
Subjective Symptoms Linked to Sleep Duration: An Analysis from Japanese National Statistics

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
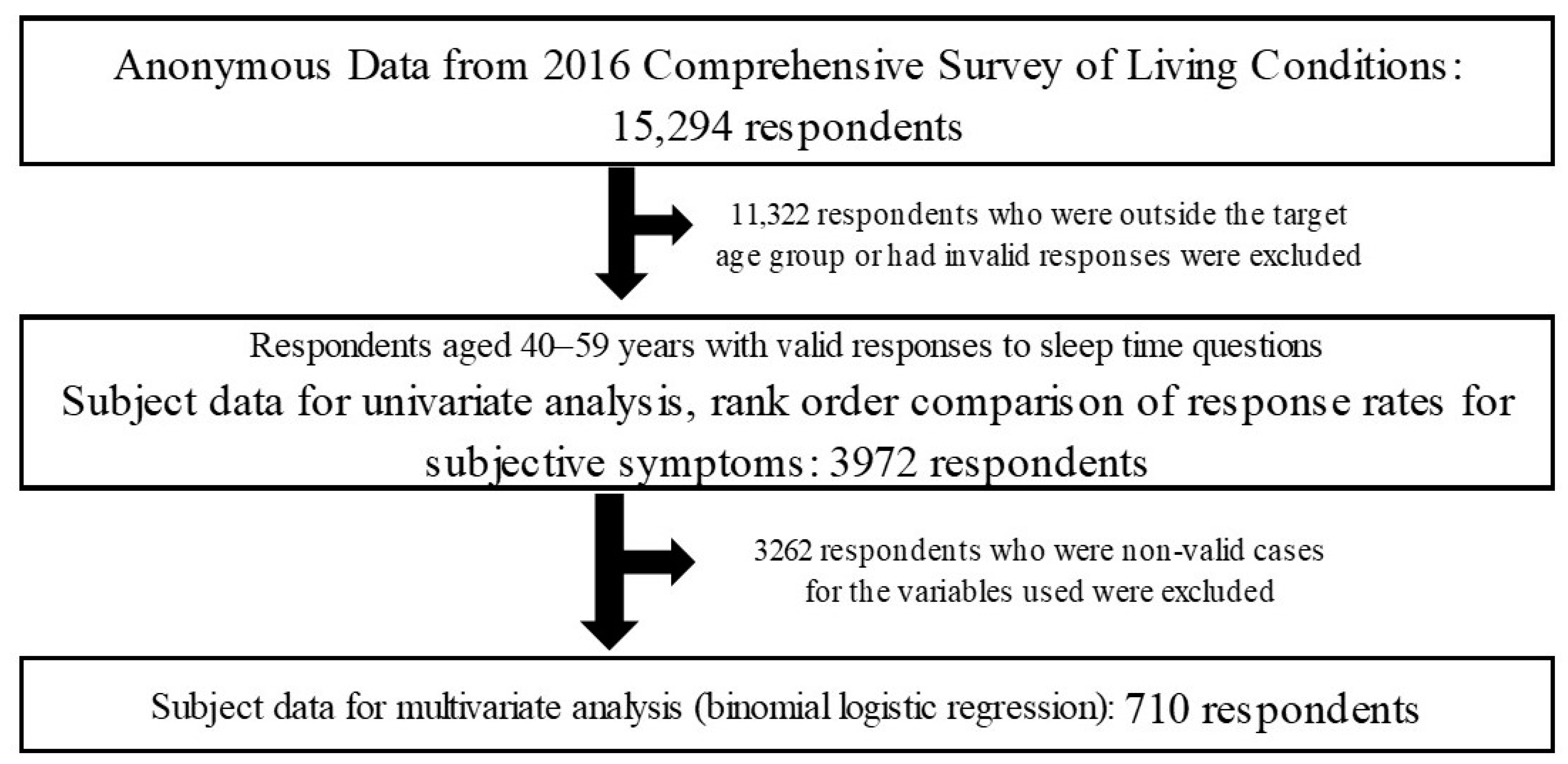
2.1. Study Design and Resource Database
2.2. Selection of Subjects and Classification into Sleep Duration Groups
2.3. Comparison of Response Rate for Each Survey Item between Sleep Duration Groups
2.4. Comparison of the Response Rate Ranking for Each Subjective Symptom between Sleep Duration Groups
2.5. Investigation of the Degree of Effect on Sleep Duration and Subjective Health Assessment by Multivariate Analysis (Binomial Logistic Regression)
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
3.1. Classification into Groups by Sleep Duration
3.2. Univariate Analysis of Sex and Other Survey Items with Sleep Duration
3.3. Univariate Analysis of Responses for Subjective Symptoms and Sleep Duration
3.4. Comparison of Ranking of Response Rates for Subjective Symptoms by Sleep Duration Group
3.5. Multivariate Analyses with Sleep Duration and Subjective Health Assessment as Objective Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sateia, M.J. International Classification of Sleep Disorders-Third Edition. Highlights and modifications. CHEST 2014, 146, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). International Classification of Diseases 11th Revision. Available online: https://www.who.int/standards/classifications/classification-of-diseases (accessed on 25 July 2023).
- Hassan, W.; Zafar, M.; Noreen, H.; Ara, A.; Duarte, A.E.; Kamdem, J.P.; Kamal, M.A.; Rocha, J.B.T. Sleep disorders research from 1945 to 2020: A bibliometric analysis. CNS Neurol. Disord. Drug Targets 2021, 20, 574–593. [Google Scholar] [CrossRef]
- OECD. Gender Data Portal 2021. Data on Time Use. Available online: http://www.oecd.org/gender/data/ (accessed on 25 July 2023).
- Ohtsu, T.; Kaneita, Y.; Aritake, S.; Mishima, K.; Uchiyama, M.; Akashiba, T.; Uchimura, N.; Nakaji, S.; Munezawa, T.; Kokaze, A.; et al. A cross-sectional study of the association between working hours and sleep duration among the Japanese working population. J. Occup. Health 2013, 55, 307–311. [Google Scholar] [CrossRef]
- Svensson, T.; Inoue, M.; Saito, E.; Sawada, N.; Iso, H.; Mizoue, T.; Goto, A.; Yajima, T.; Shimizu, T.; Iwasaki, M.; et al. The association between habitual sleep duration and mortality according to sex and age: The Japan Public Health Center-based Prospective Study. J. Epidemiol. 2021, 31, 109–118. [Google Scholar] [PubMed]
- Sullivan, C.E.; Issa, F.G.; Berthon, J.M.; Eves, L. Reversal of obstructive sleep apnea by continuous positive airway pressure applied through the nares. Lancet 1981, 1, 862–865. [Google Scholar] [CrossRef]
- Tamakoshi, A.; Ohno, Y.; JACC Study Group. Self-reported sleep duration as a predictor of all-cause mortality: Results from the JACC study, Japan. Sleep 2004, 27, 51–54. [Google Scholar] [PubMed]
- Liu, X.; Uchyama, M.; Kim, K.; Okawa, M.; Shibui, K.; Kudo, Y.; Doi, Y.; Minowa, M.; Ogihara, R. Sleep loss and daytime sleepiness in the general adult population of Japan. Psychiatry Res. 2000, 93, 1–11. [Google Scholar]
- Ikeda, H.; Matsumoto, S.; Kubo, T.; Izawa, S.; Takahashi, M. Relationship between sleep problems and dangerous driving behaviors in Japanese short-haul commercial truck drivers: A cross-sectional survey using digital tachograph data. Sleep Biol. Rhythms 2021, 19, 297–303. [Google Scholar]
- National Institute of Health and Nutrition; Health Japan 21 (the Second Term). Available online: https://www.nibiohn.go.jp/eiken/kenkounippon21/en/kenkounippon21 (accessed on 25 July 2022).
- Komatsuzaki, A.; Ono, S. Study of the effects of recognition of stress on symptoms and regular hospital visits: An analysis from Japanese National Statistics. Healthcare 2020, 8, 274. [Google Scholar] [CrossRef]
- Kamoda, T.; Komatsuzaki, A.; Ono, S.; Tanaka, S.; Yokoi, Y. Association between drinking habits and oral symptoms: A cross-sectional study based on Japanese National Statistical Data. Int. J. Dent. 2020, 2020, 8874587. [Google Scholar] [CrossRef]
- Ono, S.; Komatsuzaki, A.; Yokoi, Y.; Kamoda, T. A study of the effects of smoking on recognition of symptoms and subjective health. Int. J. Clin. Prev. Dent. 2020, 16, 80–87. [Google Scholar] [CrossRef]
- Dement, W.C.; Miles, L.E.; Garskadon, M.A. White paper on sleep and aging. J. Am. Geriatr. Soc. 1982, 30, 25–50. [Google Scholar] [PubMed]
- Dement, W.C. Wake up America: A National Sleep Alert: Executive Summary and Executive Report, Report of the National Commission on Sleep Disorders Research; National Institutes of Health, US Department of Health and Human Services: Washington, DC, USA, 1993.
- Yi, H.; Shin, K.; Shin, C. Development of the Sleep Quality Scale. J. Sleep Res. 2006, 15, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Kageyama, T.; Nishikido, N.; Kobayashi, T.; Kawagoe, H. Estimated sleep debt and work stress in Japanese white-collar workers. Psychiatry Clin. Neurosci. 2001, 55, 217–219. [Google Scholar] [CrossRef]
- Roth, T.; Ancoli, I.S. Daytime consequences and correlates of insomnia in the United States: Results of the 1991 Nation Sleep Foundation Survey II. Sleep 1999, 22 (Suppl. S12), 354–358. [Google Scholar]
- OECD. Average Minutes per Day Spent Sleeping in OECD Countries plus China, India and South Africa by Gender, as of 2016. Available online: https://www.statista.com/statistics/521957/time-spent-sleeping-countries (accessed on 25 July 2023).
- Iwasaki, K.; Takahashi, M.; Nakata, A. Health problems due to long working hours in Japan: Working hours, worker’s compensation (Karoshi), and preventive measures. Ind. Health 2006, 44, 537–540. [Google Scholar] [PubMed]
- Wada, K.; Sakata, Y.; Theriault, G.; Narai, R.; Yoshino, Y.; Tanaka, K.; Aizawa, Y. Associations of excessive sleepiness on duty with sleeping hours and number of days of overnight work among medical residents in Japan. J. Occup. Health 2007, 49, 523–527. [Google Scholar] [CrossRef]
- Ishibashi, Y.; Shimamura, A. Association between work productivity and sleep health: A cross-sectional study in Japan. Sleep Health 2020, 6, 270–276. [Google Scholar] [CrossRef]
- Ohida, T.; Kamal, A.M.; Uchiyama, M.; Kim, K. The influence of lifestyle and health status factors on sleep loss among the Japanese general population. Sleep 2001, 24, 333–338. [Google Scholar] [CrossRef]
- Kripke, D.F.; Garfinkel, L.; Wingard, D.L.; Klauber, M.R.; Marler, M.R. Mortality associated with sleep duration and insomnia. Arch. Gen. Psychiatry 2002, 59, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Yokoi, Y.; Komatsuzaki, A. How sleep quality relates to bodily and oral symptoms: An analysis from Japanese National Statistics. Healthcare 2022, 10, 2298. [Google Scholar] [CrossRef] [PubMed]
- Amagi, Y.; Ishikawa, S.; Gotoh, T.; Kayaba, K.; Nakamura, Y.; Kajii, E. Sleep duration and incidence of cardiovascular events in a Japanese population: The Jichi Medical School Cohort Study. J. Epidemiol. 2010, 20, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Hayashino, Y.; Yamazaki, S.; Nakayama, T.; Soejima, S.; Fukuhara, S. Relationship between diabetes mellitus and excessive sleepiness during driving. Exp. Clin. Endocrinol. Diabetes 2008, 116, 1–5. [Google Scholar] [CrossRef]
- Sejbuk, M.; Chodakowska, I.M.; Witkowska, A.M. Sleep quality: A narrative review on nutrition, stimulants and physical activity as important factors. Nutrients 2022, 14, 1912. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Carlson, S.A.; Wheaton, A.G.; Greenlund, K.J.; Croft, J.B. Sleep disorder symptoms among adults in 8 states and the District of Columbia, 2017. Prev. Chronic Dis. 2021, 18, E105. [Google Scholar] [CrossRef]
- Spiegelhalder, K.; Regen, W.; Nanovska, S.; Baglioni, C.; Riemann, D. Comorbid sleep disorder in neuropsychiatric disorders across the life cycle. Curr. Psychatry Rep. 2013, 15, 364. [Google Scholar] [CrossRef]
- Koutsourelakis, I.; Kontovazainitis, G.; Lamprou, K.; Gogou, E.; Samartzi, E.; Tzakis, M. The role of sleep endoscopy in oral appliance therapy for obstructive sleep apnea. Auris. Nasus. Larynx. 2021, 48, 255–260. [Google Scholar] [CrossRef]
- Saczuk, K.; Lapinska, B.; Wilmont, P.; Pawlak, L.; Szymanska, M.L. Relationship between sleep bruxism, perceived stress, and coping strategies. Int. J. Environ. Res. 2019, 16, 3193. [Google Scholar] [CrossRef]
- Ohkuma, T.; Fujii, H.; Iwase, M.; Kikuchi, Y.; Ogata, S.; Idewaki, Y.; Ide, H.; Doi, Y.; Hirakawa, Y.; Nakamura, U.; et al. Impact of sleep duration on obesity and the glycemic level in patients with type 2 diabetes: The Fukuoka Diabetes Registry. Diabetes Care 2013, 36, 611–617. [Google Scholar] [CrossRef]
- Frauscher, B.; Brandauer, E.; Gschliesser, V.; Falkenstetter, T.; Furtner, M.T.; Ulmer, H.; Poewe, W.; Högl, B. A descriptive analysis of neck myoclonus during routine polysomnography. Sleep 2010, 33, 1091–1096. [Google Scholar] [CrossRef]
- Dongen, H.P.A.V.; Rogers, N.L.; Dinges, D.F. Sleep debt: Theoretical and empirical issues. Sleep Biol. Rhythms 2003, 1, 5–13. [Google Scholar] [CrossRef]
- Gallina, S.; Dispenza, F.; Kulamarva, G.; Riggio, F.; Speciale, R. Obstructive sleep apnoea syndrome (OSAS): Effects on the vestibular system. Acta Otorhinolaryngo 2010, 30, 281–284. [Google Scholar]
- Kawada, T. Magnesium-containing laxative agent in senile patients with chronic constipation: Age, sex and drug interactions for risk assessment. Geriatr. Gerontol. Int. 2023, 23, 154–155. [Google Scholar] [CrossRef] [PubMed]
- Kageyama, T.; Nishikido, N.; Kobayashi, T.; Kurokawa, Y.; Kaneko, T.; Kabuto, M. Self-reported sleep quality, job stress, and daytime autonomic activities in terms of short-term heart rate variability among male white-collar workers. Ind. Health 1998, 36, 263–272. [Google Scholar] [CrossRef]
- Cappuccio, F.P.; D’Elia, L.; Strazzullo, P.; Miller, M.A. Sleep duration and all-cause mortality: A systematic review and meta-analysis of prospective studies. Sleep 2010, 33, 585–592. [Google Scholar] [CrossRef]
- Andreasson, A.; Axelsson, J.; Bosch, J.A.; Balter, L.J.T. Poor sleep quality is associated with worse self-rated health in long sleep duration but not short sleep duration. Sleep Med. 2021, 88, 262–266. [Google Scholar] [CrossRef]
- Masse, M.; Henry, H.; Cuvelier, E.; Pinçon, C.; Pavy, M.; Beeuwsaert, A.; Barthélémy, C.; Cuny, D.; Gautier, S.; Kambia, N.; et al. Sleep medication in older adults: Identifying the need for support by a community pharmacist. Healthcare 2022, 10, 147. [Google Scholar] [CrossRef]


{kind=link}
| Item | Response (§) | <6 h | (%) | ≥6 h | (%) | Total | (%) | χ2 Test | Odds Ratio | 95% CI |
|---|---|---|---|---|---|---|---|---|---|---|
| Sex | Woman (1) | 1027 | (50.5) | 1006 | (49.5) | 2033 | (100.0) | ** | 1.34 | 1.19–1.52 |
| Man (0) | 837 | (43.2) | 1102 | (56.8) | 1939 | (100.0) | ||||
| Age | 50s | 897 | (47.1) | 1007 | (52.9) | 1904 | (100.0) | 1.01 | 0.89–1.14 | |
| 40s | 967 | (46.8) | 1101 | (53.2) | 2068 | (100.0) | ||||
| Outpatient treatment | Yes (1) | 721 | (49.5) | 737 | (50.6) | 1458 | (100.0) | * | 1.17 | 1.03–1.33 |
| No (0) | 1137 | (45.5) | 1361 | (54.5) | 2498 | (100.0) | ||||
| Working hours per week | ≥56 h (1) | 562 | (50.2) | 558 | (49.8) | 1120 | (100.0) | ** | 1.20 | 1.05–1.38 |
| <56 h (0) | 1274 | (45.6) | 1522 | (54.4) | 2796 | (100.0) | ||||
| household economy | Difficult (1) | 1089 | (48.4) | 1159 | (51.6) | 2248 | (100.0) | * | 1.15 | 1.01–1.30 |
| Normal, Comfortable (0) | 775 | (49.0) | 949 | (55.1) | 1724 | (100.0) | ||||
| Worries and stress | Yes (1) | 1121 | (52.4) | 1017 | (51.6) | 2138 | (100.0) | ** | 1.62 | 1.43–1.84 |
| No (0) | 743 | (40.5) | 1091 | (55.1) | 1834 | (100.0) | ||||
| Effect on everyday life | Effect | 174 | (50.9) | 168 | (49.1) | 342 | (100.0) | 1.18 | 0.95–1.02 | |
| No effect | 1690 | (46.6) | 1940 | (53.4) | 3630 | (100.0) | ||||
| Subjective health assessment | Bad, Not good (1) | 266 | (57.7) | 195 | (42.3) | 461 | (100.0) | ** | 1.63 | 1.34–1.98 |
| Not bad, Good, Very good (0) | 1598 | (45.5) | 1913 | (54.5) | 3511 | (100.0) |
| Symptom | Response (§) | <6 h | (%) | ≥6 h | (%) | Total | (%) | χ2 Test | Odds Ratio | 95% CI |
|---|---|---|---|---|---|---|---|---|---|---|
| Presence of subjective symptoms | Yes | 640 | (52.6) | 576 | (47.4) | 1216 | (100.0) | ** | 1.39 | 1.21–1.59 |
| No | 1214 | (44.4) | 1520 | (55.6) | 2734 | (100.0) | ||||
| Stiff shoulders | Yes (1) | 291 | (58.0) | 211 | (42.0) | 502 | (100.0) | ** | 1.44 | 1.15–1.82 |
| No (0) | 349 | (48.9) | 365 | (51.1) | 714 | (100.0) | ||||
| Lower back pain | Yes (1) | 255 | (55.2) | 207 | (44.8) | 462 | (100.0) | 1.18 | 0.94–1.49 | |
| No (0) | 385 | (51.1) | 369 | (48.9) | 754 | (100.0) | ||||
| Headache | Yes (1) | 128 | (58.7) | 90 | (41.3) | 218 | (100.0) | * | 1.35 | 1.00–1.82 |
| No (0) | 512 | (51.3) | 486 | (48.7) | 998 | (100.0) | ||||
| Lethargic | Yes (1) | 126 | (58.6) | 89 | (41.4) | 215 | (100.0) | 1.34 | 0.99–1.81 | |
| No (0) | 514 | (51.4) | 487 | (48.6) | 1001 | (100.0) | ||||
| Joint pain in hands/feet | Yes (1) | 117 | (60.2) | 76 | (39.4) | 193 | (100.0) | * | 1.47 | 1.08–2.01 |
| No (0) | 523 | (51.1) | 500 | (48.9) | 1023 | (100.0) | ||||
| Blocked/runny nose | Yes (1) | 83 | (49.4) | 85 | (50.6) | 168 | (100.0) | 0.86 | 0.62–1.19 | |
| No (0) | 557 | (53.2) | 491 | (46.8) | 1048 | (100.0) | ||||
| Cough, phlegmatic | Yes (1) | 87 | (53.1) | 77 | (46.9) | 164 | (100.0) | 1.01 | 0.73–1.41 | |
| No (0) | 553 | (52.6) | 499 | (47.4) | 1052 | (100.0) | ||||
| Blurred vision | Yes (1) | 84 | (58.3) | 60 | (41.7) | 144 | (100.0) | 1.29 | 0.91–1.85 | |
| No (0) | 556 | (51.9) | 516 | (48.1) | 1072 | (100.0) | ||||
| Visual impairment | Yes (1) | 85 | (59.4) | 58 | (40.6) | 143 | (100.0) | 1.36 | 0.95–1.95 | |
| No (0) | 555 | (51.7) | 518 | (48.3) | 1073 | (100.0) | ||||
| Numb limbs | Yes (1) | 82 | (58.2) | 59 | (41.8) | 141 | (100.0) | 1.28 | 0.91–1.84 | |
| No (0) | 558 | (51.9) | 517 | (48.1) | 1075 | (100.0) | ||||
| Irritable | Yes (1) | 86 | (64.2) | 48 | (35.8) | 134 | (100.0) | ** | 1.71 | 1.17–2.48 |
| No (0) | 554 | (51.2) | 528 | (48.8) | 1082 | (100.0) | ||||
| Itchiness (eczema, athlete’s foot, etc.) | Yes (1) | 68 | (53.5) | 59 | (46.5) | 127 | (100.0) | 1.04 | 0.72–1.51 | |
| No (0) | 572 | (52.5) | 517 | (47.5) | 1089 | (100.0) | ||||
| Swollen/heavy feet | Yes (1) | 67 | (59.3) | 46 | (40.7) | 113 | (100.0) | 1.35 | 0.91–1.99 | |
| No (0) | 573 | (51.9) | 530 | (48.1) | 1103 | (100.0) | ||||
| Ringing ears | Yes (1) | 68 | (63.6) | 39 | (36.4) | 107 | (100.0) | * | 1.64 | 1.09–2.47 |
| No (0) | 572 | (51.6) | 537 | (48.4) | 1109 | (100.0) | ||||
| Poor sleep quality | Yes (1) | 70 | (70.0) | 30 | (30.0) | 100 | (100.0) | ** | 2.24 | 1.43–3.48 |
| No (0) | 570 | (51.1) | 546 | (48.9) | 1116 | (100.0) | ||||
| Dizziness | Yes (1) | 64 | (65.3) | 34 | (34.7) | 98 | (100.0) | ** | 1.77 | 1.15–2.73 |
| No (0) | 576 | (51.5) | 542 | (48.5) | 1118 | (100.0) | ||||
| Constipation | Yes (1) | 68 | (70.1) | 29 | (29.9) | 97 | (100.0) | ** | 2.24 | 1.42–3.51 |
| No (0) | 572 | (51.1) | 547 | (48.9) | 1119 | (100.0) | ||||
| Stomach upset/heartburn | Yes (1) | 53 | (58.9) | 37 | (41.1) | 90 | (100.0) | 1.32 | 0.85–2.03 | |
| No (0) | 587 | (52.1) | 539 | (47.9) | 1126 | (100.0) | ||||
| Swollen/bleeding gums | Yes (1) | 49 | (56.3) | 38 | (43.7) | 87 | (100.0) | 1.17 | 0.76–1.82 | |
| No (0) | 591 | (52.3) | 538 | (47.7) | 1129 | (100.0) | ||||
| Forgetful | Yes (1) | 52 | (61.2) | 33 | (38.8) | 85 | (100.0) | 1.45 | 0.93–2.29 | |
| No (0) | 588 | (52.0) | 543 | (48.0) | 1131 | (100.0) |
| Ranking of Symptom | <6 h: No. of Responses (%) * | ≥6 h: No. of Responses (%) * |
|---|---|---|
| 1st | Stiff shoulders 291 (45.5) | Stiff shoulders 211 (36.6) |
| 2nd | Lower back pain 255 (39.8) | Lower back pain 207 (35.9) |
| 3rd | Headache 128 (20.0) | Headache 90 (15.6) |
| 4th | Lethargic 126 (19.7) | Lethargic 89 (15.5) |
| 5th | Joint pain in hands/feet 117 (18.3) | Blocked/runny nose 85 (14.8) |
| 6th | Cough, phlegmatic 87 (13.6) | Cough, phlegmatic 77 (13.4) |
| 7th | Irritable 86 (13.4) | Joint pain in hands/feet 76 (13.2) |
| 8th | Visual impairment 85 (13.3) | Blurred vision 60 (10.4) |
| 9th | Blurred vision 84 (13.1) | Numb limbs/Itchiness (eczema, athlete’s foot, etc.) 59 (10.2) |
| 10th | Blocked/runny nose 83 (13.0) | Visual impairment 58 (10.1) |
| Wilcoxon signed-rank test (Comparison of all 42 symptoms) | p < 0.001 | |
| Analysis Model | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| Objective Variable | Sleep Time (<6 h: 1, ≥6 h: 0) | Subjective Health Assessment (Bad/Not Good: 1, Not Bad/Good/Very Good: 0) | ||||
| Explanatory Variable | Adjusted Odds Ratio | 95% C.I. | Explanatory Variable | Adjusted Odds Ratio | 95% C.I. | |
| Constipation | 1.72 * | 1.07–2.77 | Dizziness | 4.18 ** | 2.55–6.87 | |
| Poor sleep quality | 1.66 * | 1.03–2.66 | Worries and stress | 3.36 ** | 2.19–5.14 | |
| Worries and stress | 1.39 * | 1.04–1.86 | Gender ¶ | 1.74 ** | 1.30–2.32 | |
| Stiff shoulders | 1.28 * | 1.00–1.64 | Outpatient treatment ¶ | 1.74 ** | 1.31–2.16 | |
| Constipation | 1.69 * | 1.03–2.77 | ||||
| Irritable | 1.63 * | 1.07–2.49 | ||||
| Working hours ¶ | 1.62 * | 1.07–2.16 | ||||
| Headache | 1.48 * | 1.03–2.12 | ||||
| Coefficient of determination | R2 (Cox–Snell) | 0.05 | R2 (Cox–Snell) | 0.16 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kato, C.; Komatsuzaki, A.; Ono, S.; Iguchi, A.; Arashi, K.; Motoi, S.; Susuga, M. Subjective Symptoms Linked to Sleep Duration: An Analysis from Japanese National Statistics. Medicines 2023, 10, 60. https://doi.org/10.3390/medicines10110060
Kato C, Komatsuzaki A, Ono S, Iguchi A, Arashi K, Motoi S, Susuga M. Subjective Symptoms Linked to Sleep Duration: An Analysis from Japanese National Statistics. Medicines. 2023; 10(11):60. https://doi.org/10.3390/medicines10110060
Chicago/Turabian StyleKato, Chikage, Akira Komatsuzaki, Sachie Ono, Asami Iguchi, Kiyoka Arashi, Shiho Motoi, and Mio Susuga. 2023. "Subjective Symptoms Linked to Sleep Duration: An Analysis from Japanese National Statistics" Medicines 10, no. 11: 60. https://doi.org/10.3390/medicines10110060
APA StyleKato, C., Komatsuzaki, A., Ono, S., Iguchi, A., Arashi, K., Motoi, S., & Susuga, M. (2023). Subjective Symptoms Linked to Sleep Duration: An Analysis from Japanese National Statistics. Medicines, 10(11), 60. https://doi.org/10.3390/medicines10110060