
Understanding Motor Skill Learning as Related to Dentistry




Abstract
1. Introduction
2. Materials and Methods
3. Motor Skill Learning Theories
3.1. Schema Theory
3.2. The OPTIMAL Theory of Motor Learning
3.3. Cognitive Load Theory
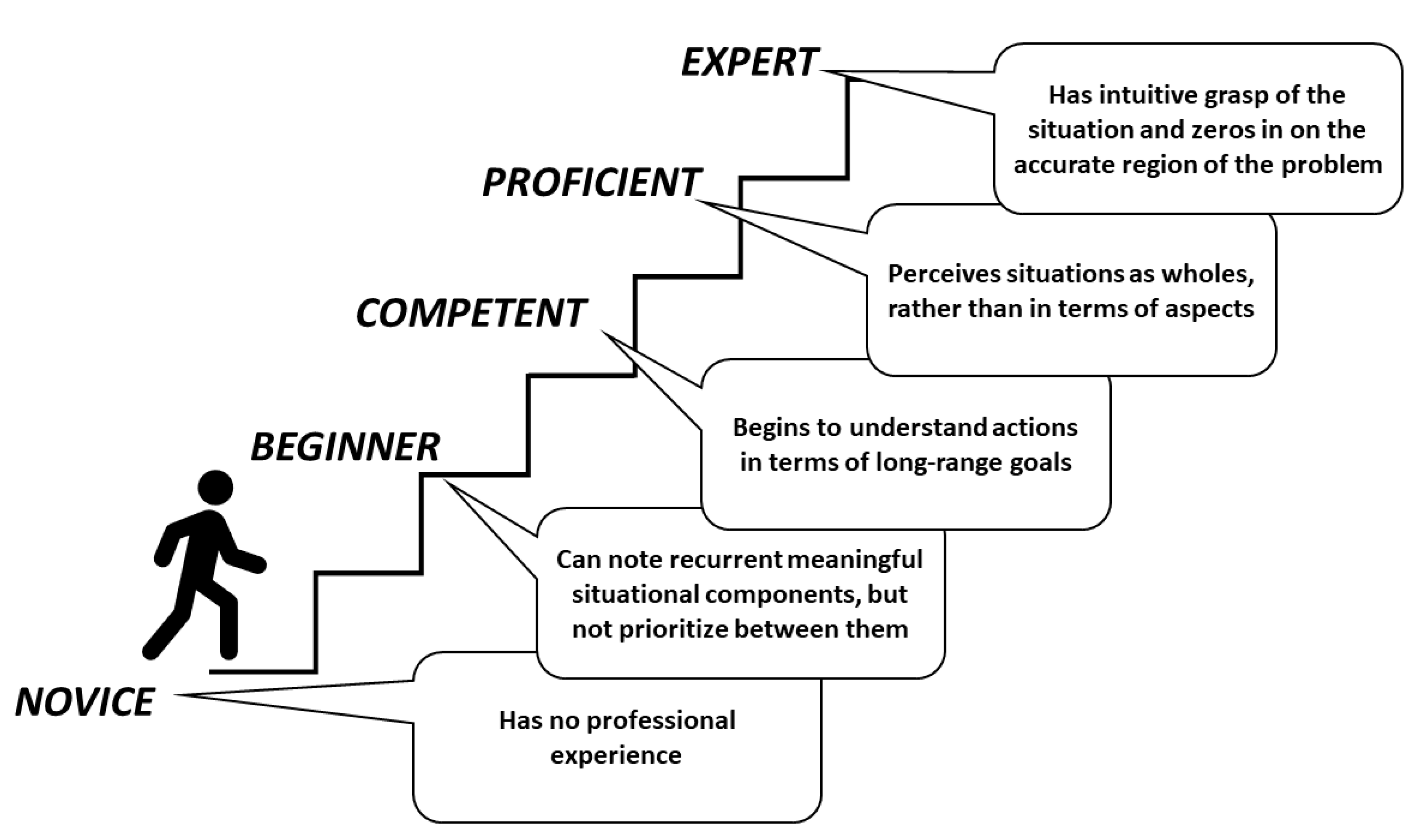
3.4. Novice-Expert Continuum and Deliberate Practice Principles
3.5. Reinvestment Theory
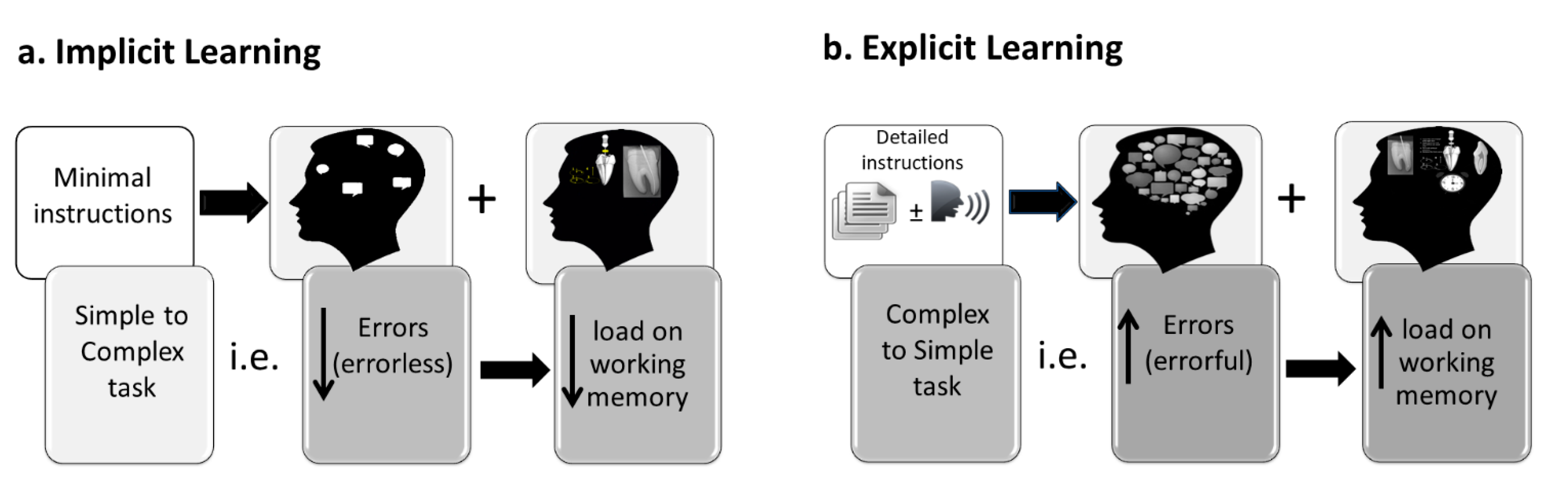
Implicit and Explicit Learning
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Tedesco, L. Issues in dental curriculum development and change. J. Dent. Educ. 1995, 59, 97–147. [Google Scholar] [CrossRef]
- Glickman, G.; Gluskin, A.; Johnson, W.; Lin, J. The crisis in endodontic education: Current perspectives and strategies for change. J. Endod. 2005, 31, 255–261. [Google Scholar] [CrossRef]
- McNally, M.; Dunning, D.; Lange, B.; Gound, T. A survey of endodontic residents’ attitudes about a career in dental education. J. Endod. 2002, 28, 592–594. [Google Scholar] [CrossRef]
- Knight, G.; Guenzel, P.; Feil, P. Using questions to facilitate motor skill acquisition. J. Dent. Educ. 1997, 61, 56–65. [Google Scholar] [CrossRef]
- Wierinck, E.; Puttemans, V.; Swinnen, S.; van Steenberghe, D. Expert performance on a virtual reality simulation system. J. Dent. Educ. 2007, 71, 759–766. [Google Scholar] [CrossRef]
- Winning, T.; Malhotra, N.; Masters, R. Investigating an errorless learning approach for developing dental operative technique skills: A pilot study. Eur. J. Dent. Educ. 2018, 22, e706–e714. [Google Scholar] [CrossRef] [PubMed]
- Koedijker, J.; Poolton, J.; Maxwell, J.; Oudejans, R.; Beek, P.; Masters, R. Attention and time constraints in perceptual-motor learning and performance: Instruction, analogy, and skill level. Conscious. Cogn. 2011, 20, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Friedlander, L.; Anderson, V. A new predoctoral endodontic module: Evaluating learning and effectiveness. J. Dent. Educ. 2011, 75, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Sonntag, D.; Barwald, R.; Hulsmann, M.; Stachniss, V. Pre-clinical endodontics: A survey amongst German dental schools. Int. Endod. J. 2008, 41, 863–868. [Google Scholar] [CrossRef] [PubMed]
- Chandler, N.; Shaw, J.; Treble, S. Effect of endodontic instrument handle diameter on operator performance. J. Endod. 1996, 22, 110–111. [Google Scholar] [CrossRef]
- Chandler, N.; Ford, T.; Monteith, B. Pulp size in molars: Underestimation on radiographs. J. Oral. Rehabil. 2004, 31, 764–769. [Google Scholar] [CrossRef] [PubMed]
- Min, L.; Yun-hui, L.; Qiang, H. An optimized haptic interaction model based on support vector regression for evaluation of endodontic shaping skill. In Proceedings of the IEEE International Conference on Robotics and Biomimetics (ROBIO), Sanya, China, 15–18 December 2007; pp. 617–622. [Google Scholar]
- El-Kishawi, M.; Khalaf, K.; Masters, R.; Winning, T. Effect of errorless learning on the acquisition of fine motor skills in pre-clinical endodontics. Aust. Endod. J. 2021, 47, 43–53. [Google Scholar] [CrossRef]
- El-Kishawi, M.Y.; Khalaf, K.; Odeh, R.M. Determining the impact of stressors on students’ clinical performance in endodontics. J. Taibah. Univ. Med. Sci. 2021. [Google Scholar] [CrossRef]
- El-Kishawi, M.; Khalaf, K.; Winning, T. How to Improve Fine Motor Skill Learning in Dentistry. Int. J. Dent. 2021, 2021, 1–8. [Google Scholar] [CrossRef]
- Schmidt, R. A schema theory of discrete motor skill learning. Psychol. Rev. 1975, 82, 225–260. [Google Scholar] [CrossRef]
- Wulf, G.; Lewthwaite, R. Optimizing performance through intrinsic motivation and attention for learning: The OPTIMAL theory of motor learning. Psychon. Bull. Rev. 2016, 23, 1382–1414. [Google Scholar] [CrossRef]
- Sweller, J. Cognitive load during problem solving: Effects on learning. Cogn. Sci. 1988, 12, 257–285. [Google Scholar] [CrossRef]
- Dreyfus, H.; Dreyfus, S.; Zadeh, L. Mind over machine: The power of human intuition and expertise in the era of the computer. IEEE Expert 1987, 2, 110–111. [Google Scholar] [CrossRef]
- Masters, R.; Polman, R.; Hammond, N. ‘Reinvestment’: A dimension of personality implicated in skill breakdown under pressure. Pers. Individ. Dif. 1993, 14, 655–666. [Google Scholar] [CrossRef]
- Miller, G. The magical number seven, plus or minus two: Some limits on our capacity for processing information. Psychol. Rev. 1956, 63, 81–97. [Google Scholar] [CrossRef]
- Adams, J. A closed-loop theory of motor learning. J. Mot. Behav. 1971, 3, 111–149. [Google Scholar] [CrossRef]
- Schmidt, R. Motor schema theory after 27 years: Reflections and implications for a new theory. Res. Q. Exerc. Sport 2003, 74, 366–375. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.; Lee, T. The learning process. In Motor Control and Learning: A Behavioral Emphasis, 4th ed.; Human Kinetics: Champaign, IL, USA, 2005; pp. 401–431. [Google Scholar]
- Hendricson, W.D. Changes in educational methodologies in predoctoral dental education: Finding the perfect intersection. J Dent. Educ. 2012, 76, 118–141. [Google Scholar] [CrossRef]
- Sherwood, D.; Lee, T. Schema theory: Critical review and implications for the role of cognition in a new theory of motor learning. Res. Q. Exerc. Sport 2003, 74, 376–382. [Google Scholar] [CrossRef]
- Rose, D.; Christina, R. A Multilevel Approach to the Study of Motor Control and Learning, 2nd ed.; Pearson/Benjamin Cummings: San Francisco, CA, USA, 2006. [Google Scholar]
- Schmidt, R.; Lee, T. Augmented feedback. In Motor Control and Learning: A Behavioral Emphasis, 4th ed.; Human Kinetics: Champaign, IL, USA, 2005; pp. 364–400. [Google Scholar]
- Lai, Q.; Shea, C. Generalized motor program (GMP) learning: Effects of reduced frequency of knowledge of results and practice variability. J. Mot. Behav. 1998, 30, 51–59. [Google Scholar] [CrossRef]
- Lai, Q.; Shea, C. Bandwidth knowledge of results enhances generalized motor program learning. Res. Q. Exerc. Sport 1999, 70, 79–83. [Google Scholar] [CrossRef]
- Wulf, G.; Shea, C.; Lewthwaite, R. Motor skill learning and performance: A review of influential factors. Med. Educ. 2010, 44, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Wulf, G.; Prinz, W. Directing attention to movement effects enhances learning: A review. Psychon. Bull. Rev. 2001, 8, 648–660. [Google Scholar] [CrossRef]
- Hendricson, W.; Andrieu, S.; Chadwick, D.; Chmar, J.; Cole, J.; George, M.; Glickman, G.; Glover, J.; Goldberg, J.; Haden, N.; et al. Educational strategies associated with development of problem-solving, critical thinking, and self-directed learning. J. Dent. Educ. 2006, 70, 925–936. [Google Scholar]
- Lam, W.; Masters, R.; Maxwell, J. Cognitive demands of error processing associated with preparation and execution of a motor skill. Conscious. Cogn. 2010, 19, 1058–1061. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J. Acquisition of cognitive skill. Psychol. Rev. 1982, 89, 369–406. [Google Scholar] [CrossRef]
- de Jong, T. Cognitive load theory, educational research, and instructional design: Some food for thought. Instr. Sci. 2010, 38, 105–134. [Google Scholar] [CrossRef]
- Sweller, J.; van Merrienboer, J.; Paas, F. Cognitive architecture and instructional design. Educ. Psychol. Rev. 1998, 10, 251–296. [Google Scholar] [CrossRef]
- Robertson, L. Memory and the brain. J. Dent. Educ. 2002, 66, 30–42. [Google Scholar] [CrossRef]
- Sweller, J.; Ayres, P.; Kalyuga, S. Interacting with the external environment: The narrow limits of change principle and the environmental organising and linking principle. In Cognitive Load Theory; Springer: Berlin/Heidelberg, Germany, 2011; pp. 39–53. [Google Scholar]
- van Merrienboer, J.; Sweller, J. Cognitive load theory in health professional education: Design principles and strategies. Med. Educ. 2010, 44, 85–93. [Google Scholar] [CrossRef]
- Cowan, N. Working Memory Underpins Cognitive Development, Learning, and Education. Educ. Psychol. Rev. 2014, 26, 197–223. [Google Scholar] [CrossRef]
- Chase, W.; Simon, H. Perception in chess. Cogn. Psychol. 1973, 4, 55–81. [Google Scholar] [CrossRef]
- Paas, F.; Ayres, P. Cognitive Load Theory: A broader view on the role of memory in learning and education. Educ. Psychol. Rev. 2014, 26, 191–195. [Google Scholar] [CrossRef]
- Hendricson, W.; Kleffner, J. Curricular and instructional implications of competency-based dental education. J. Dent. Educ. 1998, 62, 183–196. [Google Scholar] [CrossRef]
- Abernethy, B.; Poolton, J.; Masters, R.; Patil, N. Implications of an expertise model for surgical skills training. ANZ J. Surg. 2008, 78, 1092–1095. [Google Scholar] [CrossRef]
- Hendricson, W.; Kleffner, J. Assessing and helping challenging students: Part one, why do some students have difficulty learning? J. Dent. Educ. 2002, 66, 43–61. [Google Scholar] [CrossRef]
- Masters, R.; Poolton, J. Advances in implicit motor learning. In Skill Acquisition in Sport: Research, Theory and Practice, 2nd ed.; Hodges, N., Williams, M., Eds.; Routledge: London, UK, 2012; pp. 59–75. [Google Scholar]
- Kleynen, M.; Braun, S.; Bleijlevens, M.; Lexis, M.; Rasquin, S.; Halfens, J.; Wilson, M.; Beurskens, A.; Masters, R. Using a Delphi technique to seek consensus regarding definitions, descriptions and classification of terms related to implicit and explicit forms of motor learning. PLoS ONE 2014, 9, e100227. [Google Scholar] [CrossRef]
- Malhotra, N.; Poolton, J.; Wilson, M.; Ngo, K.; Masters, R. Conscious monitoring and control (reinvestment) in surgical performance under pressure. Surg. Endosc. 2012, 26, 2423–2429. [Google Scholar] [CrossRef]
- Poolton, J.; Zhu, F.; Malhotra, N.; Leung, G.; Fan, J.; Masters, R. Multitask training promotes automaticity of a fundamental laparoscopic skill without compromising the rate of skill learning. Surg. Endosc. 2016, 30, 4011–4018. [Google Scholar] [CrossRef] [PubMed]
- Masters, R.; Maxwell, J. The theory of reinvestment. Int. Rev. Sport Exerc. Psychol. 2008, 1, 160–183. [Google Scholar] [CrossRef]
- Masters, R. Knowledge, knerves and know-how: The role of explicit versus implicit knowledge in the breakdown of a complex motor skill under pressure. Br. J. Psychol. 1992, 83, 343–358. [Google Scholar] [CrossRef]
- Jackson, R.C.; Kinrade, N.P.; Hicks, T.; Wills, R. Individual propensity for reinvestment: Field-based evidence for the predictive validity of three scales. Inter. J. Sport Psychol. 2013, 44, 331–350. [Google Scholar]
- Masters, R.; Maxwell, J. Implicit motor learning, reinvestment and movement disruption: What you. In Skill Acquisition in Sport: Research, Theory and Practice, 1st ed.; Williams, A., Hodges, N., Eds.; Routledge: London, UK, 2004; pp. 207–228. [Google Scholar]
- Liao, C.; Masters, R. Analogy learning: A means to implicit motor learning. J. Sports Sci. 2001, 19, 307–319. [Google Scholar] [CrossRef]
- Dubrowski, A.; Brydges, R.; Satterthwaite, L.; Xeroulis, G.; Classen, R. Do not teach me while I am working! Am. J. Surg. 2012, 203, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Poolton, J.; Wilson, M.; Hu, Y.; Maxwell, J.; Masters, R. Implicit motor learning promotes neural efficiency during laparoscopy. Surg. Endosc. 2011, 25, 2950–2955. [Google Scholar] [CrossRef]
- Poolton, J.; Masters, R.; Maxwell, J. The relationship between initial errorless learning conditions and subsequent performance. Hum. Mov. Sci. 2005, 24, 362–378. [Google Scholar] [CrossRef] [PubMed]
- Kleynen, M.; Braun, S.; Rasquin, S.; Bleijlevens, M.; Lexis, M.; Halfens, J.; Wilson, M.; Masters, R.; Beurskens, A. Multidisciplinary views on applying explicit and implicit motor learning in practice: An international survey. PLoS ONE 2015, 10, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Lam, W.; Maxwell, J.; Masters, R. Probing the allocation of attention in implicit (motor) learning. J. Sports Sci. 2010, 28, 1543–1554. [Google Scholar] [CrossRef]
- Masters, R.; Poolton, J.; Abernethy, B.; Patil, N. Implicit learning of movement skills for surgery. ANZ J. Surg. 2008, 78, 1062–1064. [Google Scholar] [CrossRef]
- Masters, R.; Lo, C.; Maxwell, J.; Patil, N. Implicit motor learning in surgery: Implications for multi-tasking. Surgery 2008, 143, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Seger, C. Implicit learning. Psychol Bull 1994, 115, 163–196. [Google Scholar] [CrossRef]
- Maxwell, J.; Masters, R.; Kerr, E.; Weedon, E. The implicit benefit of learning without errors. Q. J. Exp. Psychol. A 2001, 54, 1049–1068. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Term | Description |
|---|---|
| Augmented (extrinsic) feedback | Supplementary or reinforcing feedback received from the surrounding environment related to the movement outcome and the quality of the executed movement. |
| Block practice | Performing a motor task in a repetitive manner without variation in the practice (e.g., AAA, BBB, CCC). |
| Chunking | Dividing large pieces of information into smaller elements that are easier to store in the short-term memory. |
| Cognitive knowledge | Acquiring factual existing information and discovering new knowledge through human thinking. |
| Declarative knowledge | Descriptive information stored in memory that is static in nature which describes things, events, or processes. |
| Errorful learning | Learning by loading the learning environment (e.g., instructions, skill difficulty) aiming to increase errors. |
| Errorless learning | Learning by constraining the learning environment (e.g., instructions, skill difficulty) aiming to reduce errors. |
| Explicit learning | Learning which generates verbal knowledge of movement performance (i.e., facts and rules) that is dependent on working memory. |
| External focus | Occurs when the learner’s focus of attention is directed toward the effect of the motor task (e.g., final shape of the cavity preparation). |
| Extraneous cognitive load | Dependent on how movement information is presented to learner and controlled by the design of instructions. |
| Generalized motor program | Stored muscle general rules that may be applied to different environmental or situational contexts. |
| Germane cognitive load | The work put into processing, construction, and automation of movement knowledge to create a permanent store in memory. |
| Hypothesis testing | Learning by repetitive attempt to perform a task by detecting and correcting errors. |
| Implicit learning | Learning with minimal increase in verbal knowledge (i.e., facts and rules) of movement resulting in skills that are unconsciously retrieved from memory. |
| Inherent (intrinsic) feedback | Feedback related to information about motor task gained through sensory channels during or after the execution of the movement. |
| Internal focus | Occurs when the learner’s focus of attention is directed toward the action of the motor task (e.g., hand movement or bur angulation). |
| Intrinsic cognitive load | Directly related to learning task and defined by the number and interaction of the processed elements. |
| Random practice | Performing a motor task in a random manner with variation in the practice (e.g., ABC, BCA, CAB). |
| Sensory memory | Type of short-term memory that is able to process and recall information related to sensory input. |
| Working memory | Short-term memory that can store small amount of information for the execution of cognitive processes. |
| Theory | Description | Points in Favor | Points Against |
|---|---|---|---|
| 1. Schema Theory [16] | Motor learning involves ongoing processes that update the recall and recognition of proprioceptive information from limbs and fingers. The response parameters (e.g., speed and force) are specified according to stored knowledge of the results. |
|
|
| 2. The OPTIMAL theory of motor learning [17] | Focuses on discovering the correct instructional approach to support motivation and direction of motor learning to the desired outcome of the motor task. |
|
|
| 3. Cognitive Load Theory [18] | Based on the assumption that cognitive system is limited as working memory can only store and process a small amount of information for a few seconds. |
|
|
| 4. Novice-Expert continuum and deliberate practice principles [19] | Development of expert motor performance depends on continuous deliberate practice improved by trial-and-error learning and supported by appropriate supervision. |
|
|
| 5. Reinvestment Theory [20] | Based on the distinction between individual’s movement self-consciousness features related to movement processing and decision making. |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El-Kishawi, M.; Khalaf, K.; Winning, T. Understanding Motor Skill Learning as Related to Dentistry. Dent. J. 2021, 9, 68. https://doi.org/10.3390/dj9060068
El-Kishawi M, Khalaf K, Winning T. Understanding Motor Skill Learning as Related to Dentistry. Dentistry Journal. 2021; 9(6):68. https://doi.org/10.3390/dj9060068
Chicago/Turabian StyleEl-Kishawi, Mohamed, Khaled Khalaf, and Tracey Winning. 2021. "Understanding Motor Skill Learning as Related to Dentistry" Dentistry Journal 9, no. 6: 68. https://doi.org/10.3390/dj9060068
APA StyleEl-Kishawi, M., Khalaf, K., & Winning, T. (2021). Understanding Motor Skill Learning as Related to Dentistry. Dentistry Journal, 9(6), 68. https://doi.org/10.3390/dj9060068