induced obese mice by enhancing hepatic and peripheral insulin signaling [92].
- Conversely, miR-196a mimics promote the browning of white adipose tissue—upregulating uncoupling protein 1 and other thermogenic genes—thereby increasing energy expenditure and conferring resistance to diet-induced obesity [93].
- Long noncoding RNA modulation—for example, lipid nanoparticle-mediated silencing of the adipocyte-specific lncRNA lncOb—restores leptin expression, reduces fat mass, and improves glucose tolerance in obese mouse models [94].
10. Long Term Strategies for Sustained Weight Loss
- Calorie Restriction and Dietary Quality
- Physical Activity
- Behavioral and Supportive Interventions
- Sleep and Stress Management
11. Future Direction in Obesity Treatment Research
12. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight: Key Facts. 2024. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 5 May 2025).
- Ward, Z.J.; Bleich, S.N.; Cradock, A.L.; Barrett, J.L.; Giles, C.M.; Flax, C.; Long, M.W.; Gortmaker, S.L. Projected U.S. State-Level Prevalence of Adult Obesity and Severe Obesity. N. Engl. J. Med. 2019, 381, 2440–2450. [Google Scholar] [CrossRef] [PubMed]
- Connolly, H.M.; Crary, J.L.; McGoon, M.D.; Hensrud, D.D.; Edwards, B.S.; Edwards, W.D.; Schaff, H.V. Valvular heart disease associated with fenfluramine and phentermine. N. Engl. J. Med. 1997, 11, 141. [Google Scholar] [CrossRef] [PubMed]
- James, W.P.T.; Caterson, I.D.; Coutinho, W.; Finer, N.; Van Gaal, L.F.; Maggioni, A.P.; Sharma, A.M.; Shepherd, G.M.; Rode, R.A.; Renz, C.L.; et al. Effect of Sibutramine on Cardiovascular Outcomes in Overweight and Obese Subjects. N. Engl. J. Med. 2010, 363, 905–917. [Google Scholar] [CrossRef] [PubMed]
- Adams, T.D.; Davidson, L.E.; Litwin, S.E.; Kolotkin, R.L.; LaMonte, M.J.; Pendleton, R.C.; Strong, M.B.; Vinik, R.; Wanner, N.A.; Hopkins, P.N.; et al. Health benefits of gastric bypass surgery after 6 years. JAMA 2012, 308, 1122–1131. [Google Scholar] [CrossRef] [PubMed]
- Wilding, J.P.H.; Batterham, R.L.; Calanna, S.; Davies, M.; Van Gaal, L.F.; Lingvay, I.; McGowan, B.M.; Rosenstock, J.; Tran, M.T.; Wadden, T.A.; et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N. Engl. J. Med. 2021, 384, 989–1002. [Google Scholar] [CrossRef] [PubMed]
- Jastreboff, A.M.; Aronne, L.J.; Ahmad, N.N.; Wharton, S.; Connery, L.; Alves, B.; Kiyosue, A.; Zhang, S.; Liu, B.; Bunck, M.C.; et al. Tirzepatide Once Weekly for the Treatment of Obesity. N. Engl. J. Med. 2022, 387, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsson, N.; Davies, M.; Hesse, D.; Greenway, F.L.; Jensen, C.; Lingvay, I.; Mosenzon, O.; Rosenstock, J.; Rudofsky, G.; Tadayon, S.; et al. Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance in Adults With Overweight or Obesity: The STEP 4 Randomized Clinical Trial. JAMA 2021, 325, 1414–1425. [Google Scholar] [CrossRef]
- Rubino, F.; Cummings, D.E.; Eckel, R.H.; Cohen, R.V.; Wilding, J.P.H.; Brown, W.A.; Stanford, F.C.; Batterhaml, R.L.; Farooqi, P.I.S.; Farpour-Lambert, N.J.; et al. Definition and diagnostic criteria of clinical obesity. Lancet Diabetes Endocrinol. 2025, 13, 221–262. [Google Scholar] [CrossRef] [PubMed]
- WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.M.; Kushner, R.F. A proposed clinical staging system for obesity. Int. J. Obes. 2009, 33, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Romero-Corral, A.; Somers, V.K.; Sierra-Johnson, J.; Thomas, R.J.; Collazo-Clavell, M.L.; Korinek, J.; Allison, T.G.; Batsis, J.A.; Sert-Kuniyoshi, F.H.; Lopez-Jimenez, F. Accuracy of body mass index in diagnosing obesity in the adult general population. Int. J. Obes. 2008, 32, 959–966. [Google Scholar] [CrossRef] [PubMed]
- Neeland, I.J.; Ross, R.; Després, J.P.; Matsuzawa, Y.; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, R.D.; Arsenault, B.; et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: A position statement. Lancet Diabetes Endocrinol. 2019, 7, 715–725. [Google Scholar] [CrossRef] [PubMed]
- Stefan, N.; Häring, H.-U.; Hu, F.B.; Schulze, M.B. Metabolically healthy obesity: Epidemiology, mechanisms, and clinical implications. Lancet Diabetes Endocrinol. 2013, 1, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Lear, S.; James, P.; Ko, G.; Clinical, S.K.-E. Appropriateness of waist circumference and waist-to-hip ratio cutoffs for different ethnic groups. Eur. J. Clin. Nutr. 2010, 64, 42–61. [Google Scholar] [CrossRef] [PubMed]
- Natale, V.; Rajagopalan, A. Worldwide variation in human growth and the World Health Organization growth standards: A systematic review. BMJ Open 2014, 4, e003735. [Google Scholar] [CrossRef] [PubMed]
- Zapata, J.K.; Azcona-Sanjulian, M.C.; Catalán, V.; Ramírez, B.; Silva, C.; Rodríguez, A.; Escalada, J.; Frühbeck, G.; Gómez-Ambrosi, J. BMI-based obesity classification misses children and adolescents with raised cardiometabolic risk due to increased adiposity. Cardiovasc. Diabetol. 2023, 22, 240. [Google Scholar] [CrossRef] [PubMed]
- Lemos, T.; Gallagher, D. Current body composition measurement techniques. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Ross, R.; Neeland, I.J.; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, R.D.; Arsenault, B.; Cuevas, A.; Hu, F.B.; et al. Waist circumference as a vital sign in clinical practice: A Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat. Rev. Endocrinol. 2020, 16, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Blüher, M. Metabolically Healthy Obesity. Endocr. Rev. 2020, 41, 405–420. [Google Scholar] [CrossRef] [PubMed]
- Loos, R.J.F.; Yeo, G.S.H. The genetics of obesity: From discovery to biology. Nat. Rev. Genet. 2021, 23, 120–133. [Google Scholar] [CrossRef] [PubMed]
- Frayling, T.M.; Timpson, N.J.; Weedon, M.N.; Zeggini, E.; Freathy, R.M.; Lindgren, C.M.; Perry, J.R.B.; Elliott, K.S.; Lango, H.; Rayner, N.W.; et al. A common variant in the FTO gene is associated with body mass index and predisposes to childhood and adult obesity. Science 2007, 316, 889–894. [Google Scholar] [CrossRef] [PubMed]
- Lillycrop, K.A.; Burdge, G.C. The effect of nutrition during early life on the epigenetic regulation of transcription and implications for human diseases. J. Nutr. Nutr. 2011, 4, 248–260. [Google Scholar] [CrossRef] [PubMed]
- Khera, A.V.; Chaffin, M.; Wade, K.H.; Zahid, S.; Brancale, J.; Xia, R.; Distefano, M.; Senol-Cosar, O.; Haas, M.E.; Bick, A.; et al. Polygenic Prediction of Weight and Obesity Trajectories from Birth to Adulthood. Cell 2019, 177, 587–596.e9. [Google Scholar] [CrossRef] [PubMed]
- Healy, D.R.; Zarei, I.; Mikkonen, S.; Soininen, S.; Viitasalo, A.; Haapala, E.A.; Auriola, S.; Hanhineva, K.; Kolehmainen, M.; Lakka, T.A. Longitudinal associations of an exposome score with serum metabolites from childhood to adolescence. Commun. Biol. 2024, 7, 890. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Cannon, G.; Levy, R.B.; Moubarac, J.-C.; Louzada, M.L.C.; Rauber, F.; Khandpur, N.; Cediel, G.; Neri, D.; Martinez-Steele, E.; et al. Ultra-processed foods: What they are and how to identify them. Public Health Nutr. 2019, 22, 936–941. [Google Scholar] [CrossRef] [PubMed]
- Cappuccio, F.P.; Taggart, F.M.; Kandala, N.-B.; Currie, A.; Peile, E.; Stranges, S.; Miller, M.A. Meta-Analysis of Short Sleep Duration and Obesity in Children and Adults. Sleep 2008, 31, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Maharana, A.; Nsoesie, E.O. Use of Deep Learning to Examine the Association of the Built Environment with Prevalence of Neighborhood Adult Obesity. JAMA Netw. Open 2018, 1, e181535. [Google Scholar] [CrossRef] [PubMed]
- Brakefield, W.S.; Olusanya, O.A.; Shaban-Nejad, A. Association Between Neighborhood Factors and Adult Obesity in Shelby County, Tennessee: Geospatial Machine Learning Approach. JMIR Public Health Surveill. 2022, 8, e37039. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Specter, S.E. Poverty and obesity: The role of energy density and energy costs. Am. J. Clin. Nutr. 2004, 79, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Tomiyama, A.J.; Carr, D.; Granberg, E.M.; Major, B.; Robinson, E.; Sutin, A.R.; Brewis, A. How and why weight stigma drives the obesity “epidemic” and harms health. BMC Med. 2018, 16, 123. [Google Scholar] [CrossRef] [PubMed]
- Volkow, N.D.; Wise, R.A.; Baler, R. The dopamine motive system: Implications for drug and food addiction. Nat. Rev. Neurosci. 2017, 18, 741–752. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.; Dawson, L.; Welker, E. Early Life Stress and Childhood Obesity Risk; Healthy Eating Research: Durham, NC, USA, 2017. [Google Scholar]
- Heindel, J.J.; Blumberg, B.; Cave, M.; Machtinger, R.; Mantovani, A.; Mendez, M.A.; Nadal, A.; Palanza, P.; Panzica, G.; Sargis, R.; et al. Metabolism disrupting chemicals and metabolic disorders. Reprod. Toxicol. 2017, 68, 3–33. [Google Scholar] [CrossRef] [PubMed]
- Turnbaugh, P.J.; Ley, R.E.; Mahowald, M.A.; Magrini, V.; Mardis, E.R.; Gordon, J.I. An obesity-associated gut microbiome with increased capacity for energy harvest. Nature 2006, 444, 1027–1031. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Yu, C.; He, Y.; Zhu, S.; Wang, S.; Xu, Z.; You, S.; Jiao, Y.; Liu, S.-L.; Bao, H. Integrative metagenomic analysis reveals distinct gut microbial signatures related to obesity. BMC Microbiol. 2024, 24, 119. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, G.P.; McGowan, O.O. Mechanisms underlying metabolic disturbances associated with psychosis and antipsychotic drug treatment. J. Psychopharmacol. 2017, 31, 1430–1436. [Google Scholar] [CrossRef] [PubMed]
- Apovian, C.M.; Aronne, L.J.; Bessesen, D.H.; McDonnell, M.E.; Murad, M.H.; Pagotto, U.; Ryan, D.H.; Still, C.D. Pharmacological Management of Obesity: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2015, 100, 342–362. [Google Scholar] [CrossRef] [PubMed]
- Kahn, S.E.; Hull, R.L.; Utzschneider, K.M. Mechanisms linking obesity to insulin resistance and type 2 diabetes. Nature 2006, 444, 840–846. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Golabi, P.; de Avila, L.; Paik, J.M.; Srishord, M.; Fukui, N.; Qiu, Y.; Burns, L.; Afendy, A.; Nader, F. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. J. Hepatol. 2019, 71, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.E.; Do Carmo, J.M.; Da Silva, A.A.; Wang, Z.; Hall, M.E. Obesity-Induced Hypertension: Interaction of Neurohumoral and Renal Mechanisms. Circ. Res. 2015, 116, 991–1006. [Google Scholar] [CrossRef] [PubMed]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Després, J.-P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. Obesity and Cardiovascular Disease a Scientific Statement from the American Heart Association. Circulation 2021, 143, E984–E1010. [Google Scholar] [CrossRef] [PubMed]
- Drager, L.F.; Togeiro, S.M.; Polotsky, V.Y.; Lorenzi-Filho, G. Obstructive Sleep Apnea: A Cardiometabolic Risk in Obesity and the Metabolic Syndrome. J. Am. Coll. Cardiol. 2013, 62, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Z.; Wang, Y.; Zhao, X.; Cui, H.; Han, M.; Ren, X.; Gang, X.; Wang, G. Obesity and chronic kidney disease. Am. J. Physiol. Endocrinol. Metab. 2023, 324, E24–E41. [Google Scholar] [CrossRef] [PubMed]
- Canney, A.L.; Cohen, R.V.; Elliott, J.A.; Aboud, C.M.; Martin, W.P.; Docherty, N.G.; le Roux, C.W. Improvements in diabetic albuminuria and podocyte differentiation following Roux-en-Y gastric bypass surgery. Diabetes Vasc. Dis. Res. 2019, 17, 1479164119879039. [Google Scholar] [CrossRef] [PubMed]
- Berenbaum, F.; Eymard, F.; Houard, X. Osteoarthritis, inflammation and obesity. Curr. Opin. Rheumatol. 2013, 25, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Grosse, Y.; Bianchini, F.; Straif, K. Body Fatness and Cancer—Viewpoint of the IARC Working Group. N. Engl. J. Med. 2016, 375, 794–798. [Google Scholar] [CrossRef] [PubMed]
- Avgerinos, K.I.; Spyrou, N.; Mantzoros, C.S.; Dalamaga, M. Obesity and cancer risk: Emerging biological mechanisms and perspectives. Metabolism 2019, 92, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Myers, M.G.; Leibel, R.L.; Seeley, R.J.; Schwartz, M.W. Obesity and leptin resistance: Distinguishing cause from effect. Trends Endocrinol. Metab. 2010, 21, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Luppino, F.S.; de Wit, L.M.; Bouvy, P.F.; Stijnen, T.; Cuijpers, P.; Penninx, B.W.J.H.; Zitman, F.G. Overweight, Obesity, and Depression: A Systematic Review and Meta-analysis of Longitudinal Studies. Arch. Gen. Psychiatry 2010, 67, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef] [PubMed]
- Ngandu, T.; Lehtisalo, J.; Solomon, A.; Levälahti, E.; Ahtiluoto, S.; Antikainen, R.; Bäckman, L.; Hänninen, T.; Jula, A.; Laatikainen, T.; et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): A randomised controlled trial. Lancet 2015, 385, 2255–2263. [Google Scholar] [CrossRef] [PubMed]
- Shanik, M.H.; Xu, Y.; Skrha, J.; Dankner, R.; Zick, Y.; Roth, J. Insulin Resistance and HyperinsulinemiaIs hyperinsulinemia the cart or the horse? Diabetes Care 2008, 31, S262–S268. [Google Scholar] [CrossRef] [PubMed]
- Catalano, P.M.; Shankar, K. Obesity and pregnancy: Mechanisms of short term and long term adverse consequences for mother and child. BMJ 2017, 356, 1. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Z.; Tabuchi, C.; Gayer, S.G.; Bapat, S.P. Immune Dysregulation in Obesity. Annu. Rev. Pathol. 2025, 20, 483–509. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, N. On Speed: The Many Lives of Amphetamine; New York University Press: New York, NY, USA, 2008; Available online: https://psycnet.apa.org/record/2008-03283-000 (accessed on 6 May 2025).
- Padwal, R.; Li, S.K.; Lau, D.C.W. Long-term pharmacotherapy for overweight and obesity: A systematic review and meta-analysis of randomized controlled trials. Int. J. Obes. 2003, 27, 1437–1446. [Google Scholar] [CrossRef] [PubMed]
- Buchwald, H.; Oien, D.M. Metabolic/bariatric surgery worldwide 2011. Obes. Surg. 2013, 23, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.T.; Goldman, C.; Rosenquist, C.J.; Arango, A.; Cole, C.J.; Lee, S.J.; Wolfe, B.M. Laparoscopic Versus Open Gastric Bypass: A Randomized Study of Outcomes, Quality of Life, and Costs. Ann. Surg. 2001, 234, 279–291. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, P.E.; MacDonald, L.; Anderson, M.; Brennan, L.; Brown, W.A. Long-term outcomes after bariatric surgery: Fifteen-year follow-up of adjustable gastric banding and a systematic review of the bariatric surgical literature. Ann. Surg. 2013, 257, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Drucker, D.J.; Nauck, M.A. The incretin system: Glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes. Lancet 2006, 368, 1696–1705. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Garrido, M.A.; Brandt, S.J.; Clemmensen, C.; Müller, T.D.; DiMarchi, R.D.; Tschöp, M.H. GLP-1/glucagon receptor co-agonism for treatment of obesity. Diabetologia 2017, 60, 1851–1861. [Google Scholar] [CrossRef] [PubMed]
- Kruse, T.; Hansen, J.L.; Dahl, K.; Schäffer, L.; Sensfuss, U.; Poulsen, C.; Schlein, M.; Hansen, A.M.K.; Jeppesen, C.B.; de la Cour, C.D.; et al. Development of Cagrilintide, a Long-Acting Amylin Analogue. J. Med. Chem. 2021, 64, 11183–11194. [Google Scholar] [CrossRef] [PubMed]
- Yabe, D.; Deenadayalan, S.; Horio, H.; Kaneto, H.; Jensen, T.B.; Terauchi, Y.; Yamada, Y.; Inagaki, N. Efficacy and safety of oral semaglutide in Japanese patients with type 2 diabetes: A subgroup analysis by baseline variables in the PIONEER 9 and PIONEER 10 trials. J. Diabetes Investig. 2022, 13, 975–985. [Google Scholar] [CrossRef] [PubMed]
- Khera, R.; Murad, M.H.; Chandar, A.K.; Dulai, P.S.; Wang, Z.; Prokop, L.J.; Loomba, R.; Camilleri, M.; Singh, S. Association of Pharmacological Treatments for Obesity with Weight Loss and Adverse Events: A Systematic Review and Meta-analysis. JAMA 2016, 315, 2424–2434. [Google Scholar] [CrossRef] [PubMed]
- US FDA. FDA Approves First Medication for Obstructive Sleep Apnea 2024. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-medication-obstructive-sleep-apnea (accessed on 7 May 2025).
- Coskun, T.; Sloop, K.W.; Loghin, C.; Alsina-Fernandez, J.; Urva, S.; Bokvist, K.B.; Cui, X.; Briere, D.A.; Cabrera, O.; Roell, W.C.; et al. LY3298176, a novel dual GIP and GLP-1 receptor agonist for the treatment of type 2 diabetes mellitus: From discovery to clinical proof of concept. Mol. Metab. 2018, 18, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Frias, J.P.; Nauck, M.A.; Van, J.; Kutner, M.E.; Cui, X.; Benson, C.; Urva, S.; Gimeno, R.E.; Milicevic, Z.; Robins, D.; et al. Efficacy and safety of LY3298176, a novel dual GIP and GLP-1 receptor agonist, in patients with type 2 diabetes: A randomised, placebo-controlled and active comparator-controlled phase 2 trial. Lancet 2018, 392, 2180–2193. [Google Scholar] [CrossRef] [PubMed]
- Jalleh, R.J.; Plummer, M.P.; Marathe, C.S.; Umapathysivam, M.M.; Quast, D.R.; Rayner, C.K.; Jones, K.L.; Wu, T.; Horowitz, M.; Nauck, M.A. Clinical Consequences of Delayed Gastric Emptying With GLP-1 Receptor Agonists and Tirzepatide. J. Clin. Endocrinol. Metab. 2024, 110, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Kaur, M.; Misra, S. A review of an investigational drug retatrutide, a novel triple agonist agent for the treatment of obesity. Eur. J. Clin. Pharmacol. 2024, 80, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Rahman, T.; Roy, P.; Ahmed, F.K.; Mueller-Gomez, J.L.; Sarkar, S.; Garg, N.; Femi-Lawal, V.O.; Wireko, A.A.; Thaalibi, H.I.; Hashmi, M.U.; et al. The power of three: Retatrutide’s role in modern obesity and diabetes therapy. Eur. J. Pharmacol. 2024, 985, 177095. [Google Scholar] [CrossRef] [PubMed]
- Frias, J.P.; Deenadayalan, S.; Erichsen, L.; Knop, F.K.; Lingvay, I.; Macura, S.; Mathieu, C.; Pedersen, S.D.; Davies, M. Efficacy and safety of co-administered once-weekly cagrilintide 2·4 mg with once-weekly semaglutide 2·4 mg in type 2 diabetes: A multicentre, randomised, double-blind, active-controlled, phase 2 trial. Lancet 2023, 402, 720–730. [Google Scholar] [CrossRef] [PubMed]
- Lau, D.C.W.; Erichsen, L.; Francisco, A.M.; Satylganova, A.; le Roux, C.W.; McGowan, B.; Pedersen, S.D.; Pietiläinen, K.H.; Rubino, D.; Batterham, R.L. Once-weekly cagrilintide for weight management in people with overweight and obesity: A multicentre, randomised, double-blind, placebo-controlled and active-controlled, dose-finding phase 2 trial. Lancet 2021, 398, 2160–2172. [Google Scholar] [CrossRef] [PubMed]
- D’Ascanio, A.M.; Mullally, J.A.; Frishman, W.H. Cagrilintide: A Long-Acting Amylin Analog for the Treatment of Obesity. Cardiol. Rev. 2024, 32, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Wharton, S.; Blevins, T.; Connery, L.; Rosenstock, J.; Raha, S.; Liu, R.; Ma, X.; Mather, K.J.; Haupt, A.; Robins, D.; et al. Daily Oral GLP-1 Receptor Agonist Orforglipron for Adults with Obesity. N. Engl. J. Med. 2023, 389, 877–888. [Google Scholar] [CrossRef] [PubMed]
- Frias, J.P.; Hsia, S.; Eyde, S.; Liu, R.; Ma, X.; Konig, M.; Kazda, C.; Mather, K.J.; Haupt, A.; Pratt, E.; et al. Efficacy and safety of oral orforglipron in patients with type 2 diabetes: A multicentre, randomised, dose-response, phase 2 study. Lancet 2023, 402, 472–483. [Google Scholar] [CrossRef] [PubMed]
- Dutta, D.; Nagendra, L.; Anne, B.; Kumar, M.; Sharma, M.; Kamrul-Hasan, A.B.M. Orforglipron, a novel non-peptide oral daily glucagon-like peptide-1 receptor agonist as an anti-obesity medicine: A systematic review and meta-analysis. Obes. Sci. Pr. 2024, 10, e743. [Google Scholar] [CrossRef] [PubMed]
- Clément, K.; Argente, J.; Chung, W.K.; De Waele, K.; Gonneau-Lejeune, J.; Gordon, G.; Kohlsdorf, K.; Poitou, C.; Puder, L.; Yuan, G.; et al. Efficacy and safety of setmelanotide, an MC4R agonist, in individuals with severe obesity due to LEPR or POMC deficiency: Single-arm, open-label, multicentre, phase 3 trials. Lancet Diabetes Endocrinol. 2020, 8, 960–970. [Google Scholar] [CrossRef] [PubMed]
- Astrup, A.; Madsbad, S.; Breum, L.; Jensen, T.J.; Kroustrup, J.P.; Larsen, T.M. Effect of tesofensine on bodyweight loss, body composition, and quality of life in obese patients: A randomised, double-blind, placebo-controlled trial. Lancet 2008, 372, 1906–1913. [Google Scholar] [CrossRef] [PubMed]
- Melson, E.; Ashraf, U.; Papamargaritis, D.; Davies, M.J. What is the pipeline for future medications for obesity? Int. J. Obes. 2025, 49, 433–451. [Google Scholar] [CrossRef] [PubMed]
- Rooks, D.; Petricoul, O.; Praestgaard, J.; Bartlett, M.; Laurent, D.; Roubenoff, R. Safety and pharmacokinetics of bimagrumab in healthy older and obese adults with body composition changes in the older cohort. J. Cachexia Sarcopenia Muscle 2020, 11, 1525–1534. [Google Scholar] [CrossRef] [PubMed]
- Garito, T.; Zakaria, M.; Papanicolaou, D.A.; Li, Y.; Pinot, P.; Petricoul, O.; Laurent, D.; Rooks, D.; Rondon, J.C.; Roubenoff, R. Effects of bimagrumab, an activin receptor type II inhibitor, on pituitary neurohormonal axes. Clin. Endocrinol. 2018, 88, 908–919. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.D. What is the required energy deficit per unit weight loss? Int. J. Obes. 2008, 32, 573–576. [Google Scholar] [CrossRef] [PubMed]
- Wing, R.R.; Tate, D.F.; Gorin, A.A.; Raynor, H.A.; Fava, J.L. A self-regulation program for maintenance of weight loss. N. Engl. J. Med. 2006, 355, 1563–1571. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Martínez-Steele, E.; Cannon, G. Reasons to avoid ultra-processed foods. BMJ 2024, 384, q439. [Google Scholar] [CrossRef] [PubMed]
- Perri, M.G.; Shankar, M.N.; Daniels, M.J.; Durning, P.E.; Ross, K.M.; Limacher, M.C.; Janicke, D.M.; Martin, A.D.; Dhara, K.; Bobroff, L.B.; et al. Effect of Telehealth Extended Care for Maintenance of Weight Loss in Rural US Communities: A Randomized Clinical Trial. JAMA Netw. Open 2020, 3, E206764. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Wang, Y.; Chen, F.; Zhou, B. Epigenetics in obesity: Mechanisms and advances in therapies based on natural products. Pharmacol. Res. Perspect. 2024, 12, e1171. [Google Scholar] [CrossRef] [PubMed]
- Nijhawan, P.; Behl, T.; Khullar, G.; Pal, G.; Kandhwal, M.; Goyal, A. HDAC in obesity: A critical insight. Obes. Med. 2020, 18, 100212. [Google Scholar] [CrossRef]
- Lam, H.N.; Lin, S.-P.; Nguyen, D.H.N.; Chen, C.-M.; Su, C.-T.; Fang, T.-C.; Li, S.-C. Integrative Roles of Functional Foods, Microbiotics, Nutrigenetics, and Nutrigenomics in Managing Type 2 Diabetes and Obesity. Nutrients 2025, 17, 608. [Google Scholar] [CrossRef] [PubMed]
- Zecheng, L.; Donghai, L.; Runchuan, G.; Yuan, Q.; Qi, J.; Yijia, Z.; Shuaman, R.; Xiaoqi, L.; Yi, W.; Ni, M.; et al. Fecal microbiota transplantation in obesity metabolism: A meta analysis and systematic review. Diabetes Res. Clin. Pr. 2023, 202, 110803. [Google Scholar] [CrossRef] [PubMed]
- Lahtinen, P.; Juuti, A.; Luostarinen, M.; Niskanen, L.; Liukkonen, T.; Tillonen, J.; Kössi, J.; Ilvesmäki, V.; Viljakka, M.; Satokari, R.; et al. Effectiveness of Fecal Microbiota Transplantation for Weight Loss in Patients with Obesity Undergoing Bariatric Surgery: A Randomized Clinical Trial. JAMA Netw. Open 2022, 5, e2247226. [Google Scholar] [CrossRef] [PubMed]
- Trajkovski, M.; Hausser, J.; Soutschek, J.; Bhat, B.; Akin, A.; Zavolan, M.; Heim, M.H.; Stoffel, M. MicroRNAs 103 and 107 regulate insulin sensitivity. Nature 2011, 474, 649–653. [Google Scholar] [CrossRef] [PubMed]
- Mori, M.; Nakagami, H.; Rodriguez-Araujo, G.; Nimura, K.; Kaneda, Y. Essential role for miR-196a in brown adipogenesis of white fat progenitor cells. PLoS Biol. 2012, 10, e1001314. [Google Scholar] [CrossRef] [PubMed]
- Dallner, O.S.; Marinis, J.M.; Lu, Y.-H.; Birsoy, K.; Werner, E.; Fayzikhodjaeva, G.; Dill, B.D.; Molina, H.; Moscati, A.; Kutalik, Z.; et al. Dysregulation of a long noncoding RNA reduces leptin leading to a leptin-responsive form of obesity. Nat. Med. 2019, 25, 507–516. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.O.; Wyatt, H.R.; Peters, J.C. Energy balance and obesity. Circulation 2012, 126, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Li, Y.; Chen, M.; Cai, Z.; Cai, Z.; Jiang, Z. Comparing caloric restriction regimens for effective weight management in adults: A systematic review and network meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2024, 21, 108. [Google Scholar] [CrossRef] [PubMed]
- Leidy, H.J.; Clifton, P.M.; Astrup, A.; Wycherley, T.P.; Westerterp-Plantenga, M.S.; Luscombe-Marsh, N.D.; Woods, S.C.; Mattes, R.D. The role of protein in weight loss and maintenance. Am. J. Clin. Nutr. 2015, 101, 1320S–1329S. [Google Scholar] [CrossRef] [PubMed]
- Slavin, J. Fiber and prebiotics: Mechanisms and health benefits. Nutrients 2013, 5, 1417–1435. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.; Cannon, G.; Lawrence, M.; Louzada, M.L.; Machado, P. Ultra-Processed Foods, Diet Quality, and Health Using the NOVA Classification System; FAO: Rome, Italy, 2019. [Google Scholar]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- American Heart Association. Recommendations for Physical Activity in Adults and Kids. 2024. Available online: https://www.heart.org/en/healthy-living/fitness/fitness-basics/aha-recs-for-physical-activity-in-adults (accessed on 9 May 2025).
- Church, T.S.; Martin, C.K.; Thompson, A.M.; Earnest, C.P.; Mikus, C.R.; Blair, S.N. Changes in weight, waist circumference and compensatory responses with different doses of exercise among sedentary, overweight postmenopausal women. PLoS ONE 2009, 4, e4515. [Google Scholar] [CrossRef] [PubMed]
- Levine, J.A. Nonexercise activity thermogenesis (NEAT): Environment and biology. Am. J. Physiol. Endocrinol. Metab. 2004, 286, E675–E685. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.M.; Winkler, E.A.H.; Eakin, E.G.; Gardiner, P.A.; Dunstan, D.W.; Owen, N.; Healy, G.N. Sensitivity to Change of Objectively-Derived Measures of Sedentary Behavior. Meas. Phys. Educ. Exerc. Sci. 2015, 19, 138–147. [Google Scholar] [CrossRef]
- Burke, L.E.; Wang, J.; Sevick, M.A. Self-monitoring in weight loss: A systematic review of the literature. J. Am. Diet. Assoc. 2011, 111, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, M.J.; Mottershead, T.A.; Ronksley, P.E.; Sigal, R.J.; Campbell, T.S.; Hemmelgarn, B.R. Motivational interviewing to improve weight loss in overweight and/or obese patients: A systematic review and meta-analysis of randomized controlled trials. Obes. Rev. 2011, 12, 709–723. [Google Scholar] [CrossRef] [PubMed]
- Taheri, S.; Lin, L.; Austin, D.; Young, T.; Mignot, E. Short sleep duration is associated with reduced leptin, elevated ghrelin, and increased body mass index. PLoS Med. 2004, 1, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.P.; Després, J.P.; Bouchard, C.; Tremblay, A. The association between sleep duration and weight gain in adults: A 6-year prospective study from the Quebec Family Study. Sleep 2008, 31, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Adam, T.C.; Epel, E.S. Stress, eating and the reward system. Physiol. Behav. 2007, 91, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Forman, E.M.; Butryn, M.L.; Manasse, S.M.; Crosby, R.D.; Goldstein, S.P.; Wyckoff, E.P.; Thomas, J.G. Acceptance-based versus standard behavioral treatment for obesity: Results from the mind your health randomized controlled trial. Obesity 2016, 24, 2050–2056. [Google Scholar] [CrossRef] [PubMed]
- Müller, T.D.; Blüher, M.; Tschöp, M.H.; DiMarchi, R.D. Anti-obesity drug discovery: Advances and challenges. Nat. Rev. Drug Discov. 2021, 21, 201–223. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Drug (Brand Name) | Indication of Use | Mechanism of Action | Side Effects | Route of Administration |
|---|---|---|---|---|
| Semaglutide (Wegovy®) | Chronic weight management in adults with obesity or overweight with at least one weight-related condition | GLP-1 receptor agonist | Nausea, vomiting, diarrhea, constipation, abdominal pain | Subcutaneous injection |
| Semaglutide (Rybelsus®) | Type 2 diabetes; used off-label for weight loss | GLP-1 receptor agonist | Nausea, diarrhea, decreased appetite | Oral |
| Tirzepatide (Mounjaro®, Zepbound®) | Zepbound: obesity, OSA; Mounjaro: type 2 diabetes | Dual GIP and GLP-1 receptor agonist | Nausea, diarrhea, vomiting, constipation | Subcutaneous injection |
| Ritatrutide | Investigational for obesity and type 2 diabetes | Triple agonist: GIP, GLP-1, and glucagon receptors | Nausea, vomiting, diarrhea | Subcutaneous injection |
| cagrilintide + Semaglutide (CagriSema®) | Investigational for obesity and type 2 diabetes | Combination of cagrilintide (amylin analog) and semaglutide (GLP-1 agonist) | Nausea, vomiting, decreased appetite | Subcutaneous injection |
| Orforglipron | Investigational for obesity and type 2 diabetes | Non-peptide oral GLP-1 receptor agonist | Nausea, vomiting, diarrhea | Oral |
| Setmelanotide (Imcivree®) | Chronic weight management in patients with rare genetic obesity disorders (e.g., POMC deficiency) | MC4 receptor agonist | Skin hyperpigmentation, nausea, injection site reactions | Subcutaneous injection |
| Tesofensine | Investigational for obesity | Triple Monoamine reuptake inhibitor (dopamine, norepinephrine, serotonin) | Dry mouth, nausea, constipation, increased heart rate | Oral |
| Bimagrumab | Investigational for obesity and sarcopenia | human monoclonal antibody targeting Activin type II receptor (ActRII); increases muscle mass, reduces fat | Muscle spasms, diarrhea, fatigue | Intravenous infusion |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ullah, M.I.; Tamanna, S. Obesity: Clinical Impact, Pathophysiology, Complications, and Modern Innovations in Therapeutic Strategies. Medicines 2025, 12, 19. https://doi.org/10.3390/medicines12030019
Ullah MI, Tamanna S. Obesity: Clinical Impact, Pathophysiology, Complications, and Modern Innovations in Therapeutic Strategies. Medicines. 2025; 12(3):19. https://doi.org/10.3390/medicines12030019
Chicago/Turabian StyleUllah, Mohammad Iftekhar, and Sadeka Tamanna. 2025. "Obesity: Clinical Impact, Pathophysiology, Complications, and Modern Innovations in Therapeutic Strategies" Medicines 12, no. 3: 19. https://doi.org/10.3390/medicines12030019
APA StyleUllah, M. I., & Tamanna, S. (2025). Obesity: Clinical Impact, Pathophysiology, Complications, and Modern Innovations in Therapeutic Strategies. Medicines, 12(3), 19. https://doi.org/10.3390/medicines12030019