
Heroin-Related Fatalities in Jeddah, Saudi Arabia, between 2008 and 2018

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Reagents and Standards
2.2. Solid Phase Extraction (SPE)
2.3. LC-MS/MS Systems
2.4. Case Samples
2.4.1. Ethical Approval
2.4.2. Sample Collection
2.4.3. Data Collecting for Post-Mortem Cases
2.4.4. Inclusion/Exclusion Criteria
2.4.5. Other Toxicological Investigations
2.5. Statistical Analysis
2.6. Method Validation
3. Results
3.1. Method Validation
3.2. Case Samples
3.2.1. Demographic Profile
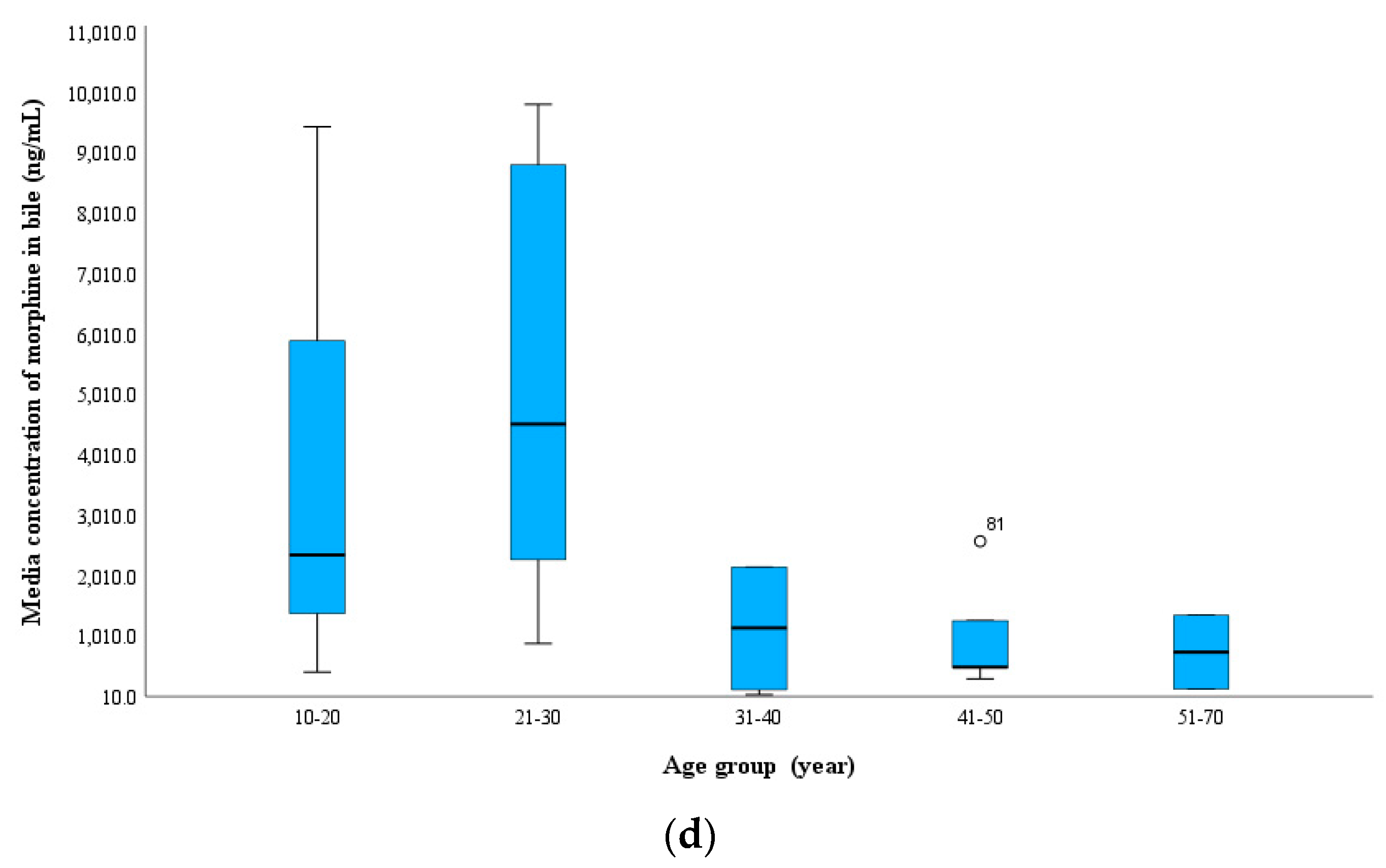
3.2.2. Age Groups and Analyte Concentrations
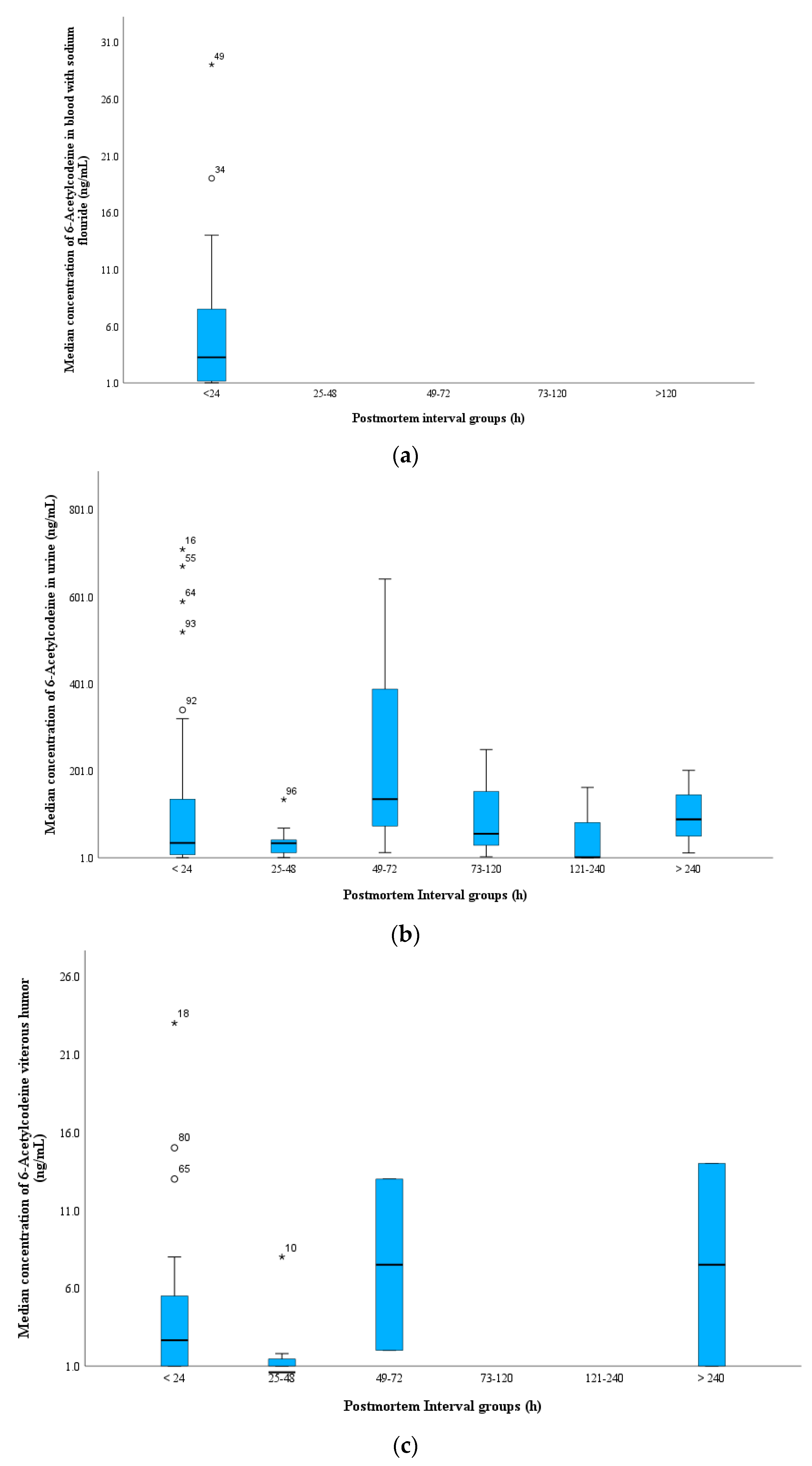
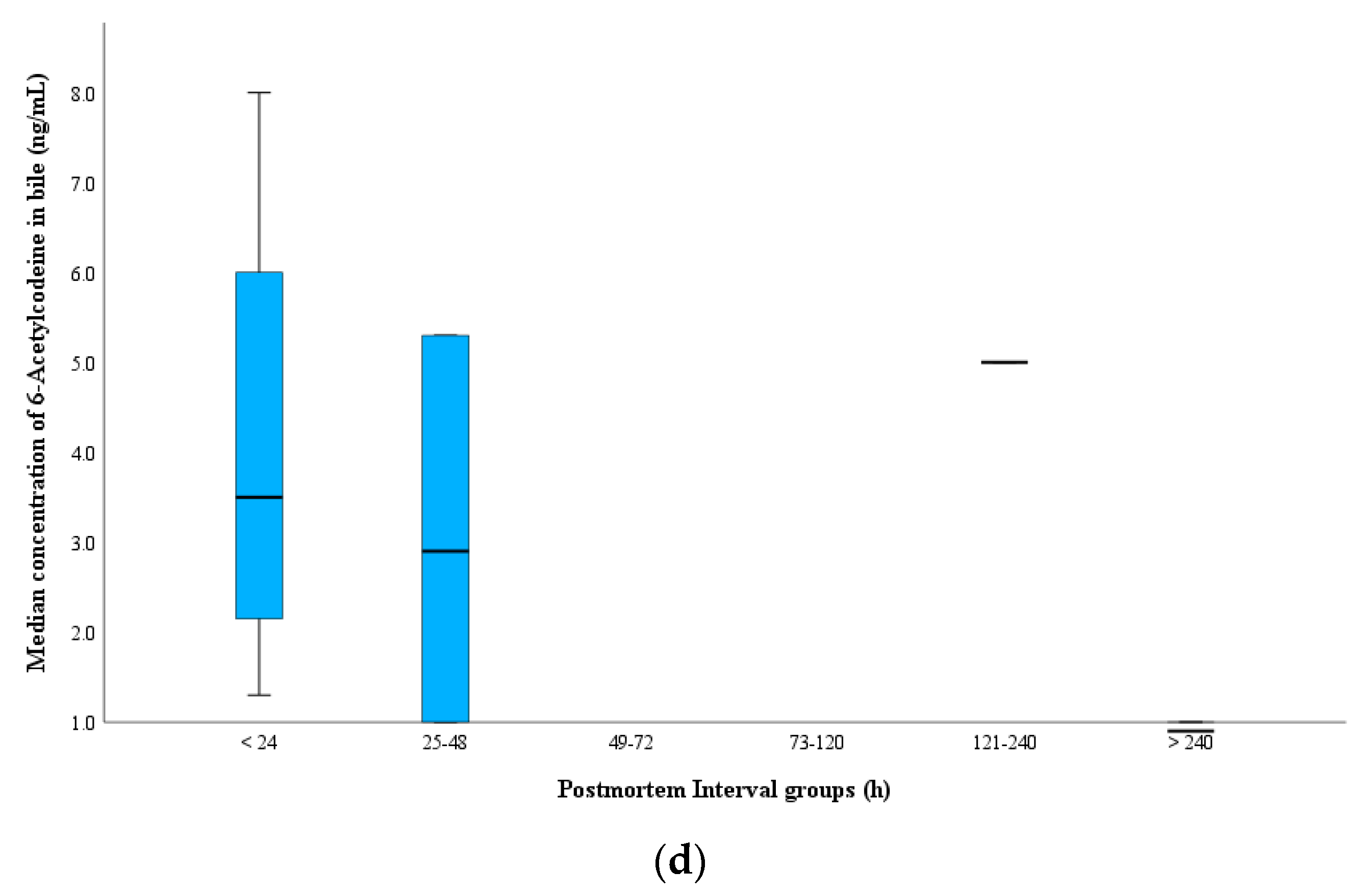
3.2.3. PMI and Analyte Concentrations
3.2.4. Mode of Death
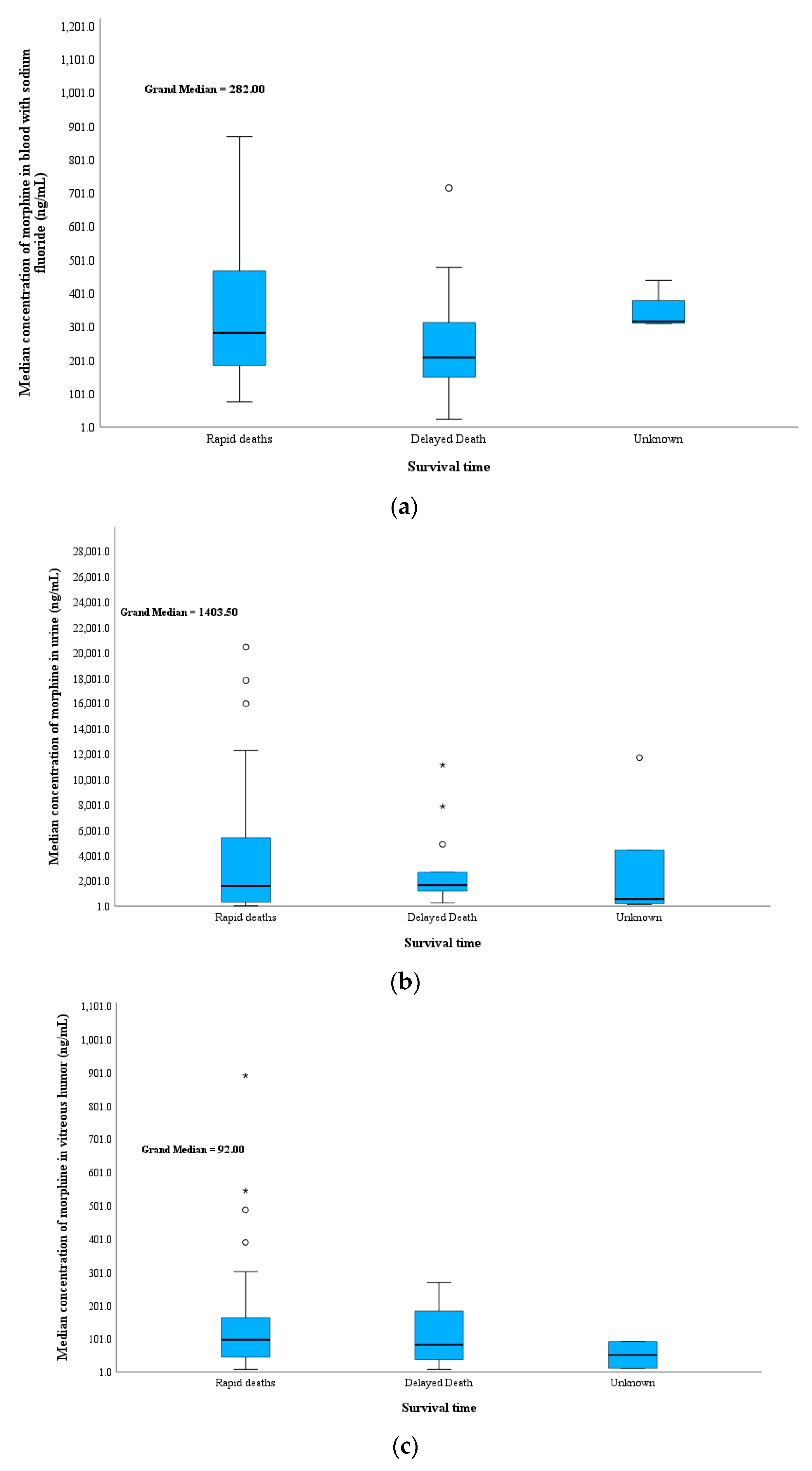
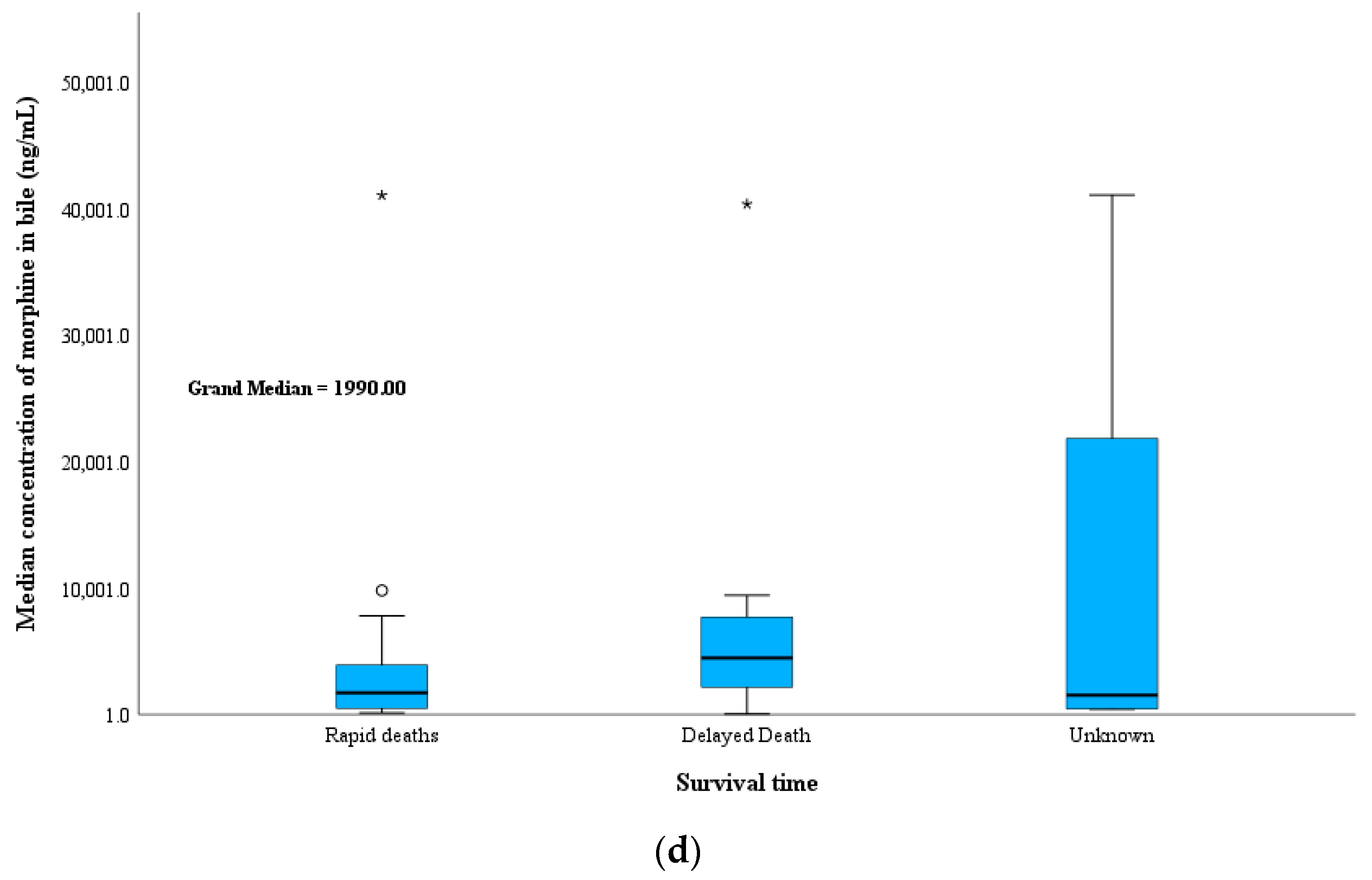
3.2.5. Time Span between Heroin Intake and Death
3.2.6. Manner of Death
3.2.7. Route of Administration
3.2.8. Location of Deaths and Putrefaction
3.2.9. Seasonal Distribution
3.2.10. Multiple Specimens
4. Discussion
4.1. History of Heroin Abuse
4.2. Age Group and Analyte Concentrations
4.3. PMI and Analytes Concentration
4.4. Mode of Death
4.5. Time Span between Heroin Intake and Death
4.6. Manner of Death
4.7. Route of Administration
4.8. Location of Deaths and Putrefaction
4.9. Seasonal Distribution
4.10. Multiple Specimens
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nation Office on Drugs and Crime. World Drug Report 2022; United Nations Publication: Vienna, Austria, 2022; Available online: https://www.unodc.org/unodc/en/data-and-analysis/world-drug-report-2022.html (accessed on 20 January 2023).
- Jones, A.W.; Holmgren, A.; Ahlner, J. Concentrations of Free-Morphine in Peripheral Blood after Recent Use of Heroin in Overdose Deaths and in Apprehended Drivers. Forensic Sci. Int. 2012, 215, 18–24. [Google Scholar] [CrossRef]
- Thaulow, C.H.; Øiestad, Å.M.L.; Rogde, S.; Andersen, J.M.; Høiseth, G.; Handal, M.; Mørland, J.; Vindenes, V. Can Measurements of Heroin Metabolites in Post-Mortem Matrices Other than Peripheral Blood Indicate If Death Was Rapid or Delayed? Forensic Sci. Int. 2018, 290, 121–128. [Google Scholar] [CrossRef]
- Maskell, P.D.; Wilson, N.E.; Seetohul, L.N.; Crichton, M.L.; Beer, L.J.; Drummond, G.; de Paoli, G. Postmortem Tissue Distribution of Morphine and Its Metabolites in a Series of Heroin-Related Deaths. Drug Test. Anal. 2019, 11, 292–304. [Google Scholar] [CrossRef] [PubMed]
- European Monitoring Center for Drugs and Drug Addiction, Drug-Related Deaths and Mortality Rates in Europe. 2019. Available online: https://www.emcdda.europa.eu/topics/drug-related-deaths_en (accessed on 20 January 2023).
- Evans, A.; Krause, M.; Leach, S.; Levitas, M.; Nguyen, L.; Short, L.C. Analysis of Drug Residue in Needle-Exchange Syringes in Washington, D.C. Forensic Sci. Int. 2021, 329, 111083. [Google Scholar] [CrossRef] [PubMed]
- Drug Enforcement Administration. 2020 National Drug Threat Assessment (NDTA). Available online: https://www.dea.gov/sites/default/files/2021-02/DIR-008-21%202020%20National%20Drug%20Threat%20Assessment_WEB.pdf (accessed on 20 February 2023).
- Bassiony, M. Substance Use Disorders in Saudi Arabia: Review Article. J. Subst. Use 2013, 18, 450–466. [Google Scholar] [CrossRef]
- Osman, A.A. Substance Abuse among Patients Attending a Psychiatric Hospital in Jeddah: A Descriptive Study. Ann. Saudi Med. 1992, 12, 289–293. [Google Scholar] [CrossRef]
- Al-Matrouk, A.; Al-Hasan, M.; Naqi, H.; Al-Abkal, N.; Mohammed, H.; Haider, M.; Al-Shammeri, D.; Bojbarah, H. Snapshot of Narcotic Drugs and Psychoactive Substances in Kuwait: Analysis of Illicit Drugs Use in Kuwait from 2015 to 2018. BMC Public Health 2021, 21, 671. [Google Scholar] [CrossRef]
- Al-Asmari, A.I.; Al-Amoudi, D.H. The Role of Ethanol in Fatalities in Jeddah, Saudi Arabia. Forensic Sci. Int. 2020, 316, 110464. [Google Scholar] [CrossRef]
- Al-Asmari, A.I. Applications of LC-MS/MS in Forensic Toxicology for the Analysis of Drugs and Their Metabolites. Ph.D. Dissertation, University of Glasgow, Glasgow, UK, 2009. [Google Scholar]
- Abiragi, M.; Bauler, L.D.; Brown, T. Importance and Approach to Manner of Death Opinions in Opioid-Related Deaths. J. Forensic Sci. 2020, 65, 1009–1011. [Google Scholar] [CrossRef]
- Elfawal, M.A. Trends in Fatal Substance Overdose in Eastern Saudi Arabia. J. Clin. Forensic Med. 1999, 6, 30–34. [Google Scholar] [CrossRef]
- Maas, A.; Madea, B.; Hess, C. Confirmation of Recent Heroin Abuse: Accepting the Challenge. Drug Test. Anal. 2018, 10, 54–71. [Google Scholar] [CrossRef]
- Pragst, F.; Spiegel, K.; Leuschner, U.; Hager, A. Detection of 6-Acetylmorphine in Vitreous Humor and Cerebrospinal Fluid-Comparison with Urinary Analysis for Proving Heroin Administration in Opiate Fatalities. J. Anal. Toxicol. 1999, 23, 168–172. [Google Scholar] [CrossRef] [PubMed]
- Brenneisen, R.; Hasler, F.; Würsch, D. Acetylcodeine as a Urinary Marker to Differentiate the Use of Street Heroin and Pharmaceutical Heroin. J. Anal. Toxicol. 2002, 26, 561–566. [Google Scholar] [CrossRef]
- Staub, C.; Jeanmonod, R.; Frye, O. Morphine in Postmortem Blood: Its Importance for the Diagnosis of Deaths Associated with Opiate Addiction. Int. J. Leg. Med. 1990, 104, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Al-Asmari, A.I.; Anderson, R.A. Method for Quantification of Opioids and Their Metabolites in Autopsy Blood by Liquid Chromatography-Tandem Mass Spectrometry. J. Anal. Toxicol. 2007, 31, 394–408. [Google Scholar] [CrossRef]
- Al-Asmari, A.I. Postmortem Fluid Concentrations of Heroin Biomarkers and Their Metabolites. J. Forensic Sci. 2020, 65, 570–579. [Google Scholar] [CrossRef]
- Al-Asmari, A.I.; Alharbi, H.; Zughaibi, T.A. Post-Mortem Analysis of Heroin Biomarkers, Morphine and Codeine in Stomach Wall Tissue in Heroin-Related Deaths. Toxics 2022, 10, 473. [Google Scholar] [CrossRef]
- ANSI/ASB Standard 036; American Academy of Forensic Sciences Standards Board 2019. Method Validation in Forensic Toxicology: Colorado Springs, CO, USA, 2019.
- Bidny, S.; Gago, K.; Chung, P.; Albertyn, D.; Pasin, D. Simultaneous Screening and Quantification of Basic, Neutral and Acidic Drugs in Blood Using UPLC-QTOF-MS. J. Anal. Toxicol. 2017, 41, 181–195. [Google Scholar] [CrossRef] [PubMed]
- Di Rago, M.; Saar, E.; Rodda, L.N.; Turfus, S.; Kotsos, A.; Gerostamoulos, D.; Drummer, O.H. Fast Targeted Analysis of 132 Acidic and Neutral Drugs and Poisons in Whole Blood Using LC-MS/MS. Forensic Sci. Int. 2014, 243, 35–43. [Google Scholar] [CrossRef]
- Al-Asmari, A.I. Method for the Identification and Quantification of Sixty Drugs and Their Metabolites in Postmortem Whole Blood Using Liquid Chromatography Tandem Mass Spectrometry. Forensic Sci. Int. 2020, 309, 110193. [Google Scholar] [CrossRef]
- Maurer, H.H. Chapter 12 Forensic Screening with GC-MS. Handb. Anal. Sep. 2008, 6, 425–445. [Google Scholar] [CrossRef]
- Wylie, F.M.; Torrance, H.; Seymour, A.; Buttress, S.; Oliver, J.S. Drugs in Oral Fluid: Part II. Investigation of Drugs in Drivers. Forensic Sci. Int. 2005, 150, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Matuszewski, B.K.; Constanzer, M.L.; Chavez-Eng, C.M. Strategies for the Assessment of Matrix Effect in Quantitative Bioanalytical Methods Based on HPLC-MS/MS. Anal. Chem. 2003, 75, 3019–3030. [Google Scholar] [CrossRef] [PubMed]
- Peters, F.T.; Drummer, O.H.; Musshoff, F. Validation of New Methods. Forensic Sci. Int. 2007, 165, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Kintz, P.; Jamey, C.; Cirimele, V.; Brenneisen, R.; Ludes, B. Evaluation of Acetylcodeine as a Specific Marker of Illicit Heroin in Human Hair. J. Anal. Toxicol. 1998, 22, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Staub, C.; Marset, M.; Mino, A.; Mangin, P. Detection of Acetylcodeine in Urine as an Indicator of Illicit Heroin Use: Method Validation and Results of a Pilot Study. Clin. Chem. 2001, 47, 301–307. [Google Scholar] [CrossRef]
- O′Neal, C.L.; Poklis, A. Postmortem Production of Ethanol and Factors That Influence Interpretation: A Critical Review. Am. J. Forensic Med. Pathol. 1996, 17, 8–20. [Google Scholar] [CrossRef]
- Al-Asmari, A.I.; Altowairgi, M.M.; Al-Amoudi, D.H. Effects of Postmortem Interval, Putrefaction, Diabetes, and Location of Death on the Analysis of Ethyl Glucuronide and Ethyl Sulfate as Ethanol Biomarkers of Antemortem Alcohol Consumption. Forensic Sci. Int. 2022, 335, 111280. [Google Scholar] [CrossRef]
- Steentoft, A.; Worm, K.; Christensen, H. Morphine Concentrations in Autopsy Material from Fatal Cases after Intake of Morphine and/or Heroin. J. Forensic Sci. Soc. 1988, 28, 87–94. [Google Scholar] [CrossRef]
- Lee, D.; Delcher, C.; Maldonado-Molina, M.M.; Thogmartin, J.R.; Goldberger, B.A. Manners of Death in Drug-Related Fatalities in Florida. J. Forensic Sci. 2016, 61, 735–742. [Google Scholar] [CrossRef]
- Hadidi, M.S.; Ibrahim, M.I.; Abdallat, I.M.; Hadidi, K.A. Current Trends in Drug Abuse Associated Fatalities-Jordan, 2000–2004. Forensic Sci. Int. 2009, 186, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Taghaddosinejad, F.; Arefi, M.; Fayaz, A.F.; Tanhaeivash, R. Determination of Substance Overdose in Two Iranian Centers: Comparison between Opioids and Non-Opioids. J. Forensic Leg. Med. 2013, 20, 155–157. [Google Scholar] [CrossRef] [PubMed]
- Gerostamoulos, J.; Staikos, V.; Drummer, O.H. Heroin-Related Deaths in Victoria: A Review of Cases for 1997 and 1998. Drug Alcohol Depend. 2001, 61, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Fugelstad, A.; Ahlner, J.; Brandt, L.; Ceder, G.; Eksborg, S.; Rajs, J.; Beck, O. Use of Morphine and 6-Monoacetylmorphine in Blood for the Evaluation of Possible Risk Factors for Sudden Death in 192 Heroin Users. Addiction 2003, 98, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Burt, M.J.; Kloss, J.; Apple, F.S. Postmortem Blood Free and Total Morphine Concentrations in Medical Examiner Cases. J. Forensic Sci. 2001, 46, 1138–1142. [Google Scholar] [CrossRef] [PubMed]
- Darke, S.; Duflou, J.; Torok, M. Comparative Toxicology of Intentional and Accidental Heroin Overdose. J. Forensic Sci. 2010, 55, 1015–1018. [Google Scholar] [CrossRef]
- Jakobsson, G.; Truver, M.T.; Wrobel, S.A.; Gréen, H.; Kronstrand, R. Heroin-Related Compounds and Metabolic Ratios in Postmortem Samples Using LC-MS-MS. J. Anal. Toxicol. 2021, 45, 215–225. [Google Scholar] [CrossRef]
- Frost, J.; Løkken, T.N.; Helland, A.; Nordrum, I.S.; Slørdal, L. Post-Mortem Levels and Tissue Distribution of Codeine, Codeine-6-Glucuronide, Norcodeine, Morphine and Morphine Glucuronides in a Series of Codeine-Related Deaths. Forensic Sci. Int. 2016, 262, 128–137. [Google Scholar] [CrossRef]
- Skopp, G. Postmortem Toxicology. Forensic Sci. Med. Pathol. 2010, 6, 314–325. [Google Scholar] [CrossRef]
- Gerostamoulos, J.; Drummer, O.H. Postmortem Redistribution of Morphine and Its Metabolites. J. Forensic Sci. 2000, 45, 843–845. [Google Scholar] [CrossRef]
- Logan, B.K.; Smirnow, D. Postmortem Distribution and Redistribution of Morphine in Man. J. Forensic Sci. 1996, 41, 37–46. [Google Scholar] [CrossRef]
- Sawyer, W.R.; Forney, R.B. Postmortem Disposition of Morphine in Rats. Forensic Sci. Int. 1988, 38, 259–273. [Google Scholar] [CrossRef] [PubMed]
- Degouffe, M.; Drost, M. A Comparison of Drug Concentrations in Postmortem Cardiac and Peripheral Blood in 320 Cases. J. Can. Soc. Forensic Sci. 1995, 28, 113–121. [Google Scholar] [CrossRef]
- Maskell, P.D.; Albeishy, M.; de Paoli, G.; Wilson, N.E.; Seetohul, L.N. Postmortem Redistribution of the Heroin Metabolites Morphine and Morphine-3-Glucuronide in Rabbits over 24 h. Int. J. Leg. Med. 2016, 130, 519–531. [Google Scholar] [CrossRef] [PubMed]
- Romberg, R.W.; Lee, L. Comparison of the Hydrolysis Rates of Morphine-3-Glucuronide and Morphine-6-Glucuronide with Acid and β-Glucuronidase. J. Anal. Toxicol. 1995, 19, 157–162. [Google Scholar] [CrossRef]
- Rees, K.A.; Pounder, D.J.; Osselton, M.D. Distribution of Opiates in Femoral Blood and Vitreous Humour in Heroin/Morphine-Related Deaths. Forensic Sci. Int. 2013, 226, 152–159. [Google Scholar] [CrossRef]
- Scott, K.S.; John, G.; Oliver, S.; Frsc, C. Vitreous Humor as an Alternative Sample to Blood for the Supercritical Fluid Extraction of Morphine and 6-Monoacetylmorphine. Med. Sci. Law 1999, 39, 77–81. [Google Scholar] [CrossRef]
- Moffat, A.C.; Osselton, M.D.; Widdop, B. Diamorphine. In Clarke’s Analysis of Drugs and Poisons in Pharmaceuticals, Body Fluids and Postmortem Material, 4th ed.; Pharmaceutical Press: London, UK, 2011; pp. 1225–1227. [Google Scholar]
- Baselt, R.C.; Cravey, R.H. Heroin. In Disposition of Toxic Drugs and Chemicals in Man, 11th ed.; Baselt, R.C., Ed.; Biomedical Publications: Foster City, CA, USA, 2020; pp. 1031–1036. [Google Scholar]
- Nassibou, S.; Richeval, C.; Wiart, J.F.; Hakim, F.; Allorge, D.; Gaulier, J.M. In Heroin-Related Fatalities, Testing for 6-Acetylmorphine in Vitreous Humor Seems to Be of Higher Sensitivity than in Blood or Urine. J. Anal. Toxicol. 2020, 44, E9–E10. [Google Scholar] [CrossRef]
- Jones, A.W.; Holmgren, A.; Ahlner, J. Heroin Poisoning Deaths with 6-Acetylmorphine in Blood: Demographics of the Victims, Previous Drug-Related Offences, Polydrug Use, and Free Morphine Concentrations in Femoral Blood. Forensic Toxicol. 2012, 30, 19–24. [Google Scholar] [CrossRef]
- Meissner, C.; Recker, S.; Reiter, A.; Friedrich, H.J.; Oehmichen, M. Fatal versus Non-Fatal Heroin “Overdose”: Blood Morphine Concentrations with Fatal Outcome in Comparison to Those of Intoxicated Drivers. Forensic Sci. Int. 2002, 130, 49–54. [Google Scholar] [CrossRef]
- Polettini, A.; Poloni, V.; Groppi, A.; Stramesi, C.; Vignali, C.; Politi, L.; Montagna, M. The Role of Cocaine in Heroin-Related Deaths: Hypothesis on the Interaction between Heroin and Cocaine. Forensic Sci. Int. 2005, 153, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Darke, S.; Duflou, J. The Toxicology of Heroin-Related Death: Estimating Survival Times. Addiction 2016, 111, 1607–1613. [Google Scholar] [CrossRef] [PubMed]
- The Saudi Food and Drug Authority Regulations and Regulations for General Provisions on Schedules Attached to the Anti-Drug and Psychotropic Substances System. Um Alqura Newspaper, 2019.
- Logan, B.K.; Fligner, C.L.; Haddix, T. Cause and Manner of Death in Fatalities Involving Methamphetamine. J. Forensic Sci. 1998, 43, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Darke, S.; Duflou, J.; Lappin, J.; Kaye, S. Clinical and Autopsy Characteristics of Fatal Methamphetamine Toxicity in Australia. J. Forensic Sci. 2018, 63, 1466–1471. [Google Scholar] [CrossRef] [PubMed]
- Al-Asmari, A.I.; Al-Solami, F.D.; Al-Zahrani, A.E.; Zughaibi, T.A. Post-Mortem Quantitation of Amphetamine in Cadaveric Fluids in Saudi Arabia. Forensic Sci. 2022, 2, 222–237. [Google Scholar] [CrossRef]
- Al-Asmari, A.I. Methamphetamine-Related Postmortem Cases in Jeddah, Saudi Arabia. Forensic Sci. Int. 2021, 321, 110746. [Google Scholar] [CrossRef]
- Rintoul, A.C.; Dobbin, M.D.H.; Nielsen, S.; Degenhardt, L.; Drummer, O.H. Recent Increase in Detection of Alprazolam in Victorian Heroin-Related Deaths. Med. J. Aust. 2013, 198, 206–209. [Google Scholar] [CrossRef]
- Wolf, B.C.; Lavezzi, W.A.; Sullivan, L.M.; Middleberg, R.A.; Flannagan, L.M. Alprazolam-Related Deaths in Palm Beach County. Am. J. Forensic Med. Pathol. 2005, 26, 24–27. [Google Scholar] [CrossRef]
- Thaulow, C.H.; Øiestad, Å.M.L.; Rogde, S.; Karinen, R.; Brochmann, G.W.; Andersen, J.M.; Høiseth, G.; Handal, M.; Mørland, J.; Arnestad, M.; et al. Metabolites of Heroin in Several Different Post-Mortem Matrices. J. Anal. Toxicol. 2018, 42, 311–320. [Google Scholar] [CrossRef]
- Spiehler, V.; Brown, R. Unconjugated Morphine in Blood by Radioimmunoassay and Gas Chromatography/Mass Spectrometry. J. Forensic Sci. 1987, 32, 906–916. [Google Scholar] [CrossRef]
- Garriott, J.C.; Sturner, W.Q. Morphine Concentrations and Survival Periods in Acute Heroin Fatalities. N. Engl. J. Med. 1973, 289, 1276–1278. [Google Scholar] [CrossRef] [PubMed]
- Goldberger, B.A.; Cone, E.J.; Grant, T.M.; Levine, B.S.; Smialek, J.E. Disposition of Heroin and Its Metabolites in Heroin-Related Deaths. J. Anal. Toxicol. 1994, 18, 22–28. [Google Scholar] [CrossRef]
- Singer, R. The Forensic Pharmacology of Drugs of Abuse. Int. J. Toxicol. 2002, 21, 436–437. [Google Scholar] [CrossRef]
- Darke, S.; Ross, J. Suicide among Heroin Users: Rates, Risk Factors and Methods. Addiction 2002, 97, 1383–1394. [Google Scholar] [CrossRef] [PubMed]
- Concool, B.; Smith, H.; Stimmel, B. Mortality Rates of Persons Entering Methadone Maintenance: A Seven-Year Study. Am. J. Drug Alcohol Abus. 1979, 6, 345–353. [Google Scholar] [CrossRef]
- Darke, S. The Toxicology of Homicide Offenders and Victims: A Review. Drug Alcohol Rev. 2010, 29, 202–215. [Google Scholar] [CrossRef]
- Paul, A.B.M.; Simms, L.; Mahesan, A.M. Intentional Heroin Administration Resulting in Homicide in a 10-Month Old Infant. Forensic Sci. Int. 2018, 290, e15–e18. [Google Scholar] [CrossRef]
- Missliwetz, J.; Vycudilik, W. Homicide by Strangling or Dumping with Postmortem Injuries after Heroin Poisoning? Am. J. Forensic Med. Pathol. 1997, 18, 211–214. [Google Scholar] [CrossRef]
- Reed, D.; Spiehler, V.R.; Cravey, R.H. Two Cases of Heroin-Related Suicide. Forensic Sci. 1977, 9, 49–52. [Google Scholar] [CrossRef]
- Denning, D.G.; Conwell, Y.; King, D.; Cox, C. Method Choice, Intent, and Gender in Completed Suicide. Suicide Life Threat. Behav. 2000, 30, 282–288. [Google Scholar]
- Marx, A.; Schick, M.T.; Minder, C.E. Drug-Related Mortality in Switzerland from 1987 to 1989 in Comparison to Other Countries. Int. J. Addict. 1994, 29, 837–860. [Google Scholar] [CrossRef] [PubMed]
- Rossow, I. Suicide among Drug Addicts in Norway. Addiction 1994, 89, 1667–1673. [Google Scholar] [CrossRef] [PubMed]
- Dukes, P.D.; Robinson, G.M.; Robinson, B.J. Mortality of Intravenous Drug Users: Attenders of the Wellington Drug Clinic, 1972–1989. Drug Alcohol Rev. 1992, 11, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Stam, N.C.; Gerastamoulos, D.; Pilgrim, J.L.; Smith, K.; Moran, L. Letter to the Editor Drug-Related Deaths-A Wider View Is Necessary. Addiction 2019, 114, 1504. [Google Scholar] [CrossRef]
- Roxburgh, A.; Pilgrim, J.L.; Hall, W.D.; Burns, L.; Degenhardt, L. Accurate Identification of Opioid Overdose Deaths Using Coronial Data. Forensic Sci. Int. 2018, 287, 40–46. [Google Scholar] [CrossRef]
- Thiblin, I.; Eksborg, S.; Petersson, A.; Fugelstad, A.; Rajs, J. Fatal Intoxication as a Consequence of Intranasal Administration (Snorting) or Pulmonary Inhalation (Smoking) of Heroin. Forensic Sci. Int. 2004, 139, 241–247. [Google Scholar] [CrossRef]
- Crandall, C.S.; Kerrigan, S.; Aguero, R.L.; LaValley, J.; McKinney, P.E. The Influence of Collection Site and Methods on Postmortem Morphine Concentrations in a Porcine Model. J. Anal. Toxicol. 2006, 30, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Soravisut, N.; Rattanasalee, P.; Junkuy, A.; Thampitak, S.; Sribanditmongkol, P. Comparative Analysis of Pathological and Toxicological Features of Opiate Overdose and Non-Overdose Fatalities. J. Med. Assoc. Thail. Chotmaihet Thangphaet 2011, 94, 1540–1546. [Google Scholar]
- Darke, S.; Ross, J. Fatal Heroin Overdoses Resulting from Non-Injecting Routes of Administration, NSW, Australia, 1992–1996. Addiction 2000, 95, 569–573. [Google Scholar] [CrossRef]
- Warner-Smith, M.; Darke, S.; Lynskey, M.; Hall, W. Heroin Overdose: Causes and Consequences. Addiction 2001, 96, 1113–1125. [Google Scholar] [CrossRef]
- Crump, K.L.; Mclntyre, M.; Drummer, O.H. Simultaneous Determination of Morphine and Codeine in Blood and Bile Using Dual Ultraviolet and Fluorescence High-Performance Liquid Chromatography. J. Anal. Toxicol. 1994, 18, 208–212. [Google Scholar] [CrossRef]
- Reisinger, A.J.; Miller, A.C.; Shaw, L.A.; Champion, J.L.; Neiswonger, M.A. Oral Cavity Fluid as an Investigative Approach for Qualitative and Quantitative Evaluations of Drugs in Postmortem Subjects. J. Anal. Toxicol. 2019, 43, 444–451. [Google Scholar] [CrossRef]
- Kringsholm, B.; Voigt, J.; Dalgaard, J.B.; Simonsen, J. Deaths among Narcotic Addicts in Denmark in 1978 and 1979. Forensic Sci. Int. 1981, 18, 19–30. [Google Scholar] [CrossRef]
- Jones, A.W.; Holmgren, A. Concentration Ratios of Free-Morphine to Free-Codeine in Femoral Blood in Heroin-Related Poisoning Deaths. Leg. Med. 2011, 13, 171–173. [Google Scholar] [CrossRef]
- Berg-Pedersen, R.M.; Ripel, Å.; Karinen, R.; Vevelstad, M.; Bachs, L.; Vindenes, V. Codeine to Morphine Concentration Ratios in Samples from Living Subjects and Autopsy Cases after Incubation. J. Anal. Toxicol. 2014, 38, 99–105. [Google Scholar] [CrossRef]
- Skopp, G.; Pötsch, L.; Klingmann, A.; Mattern, R. Stability of Morphine, Morphine-3-Glucuronide, and Morphine-6-Glucuronide in Fresh Blood and Plasma and Postmortem Blood Samples. J. Anal. Toxicol. 2001, 25, 2–7. [Google Scholar] [CrossRef]
- Moriya, F.; Hashimoto, Y. Distribution of Free and Conjugated Morphine in Body Fluids and Tissues in a Fatal Heroin Overdose: Is Conjugated Morphine Stable in Postmortem Specimens? J. Forensic Sci. 1997, 42, 736–740. [Google Scholar] [CrossRef]
- Duflou, J.; Darke, S.; Easson, J. Morphine Concentrations in Stomach Contents of Intravenous Opioid Overdose Deaths. J. Forensic Sci. 2009, 54, 1181–1184. [Google Scholar] [CrossRef]
- Al-Asmari, A.I. Postmortem Liver and Kidney Tissue Concentrations of Heroin Biomarkers and Their Metabolites in Heroin-Related Fatalities. J. Forensic Sci. 2020, 65, 2087–2093. [Google Scholar] [CrossRef]
- Mercurio, I.; Ceraso, G.; Melai, P.; Gili, A.; Troiano, G.; Agostinelli, F.; Lancia, M.; Bacci, M. Significance of Morphine Concentration in Bile, Liver, and Blood: Analysis of 52 Cases of Heroin Overdoses. Am. J. Forensic Med. Pathol. 2019, 40, 329–335. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Analytes & | Internal Standards | RT * (min) | Quantifier Ion | Qualifier Ion | RT (min) | Quantifier Ion | Qualifier Ion |
|---|---|---|---|---|---|---|---|
| LC-MS 8050 | LCQ Fleet | ||||||
| Analytes | |||||||
| 6-MAM | 6-MAM-d3 | 6.9 | m/z = 328−165 | m/z = 328−221 | 15.1 | m/z1 = 328−211 | m/z = 328−268 |
| 6-MAM-d3 # | - | 7.0 | m/z = 331–165 | m/z = 331–221 | 15.1 | m/z = 331–165 | m/z = 331–221 |
| 6-AC | Codeine-d3 | 9.3 | m/z = 342–225 | m/z = 342–165 | 19.0 | m/z = 342–225 | m/z = 342–282 |
| Morphine | Morphine-d3 | 4.7 | m/z = 286–165 | m/z = 286–153 | 8.4 | m/z = 286–201 | m/z = 286–229 |
| Morphine-d3 # | - | 4.6 | m/z = 289–165 | m/z = 289–153 | 8.2 | m/z = 289–201 | m/z = 289–229 |
| Codeine | Codeine-d3 | 6.8 | m/z = 300–165 | m/z = 300–44 | 13.9 | m/z = 300–215 | m/z = 300–243 |
| Codeine-d3 # | - | 6.7 | m/z = 303–165 | m/z = 300–199 | 13.9 | m/z = 303–215 | m/z = 300–243 |
| Cause of Deaths | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Heroin Only | Poly Drug Intoxication | ||||||||
| Total case number | 66 | 31 | |||||||
| N | Med | Min | Max | N | Med | Min | Max | ||
| Specimens | Analytes & | ng/mL | ng/mL | ||||||
| Blood with Sodium Fluoride | 6-MAM | 36 | 10 | 1 | 420 | 14 | 10 | Tr | 100 |
| 6-AC | 11 | 5 | Tr | 30 | 9 | 2 | Tr | 10 | |
| Morphine | 57 | 310 | 100 | 4400 | 27 | 250 | 23 | 670 | |
| Codeine | 57 | 20 | 4 | 140 | 27 | 20 | 3 | 110 | |
| Urine | 6-MAM | 46 | 330 | 1 | 18,900 | 28 | 320 | 1 | 4600 |
| 6-AC | 30 | 40 | 1 | 670 | 20 | 40 | 1 | 710 | |
| Morphine | 46 | 1340 | 90 | 50,400 | 2 | 1850 | 10 | 20,400 | |
| Codeine | 43 | 210 | 5 | 12,110 | 27 | 170 | 3 | 1210 | |
| Vitreous Humor | 6-MAM | 45 | 30 | 1 | 240 | 25 | 20 | 1 | 210 |
| 6-AC | 18 | 2 | Tr | 10 | 17 | 2 | Tr | 20 | |
| Morphine | 45 | 90 | 10 | 890 | 26 | 90 | 10 | 490 | |
| Codeine | 44 | 10 | 3 | 140 | 25 | 10 | 1 | 70 | |
| Bile | 6-MAM | 9 | 10 | 1 | 160 | 8 | 10 | 2 | 40 |
| 6-AC | 3 | 5 | 1 | 10 | 5 | 3 | 1 | 5 | |
| Morphine | 18 | 2400 | 40 | 41,100 | 10 | 1700 | 300 | 4 | |
| Codeine | 15 | 20 | 5 | 230 | 10 | 40 | 10 | 120 | |
| Survival Time | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Rapid Deaths | Delayed Death | Unknown | |||||||||||
| Total case number | 69 | 19 | 9 | ||||||||||
| Specimens | Analytes & | N # | Median | Minimum | Maximum | N | Median | Minimum | Maximum | N | Median | Minimum | Maximum |
| Blood with Sodium Fluoride | 6-MAM | 48 | 10 | Tr | 420 | 0 | 0 | ||||||
| 6-AC | 19 | 3 | Tr * | 30 | 0 | 0 | |||||||
| MOR | 66 | 310 | 80.0 | 4400 | 14 | 210 | 23.0 | 715 | 4 | 317 | 310.0 | 439 | |
| COD | 66 | 20 | 3.0 | 140 | 14 | 10 | 3.0 | 40 | 4 | 30 | 4.0 | 60 | |
| Urine | 6-MAM | 54 | 380 | 1.0 | 18,876 | 14 | 380 | 10.0 | 820 | 6 | 50 | 1.0 | 130 |
| 6-AC | 37 | 40 | 1.0 | 710 | 12 | 10 | 1.0 | 320 | 0 | ||||
| MOR | 54 | 2100 | 14.0 | 50,401 | 14 | 1300 | 244.0 | 11,100 | 6 | 550 | 120.0 | 11,700 | |
| COD | 51 | 210 | 3.0 | 12,110 | 13 | 90 | 3.0 | 630 | 6 | 20 | 5.0 | 660 | |
| Vitreous Humor | 6-MAM | 50 | 40 | 1.3 | 240 | 18 | 10 | 3.0 | 40 | 2 | n.a. | 1.0 | 13 |
| 6-AC | 25 | 3 | Tr | 20 | 9 | 1 | Tr | 14 | 1 | n.a. | 1.0 | 1 | |
| MOR | 51 | 90 | 10.0 | 900 | 18 | 60 | 10.0 | 270 | 2 | n.a | 11.0 | 90 | |
| COD | 50 | 10 | 1.0 | 140 | 17 | 10 | 3.0 | 70 | 2 | n.a. | 2.0 | 10 | |
| Bile | 6-MAM | 10 | 10 | 2.0 | 160 | 4 | 10 | 10.0 | 40 | 3 | 10 | 2.0 | 40 |
| 6-AC | 4 | 2 | Tr | 5 | 3 | 5 | 4.0 | 10 | 1 | n.a | 1.0 | 1 | |
| MOR | 17 | 2200 | 30.0 | 41,100 | 6 | 2800 | 40.0 | 9,400 | 4 | 1520 | 410.0 | 41,100 | |
| COD | 16 | 30 | 5.0 | 190 | 5 | 40 | Tr | 230 | 4 | 40 | 10.0 | 170 | |
| Manner of Deaths | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Accidental | Suicidal | Homicidal | Undetermined | ||||||||||||||
| Total Case Number | 74 | 7 | 5 | 11 | |||||||||||||
| Specimens | Analytes & | N# | Median | Minimum | Maximum | N | Median | Minimum | Maximum | N | Median | Minimum | Maximum | N | Median | Minimum | Maximum |
| ng/mL | ng/mL | ng/mL | ng/mL | ||||||||||||||
| Blood with Sodium Fluoride | 6-MAM | 39 | 10 | Tr * | 150 | 6 | 210 | 5.0 | 420 | 2 | 6 | 2.0 | 10 | 3 | 3 | 1.0 | 20 |
| 6-AC | 15 | 2 | Tr | 10 | 5 | 10 | 4.0 | 30 | 0 | 0 | |||||||
| MOR | 67 | 280 | 20.0 | 830 | 7 | 480 | 220.0 | 4400 | 3 | 180 | 150.0 | 870 | 7 | 210 | 120.0 | 720 | |
| COD | 67 | 20 | 3.0 | 110 | 7 | 30 | 5.0 | 140 | 3 | 10 | 4.0 | 50 | 7 | 10 | 4.0 | 40 | |
| Urine | 6-MAM | 57 | 310 | 1.0 | 4600 | 6 | 810 | 30.0 | 18,900 | 5 | 480 | 54.0 | 2520 | 6 | 540 | 40.0 | 1580 |
| 6-AC | 36 | 36 | 1.0 | 710 | 5 | 40 | 13.0 | 670 | 4 | 40 | 1.0 | 250 | 5 | 10 | 1.0 | 160 | |
| MOR | 57 | 1330 | 10.0 | 20,400 | 6 | 3630 | 100.0 | 50,400 | 5 | 2100 | 1240.0 | 5350 | 6 | 990 | 190.0 | 4110 | |
| COD | 54 | 140 | 3.0 | 1300 | 6 | 240 | 5.0 | 12,110 | 4 | 540 | 170.0 | 1210 | 6 | 150 | 10.0 | 2100 | |
| Vitreous Humor | 6-MAM | 57 | 20 | 1.0 | 200 | 5 | 210 | 60.0 | 240 | 3 | 20 | 3.0 | 30 | 5 | 20 | 1.0 | 50 |
| 6-AC | 28 | 2 | Tr | 20 | 5 | 3 | 1.0 | 10 | 1 | 10 | 10.0 | 10 | 1 | 1 | 1.0 | 1 | |
| MOR | 57 | 80 | 10.0 | 890 | 5 | 150 | 40.0 | 550 | 3 | 50 | 40.0 | 150 | 6 | 120 | 40.0 | 300 | |
| COD | 55 | 10 | 1.0 | 140 | 5 | 20 | 10.0 | 30 | 3 | 10 | 10.0 | 10 | 6 | 10 | 3.0 | 20 | |
| Bile | 6-MAM | 9 | 10 | 2.0 | 40 | 1 | 10 | 10.0 | 10 | 2 | 30 | 10.0 | 40 | 5 | 2 | 1.0 | 160 |
| 6-AC | 5 | 3 | 1.0 | 5 | 0 | 2 | 4 | Tr | 10 | 1 | 5 | 5.0 | 5 | ||||
| MOR | 16 | 2100 | 40.0 | 41,100 | 2 | 310 | 130.0 | 490 | 3 | 1350 | 1260.0 | 9440 | 7 | 2807 | 120.0 | 41,100 | |
| COD | 13 | 40 | 10.0 | 170 | 2 | 20 | 10.0 | 20 | 3 | 70 | 5.0 | 230 | 7 | 10 | 10 | 190 | |
| Route of Administration | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Injection | Sniffing | Unknown | |||||||||||
| Total Case Number | 72 | 9 | 16 | ||||||||||
| Specimens | Analytes & | N # | Median | Minimum | Maximum | N | Median | Minimum | Maximum | N | Median | Minimum | Maximum |
| Blood with Sodium Fluoride | 6-MAM | 41 | 10 | 1.0 | 420 | 5 | 4 | Tr | 10 | 4 | 5 | 1.3 | 20 |
| 6-Ac | 17 | 4 | Tr * | 30 | 3 | 3 | Tr | 10 | 0 | ||||
| Morphine | 63 | 310 | 20.0 | 4400 | 8 | 150 | 75.0 | 360 | 13 | 220 | 120.0 | 720 | |
| Codeine | 63 | 20 | 3.0 | 140 | 8 | 10 | 3.0 | 40 | 13 | 20 | 10.0 | 70 | |
| Urine | 6-MAM | 53 | 470 | 1.0 | 18,900 | 9 | 280 | 20.0 | 480 | 12 | 75 | 1.0 | 2520 |
| 6-Ac | 36 | 40 | 1.0 | 710 | 7 | 20 | 1.0 | 40 | 7 | 10 | 1.0 | 250 | |
| Morphine | 53 | 2650 | 10.0 | 50,400 | 9 | 1330 | 20.0 | 11,700 | 12 | 310 | 90.0 | 5350 | |
| Codeine | 52 | 220 | 3.0 | 12,110 | 7 | 140 | 3.0 | 660 | 11 | 20 | 5.0 | 1210 | |
| Vitreous Humor | 6-MAM | 53 | 25 | 3.0 | 240 | 9 | 20 | 3.4 | 125 | 8 | 30 | 1.0 | 80 |
| 6-Ac | 27 | 2 | Tr | 20 | 6 | 4 | 1.0 | 20 | 2 | 10 | 1.0 | 10 | |
| Morphine | 53 | 90 | 10.0 | 890 | 9 | 90 | 10.0 | 260 | 9 | 120 | 11.0 | 300 | |
| Codeine | 52 | 10 | 1.0 | 140 | 9 | 10 | 3.0 | 20 | 8 | 10 | 200 | 30 | |
| Bile | 6-MAM | 8 | 10 | 2.0 | 40 | 6 | 10 | 10.0 | 40 | 3 | 10 | 1.0 | 160 |
| 6-Ac | 2 | 3 | 1.0 | 5 | 5 | 4 | 1.0 | 10 | 1 | 1 | 1.0 | 1 | |
| Morphine | 16 | 1590 | 130.0 | 41,100 | 6 | 4180 | 1510.0 | 9440 | 6 | 1060 | 40.0 | 403400 | |
| Codeine | 15 | 30 | 5.0 | 170 | 6 | 50 | 20.0 | 230 | 4 | 20 | 10 | 190 | |
| Location of Death | Putrefaction | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Indoor | Outdoor | Non-Putrefied | Partial Putrefied | Heavy Putrefied | |||||||||||||||||
| Total Case Number | 36 | 61 | 76 | 13 | 8 | ||||||||||||||||
| Analytes & | N # | Median | Minimum | Maximum | N | Median | Minimum | Maximum | N | Median | Minimum | Maximum | N | Median | Minimum | Maximum | N | Median | Minimum | Maximum | |
| Blood with Sodium Fluoride | 6-MAM | 21 | 10 | Tr * | 420 | 29 | 10 | 1.0 | 150 | 46 | 10 | Tr | 420 | 2 | 10 | 1.0 | 10 | 2 | 10 | 3.0 | 20 |
| 6-AC | 9 | 4 | Tr | 30 | 11 | 2 | Tr | 10 | 20 | 3 | Tr | 30 | 0 | ||||||||
| MOR | 33 | 320 | 20.0 | 4400 | 51 | 240 | 100.0 | 830 | 68 | 270 | 20.0 | 4400 | 10 | 320 | 121.0 | 725 | 6 | 370 | 200.0 | 720 | |
| COD | 33 | 20 | 3.0 | 140 | 51 | 20 | 3.0 | 110 | 68 | 20 | 3.0 | 140 | 10 | 20 | 3.0 | 60 | 6 | 20 | 4.0 | 70 | |
| Urine | 6-MAM | 30 | 310 | 10.0 | 18,900 | 44 | 360 | 1.0 | 4600 | 60 | 320 | 1.0 | 18,900 | 8 | 340 | 1.0 | 2520 | 6 | 540 | 130.0 | 1580 |
| 6-AC | 17 | 30 | 3.0 | 670 | 33 | 40 | 1.0 | 710 | 39 | 35 | Tr | 710 | 6 | 50 | 1.0 | 250 | 5 | 10 | 2.0 | 160 | |
| MOR | 30 | 1090 | 100.0 | 42,300 | 44 | 2030 | 10.0 | 50,400 | 60 | 1850 | 10.0 | 42,300 | 8 | 710 | 122.0 | 50,400 | 6 | 1140 | 520.0 | 4110 | |
| COD | 28 | 180 | 5.0 | 12,110 | 42 | 210 | 3.0 | 2100 | 56 | 200 | 3.0 | 12,110 | 8 | 50 | 3.0 | 1590 | 6 | 130 | 10.0 | 2100 | |
| Vitreous Humor | 6-MAM | 27 | 40 | 10.0 | 240 | 43 | 20 | 1.0 | 215 | 60 | 20 | 1.0 | 240 | 6 | 40 | 1.0 | 220 | 4 | 25 | 20.0 | 30 |
| 6-AC | 12 | 3 | Tr | 20 | 23 | 1 | Tr | 15 | 32 | 2 | Tr | 20 | 2 | 10 | 1.0 | 10 | 1 | 1 | 1.0 | 1 | |
| MOR | 27 | 100 | 10.0 | 490 | 44 | 80 | 10.0 | 890 | 60 | 70 | 10.0 | 890 | 6 | 220 | 11.0 | 550 | 5 | 140 | 40.0 | 300 | |
| COD | 26 | 20 | 3.0 | 70 | 43 | 10 | 1.0 | 140 | 58 | 10 | 1.0 | 140 | 6 | 15 | 2.0 | 30 | 5 | 10 | 3.0 | 10 | |
| Bile | 6-MAM | 9 | 10 | 2.0 | 40 | 8 | 10 | 1.0 | 160 | 12 | 10 | 1.0 | 160 | 3 | 10 | 2.0 | 40 | 2 | 10 | 2.0 | 10 |
| 6-AC | 3 | 1 | 1.0 | 3 | 5 | 5 | 1.0 | 10 | 6 | 2 | Tr | 10 | 1 | 4 | 4.0 | 4 | 1 | 5 | 5.0 | 5 | |
| MOR | 14 | 1075 | 40.0 | 7800 | 14 | 3520 | 120.0 | 41,100 | 21 | 1830 | 120.0 | 41,100 | 4 | 1520 | 40.0 | 4470 | 3 | 2150 | 490.0 | 40,400 | |
| COD | 12 | 20 | 5.0 | 120 | 13 | 70 | 10 | 230 | 19 | 30 | 5.0 | 230 | 3 | 40 | 13.0 | 40 | 3 | 70 | 10.0 | 190 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Asmari, A.I.; Alharbi, H.; Al-Zahrani, A.E.; Zughaibi, T.A. Heroin-Related Fatalities in Jeddah, Saudi Arabia, between 2008 and 2018. Toxics 2023, 11, 248. https://doi.org/10.3390/toxics11030248
Al-Asmari AI, Alharbi H, Al-Zahrani AE, Zughaibi TA. Heroin-Related Fatalities in Jeddah, Saudi Arabia, between 2008 and 2018. Toxics. 2023; 11(3):248. https://doi.org/10.3390/toxics11030248
Chicago/Turabian StyleAl-Asmari, Ahmed I., Hassan Alharbi, Abdulnasser E. Al-Zahrani, and Torki A. Zughaibi. 2023. "Heroin-Related Fatalities in Jeddah, Saudi Arabia, between 2008 and 2018" Toxics 11, no. 3: 248. https://doi.org/10.3390/toxics11030248
APA StyleAl-Asmari, A. I., Alharbi, H., Al-Zahrani, A. E., & Zughaibi, T. A. (2023). Heroin-Related Fatalities in Jeddah, Saudi Arabia, between 2008 and 2018. Toxics, 11(3), 248. https://doi.org/10.3390/toxics11030248