
The Effects of Mindfulness on Glycemic Control in People with Diabetes: An Overview of Systematic Reviews and Meta-Analyses


Abstract
:1. Introduction
2. Methods
3. Results
3.1. Effects of Mindfulness Interventions on Glycemic Control
3.2. Other Effects of Mindfulness Interventions in People with Diabetes
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2021 Diabetes Collaborators. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: A systematic analysis for the Global Burden of Disease Study 2021. Lancet 2023, 402, 203–234. [Google Scholar] [CrossRef] [PubMed]
- Lakerveld, J.; Palmeira, A.L.; van Duinkerken, E.; Whitelock, V.; Peyrot, M.; Nouwen, A. Motivation: Key to a healthy lifestyle in people with diabetes? Current and emerging knowledge and applications. Diabet. Med. 2020, 37, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.D.; Lindsay, E.K.; Villalba, D.K.; Chin, B. Mindfulness training and physical health: Mechanisms and outcomes. Psychosom. Med. 2019, 81, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Lee, E.K.P.; Mak, E.C.W.; Ho, C.Y.; Wong, S.Y.S. Mindfulness-based interventions: An overall review. Br. Med. Bull. 2021, 138, 41–57. [Google Scholar] [CrossRef]
- Alsubaie, M.; Abbott, R.; Dunn, B.; Dickens, C.; Keil, T.F.; Henley, W.; Kuyken, W. Mechanisms of action in mindfulness-based cognitive therapy (MBCT) and mindfulness-based stress reduction (MBSR) in people with physical and/or psychological conditions: A systematic review. Clin. Psychol. Rev. 2017, 55, 74–91. [Google Scholar] [CrossRef]
- Loucks, E.B.; Schuman-Olivier, Z.; Britton, W.B.; Fresco, D.M.; Desbordes, G.; Brewer, J.A.; Fulwiler, C. Mindfulness and cardiovascular disease risk: State of the evidence, plausible mechanisms, and theoretical framework. Curr. Cardiol. Rep. 2015, 17, 112. [Google Scholar] [CrossRef]
- Tang, Y.Y.; Hölzel, B.K.; Posner, M.I. The neuroscience of mindfulness meditation. Nat. Rev. Neurosci. 2015, 16, 213–225. [Google Scholar] [CrossRef]
- DiNardo, M.M.; Greco, C.; Phares, A.D.; Beyer, N.M.; Youk, A.O.; Obrosky, D.S.; Morone, N.E.; Owen, J.E.; Saba, S.K.; Suss, S.J.; et al. Effects of an integrated mindfulness intervention for veterans with diabetes distress: A randomized controlled trial. BMJ Open Diabetes Res. Care 2022, 10, e002631. [Google Scholar] [CrossRef]
- Baek, R.N.; Tanenbaum, M.L.; Gonzalez, J.S. Diabetes burden and diabetes distress: The buffering effect of social support. Ann. Behav. Med. 2014, 48, 145–155. [Google Scholar] [CrossRef]
- Yadav, A.; Kaushik, R.M.; Kaushik, R. Effects of Diaphragmatic Breathing and Systematic Relaxation on Depression, Anxiety, Stress, and Glycemic Control in Type 2 Diabetes Mellitus. Int. J. Yoga Ther. 2021, 31, Article_13. [Google Scholar] [CrossRef]
- Kurian, J.; Mohanthy, S.; Nanjumdaiah, R.M. Mechanism of action of yoga on prevention and management of type 2 diabetes mellitus: Narrative review. J. Bodyw. Mov. Ther. 2022, 29, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.J.; Koh, E.; Sung, M.K.; Kang, H. Changes induced by mind-body intervention including epigenetic marks and its effects on diabetes. Int. J. Mol. Sci. 2021, 22, 1317. [Google Scholar] [CrossRef]
- García-Campayo, J.; Puebla-Guedea, M.; Labarga, A.; Urdánoz, A.; Roldán, M.; Pulido, L.; de Morentin, X.M.; Perdones-Montero, Á.; Montero-Marín, J.; Mendioroz, M. Epigenetic response to mindfulness in peripheral blood leukocytes involves genes linked to common human diseases. Mindfulness 2018, 9, 1146–1159. [Google Scholar] [CrossRef]
- Aromataris, E.; Fernandez, R.; Godfrey, C.M.; Holly, C.; Khalil, H.; Tungpunkom, P. Summarizing systematic reviews: Methodological development, conduct and reporting of an umbrella review approach. Int. J. Evid. Based Healthc. 2015, 13, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed]
- Ni, Y.; Ma, L.; Li, J. Effects of mindfulness-based stress reduction and mindfulness-based cognitive therapy in people with diabetes: A systematic review and meta-analysis. J. Nurs. Scholarsh. 2020, 52, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, M.; Kopf, S.; Kircher, C.; Faude-Lang, V.; Djuric, Z.; Augstein, F.; Friederich, H.C.; Kieser, M.; Bierhaus, A.; Humpert, P.M.; et al. Sustained effects of a mindfulness-based stress-reduction intervention in type 2 diabetic patients: Design and first results of a randomized controlled trial (the Heidelberger Diabetes and Stress-study). Diabetes Care 2012, 35, 945–947. [Google Scholar] [CrossRef] [PubMed]
- van Son, J.; Nyklícek, I.; Pop, V.J.; Blonk, M.C.; Erdtsieck, R.J.; Spooren, P.F.; Toorians, A.W.; Pouwer, F. The effects of a mindfulness-based intervention on emotional distress, quality of life, and HbA(1c) in outpatients with diabetes (DiaMind): A randomized controlled trial. Diabetes Care 2013, 36, 823–830. [Google Scholar] [CrossRef]
- Kopf, S.; Oikonomou, D.; Hartmann, M.; Feier, F.; Faude-Lang, V.; Morcos, M.; Häring, H.U.; Herzog, W.; Bierhaus, A.; Humpert, P.M.; et al. Effects of stress reduction on cardiovascular risk factors in type 2 diabetes patients with early kidney disease—Results of a randomized controlled trial (HEIDIS). Exp. Clin. Endocrinol. Diabetes 2014, 122, 341–349. [Google Scholar] [CrossRef]
- van Son, J.; Nyklíček, I.; Pop, V.J.; Blonk, M.C.; Erdtsieck, R.J.; Pouwer, F. Mindfulness-based cognitive therapy for people with diabetes and emotional problems: Long-term follow-up findings from the DiaMind randomized controlled trial. J. Psychosom. Res. 2014, 77, 81–84. [Google Scholar] [CrossRef]
- Tovote, K.A.; Fleer, J.; Snippe, E.; Peeters, A.C.; Emmelkamp, P.M.; Sanderman, R.; Links, T.P.; Schroevers, M.J. Individual mindfulness-based cognitive therapy and cognitive behavior therapy for treating depressive symptoms in patients with diabetes: Results of a randomized controlled trial. Diabetes Care 2014, 37, 2427–2434. [Google Scholar] [CrossRef] [PubMed]
- Schroevers, M.J.; Tovote, K.A.; Keers, J.C.; Links, T.P.; Sanderman, R.; Fleer, J. Individual mindfulness-based cognitive therapy for people with diabetes: A pilot randomized controlled trial. Mindfulness 2015, 6, 99–110. [Google Scholar] [CrossRef]
- Nathan, H.J.; Poulin, P.; Wozny, D.; Taljaard, M.; Smyth, C.; Gilron, I.; Sorisky, A.; Lochnan, H.; Shergill, Y. Randomized trial of the effect of mindfulness-based stress reduction on pain-related disability, pain intensity, health-related quality of life, and A1C in patients with painful diabetic peripheral neuropathy. Clin. Diabetes 2017, 35, 294–304. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Yang, J.; Zhao, X.; Kang, S.; Ge, Y.; Qin, L.; Zhang, Y. Effects of mindfulness training on diabetes-related distress and quality of life in patients with type 2 diabetes mellitus. Chin. J. Mod. Nurs. 2018, 24, 186–190. [Google Scholar]
- Teng, L.; Zhao, Q. Effect of mindfulness-base therapy on diabetes distress and quality of life in patients with type 2 diabetes. China J. Health Psychol. 2018, 26, 197–200. [Google Scholar]
- Xiang, Y.; Luo, W.; Lu, G. Effects of mindfulness-based stress reduction in patients with type 2 diabetes mellitus. Prev. Med. 2019, 31, 1068–1069, 1073. [Google Scholar]
- Ellis, D.A.; Carcone, A.I.; Slatcher, R.; Naar-King, S.; Hains, A.; Graham, A.; Sibinga, E. Efficacy of mindfulness-based stress reduction in emerging adults with poorly controlled, type 1 diabetes: A pilot randomized controlled trial. Pediatr. Diabetes 2019, 20, 226–234. [Google Scholar] [CrossRef]
- Ni, Y.X.; Ma, L.; Li, J.P. Effects of mindfulness-based intervention on glycemic control and psychological outcomes in people with diabetes: A systematic review and meta-analysis. J. Diabetes Investig. 2021, 12, 1092–1103. [Google Scholar] [CrossRef]
- Miller, C.K.; Kristeller, J.L.; Headings, A.; Nagaraja, H. Comparison of a mindful eating intervention to a diabetes self-management intervention among adults with type 2 diabetes: A randomized controlled trial. Health Educ. Behav. 2014, 41, 145–154. [Google Scholar] [CrossRef]
- Miller, C.K.; Kristeller, J.L.; Headings, A.; Nagaraja, H.; Miser, W.F. Comparative effectiveness of a mindful eating intervention to a diabetes self-management intervention among adults with type 2 diabetes: A pilot study. J. Acad. Nutr. Diet. 2012, 112, 1835–1842. [Google Scholar] [CrossRef]
- Pearson, S.; Wills, K.; Woods, M.; Warnecke, E. Effects of mindfulness on psychological distress and HbA1c in people with diabetes. Mindfulness 2018, 9, 1615–1626. [Google Scholar] [CrossRef]
- Jung, H.Y.; Lee, H.; Park, J. Comparison of the effects of Korean mindfulness-based stress reduction, walking, and patient education in diabetes mellitus. Nurs. Health Sci. 2015, 17, 516–525. [Google Scholar] [CrossRef] [PubMed]
- Ngan, H.Y.; Chong, Y.Y.; Chien, W.T. Effects of mindfulness- and acceptance-based interventions on diabetes distress and glycaemic level in people with type 2 diabetes: Systematic review and meta-analysis. Diabet. Med. 2021, 38, e14525. [Google Scholar] [CrossRef] [PubMed]
- Gregg, J.A.; Callaghan, G.M.; Hayes, S.C.; Glenn-Lawson, J.L. Improving diabetes self-management through acceptance, mindfulness, and values: A randomized controlled trial. J. Consult. Clin. Psychol. 2007, 75, 336–343. [Google Scholar] [CrossRef]
- Shayeghian, Z.; Hassanabadi, H.; Aguilar-Vafaie, M.E.; Amiri, P.; Besharat, M.A. A randomized controlled trial of acceptance and commitment therapy for type 2 diabetes management: The moderating role of coping styles. PLoS ONE 2016, 11, e0166599. [Google Scholar] [CrossRef]
- Armani Kian, A.; Vahdani, B.; Noorbala, A.A.; Nejatisafa, A.; Arbabi, M.; Zenoozian, S.; Nakhjavani, M. The impact of mindfulness-based stress reduction on emotional wellbeing and glycemic control of patients with type 2 diabetes mellitus. J. Diabetes Res. 2018, 2018, 1986820. [Google Scholar] [CrossRef]
- Maghsoudi, Z.; Razavi, Z.; Razavi, M.; Javadi, M. Efficacy of acceptance and commitment therapy for emotional distress in the elderly with type 2 diabetes: A randomized controlled trial. Diabetes Metab. Syndr. Obes. 2019, 12, 2137–2143. [Google Scholar] [CrossRef]
- Whitehead, L.C.; Crowe, M.T.; Carter, J.D.; Maskill, V.R.; Carlyle, D.; Bugge, C.; Frampton, C.M.A. A nurse-led education and cognitive behaviour therapy-based intervention among adults with uncontrolled type 2 diabetes: A randomised controlled trial. J. Eval. Clin. Pract. 2017, 23, 821–829. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Brozek, J.L.; Canelo-Aybar, C.; Akl, E.A.; Bowen, J.M.; Bucher, J.; Chiu, W.A.; Cronin, M.; Djulbegovic, B.; Falavigna, M.; Guyatt, G.H.; et al. GRADE Working Group GRADE Guidelines 30: The GRADE approach to assessing the certainty of modeled evidence-An overview in the context of health decision-making. J. Clin. Epidemiol. 2021, 129, 138–150. [Google Scholar] [CrossRef]
- Forman, E.M.; Butryn, M.L. A new look at the science of weight control: How acceptance and commitment strategies can address the challenge of self-regulation. Appetite 2015, 84, 171–180. [Google Scholar] [CrossRef]
- Heo, S.; Kang, J.; Umeakunne, E.; Lee, S.; Bertulfo, T.F.; Barbé, T.; Kim, J.; Black, V.; An, M.; Randolph, J. Effects of meditation intervention on self-management in adult patients with type 2 diabetes: A systematic literature review and meta-analysis. J. Cardiovasc. Nurs. 2023; Epub ahead of print. [Google Scholar] [CrossRef]
- Chen, S.M.; Lin, H.S.; Atherton, J.J.; MacIsaac, R.J.; Wu, C.J. Effect of a mindfulness programme for long-term care residents with type 2 diabetes: A cluster randomised controlled trial measuring outcomes of glycaemic control, relocation stress and depression. Int. J. Older People Nurs. 2020, 15, e12312. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Wang, H.; Ge, L.; Valimaki, M.; Wiley, J.; Whittemore, R. Effectiveness of a nurse-led mindfulness stress-reduction intervention on diabetes distress, diabetes self-management, and HbA1c levels among people with type 2 diabetes: A pilot randomized controlled trial. Res. Nurs. Health 2022, 45, 46–58. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, S.S.; Ahadi, M.; Hatami, M.; Khalatbari, J. Effectiveness of mindfulness-based therapy on resilience, psychological well-being, and blood sugar levels in patients with type II diabetes. Razavi Int. J. Med. 2021, 9, 74–80. [Google Scholar]
- Ravari, O.N.; Mousavi, S.Z.; Babak, A. Evaluation of the effects of 12 weeks mindfulness-based stress reduction on glycemic control and mental health indices in women with diabetes mellitus type 2. Adv. Biomed. Res. 2020, 9, 61. [Google Scholar]
- Xiao, L. Blood sugar reduction of type 2 diabetic patients through a mindfulness intervention program. NeuroQuantology 2018, 16, 57–62. [Google Scholar] [CrossRef]
- Bersch-Ferreira, Â.C.; Weber, B.; da Silva, J.G.S.T.; Pagano, R.; Figueiro, M.F.; da Silva, L.R.; de Souza Mota, L.G.; Suzumura, E.A.; Torreglosa, C.R.; de Sousa Lara, E.; et al. Mindfulness practice for glycemic control: Could it be a new strategy for an old problem? A systematic review and meta-analysis. Curr. Diabetes Rev. 2021, 17, 65–80. [Google Scholar] [CrossRef]
- Pascoe, M.C.; Thompson, D.R.; Ski, C.F. Yoga, mindfulness-based stress reduction and stress-related physiological measures: A meta-analysis. Psychoneuroendocrinology 2017, 86, 152–168. [Google Scholar] [CrossRef]
- Marinovic, D.A.; Hunter, R.L. Examining the interrelationships between mindfulness-based interventions, depression, inflammation, and cancer survival. CA Cancer J. Clin. 2022, 72, 490–502. [Google Scholar] [CrossRef]
- Black, D.S.; Slavich, G.M. Mindfulness meditation and the immune system: A systematic review of randomized controlled trials. Ann. N. Y. Acad. Sci. 2016, 1373, 13–24. [Google Scholar] [CrossRef]
- O’Reilly, G.A.; Cook, L.; Spruijt-Metz, D.; Black, D.S. Mindfulness-based interventions for obesity-related eating behaviours: A literature review. Obes. Rev. 2014, 15, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Mason, A.E.; Epel, E.S.; Kristeller, J.; Moran, P.J.; Dallman, M.; Lustig, R.H.; Acree, M.; Bacchetti, P.; Laraia, B.A.; Hecht, F.M.; et al. Effects of a mindfulness-based intervention on mindful eating, sweets consumption, and fasting glucose levels in obese adults: Data from the SHINE randomized controlled trial. J. Behav. Med. 2016, 39, 201–213. [Google Scholar] [CrossRef] [PubMed]
- Sala, M.; Geary, B.; Baldwin, A.S. A mindfulness-based physical activity intervention: A randomized pilot study. Psychosom. Med. 2021, 83, 615–623. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat. Rev. Endocrinol. 2018, 14, 88–98. [Google Scholar] [CrossRef]
- Avogaro, A.; Fadini, G.P. Microvascular complications in diabetes: A growing concern for cardiologists. Int. J. Cardiol. 2019, 291, 29–35. [Google Scholar] [CrossRef]
- Clark, E.L.M.; Gulley, L.D.; Prince, M.A.; Casamassima, M.; Sanchez, N.; Jimenez, V.; Johnson, S.A.; Miller, R.L.; Conte, I.; Kaar, J.L.; et al. The role of mindfulness in associations among depression symptoms, sleep duration, and insulin resistance in adolescents. J. Behav. Med. 2021, 44, 694–703. [Google Scholar] [CrossRef]
- Fulton, S.; Décarie-Spain, L.; Fioramonti, X.; Guiard, B.; Nakajima, S. The menace of obesity to depression and anxiety prevalence. Trends Endocrinol. Metab. 2022, 33, 18–35. [Google Scholar] [CrossRef]
- Higgins, J.P.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A. Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; John Wiley & Sons: Chichester, UK, 2019; Chapter 8; pp. 205–228. [Google Scholar]
- Margolis, K.G.; Cryan, J.F.; Mayer, E.A. The Microbiota-Gut-Brain Axis: From Motility to Mood. Gastroenterology 2021, 160, 1486–1501. [Google Scholar] [CrossRef]
- Tan, H.E. The microbiota-gut-brain axis in stress and depression. Front. Neurosci. 2023, 17, 1151478. [Google Scholar] [CrossRef]
- Iatcu, C.O.; Steen, A.; Covasa, M. Gut Microbiota and Complications of Type-2 Diabetes. Nutrients 2021, 14, 166. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Sun, B.; Yu, D.; Zhu, C. Gut Microbiota: An Important Player in Type 2 Diabetes Mellitus. Front. Cell Infect. Microbiol. 2022, 12, 834485. [Google Scholar] [CrossRef] [PubMed]
- Househam, A.M. Effects of stress and mindfulness on epigenetics. In Vitamins and Hormones; Litwack, G., Ed.; Elsevier: Amsterdam, The Netherlands, 2023; Volume 122, pp. 283–306. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.F.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
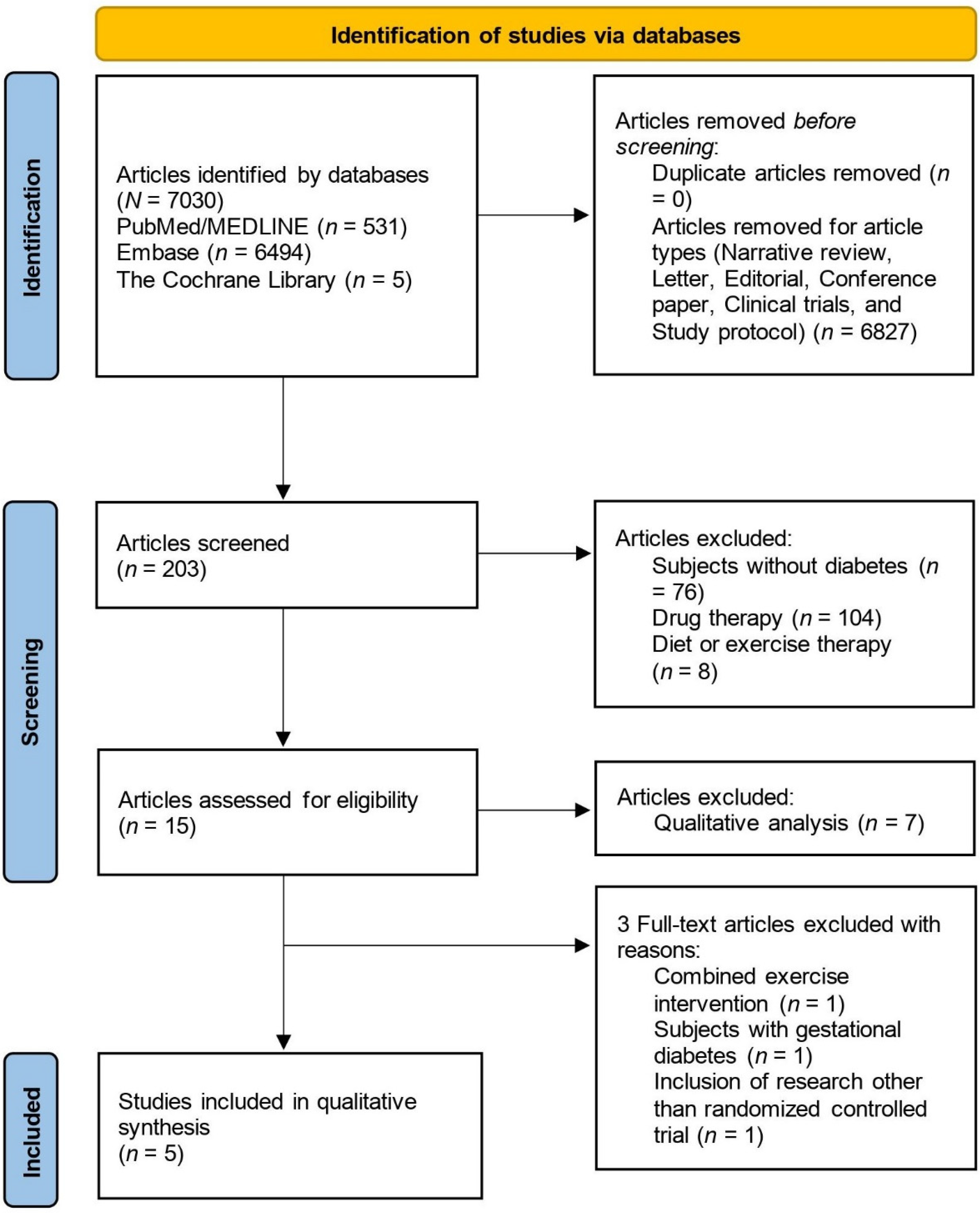

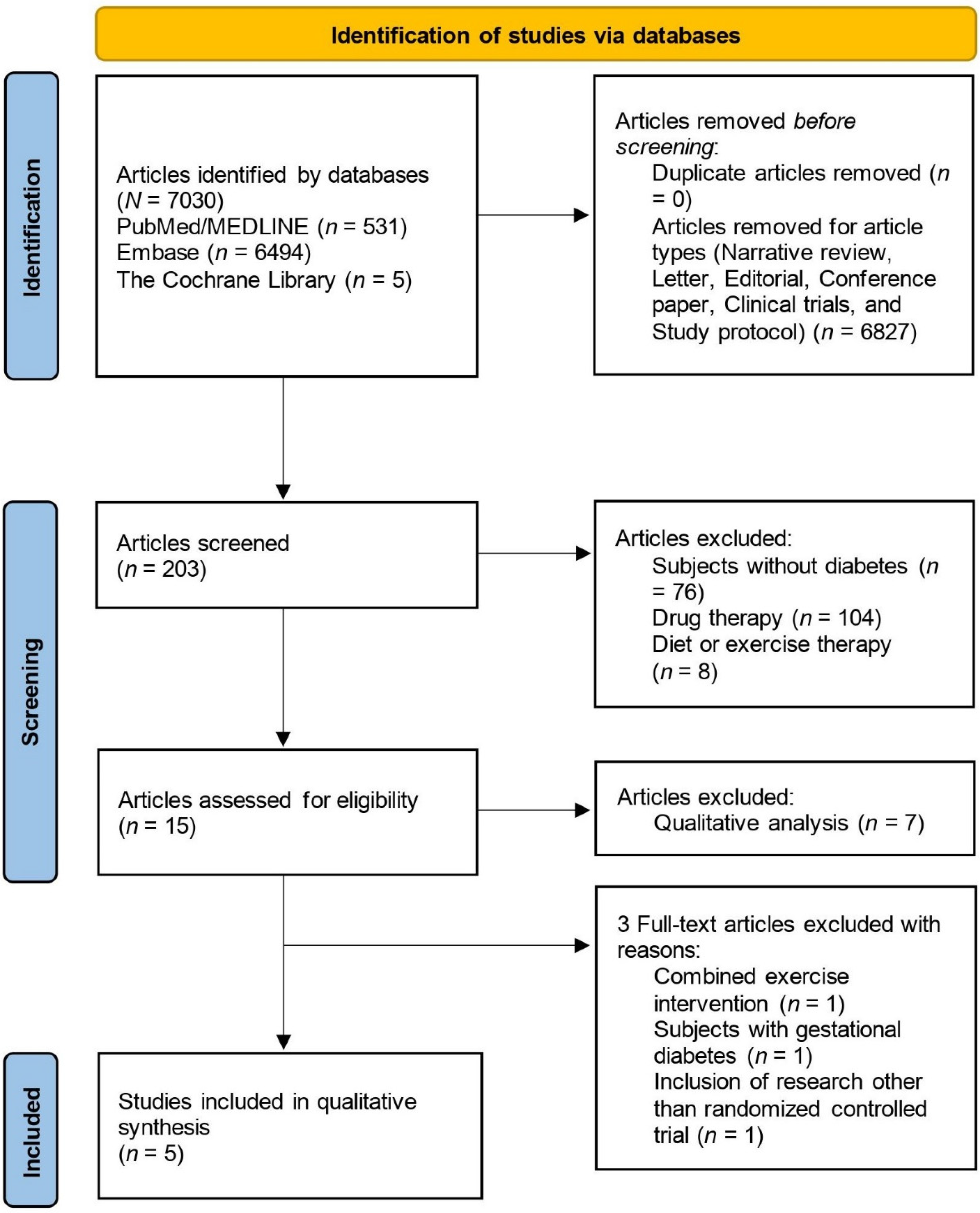{kind=link}
| Authors, Year | Subjects | Interventions | Comparators | Outcomes | Results |
|---|---|---|---|---|---|
| Ni et al., 2020 [16] | People with type 2 or type 1 diabetes Age: 18.0–68.7 years in the intervention group; 18.5–59.8 years in the control group Sex (male): 44–78.2% | MBSR or MBCT Method of conducting sessions: Face-to-face (individual or group), video group Duration of sessions: 45–180 min/session Number of sessions: 6–9 sessions Duration of interventions: 2–9 weeks | Usual care, wait-list, no intervention, or health education | HbA1c, QoL, depression | HbA1c levels ↓ QoL ↑ Depression ↓ |
| Ni et al., 2021 [28] | People with type 2 or type 1 diabetes Age: No description Sex (male): 36.6–78.2% | MBSR, MBCT, MB-EAT, or unspecific mindfulness-based intervention Method of conducting sessions: Face-to-face (individual or group), using audio compact disc at home Duration of sessions: 30–150 min/session Number of sessions: 8–9 sessions Duration of interventions: 8 weeks–3 months | Usual care, walking, patient education, diabetes self-management education-based intervention, wait-list, CBT | HbA1c, stress, depression, anxiety, distress | HbA1c levels ↓ Diabetes-related distress ↓ Stress ↓ Depression ↓ Anxiety → (based on a qualitative synthesis) |
| Ngan et al., 2020 [33] | People with type 2 or type 1 diabetes Age: 53.8–66.3 years (mean) Sex: No description | MBSR, MBCT, acceptance and commitment therapy, or self-directed mindfulness practice Method of conducting sessions: Face-to-face (individual or group), using audio compact disc at home Duration of sessions: 30–420 (one day workshop) min/session Number of sessions: 1–10 sessions Duration of interventions: One day (7-h workshop)–10 weeks | Diabetes education, usual care, annual routine visit, no intervention | HbA1c, diabetes distress, diabetes self-management, psychological symptoms | HbA1c levels ↓ Diabetes distress ↓ Self-management → Anxiety ↓ Depression ↓ |
| Heo et al., 2023 [42] | People with type 2 diabetes Age: 42.1–78.9 years (mean) Sex (male): 0–78.2% | MBSR, MBCT, or mindfulness meditation program Method of conducting sessions: Face-to-face (individual or group), using audio compact disc at home Duration of sessions: 30–150 min/session Number of sessions: 8–10 sessions Duration of interventions: 8–10 weeks | Usual care, diabetes education, wait-list, walking | Blood glucose levels, HbA1c, self-management (e.g., diet, exercise, blood pressure, cholesterol, obesity, and foot care) | HbA1c levels ↓ Fasting blood glucose levels → Self-management (unknown) |
| Bersch-Ferreira et al., 2021 [48] | People with type 2 diabetes Age: 53.5–68.5 years (mean) Sex (male/female): 188/134 | MBSR and MB-EAT Method of conducting sessions: Face-to-face (individual or group) Duration of sessions: 30–150 min/session Number of sessions: 6–8 sessions Duration of interventions: 8–12 weeks | Usual care, diabetes education, walking, no intervention | Blood glucose levels, HbA1c | HbA1c → Blood glucose levels → |
| Ni et al., 2020 [16] | Ni et al., 2021 [28] | Ngan et al., 2020 [33] | Heo et al., 2023 [42] | Bersch-Ferreira et al., 2021 [48] | |
|---|---|---|---|---|---|
| 1. Did the research questions and inclusion criteria for the review include the components of PICO? | Yes | Yes | Yes | Yes | Yes |
| 2. Did the report of the review contain an explicit statement that the review methods were established prior to conducting the review and did the report justify any significant deviations from the protocol? | Yes | Yes | Unclear | Unclear | Yes |
| 3. Did the review authors explain their selection of the study designs for inclusion in the review? | Yes | Yes | Yes | Yes | Yes |
| 4. Did the review authors use a comprehensive literature search strategy? | Yes | Yes | Yes | Yes | Yes |
| 5. Did the review authors perform study selection in duplicate? | Yes | Yes | Yes | Yes | Yes |
| 6. Did the review authors perform data extraction in duplicate? | Yes | Yes | Yes | Yes | Yes |
| 7. Did the review authors provide a list of excluded studies and justify the exclusions? | Yes | Yes | Yes | Yes | Yes |
| 8. Did the review authors describe the included studies in adequate detail? | No | No | No | No | Partly Yes |
| 9. Did the review authors use a satisfactory technique for assessing the risk of bias (RoB) in individual studies that were included in the review? | Yes | Yes | Yes | Yes | Yes |
| 10. Did the review authors report on the sources of funding for the studies included in the review? | No | No | No | No | No |
| 11. If meta-analysis was performed, did the review authors use appropriate methods for statistical combination of results? | Yes | Yes | Yes | Yes | Yes |
| 12. If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? | Yes | Yes | Yes | Yes | Yes |
| 13. Did the review authors account for RoB in individual studies when interpreting/discussing the results of the review? | Yes | Yes | Yes | Yes | Yes |
| 14. Did the review authors provide a satisfactory explanation for and discussion of any heterogeneity observed in the results of the review? | Yes | Yes | Yes | Yes | Yes |
| 15. If they performed quantitative synthesis, did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review? | Unassesable | Unassesable | Unassesable | Unassesable | Unassesable |
| 16. Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? | No | Yes | Yes | Yes | Yes |
| Rating result | Low | Moderate | Low | Low | Moderate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamasaki, H. The Effects of Mindfulness on Glycemic Control in People with Diabetes: An Overview of Systematic Reviews and Meta-Analyses. Medicines 2023, 10, 53. https://doi.org/10.3390/medicines10090053
Hamasaki H. The Effects of Mindfulness on Glycemic Control in People with Diabetes: An Overview of Systematic Reviews and Meta-Analyses. Medicines. 2023; 10(9):53. https://doi.org/10.3390/medicines10090053
Chicago/Turabian StyleHamasaki, Hidetaka. 2023. "The Effects of Mindfulness on Glycemic Control in People with Diabetes: An Overview of Systematic Reviews and Meta-Analyses" Medicines 10, no. 9: 53. https://doi.org/10.3390/medicines10090053
APA StyleHamasaki, H. (2023). The Effects of Mindfulness on Glycemic Control in People with Diabetes: An Overview of Systematic Reviews and Meta-Analyses. Medicines, 10(9), 53. https://doi.org/10.3390/medicines10090053