Drilling Capability of Orthodontic Miniscrews: In Vitro Study

Abstract
1. Introduction
2. Materials and Methods
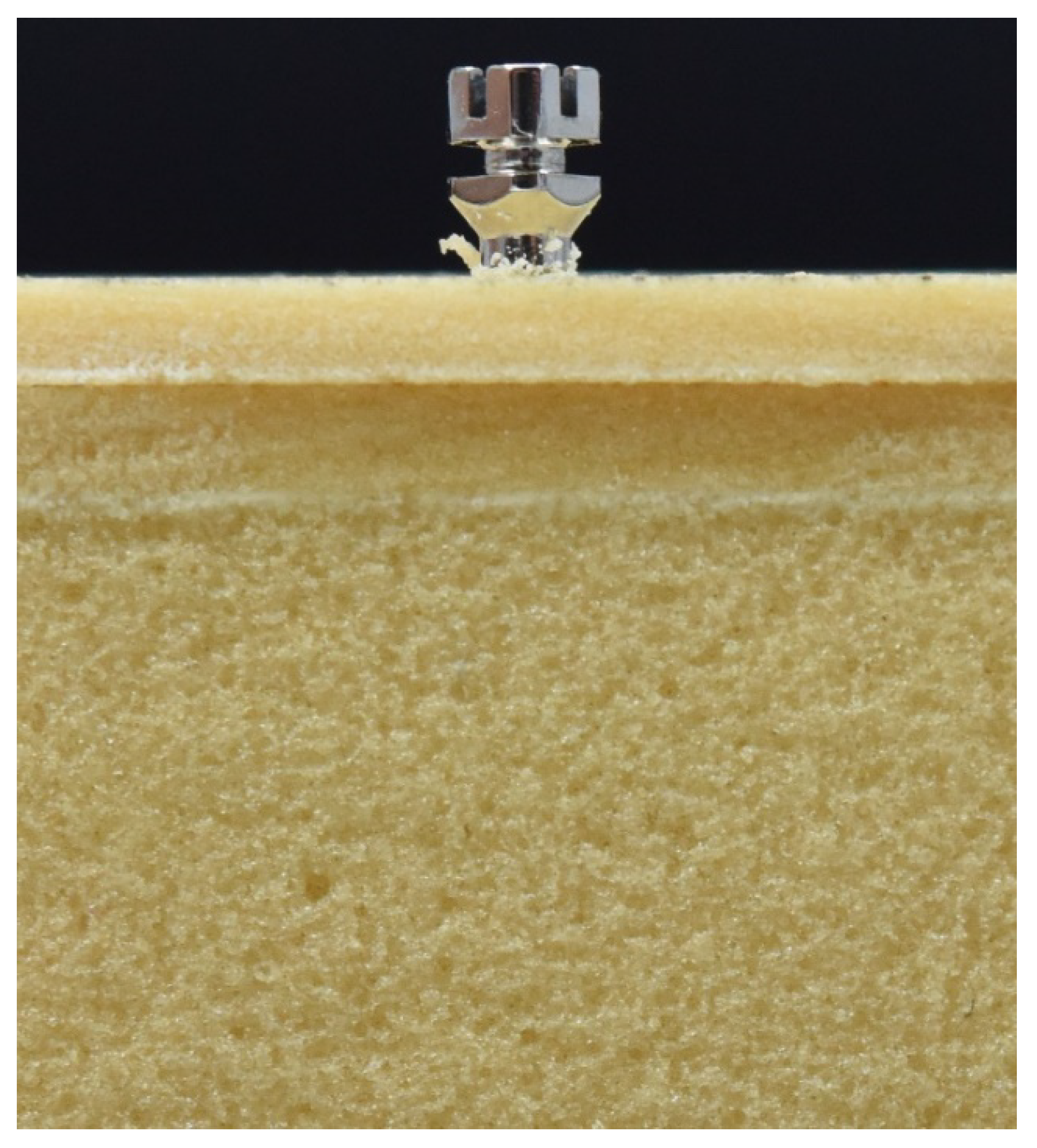
- Sample 1. Blocks composed of a cortical layer with a density of 0.64 g/cm3 (40 pounds per cubic foot (PCF)) and a thickness of 2 mm, and a cancellous bone layer with a density of 0.32 g/cm3 (20 PCF);
- Sample 2. Blocks composed of a cortical layer with a density of 0.64 g/cm3 (40 PCF) and a thickness of 4 mm, and a cancellous bone layer with a density of 0.32 g/cm3 (20 PCF);
- Sample 3. Blocks composed of a cancellous bone layer with a density of 0.32 g/cm3 (20 PCF);
- Sample 4. Blocks composed of a cortical bone layer with a density of 0.64 g/cm3 (40 PCF).
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
- -
- Clinically, it is difficult to evaluate the thickness of the cortex and its density;
- -
- The perpendicular insertion of the miniscrew is very difficult;
- -
- The force applied to insert the miniscrew is operator-dependent.
Author Contributions
Funding
Conflicts of Interest
References
- Daskaloggianakis, J. Glossary of Orthodontic Terms; Quintessence Publishing CO.: Leipzig, Germany, 2000. [Google Scholar]
- Derton, N.; Gracco, A.; Greco, A.; Luzi, C. Le Miniviti Ortodontiche, Guida All’utilizzo Clinico; Edizioni Martina: Bologna, Italy, 2015; Volume 1, p. 7. [Google Scholar]
- Cope, J.B. Temporary anchorage devices in orthodontics: A paradigm shift. Semin. Orthod. 2005, 11, 3–9. [Google Scholar] [CrossRef]
- Elias, C.N.; Ruellas, A.C.D.O.; Fernandes, D.J. Orthodontic implants: Concepts for the orthodontic practitioner. Int. J. Dent. 2012, 2012, 549761. [Google Scholar] [CrossRef] [PubMed]
- Tepedino, M.; Masedu, F.; Chimenti, C. Comparative evaluation of insertion torque and mechanical stability for self-tapping and self-drilling orthodontic miniscrews-An in vitro study. Head Face Med. 2017, 13, 10. [Google Scholar] [CrossRef] [PubMed]
- Wehrbein, H. Skeletal Anchorage in Orthodontics-Basics and Clinical Application. J. Orofac. Orthop. 2007, 68, 443–461. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.-K.; Baek, S.-H. Effects of the diameter and shape of orthodontic miniimplants on microdamage to the cortical bone. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 8.e1–8.e8. [Google Scholar] [CrossRef]
- Reynders, R.; Ronchi, L.; Ladu, L.; Van Etten-Jamaludin, F.; Bipat, S. Insertion torque and success of orthodontic mini-implants: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 596–614.e5. [Google Scholar] [CrossRef]
- Motoyoshi, M.; Hirabayashi, M.; Uemura, M.; Shimizu, N. Recommended placement torque when tightening an orthodontic mini-implant. Clin. Oral Implant. Res. 2005, 17, 109–114. [Google Scholar] [CrossRef]
- Miyawaki, S.; Koyama, I.; Inoue, M.; Mishima, K.; Sugahara, T.; Takano-Yamamoto, T. Factors associated with the stability of titanium screws placed in the posterior region for orthodontic anchorage. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 373–378. [Google Scholar] [CrossRef]
- Yerby, S.; Scott, C.C.; Evans, N.J.; Messing, K.L.; Carter, D.R. Effect of cutting flute design on cortical bone screw insertion torque and pullout strength. J. Orthop. Trauma 2001, 15, 216–221. [Google Scholar] [CrossRef]
- O′Sullivan, D.J.; Sennerby, L.; Meredith, N. Influence of implant taper on the primary and secondary stability of osseointegrated titanium implants. Clin. Oral Implant. Res. 2004, 15, 474–480. [Google Scholar] [CrossRef]
- Öktenoǧlu, B.T.; Ferrara, L.A.; Andalkar, N.; Özer, A.F.; Sarioǧlu, A. Çetin; Benzel, E.C. Effects of hole preparation on screw pullout resistance and insertional torque: A biomechanical study. J. Neurosurg. Spine 2001, 94, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Heidemann, W.; Gerlach, K.L.; Gröbel, K.-H.; Köllner, H.-G. Influence of different pilot hole sizes on torque measurements and pullout analysis of osteosynthesis screws. J. Cranio Maxillofac. Surg. 1998, 26, 50–55. [Google Scholar] [CrossRef]
- Butcher, A.; Wiechmann, D.; Koerdt, S.; Wiesmann, H.; Piffko, J.; Meyer, U. Load-related implant eaction of mini-impants used for orthodontic anchorage. Clin. Oral Implants Res. 2005, 16, 473–479. [Google Scholar]
- Chen, Y.-J.; Chen, Y.-H.; Lin, L.; Yao, C.-C.J. Removal torque of miniscrews used for orthodontic anchorage—a preliminary report. Int. J. Oral Maxillofac. Implant. 2006, 21, 283–289. [Google Scholar]
- Son, S.; Motoyoshi, M.; Uchida, Y.; Shimizu, N. Comparative study of the primary stability of self-drilling and self-tapping orthodontic miniscrews. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 480–485. [Google Scholar] [CrossRef]
- Ueda, M.; Matsuki, M.; Jacobsson, M.; Tjellström, A. Relationship between insertion torque and removal torque analyzed in fresh temporal bone. Int. J. Oral Maxillofac. Implant. 1991, 6, 442–447. [Google Scholar]
- O’Sullivan, D.; Sennerby, L.; Meredith, N. Measurements comparing the initial stability of five designs of dental implants: A human cadaver study. Clin. Implant. Dent. Relat. Res. 2000, 2, 85–92. [Google Scholar] [CrossRef]
- Ivanoff, C.; Sennerby, L.; Lekholm, U. Influence of initial implant mobility on the integration of titanium implants. An experimental study in rabbits. Clin. Oral Res. 1996, 7, 120–127. [Google Scholar] [CrossRef]
- Meredith, N. Assessment of implant stability as a prognostic determinant. Int. J. Prosthodont. 1999, 11, 491–501. [Google Scholar]
- Nguyen, M.V.; Codrington, J.; Fletcher, L.; Dreyer, C.W.; Sampson, W.J. Influence of cortical bone thickness on miniscrew microcrack formation. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 301–311. [Google Scholar] [CrossRef]
- Nguyen, M.V.; Codrington, J.; Fletcher, L.; Dreyer, C.W.; Sampson, W.J. The influence of miniscrew insertion torque. Eur. J. Orthod. 2017, 40, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, I.; Tsuboi, Y.; Wada, E.; Suwa, H.; Iizuka, T. Influence of cortical bone thickness and implant length on implant stability at the time of surgery--clinical, prospective, biomechanical, and imaging study. Bone 2005, 37, 776–780. [Google Scholar] [CrossRef] [PubMed]
- Migliorati, M.; Benedicenti, S.; Signori, A.; Drago, S.; Cirillo, P.; Barberis, F.; Biavati, A.S. Thread shape factor: Evaluation of three different orthodontic miniscrews stability. Eur. J. Orthod. 2012, 35, 401–405. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Beck, T.W. The Importance of a Priori Sample Size Estimation in Strength and Conditioning Research. J. Strength Cond. Res. 2013, 27, 2323–2337. [Google Scholar] [CrossRef]
- Heidemann, W.; Gerlach, K.; Gröbel, K.; Köllner, H. Drill Free Screws: A new form of osteosynthesis screw. J. Cranio Maxillofac. Surg. 1998, 26, 163–168. [Google Scholar] [CrossRef]
- Heidemann, W.; Terheyden, H.; Gerlach, K. Analysis of the osseous metal interface of drill free screws and self-tapping screws. J. Cranio Maxillofac. Surg. 2001, 29, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Elibol, F.K.E.; Oflaz, E.; Buğra, E.; Orhan, M.; Demir, T. Effect of cortical bone thickness and density on pullout strength of mini-implants: An experimental study. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 178–185. [Google Scholar] [CrossRef]
- Motoyoshi, M.; Uemura, M.; Ono, A.; Okazaki, K.; Shigeeda, T.; Shimizu, N. Factors affecting the long-term stability of orthodontic mini-implants. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 588.e1–588.e5. [Google Scholar] [CrossRef]
- Motoyoshi, M.; Yoshida, T.; Ono, A.; Shimizu, N. Effect of cortical bone thickness and implant placement torque on stability of orthodontic mini-implants. Int. J. Oral Maxillofac. Implant. 2007, 22, 779–784. [Google Scholar]
- Fayed, M.M.S.; Pazera, P.; Katsaros, C. Optimal sites for orthodontic mini-implant placement assessed by cone beam computed tomography. Angle Orthod. 2010, 80, 939–951. [Google Scholar] [CrossRef]
- Wilmes, B.; Rademacher, C.; Olthoff, G.; Drescher, D. Parameters Affecting Primary Stability of Orthodontic Mini-implants. J. Orofac. Orthop. 2006, 67, 162–174. [Google Scholar] [CrossRef] [PubMed]
- Nucera, R.; Giudice, A.L.; Bellocchio, A.M.; Spinuzza, P.; Caprioglio, A.; Perillo, L.; Matarese, G.; Cordasco, G. Bone and cortical bone thickness of mandibular buccal shelf for mini-screw insertion in adults. Angle Orthod. 2017, 87, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, M.; Inami, T.; Ito, K.; Kasai, K.; Tanimoto, Y. Mini-Implants in the Anchorage Armamentarium: New Paradigms in the Orthodontics, International. Int. J. Biomater. 2012, 2012, 394121. [Google Scholar] [CrossRef] [PubMed]
- Bourassa, C.; Hosein, Y.K.; Pollmann, S.I.; Galil, K.; Bohay, R.N.; Holdsworth, D.W.; Tassi, A. In-vitro comparison of different palatal sites for orthodontic miniscrew insertion: Effect of bone quality and quantity on primary stability. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 809–819. [Google Scholar] [CrossRef] [PubMed]
- Hergel, C.A.; Acar, Y.B.; Ates, M.; Kucukkeles, N. In- vitro evaluation of the effects of insertion and sterilization procedures on the mechanical and surface characteristics of mini screw. Eur. Oral Res. 2018, 53, 25–31. [Google Scholar] [CrossRef]
- Mohlhenrich, S.C.; Heussen, N.; Modabber, A.; Bock, A.; Hozle, F.; Wilmes, B.; Danesh, G.; Szalma, J. Influence of bone density, screw size and surgical procedure on orthodontic mini-implant placement—Part B: Implant stability. Int. J. Oral Maxillofac. Surg. 2020, in press. [Google Scholar] [CrossRef]
- Mohlhenrich, S.C.; Heussen, N.; Modabber, A.; Kniha, K.; Hozle F, F.; Wilmes, B.; Danesh, G.; Szalma, J. Influence of bone density, screw size and surgical procedure on orthodontic mini-implant placement—Part A: Temperature development. Int. J. Oral Maxillofac. Surg. 2020, in press. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
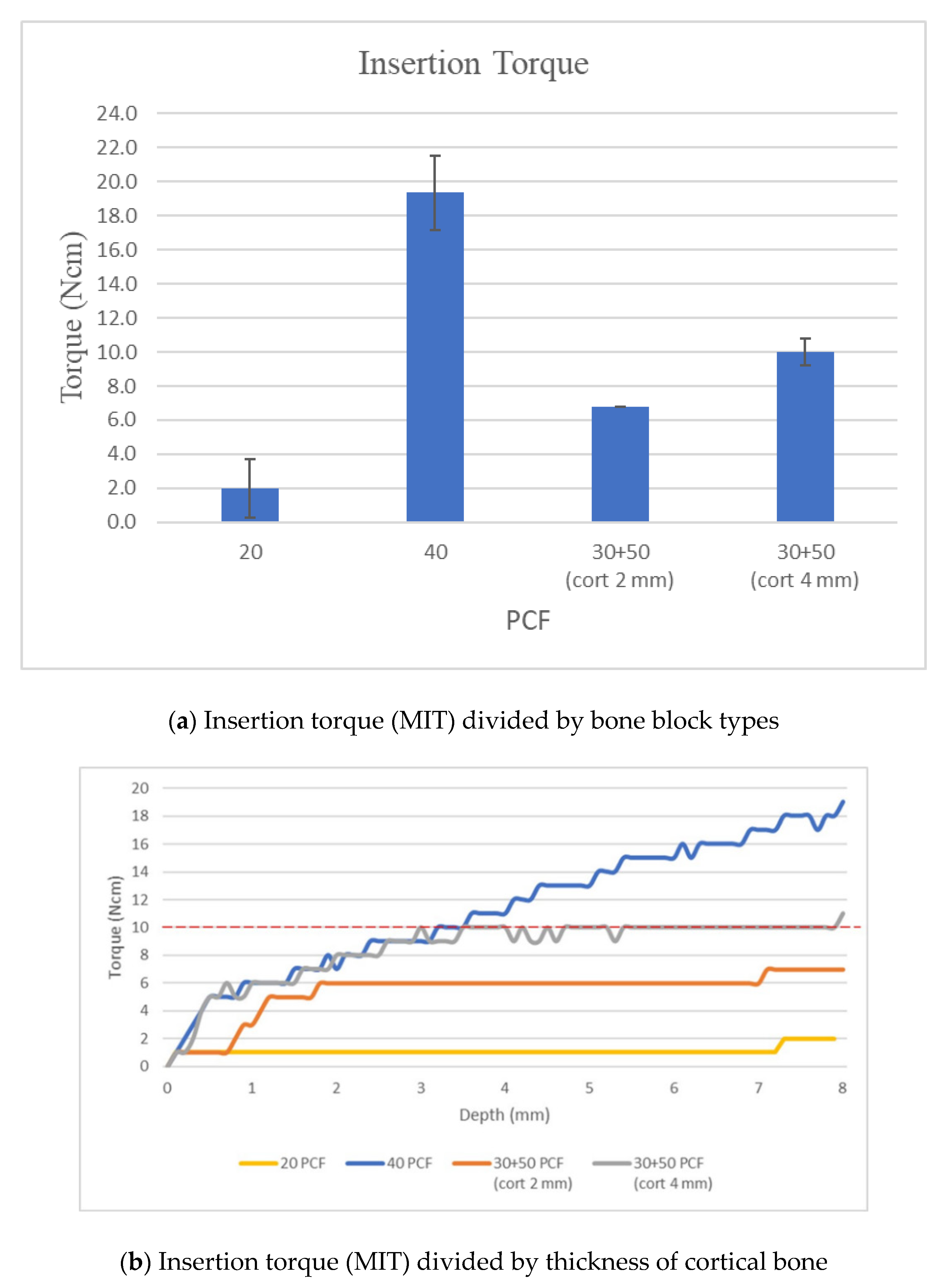
| Insertion Torque | ||||
|---|---|---|---|---|
| PCF | 20 | 40 | 30 + 50 (Cort 2 mm) | 30 + 50 (Cort 4 mm) |
| mean | 2.0 | 19.3 | 6.8 | 10.0 |
| sd | 0.8 | 1.5 | 0.5 | 0.8 |
Publisher’sNote: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marchi, A.; Camporesi, M.; Festa, M.; Salvatierra, L.; Izadi, S.; Farronato, G. Drilling Capability of Orthodontic Miniscrews: In Vitro Study. Dent. J. 2020, 8, 138. https://doi.org/10.3390/dj8040138
Marchi A, Camporesi M, Festa M, Salvatierra L, Izadi S, Farronato G. Drilling Capability of Orthodontic Miniscrews: In Vitro Study. Dentistry Journal. 2020; 8(4):138. https://doi.org/10.3390/dj8040138
Chicago/Turabian StyleMarchi, Alessandra, Matteo Camporesi, Maurizio Festa, Luis Salvatierra, Sara Izadi, and Giampietro Farronato. 2020. "Drilling Capability of Orthodontic Miniscrews: In Vitro Study" Dentistry Journal 8, no. 4: 138. https://doi.org/10.3390/dj8040138
APA StyleMarchi, A., Camporesi, M., Festa, M., Salvatierra, L., Izadi, S., & Farronato, G. (2020). Drilling Capability of Orthodontic Miniscrews: In Vitro Study. Dentistry Journal, 8(4), 138. https://doi.org/10.3390/dj8040138