
Hair Cortisol Concentrations Are Associated with Dental Anxiety during Pregnancy

 ,
, 
Abstract
1. Introduction
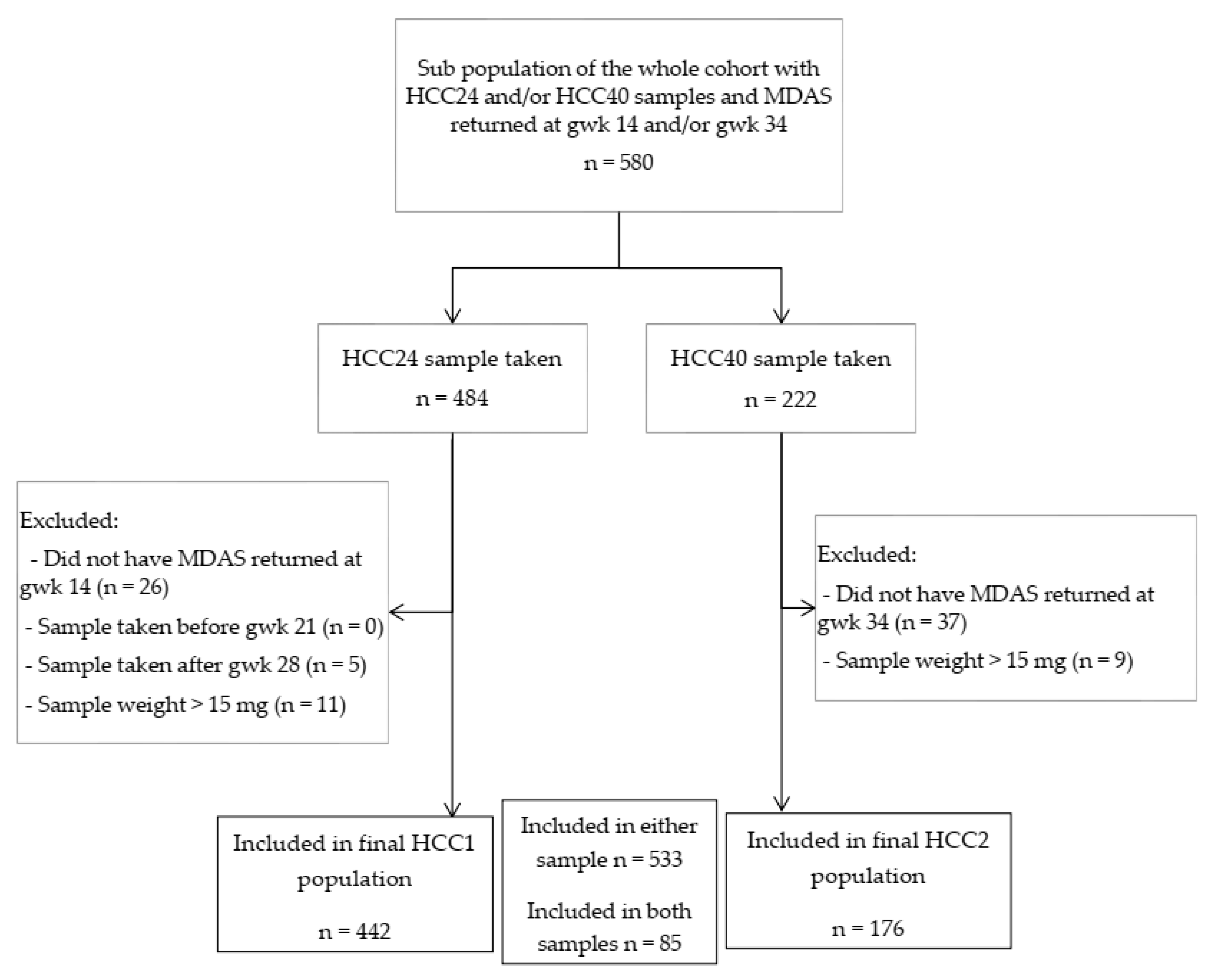
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pohjola, V.; Lahti, S.; Vehkalahti, M.M.; Tolvanen, M.; Hausen, H. Association between dental fear and dental attendance among adults in Finland. Acta Odontol. Scand. 2007, 65, 224–230. [Google Scholar] [CrossRef]
- Armfield, J.M. What goes around comes around: Revisiting the hypothesized vicious cycle of dental fear and avoidance. Community Dent. Oral 2012, 41, 279–287. [Google Scholar] [CrossRef]
- Liinavuori, A.; Tolvanen, M.; Pohjola, V.; Lahti, S. Longitudinal interrelationships between dental fear and dental attendance among adult Finns in 2000–2011. Community Dent. Oral 2019, 47, 309–315. [Google Scholar] [CrossRef]
- Pohjola, V.; Lahti, S.; Vehkalahti, M.M.; Tolvanen, M.; Hausen, H. Age-specific associations between dental fear and dental condition among adults in Finland. Acta Odontol. Scand. 2008, 66, 278–285. [Google Scholar] [CrossRef]
- Pohjola, V.; Lahti, S.; Suominen-Taipale, L.; Hausen, H. Dental fear and subjective oral impacts among adults in Finland. Eur. J. Oral Sci. 2009, 117, 268–272. [Google Scholar] [CrossRef]
- Beaton, L.; Freeman, R.; Humphris, G.M. Why Are People Afraid of the Dentist? Observations and Explanations. Med. Princ. Pract. 2014, 23, 295–301. [Google Scholar] [CrossRef]
- Locker, D.; Liddell, A.; Dempster, L.; Shapiro, D. Age of onset of dental anxiety. J. Dent. Res. 1999, 78, 790–796. [Google Scholar] [CrossRef] [PubMed]
- Locker, D.; Poulton, R.; Thomson, W.M. Psychological disorders and dental anxiety in a young adult population. Community Dent. Oral 2001, 29, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Pohjola, V.; Mattila, A.K.; Joukamaa, M.; Lahti, S. Anxiety and depressive disorders and dental fear among adults in Finland. Eur. J. Oral Sci. 2011, 119, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Aartman, I.H.A.; De Jongh, A.; Van Der Meulen, M.J. Psychological characteristics of patients applying for treatment in a dental fear clinic. Eur. J. Oral Sci. 1997, 105, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Locker, D.; Shapiro, D.; Liddell, A. Overlap between dental anxiety and blood-injury fears: Psychological characteristics and response to dental treatment. Behav. Res. Ther. 1997, 35, 583–590. [Google Scholar] [CrossRef]
- De Jongh, A.; Bongaarts, G.; Vermeule, I.; Visser, K.; De Vos, P.; Makkes, P. Blood–injury–injection phobia and dental phobia. Behav. Res. Ther. 1998, 36, 971–982. [Google Scholar] [CrossRef]
- Boman, U.W.; Lundgren, J.; Berggren, U.; Carlsson, S.G. Psychosocial and dental factors in the maintenance of severe dental fear. Swed. Dent. J. 2010, 34, 121–127. [Google Scholar] [PubMed]
- Hakeberg, M.; Hägglin, C.; Berggren, U.; Carlsson, S.G. Structural relationships of dental anxiety, mood, and general anxiety. Acta Odontol. Scand. 2001, 59, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Hagglin, C.; Hakeberg, M.; Hallstrom, T.; Berggren, U.; Larsson, L.; Waern, M.; Palsson, S.; Skoog, I. Dental anxiety in relation to mental health and personality factors. A longitudinal study of middle-aged and elderly women. Eur. J. Oral Sci. 2001, 109, 27–33. [Google Scholar] [CrossRef]
- Pekkan, G.; Kilicoglu, A.; Hatipoglu, H. Relationship between dental anxiety, general anxiety level and depression in pa-tients attending a university hospital dental clinic in Turkey. Community Dent. Health 2011, 28, 149–153. [Google Scholar] [CrossRef]
- Tolvanen, M.; Hagqvist, O.; Luoto, A.; Rantavuori, K.; Karlsson, L.; Karlsson, H.; Lahti, S. Changes over time in adult dental fear and correlation to depression and anxiety: A cohort study of pregnant mothers and fathers. Eur. J. Oral Sci. 2013, 121, 264–269. [Google Scholar] [CrossRef]
- Stenebrand, A.; Boman, U.W.; Hakeberg, M. Dental anxiety and temperament in 15-year olds. Acta Odontol. Scand. 2012, 71, 15–21. [Google Scholar] [CrossRef]
- Bernson, J.M.; Elfström, M.L.; Hakeberg, M. Dental coping strategies, general anxiety, and depression among adult patients with dental anxiety but with different dental-attendance patterns. Eur. J. Oral Sci. 2013, 121, 270–276. [Google Scholar] [CrossRef]
- Halonen, H.; Salo, T.; Hakko, H.; Räsänen, P. The association between dental anxiety, general clinical anxiety and de-pression among Finnish university students. Oral Health Dent. Manag. 2014, 13, 320–325. [Google Scholar]
- Lahti, S.M.; Tolvanen, M.M.; Humphris, G.; Freeman, R.; Rantavuori, K.; Karlsson, L.; Karlsson, H. Association of depression and anxiety with different aspects of dental anxiety in pregnant mothers and their partners. Community Dent. Oral 2019, 48, 137–142. [Google Scholar] [CrossRef]
- Hagqvist, O.; Tolvanen, M.; Rantavuori, K.; Karlsson, L.; Karlsson, H.; Lahti, S. Short-term longitudinal changes in adult dental fear. Eur. J. Oral Sci. 2018, 126, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Hagqvist, O.; Tolvanen, M.; Rantavuori, K.; Karlsson, L.; Karlsson, H.; Lahti, S. Changes in dental fear and its relations to anxiety and depression in the FinnBrain Birth Cohort Study. Eur. J. Oral Sci. 2020, 128, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.; Ho, J.T.; Torpy, D.J.; Rogers, A.; Doogue, M.; Lewis, J.G.; Czajko, R.J.; Inder, W.J. A Longitudinal Study of Plasma and Urinary Cortisol in Pregnancy and Postpartum. J. Clin. Endocrinol. Metab. 2011, 96, 1533–1540. [Google Scholar] [CrossRef]
- Stalder, T.; Kirschbaum, C. Analysis of cortisol in hair—State of the art and future directions. Brain Behav. Immun. 2012, 26, 1019–1029. [Google Scholar] [CrossRef]
- Malisiova, E.K.; Mourikis, I.; Darviri, C.; Nicolaides, N.C.; Zervas, I.M.; Papageorgiou, C.; Chrousos, G.P. Hair cortisol concentrations in mental disorders: A systematic review. Physiol. Behav. 2021, 229, 113244. [Google Scholar] [CrossRef]
- Stalder, T.; Steudte-Schmiedgen, S.; Alexander, N.; Klucken, T.; Vater, A.; Wichmann, S.; Kirschbaum, C.; Miller, R. Stress-related and basic determinants of hair cortisol in humans: A meta-analysis. Psychoneuroendocrinology 2017, 77, 261–274. [Google Scholar] [CrossRef] [PubMed]
- Vives, A.H.; De Angel, V.; Papadopoulos, A.S.; Strawbridge, R.; Wise, T.H.; Young, A.H.; Arnone, D.; Cleare, A.J. The relationship between cortisol, stress and psychiatric illness: New insights using hair analysis. J. Psychiatr. Res. 2015, 70, 38–49. [Google Scholar] [CrossRef]
- de Weerth, C.; Buitelaar, J.K. Physiological stress reactivity in human pregnancy—A review. Neurosci. Biobehav. Rev. 2005, 29, 295–312. [Google Scholar] [CrossRef]
- Howland, M.A.; Sandman, C.A.; Glynn, L.M. Developmental origins of the human hypothalamic-pituitary-adrenal axis. Expert Rev. Endocrinol. Metab. 2017, 12, 321–339. [Google Scholar] [CrossRef]
- Mustonen, P.; Karlsson, L.; Scheinin, N.M.; Kortesluoma, S.; Coimbra, B.; Rodrigues, A.J.; Karlsson, H. Hair cortisol concentration (HCC) as a measure for prenatal psychological distress—A systematic review. Psychoneuroendocrinology 2018, 92, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Mustonen, P.; Karlsson, L.; Kataja, E.-L.; Scheinin, N.M.; Kortesluoma, S.; Coimbra, B.; Rodrigues, A.J.; Sousa, N.; Karlsson, H. Maternal prenatal hair cortisol is associated with prenatal depressive symptom trajectories. Psychoneuroendocrinology 2019, 109, 104383. [Google Scholar] [CrossRef]
- Karlsson, L.; Tolvanen, M.; Scheinin, N.M.; Uusitupa, H.-M.; Korja, R.; Ekholm, E.; Tuulari, J.J.; Pajulo, M.; Huotilainen, M.; Paunio, T.; et al. Cohort Profile: The FinnBrain Birth Cohort Study (FinnBrain). Int. J. Epidemiol. 2018, 47, 15–16j. [Google Scholar] [CrossRef] [PubMed]
- Greff, M.J.; Levine, J.M.; Abuzgaia, A.M.; Elzagallaai, A.A.; Rieder, M.J.; van Uum, S.H. Hair cortisol analysis: An update on methodological considerations and clinical applications. Clin. Biochem. 2019, 63, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Humphris, G.; Freeman, R.; Campbell, J.; Tuutti, H.; D’Souza, V. Further evidence for the reliability and validity of the Modified Dental Anxiety Scale. Int. Dent. J. 2000, 50, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Humphris, G.; Crawford, J.R.; Hill, K.; Gilbert, A.; Freeman, R. UK population norms for the modified dental anxiety scale with percentile calculator: Adult dental health survey 2009 results. BMC Oral Health 2013, 13, 29. [Google Scholar] [CrossRef]
- Newton, J.T.; Edwards, J.C. Psychometric properties of the modified dental anxiety scale: An independent replication. Community Dent. Health 2005, 22, 40–42. [Google Scholar]
- King, K.; Humphris, G.M. Evidence to confirm the cut-off for screening dental phobia using the Modified Dental Anxiety Scale. Soc. Sci. Dent. 2010, 1, 21–28. [Google Scholar]
- Yuan, S.; Freeman, R.; Lahti, S.; Lloyd-Williams, F.; Humphris, G. Some psychometric properties of the Chinese version of the Modified Dental Anxiety Scale with cross validation. Health Qual. Life Outcomes 2008, 6, 22. [Google Scholar] [CrossRef] [PubMed]
- Braig, S.; Grabher, F.; Ntomchukwu, C.; Reister, F.; Stalder, T.; Kirschbaum, C.; Genuneit, J.; Rothenbacher, D. Determinants of maternal hair cortisol concentrations at delivery reflecting the last trimester of pregnancy. Psychoneuroendocrinology 2015, 52, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Ursache, A.; Merz, E.C.; Melvin, S.; Meyer, J.; Noble, K.G. Socioeconomic status, hair cortisol and internalizing symptoms in parents and children. Psychoneuroendocrinology 2017, 78, 142–150. [Google Scholar] [CrossRef]
- Cox, J.L.; Chapman, G.; Murray, D.; Jones, P. Validation of the Edinburgh postnatal depression scale (EPDS) in non-postnatal women. J. Affect. Disord. 1996, 39, 185–189. [Google Scholar] [CrossRef]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of Postnatal Depression. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef]
- Derogatis, L.R.; Lipman, R.S.; Covi, L. SCL-90: An outpatient psychiatric rating scale--preliminary report. Psychopharmacol. Bull. 1973, 9, 13–28. [Google Scholar] [PubMed]
- Holi, M.M.; Sammallahti, P.R.; Aalberg, V.A. A Finnish validation study of the SCL-90. Acta Psychiatr. Scand. 1998, 97, 42–46. [Google Scholar] [CrossRef]
- Kalra, S.; Einarson, A.; Karaskov, T.; Van Uum, S.; Koren, G. The relationship between stress and hair cortisol in healthy pregnant women. Clin. Investig. Med. 2007, 30, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Orta, O.R.; Tworoger, S.S.; Terry, K.L.; Coull, B.A.; Gelaye, B.; Kirschbaum, C.; Sanchez, S.E.; Williams, M.A. Stress and hair cortisol concentrations from preconception to the third trimester. Stress 2018, 22, 60–69. [Google Scholar] [CrossRef]
- Hoffman, M.C.; Mazzoni, S.E.; Wagner, B.D.; Laudenslager, M.L.; Ross, R.G. Measures of Maternal Stress and Mood in Relation to Preterm Birth. Obstet. Gynecol. 2016, 127, 545–552. [Google Scholar] [CrossRef]
- Braig, S.; Grabher, F.; Ntomchukwu, C.; Reister, F.; Stalder, T.; Kirschbaum, C.; Rothenbacher, D.; Genuneit, J. The Association of Hair Cortisol with Self-Reported Chronic Psychosocial Stress and Symptoms of Anxiety and Depression in Women Shortly after Delivery. Paediatr. Périnat. Epidemiol. 2016, 30, 97–104. [Google Scholar] [CrossRef]
- Duffy, A.R.; Schminkey, D.L.; Groer, M.W.; Shelton, M.; Dutra, S. Comparison of Hair Cortisol Levels and Perceived Stress in Mothers Who Deliver at Preterm and Term. Biol. Res. Nurs. 2018, 20, 292–299. [Google Scholar] [CrossRef]
- Steudte, S.; Stalder, T.; Dettenborn, L.; Klumbies, E.; Foley, P.; Beesdo-Baum, K.; Kirschbaum, C. Decreased hair cortisol concentrations in generalised anxiety disorder. Psychiatry Res. 2011, 186, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Liinavuori, A.; Tolvanen, M.; Pohjola, V.; Lahti, S. Changes in dental fear among Finnish adults: A national survey. Community Dent. Oral 2015, 44, 128–134. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| HCC1 (n = 442) | HCC2 (n = 176) | |||
| Mean (SD) | Median (Q1–Q3) | Mean (SD) | Median (Q1–Q3) | |
| Age at delivery | 31.1 (4.3) | 31.1 (4.2) | ||
| BMI (kg/m2) | 24.6 (4.5) | 23.9 (21.4–26.7) | 24.4 (4.7) | 23.2 (21.2–26.2) |
| HCC (pg/mg) | 19.2 (33.4) | 10.8 (5.9–19.8) | 22.4 (30.4) | 14.4 (7.5–25.7) |
| Sample weight (mg) | 10.0 (3.1) | 9.9 (7.3–12.8) | 11.1 (3.4) | 11.8 (7.7–14.5) |
| MDAS sum | 10.0 (4.1) | 9.0 (7.0–12.0) | 9.9 (4.1) | 9.0 (7.0–11.0) |
| Anticipatory DA 1 | 3.4 (1.8) | 3.0 (2.0–4.0) | 3.2 (1.8) | 3.0 (2.0–4.0) |
| Treatment related DA 1 | 6.6 (2.7) | 6.0 (5.0–8.0) | 6.6 (2.6) | 6.0 (5.0–8.0) |
| SCL-90 score | 3.2 (3.6) | 2.0 (1.0–4.0) | 3.1 (3.7) | 2.0 (0.0–4.0) |
| EPDS score | 5.0 (3.9) | 4.0 (2.0–7.0) | 4.7 (3.8) | 4.0 (2.0–7.0) |
| HCC1 (n = 442) | HCC2 (n = 176) | |||
| n (%) | n (%) | |||
| Educational level | ||||
| High school/vocational | 106 (24.0) | 41 (23.3) | ||
| Polytechnics | 160 (36.2) | 59 (33.5) | ||
| University | 175 (39.6) | 71 (40.3) | ||
| Smoking | ||||
| No | 379 (85.7) | 150 (85.2) | ||
| Yes, before knowing about pregnancy | 47 (10.6) | 23 (13.1) | ||
| Yes | 16 (3.6) | 3 (1.7) | ||
| Use of SSRI/SNRI | ||||
| No | 416 (94.1) | 171 (97.2) | ||
| Yes | 19 (4.3) | 3 (1.7) | ||
| HCC1 (n = 442) | HCC2 (n = 176) | |||||
|---|---|---|---|---|---|---|
| n | Median (Q1–Q3) | p-Value 1 | n | Median (Q1–Q3) | p-Value 1 | |
| No to moderate DA | 419 | 11.3 (6.1–20.0) | 0.013 | 167 | 14.7 (7.4–25.9) | 0.534 |
| High DA | 23 | 6.2 (3.8–12.6) | 9 | 11.9 (7.4–22.9) | ||
| MDAS | HCC1 (n = 442) | HCC2 (n = 176) | ||||
|---|---|---|---|---|---|---|
| r | p | n | r | p | n | |
| Total score | −0.083 | 0.081 | 442 | −0.067 | 0.377 | 176 |
| Anticipatory dental anxiety | −0.099 | 0.039 | 441 | −0.083 | 0.272 | 176 |
| Treatment related dental anxiety | −0.069 | 0.148 | 442 | −0.052 | 0.491 | 176 |
| HCC1 (n = 442) | HCC2 (n = 176) | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | |
| HCC | 0.548 | 0.35–0.86 | 0.009 | 0.611 | 0.28–1.33 | 0.216 |
| SCL-90 | 0.894 | 0.74–1.08 | 0.237 | 0.827 | 0.62–1.11 | 0.204 |
| EPDS | 1.062 | 0.93–1.21 | 0.381 | 1.241 | 0.95–1.63 | 0.118 |
| Age | 0.968 | 0.88–1.07 | 0.516 | 0.912 | 0.75–1.10 | 0.341 |
| BMI | 1.112 | 1.03–1.20 | 0.007 | 0.971 | 0.83–1.13 | 0.699 |
| Smoking | 2.754 | 1.03–7.40 | 0.045 | 0.862 | 0.10–7.66 | 0.894 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viitaniemi, H.; Suominen, A.; Karlsson, L.; Mustonen, P.; Kortesluoma, S.; Rantavuori, K.; Rodrigues, A.J.; Coimbra, B.; Karlsson, H.; Lahti, S. Hair Cortisol Concentrations Are Associated with Dental Anxiety during Pregnancy. Dent. J. 2021, 9, 42. https://doi.org/10.3390/dj9040042
Viitaniemi H, Suominen A, Karlsson L, Mustonen P, Kortesluoma S, Rantavuori K, Rodrigues AJ, Coimbra B, Karlsson H, Lahti S. Hair Cortisol Concentrations Are Associated with Dental Anxiety during Pregnancy. Dentistry Journal. 2021; 9(4):42. https://doi.org/10.3390/dj9040042
Chicago/Turabian StyleViitaniemi, Hilja, Auli Suominen, Linnea Karlsson, Paula Mustonen, Susanna Kortesluoma, Kari Rantavuori, Ana João Rodrigues, Bárbara Coimbra, Hasse Karlsson, and Satu Lahti. 2021. "Hair Cortisol Concentrations Are Associated with Dental Anxiety during Pregnancy" Dentistry Journal 9, no. 4: 42. https://doi.org/10.3390/dj9040042
APA StyleViitaniemi, H., Suominen, A., Karlsson, L., Mustonen, P., Kortesluoma, S., Rantavuori, K., Rodrigues, A. J., Coimbra, B., Karlsson, H., & Lahti, S. (2021). Hair Cortisol Concentrations Are Associated with Dental Anxiety during Pregnancy. Dentistry Journal, 9(4), 42. https://doi.org/10.3390/dj9040042