Safety and Design Aspects of Powered Toothbrush—A Narrative Review



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. History
1.1. Ancient “Toothbrush”—The Chew Stick
1.2. The First Mass-Produced Modern Toothbrush
1.3. The Rise of Powered Toothbrush
2. Classification of Powered Toothbrushes
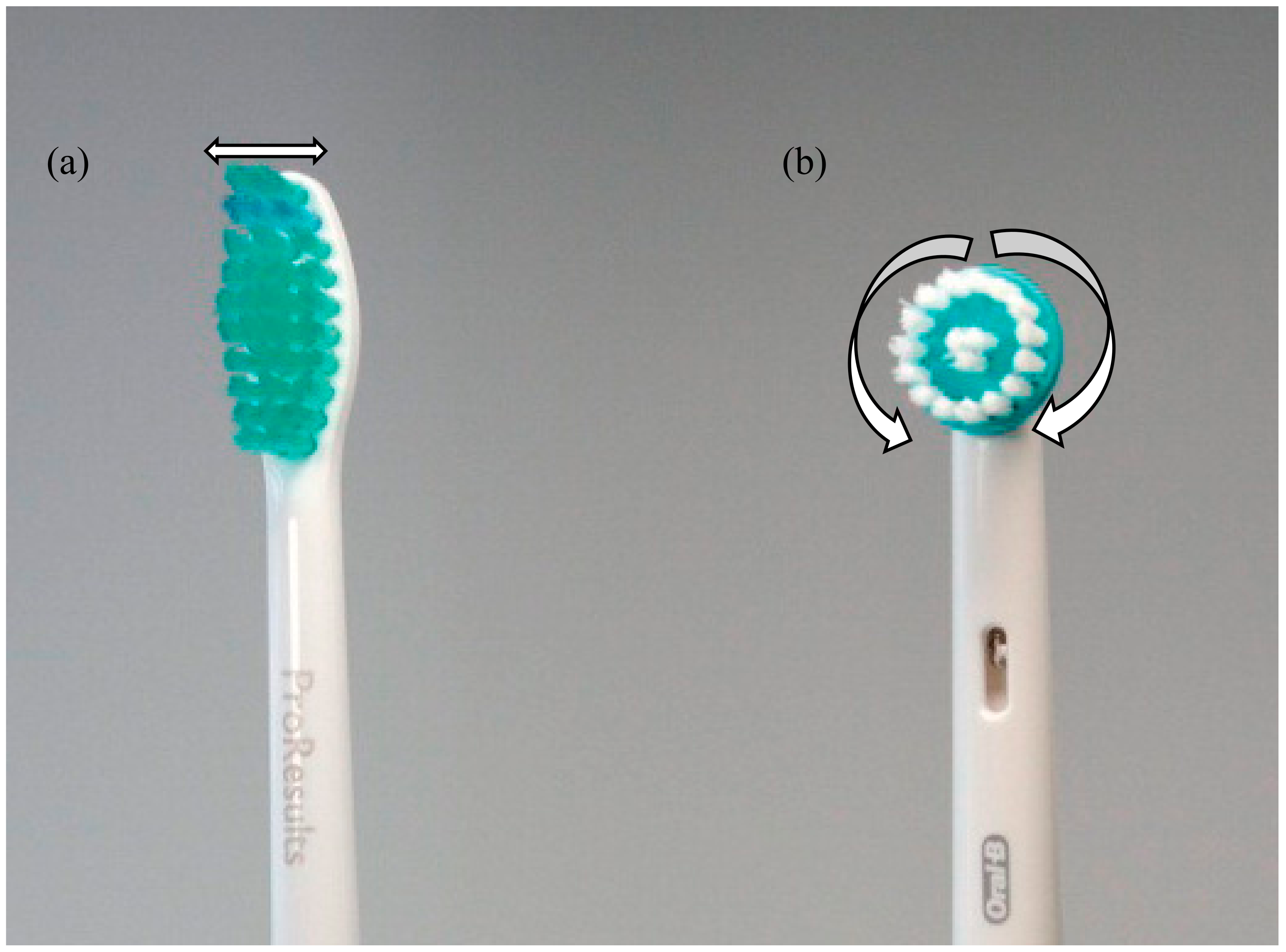
2.1. Type of Movement—Vibrational and Rotation-Oscillation Powered Toothbrushes
2.2. Speed of Movement—Sonic and Ultra-Sonic Powered Toothbrushes
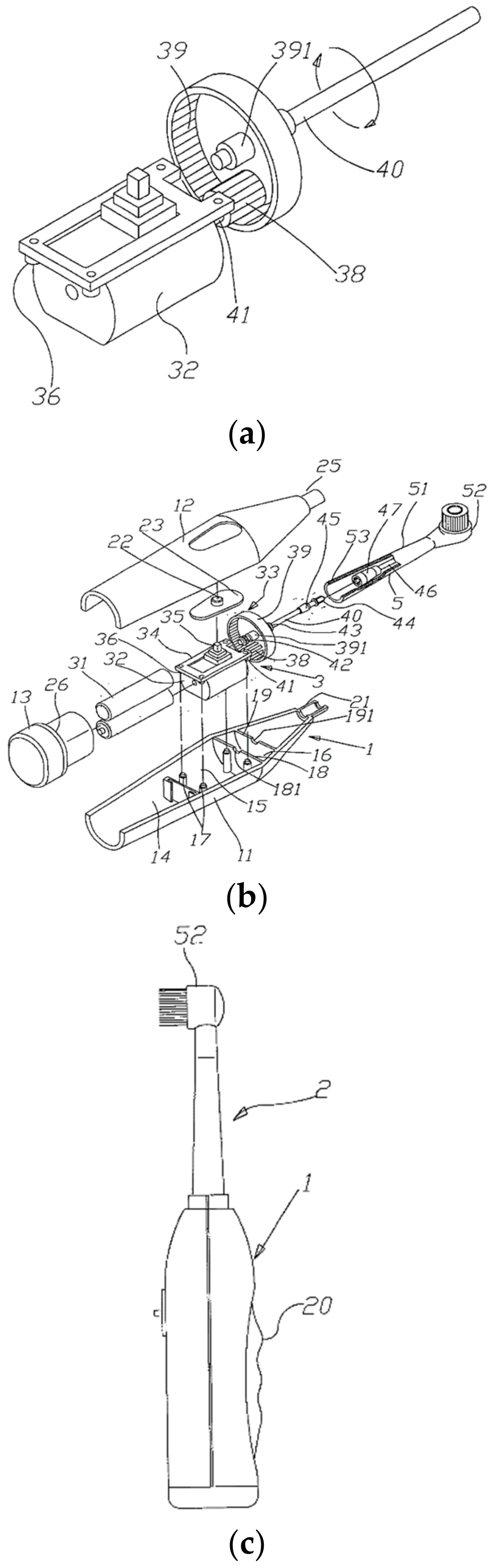
3. Mechanical Structure of a Rotation-Oscillation Powered Toothbrushes
3.1. The Power Transmission Device
3.2. The Brush Head
3.3. Switching On the Powered Toothbrush
3.4. Manufacturing the Powered Toothbrush
3.4.1. The Block Handle Case
3.4.2. The Brush Head
3.4.3. Final Stage of Production
4. Closer Look at the Brush Head
4.1. Brush Head Bristles
4.1.1. Bristle Lengths
4.1.2. Bristle Diameters
4.1.3. Bristle Materials
4.1.4. Bristle Stiffness
4.1.5. Bristle Colors
4.1.6. Other Bristles
Fluorinated Bristles
Low Friction Bristles
4.2. Brush Head Body
4.2.1. The Mechanical Structure
4.2.2. Materials of Brush Head Body
5. Powered Toothbrush vs. Manual Toothbrushes
5.1. Advantages of the Powered Brushes
5.1.1. Plaque Removal
Consequences of Plaque Accumulation
Efficacy of Powered Toothbrush
5.1.2. Dental Stain Removal
5.1.3. Maintenance of Peri-Implant Soft Tissues
5.1.4. Salivary Flow Stimulation
Xerostomia
Effect of Powered Toothbrush
5.2. Disadvantages of Powered Brushes
5.2.1. Potential Epileptic Seizures Inducer
5.2.2. Toothpaste Contamination
5.2.3. Effect of Load and Toothpaste
5.3. Safety Issues
5.3.1. The Spinbrush Issue
5.3.2. Implication of the Spinbrush Issue
6. Using the Powered Toothbrushes
6.1. Myth of Replacing Brush Heads
6.2. Brushing Force and Time
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Olmert, M. Milton’s Teeth Ovid’s Umbrella: Curiouser and Curiouser Adventures in History; Simon Schuster: New York, NY, USA, 1996. [Google Scholar]
- Sammons, R. Control of Dental Plaque; John Wiley Sons: Chichester, UK, 2003. [Google Scholar]
- Panati, C. Extraordinary Origins of Everyday Things; HarperCollins: New York, NY, USA, 2013; pp. 208–209. [Google Scholar]
- Yu, H.Y.; Qian, L.M.; Zheng, J. Dental Biotribology; Springer: New York, NY, USA, 2013. [Google Scholar]
- Kumar, J.V. Oral hygiene aids. In Textbook of Preventive and Community Dentistry, 2nd ed.; Elsevier: New Delhi/Haryana, India, 2011; pp. 412–413. [Google Scholar]
- Wisdom. Available online: https://wisdom-toothbrushes.com/contact-us/about-us/ (accessed on 3 August 2019).
- Wadsworth, H.N. Worth. U.S. Patents US18653A, 17 November 1857. [Google Scholar]
- Library of Congress, Everyday Mysteries, Who invented the toothbrush and when was it invented? Available online: https://www.loc.gov/everyday-mysteries/item/who-invented-the-toothbrush-and-when-was-it-invented/ (accessed on 31 August 2019).
- Van der Weijden, F.; Slot, D.E. The effectiveness of toothbrushing. Dent. Trib. 2012. Nov 2. Available online: https://www.dental-tribune.com/clinical/the-effectiveness-of-toothbrushing-2/ (accessed on 31 August 2019).
- Nylon, A. Petroleum Polymer. Available online: http://aoghs.org/oil-and-natural-gas-petroleum-products/petroleums-nylon-fiber/ (accessed on 1 August 2015).
- Broxodent (advertisement). J. Periotontol. 1964, 35, 101.
- Kweon, Y.J. Tapered Toothbrush Bristle and Toothbrush with Said Bristles, and Methods for Producing the Same. U.S. Patents US6090488A, 18 July 2000. [Google Scholar]
- Deacon, S.A.; Glenny, A.-M.; Deery, C.; Robinson, P.G.; Heanue, M.; Walmsley, A.D.; Shaw, W.C. Different powered toothbrushes for plaque control and gingival health. Cochrane Database Syst. Rev. 2010. [Google Scholar] [CrossRef] [PubMed]
- Panick, C. Power toothbrushes: A critical review. Int. J. Dent. Hyg. 2004, 2, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Erbe, C.; Jacobs, C.; Klukowska, M.; Timm, H.; Grender, J.; Wehrbein, H. A randomized clinical trial to evaluate the plaque removal efficacy of an oscillating-rotating toothbrush versus a sonic toothbrush in orthodontic patients using digital imaging analysis of the anterior dentition. Angle Orthodont. 2019, 89, 385–390. [Google Scholar] [CrossRef]
- Tan, C.M.; Tsoi, J.K.H.; Seneviratne, C.J.; Matinlinna, J.P. Evaluation of the Candida albicans removal and mechanical properties of denture acrylics cleaned by a low-cost powered toothbrush. J. Prosthodont. Res. 2014, 58, 243–251. [Google Scholar] [CrossRef]
- MacNeill, S.; Cobb, C.M.; Dey, A.; Glaros, A.G.; Walters, D.M. Sonic and mechanical toothbrushes: An in vitro study showing altered microbial surface structures but lack of effect on viability. J. Clin. Periodontol. 1998, 25, 988–993. [Google Scholar] [CrossRef]
- Mclnnes, C.; Engel, D.; Moncla, B.J.; Martin, R.W. Reduction in adherence of actinomyces viscosus after exposure to low-frequency acoustic energy. Oral Microbiol. Immunol. 1992, 7, 171–176. [Google Scholar] [CrossRef]
- Mclnnes, C.; Engel, D.; Martin, R.W. Fimbria damage and removal of adherent bacteria after exposure to acoustic energy. Oral Microbiol. Immunol. 1993, 8, 277–282. [Google Scholar] [CrossRef]
- Mclnnes, C.; Johnson, B.; Emling, R.C.; Yankell, S.L. Clinical and computer-assisted evaluations of the stain removal ability of the sonicare electronic toothbrush. J Clin. Dent. 1994, 5, 13–18. [Google Scholar]
- Wu-Yuan, C.D.; Anderson, R.D.; Mclnnes, C. Ability of the sonicare electronic toothbrush to generate dynamic fluid activity that removes bacteria. J. Clin. Dent. 1994, 5, 89–93. [Google Scholar]
- Johnson, B.D.; McInnes, C. Clinical evaluation of the efficacy and safety of a new sonic toothbrush. J. Periodontol. 1994, 65, 692–697. [Google Scholar] [CrossRef]
- Tritten, C.B.; Armitage, G.C. Comparison of a sonic and a manual toothbrush for efficacy in supragingival plaque removal and reduction of gingivitis. J. Clin. Periodontol. 1996, 23, 641–648. [Google Scholar] [CrossRef]
- Grossman, E.; Dembling, W.; Proskin, H.M. A comparative clinical investigation of the safety and efficacy of an oscillating/rotating electric toothbrush and a sonic toothbrush. J. Clin. Dent. 1995, 6, 108–112. [Google Scholar]
- Robinson, P.J.; Maddalozzo, D.; Breslin, S. A 6-month clinical comparison of the efficacy of the sonicare and the braun oral-b electric toothbrushes on improving periodontal health in adult periodontitis patients. J. Clin. Dent. 1997, 7, 4–9. [Google Scholar]
- O’Beirne, G.; Johnson, R.H.; Persson, G.R.; Spektor, M.D. Efficacy of a sonic toothbrush on inflammation and probing depth in adult periodontitis. J. Periodontol. 1996, 67, 900–908. [Google Scholar] [CrossRef]
- Blanco, V.L.; Cobb, C.M.; Williams, K.B.; Manch-Citron, J.N. In vitro effect of the sensonic™ toothbrush on treponema denticola. J. Clin. Periodontol. 1997, 24, 318-123. [Google Scholar] [CrossRef]
- Robrish, S.A.; Grove, S.B.; Bernstein, R.S.; Marucha, P.T.; Socransky, S.S.; Amdur, B. Effect of sonic treatment on pure cultures and aggregates of bacteria. J. Clin. Microbiol. 1976, 3, 474. [Google Scholar]
- Forgas-Brockmann, L.B.; Carter-Hanson, C.; Killoy, W.J. The effects of an ultrasonic toothbrush on plaque accumulation and gingival inflammation. J. Clin. Periodontol. 1998, 25, 375–379. [Google Scholar] [CrossRef]
- Terezhalmy, G.T.; Gagliardi, V.B.; Rybicki, L.A.; Kauffman, M.J. Clinical evaluation of the efficacy and safety of the ultrasonex ultrasonic toothbrush: A 30-day study. Compend. Contin. Educ. Dent. 1994, 15, 866–874. [Google Scholar]
- Li, M.-K. Electric Toothbrush Structure. U.S. Patents US20020174498A1, 2002. [Google Scholar]
- Chiang, C.C. Block Head Structure of Electric Toothbrush. U.S. Patents US6851150B2, 8 Feb 2005. [Google Scholar]
- Love, J. How a toothbrush is made. Available online: https://www.electricteeth.co.uk/toothbrush-manufacture/ (accessed on 30 November 2019).
- Oral-B. Type of toothbrush bristles. Available online: https://www.oralb.com.au/en-au/oral-care-topics/types-of-toothbrush-bristles (accessed on 19 July 2015).
- Mann, R.F. Adjustable Bristle Length Toothbrush. U.S. Patents US5142726A, 1 September 1992. [Google Scholar]
- Tcholakov, S.I. Adjustable Bristle Toothbrush Apparatus. U.S. Patents US7743452B1, 29 June 2010. [Google Scholar]
- Burge, D.E. Toothbrush. U.S. Patents US3410284A, 24 March 1966. [Google Scholar]
- DuPont. Dupont Tynex® 612 Nylon Filament. Available online: http://www2.dupont.com/Filaments/en_US/assets/downloads/Toothbrush/DuPont%20Tynex%20612.pdf (accessed on 1 August 2015).
- Nylon 6/12 (pa)—Polyamide 6/12. Available online: http://www.rtpcompany.com/products/product-guide/nylon-612-pa-polyamide-612/ (accessed on 1 August 2015).
- Why Do Dentists Recommend Soft Toothbrushes? Available online: http://www.canadabaydental.com.au/why-do-dentists-recommend-soft-toothbrushes/ (accessed on 19 July 2015).
- Breuer, M.M.; Hanak, J.A. Novel Brush Filaments. U.S. Patents US4802255A, 7 February 1989. [Google Scholar]
- Tseng, M.M.; Philbrook, C.M. Color Changing Matrix as Wear Indicator. U.S. Patents US7338664B2, 4 March 2008. [Google Scholar]
- Kent, S. Toothbrush with Slow Release of Disinfectant and Antibacterial Agents and Method of Manufacturing the Same. U.S. Patents US5061106A, 29 October 1991. [Google Scholar]
- Cook, C.M.; Moser, C.E. Fluorinated Toothbrush Bristle and Method of Making Same. U.S. Patents US3076218A, 5 February 1963. [Google Scholar]
- Brezler, R.A.; Loudin, S.E.; Nelson, C.F.; Su, K.Y.B. Low Friction Toothbrush. U.S. Patents US6871374B2, 29 March 2005. [Google Scholar]
- Gueret, J.L.H. Brush for Applying a Liquid Product as a Layer on A Substrate. U.S. Patents US5462798A, 31 October 1995. [Google Scholar]
- Esmaeili, A.; Pourbabaee, A.A.; Alikhani, H.A.; Shabani, F.; Esmaeili, E. Biodegradation of low-density polyethylene (ldpe) by mixed culture of lysinibacillus xylanilyticus and aspergillus niger in soil. PLoS ONE 2013, 8, e71720. [Google Scholar] [CrossRef] [PubMed]
- Polymer Thermoplastics; British Plastics Federation: London, UK, 2015.
- Karian, H.G. Handbook of Polypropylene and Polypropylene Composites, 2nd ed.; CRC Press: New York, NY, USA, 2003. [Google Scholar]
- Polypropylene (pp); British Plastics Federation: London, UK, 2015.
- Darby, M.L.; Walsh, M.M. Dental Hygiene Theory and Practice, 4th ed.; Elsevier: St Louis, MO, USA, 2015. [Google Scholar]
- Summitt, J.B.; Robbins, J.W.; Hilton, T.J.; Schwartz, R.S. Fundamentals of Operative Dentistry; Publisher House: Hanover Park, IL, USA, 2006. [Google Scholar]
- Wolf, H.; Hassell, T. Color Atlas of Dental Hygiene; Thieme New York: New York, NY, USA, 2006. [Google Scholar]
- Chandrasoma, P.; Taylor, C.R. Concise Pathology, 3rd ed.; McGraw-Hill: New York, NY, USA, 2005. [Google Scholar]
- Noble, S.L. Clinical Textbook of Dental Hygiene and Therapy, 2nd ed.; Wiley-Blackwell: West Sussex, UK, 2012. [Google Scholar]
- Rateitschak, K.H.; Rateitschak, E.M.; Wolf, H.F.; Hassell, T.M. Color Atlas of Periodontology; Thieme Inc: New York, NY, USA, 1985. [Google Scholar]
- Tonetti, M.S.; Eickholz, P.; Loos, B.G.; Papapanou, P.; Velden, U.; Armitage, G.; Bouchard, P.; Deinzer, R.; Dietrich, T.; Hughes, F.; et al. Principles in prevention of periodontal diseases. J. Clin. Periodontol. 2015, 42, S5–S11. [Google Scholar] [CrossRef] [PubMed]
- Verkaik, M.J.; Busscher, H.J.; Jager, D.; Slomp, A.M.; Abbas, F.; van der Mei, H.C. Efficacy of natural antimicrobials in toothpaste formulations against oral biofilms in vitro. J. Dent. 2011, 39, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Attin, T.; Hornecker, E. Tooth brushing and oral health: How frequently and when should tooth brushing be performed? Oral Health Prev. Dent. 2005, 3, 135–140. [Google Scholar]
- Walmsley, A.D. The powered toothbrush: A review. Br. Dent. J. 1997, 182, 209–218. [Google Scholar] [CrossRef] [PubMed]
- McCracken, G.I.; Stacey, F.K.; Heasman, L. A comparative study of two powered toothbrushes and one manual toothbrush in young adults. J. Clin. Dent. 2001, 12, 7–10. [Google Scholar]
- Dentino, A.R.; Derderian, G.; Wolf, M. Six-month comparison of powered versus manual toothbrushing for safety and efficacy in the absence of professional instruction in mechanical plaque control. J. Periodontol. 2002, 73, 770–778. [Google Scholar] [CrossRef]
- Ruhlman, C.D.; Bartizek, R.D.; Biesbrock, A.R. Plaque removal efficacy of a battery-operated toothbrush compared to a manual toothbrush. Am. J. Dent. 2001, 14, 191–194. [Google Scholar]
- Heins, P.; Bartizek, R.; Walters, P.; Biesbrock, A. Plaque removal efficacy of a battery-operated powered toothbrush compared to two control manual toothbrushes in single use studies. Am. J. Dent. 2002, 15, 28A–32A. [Google Scholar]
- Van der Weijden, G.A.; Timmerman, M.F.; Reijerse, E.; Snoek, C.M.; Van der Velden, U. Comparison of an oscillating/rotating electric toothbrush and a sonic toothbrush in plaque-removing ability. A professional toothbrushing and supervised brushing study. J. Clin. Periodontol. 1996, 23, 407–411. [Google Scholar] [CrossRef]
- Heanue, M.; Deacon, S.A.; Deery, C. Manual versus powered toothbrushing for oral health (cochrane review). Cochrane Database Syst. Res. 2003. [Google Scholar] [CrossRef]
- Guile, E.E. One type of powered toothbrush may be more effective than others in controlling plaque and gingivitis. J. Evid. Based Dent. Pract. 2012, 12, 65–68. [Google Scholar] [CrossRef]
- Grossman, E.; Cronin, M.; Dembling, W.; Proskin, H. A comparative clinical study of extrinsic tooth stain removal with two electric toothbrushes (braun d7 and d9) and a manual brush. Am. J. Dent. 1996, 9, S25–S29. [Google Scholar]
- Moran, J.; Addy, M.; Newcombe, R.G. A comparative study of stain removal with two electric toothbrushes and a manual brush. J. Clin. Dent. 1995, 6, 188–193. [Google Scholar]
- Sharma, C.N.; Galustians, H.J.; Qaqish, J.; Cugini, G.; Warren, P.R. A comparison of the braun oral-b 3d plaque remover and the sonicare plus electric toothbrush in removing naturally occurring extrinsic staining. Am. J. Dent. 2000, 13, 17–20. [Google Scholar]
- Moran, J.; Addy, M.; Courtney, M.; Smith, S.; Newcombe, R.G. A clinical study to assess the ability of a powered toothbrush to remove chlorhexidine/tea dental stain. J. Clin. Periodontol. 2004, 31, 95–98. [Google Scholar] [CrossRef]
- Truhlar, R.S.; Morris, H.F.; Ochi, S. The efficacy of a counter-rotational powered toothbrush in the maintenance of endosseous dental implants. J. Am. Dent. Assoc. 2000, 131, 101–107. [Google Scholar] [CrossRef]
- Papas, A.; Singh, M.; Harrington, D.; Rodriguez, S.; Ortblad, K.; Jager, M.; Nunn, M. Stimulation of salivary flow with a powered toothbrush in a xerostomic population. Spec. Care Dent. 2006, 26, 241–246. [Google Scholar] [CrossRef]
- Dawes, C. How much saliva is enough for avoidance of xerostomia? Caries Res. 2004, 38, 236–240. [Google Scholar] [CrossRef]
- Duplay, D. Physicians Desk Reference, 59th ed.; Thomson: New York, NY, USA, 2005. [Google Scholar]
- Talal, N.; Quinn, J.H.; Daniels, T.E. The clinical effects of electrostimulation on salivary function of sjogren’s syndrome patients. A placebo controlled study. Rheumatol. Int. 1992, 12, 43–45. [Google Scholar] [CrossRef]
- Papas, A.S.; Hecht, R.; Russell, D.; Stack, R.; Smolyar, R.; Harrington, D.; Van, H.J.; Lindstrom, P.; Papas, A.N. Effect of xerostomic medications, especially psychiatric, on oral health. Am. Soc. Clin. Pathol. 1998, 77, 280. [Google Scholar]
- Dreifuss, F.E. Classification of reflex epilepsies and reflex seizures. Adv. Neurol. 1998, 75, 5–13. [Google Scholar]
- Fisher, R.S.; Harding, G.; Erba, G.; Barkley, G.L.; Wilkins, A. Photic-and pattern-induced seizures: A review for the epilepsy foundation of america working group. Epilepsia 2005, 46, 1426–1441. [Google Scholar] [CrossRef]
- Holmes, G.; Blair, S.; Eisenberg, E.; Scheebaum, R.; Margraf, J.; Zimmerman, A. Tooth-brushing-induced epilepsy. Epilepsia 1982, 23, 657–661. [Google Scholar] [CrossRef]
- O’Brien, T.J.; Hogan, R.E.; Sedal, L.; Murrie, V.; Cook, M.J. Toothbrushing epilepsy: A report of a case with structural and functional imaging and electrophysiology demonstrating a right frontal focus. Epilepsia 1996, 37, 694–697. [Google Scholar] [CrossRef]
- Haytac, M.C.; Aslan, K.; Ozcelik, O.; Bozdemir, H. Epileptic seizures triggered by the use of a powered toothbrush. Seizure Eur. J. Epilepsy 2008, 17, 288–291. [Google Scholar] [CrossRef]
- Koutroumanidis, M.; Pearce, R.; Sadoh, D.R.; Panayiotopoulos, C.P. Tooth brushing-induced seizures: A case report. Epilepsia 2001, 42, 686–688. [Google Scholar] [CrossRef]
- Kanemoto, K.; Watanabe, Y.; Tsuji, T.; Fukami, M.; Kawasaki, J. Rub epilepsy: A somatosensory evoked reflex epilepsy induced by prolonged cutaneous stimulation. J. Neurol. Neurosurg. Psychiatry 2001, 70, 541–543. [Google Scholar] [CrossRef][Green Version]
- Colquitt, P.J. Do powered toothbrushes contaminate toothpaste with metals? Sci. Total Environ. 2002, 289, 25–32. [Google Scholar] [CrossRef]
- Johansen, J.D.; Menné, T.; Christophersen, J.; Kaaber, K.; Veien, N. Changes in the pattern of sensitization to com-mon contact allergens in denmark between 1985–86 and 1997–98, with a special view of preventative strategies. Br. J. Dermatol. 2000, 142, 490–495. [Google Scholar] [CrossRef]
- Lim, S.W.; Goh, C.L. Epidemiology of eczematous cheilitis at a tertiary dermatological referral centre in singapore. Contact Dermat. 2000, 43, 222–326. [Google Scholar] [CrossRef] [PubMed]
- Powell, J.J.; Harvey, R.S.J.; Ashwood, P.; Wolstencroft, R.; Gershwin, M.E.; Thompson, R.P.H. Immune potentiation of ultrafine dietary particles in normal subjects and patients with inflammatory bowel disease. J. Autoimmune Dis. 2000, 14, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Lomer, M.C.; Harvey, R.S.; Evans, S.M.; Thompson, R.P.; Powell, J.J. Efficacy and tolerability of a low microparticle diet in a double blind, randomised, pilot study in crohn’s disease. Eur. J. Gastroenterol. Hepatol. 2001, 13, 101–106. [Google Scholar] [CrossRef]
- Taniguchi, A.; Cakmak, M. The effect of titanium dioxide particles on the deformation behaviour and orientation development in pet films, antec 2000 conference proceedings. Soc. Plast. Eng. 2000, 1786–1790. [Google Scholar]
- Lea, S.C.; Khan, A.; Patanwala, H.S.; Landini, G.; Walmsley, A.D. The effects of load and toothpaste on powered toothbrush vibrations. J. Dent. 2007, 35, 350–354. [Google Scholar] [CrossRef]
- Deery, C.; Heanue, M.; Deacon, S.; Robinson, P.G.; Walmsley, A.D.; Worthington, H.; Shaw, W.; Glenny, A.-M. The effectiveness of manual versus powered toothbrushes for dental health: A systematic review. J. Dent. 2004, 32, 197–211. [Google Scholar] [CrossRef]
- Van Der Weijden, F.A.; Campbell, S.L.; Dörfer, C.E.; González-Cabezas, C.; Slot, D.E. Safety of oscillating-rotating powered brushes compared to manual toothbrushes: A systematic review. J. Periodontol. 2011, 82, 5–24. [Google Scholar] [CrossRef]
- Toothbrush can chip teeth and cause choking. 2012. Available online: https://www.fda.gov/ForConsumers/ConsumerUpdates/ucm291790.htm (accessed on 31 July 2015).
- Hogan, L.M.E.; Daly, C.G.; Curtis, B.H. Comparison of new and 3-month-old brush heads in the removal of plaque using a powered toothbrush. J. Clin. Periodontol. 2007, 34, 130–136. [Google Scholar] [CrossRef]
- Sforza, N.; Rimondini, L.; di Menna, F.; Camorali, C. Plaque removal by worn toothbrush. J. Clin. Periodontol. 2000, 27, 212–216. [Google Scholar] [CrossRef]
- Tan, E.; Daly, C. Comparison of new and 3-month-old toothbrushes in plaque removal. J. Clin. Periodontol. 2002, 29, 645–650. [Google Scholar] [CrossRef]
- Mccracken, G.I.; Janssen, J.; Swan, M.; Steen, N.; De Jager, M.; Heasman, P.A. Effect of brushing force and time on plaque removal using a powered toothbrush. J. Clin. Periodontol. 2003, 30, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, B.F.; Hohout, F.J.; Lainson, P.A.; Heckert, A. Duration of toothbrushing for effective plaque control. Quintessence Int. 1986, 17, 361–365. [Google Scholar] [PubMed]
- Dahl, L.O.; Muhler, J.C. Oral hygiene habits of young adults. J. Periodontol. 1955, 26, 43–46. [Google Scholar] [CrossRef]
- Pinkham, J.R. Oral hygiene in children: Relationship to age and brushing time. J. Prev. Dent. 1975, 2, 28–31. [Google Scholar]
- Van der Weijden, G.A.; Timmerman, M.F.; Nijboer, A.; Lie, M.A.; Van der Velden, U. A comparative study of electric toothbrushes for the effectiveness of plaque removal in relation to toothbrushing duration. J. Clin. Periodontol. 1993, 20, 476–481. [Google Scholar] [CrossRef]
- Van der Weijden, G.A.; Timmerman, M.F.; Reijerse, E.; Snoek, C.M.; Van der Velden, U. Toothbrushing force in relation to plaque removal. J. Clin. Periodontol. 1996, 23, 724–729. [Google Scholar] [CrossRef]
- Van der Weijden, G.A.; Timmerman, M.F.; Snoek, I.M.; Reijerse, E.; Van der Velden, U. Toothbrushing duration and plaque removing efficacy of electric toothbrushes. Am. J. Dent. 1996, 9, S31–S36. [Google Scholar]
- Van der Weijden, G.A.; Timmerman, M.F.; Danser, M.M.; Van der Velden, U. Relationship between the plaque removal efficacy of a manual toothbrush and brushing force. J. Clin. Periodontol. 1998, 25, 413–416. [Google Scholar] [CrossRef]




© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ng, C.; Tsoi, J.K.H.; Lo, E.C.M.; Matinlinna, J.P. Safety and Design Aspects of Powered Toothbrush—A Narrative Review. Dent. J. 2020, 8, 15. https://doi.org/10.3390/dj8010015
Ng C, Tsoi JKH, Lo ECM, Matinlinna JP. Safety and Design Aspects of Powered Toothbrush—A Narrative Review. Dentistry Journal. 2020; 8(1):15. https://doi.org/10.3390/dj8010015
Chicago/Turabian StyleNg, Clarence, James Kit Hon Tsoi, Edward C. M. Lo, and Jukka P. Matinlinna. 2020. "Safety and Design Aspects of Powered Toothbrush—A Narrative Review" Dentistry Journal 8, no. 1: 15. https://doi.org/10.3390/dj8010015
APA StyleNg, C., Tsoi, J. K. H., Lo, E. C. M., & Matinlinna, J. P. (2020). Safety and Design Aspects of Powered Toothbrush—A Narrative Review. Dentistry Journal, 8(1), 15. https://doi.org/10.3390/dj8010015