Effects of High Frequency Acceleration Device on Aligner Treatment—A Pilot Study

Abstract
1. Introduction
2. Materials and Methods
2.1. Statistical Analysis
2.2. Ethical Considerations
3. Results
3.1. Crowding
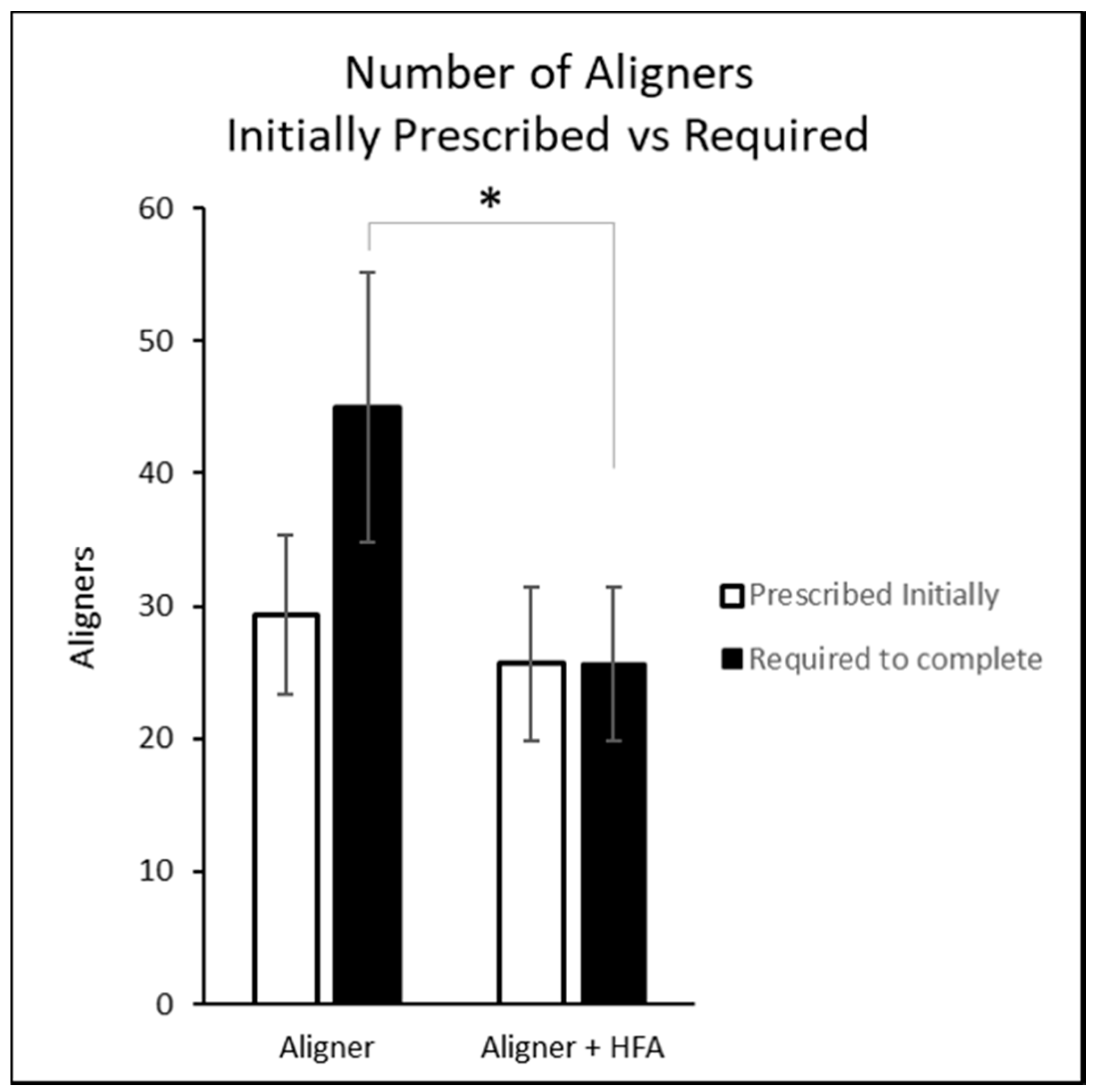
3.2. Aligner Counts
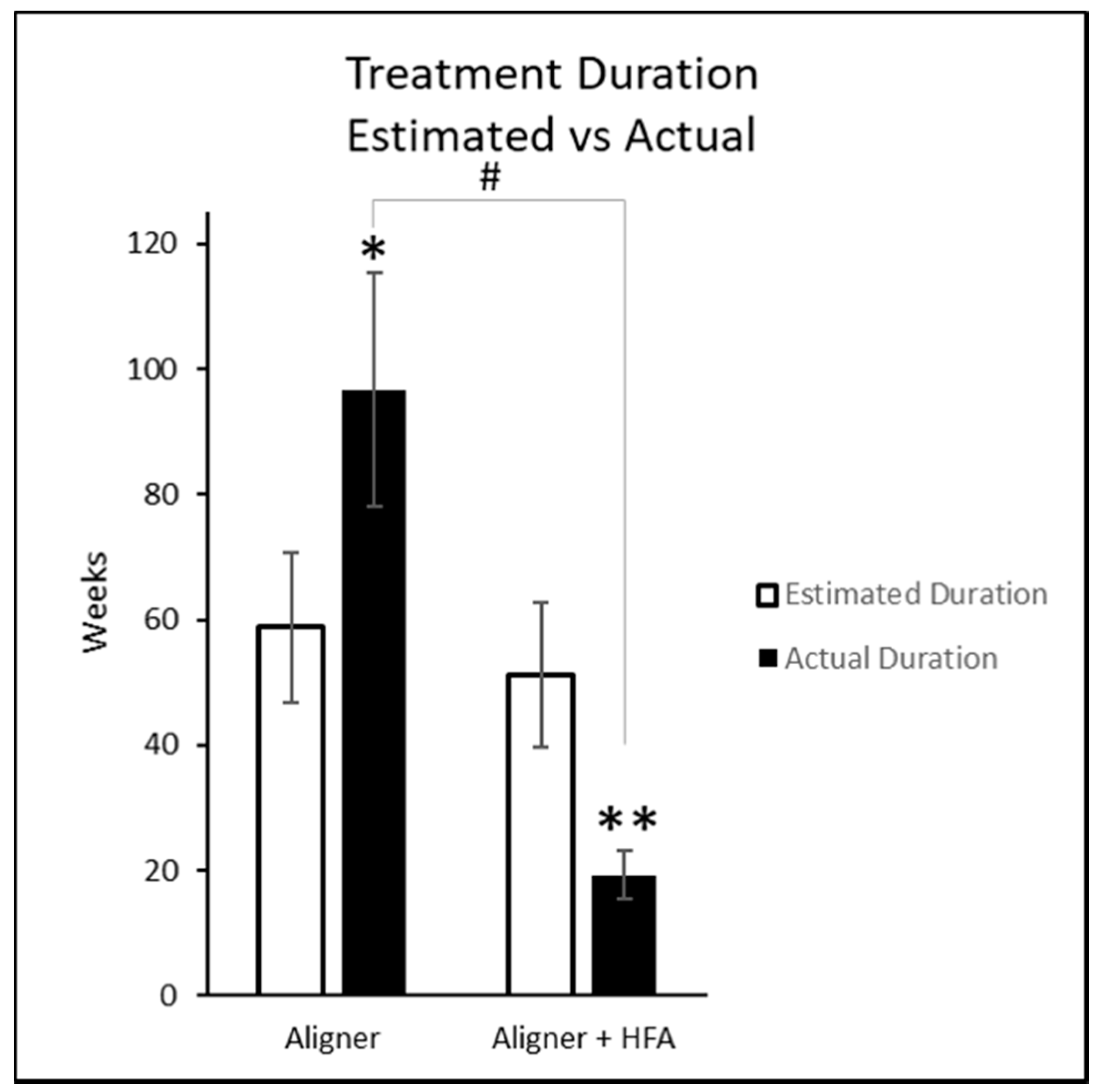
3.3. Aligner Change Interval and Treatment Duration
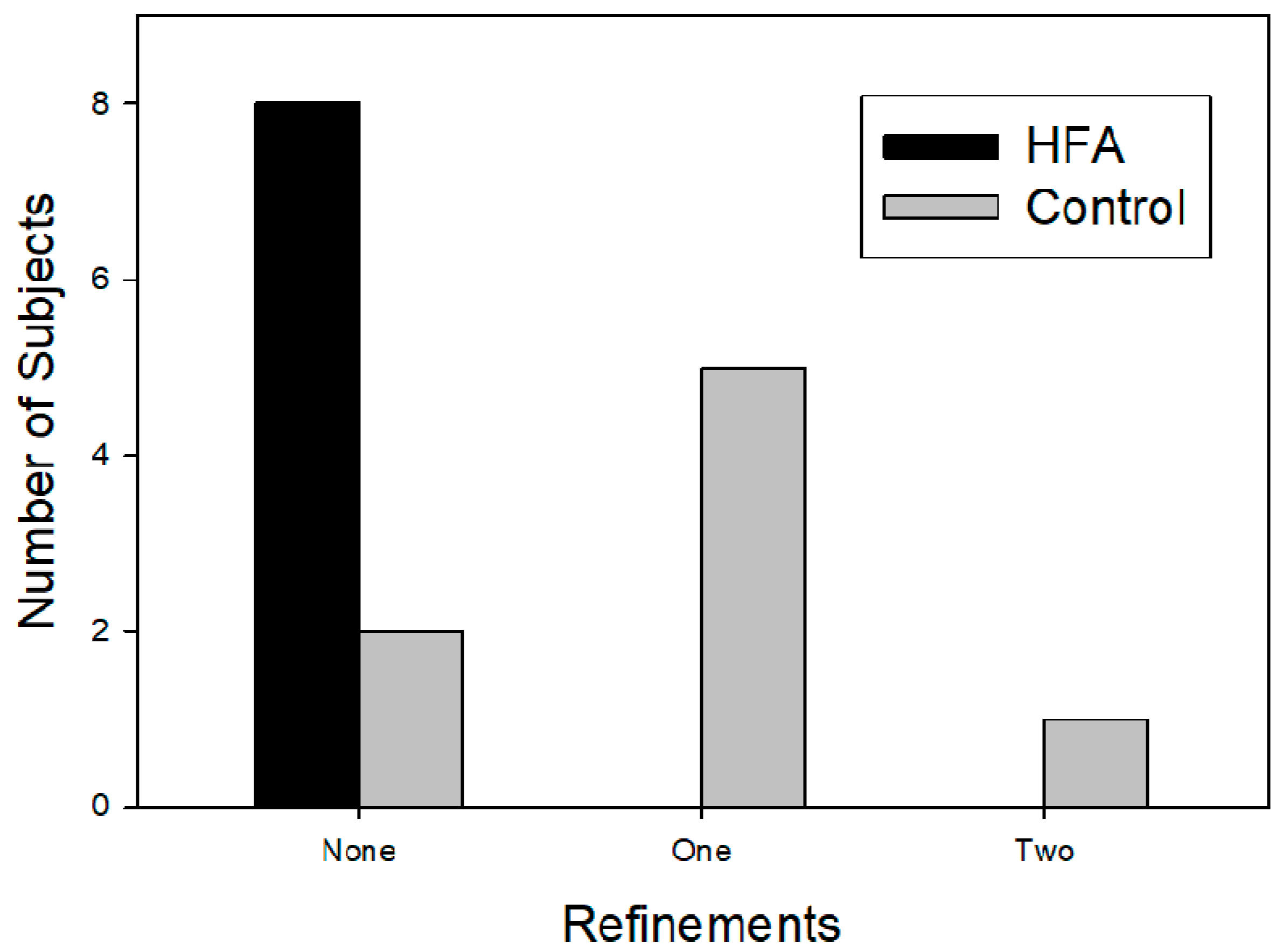
3.4. Case Refinement
3.5. Potential Sex Bias
4. Discussion
5. Conclusions
- In the present investigation, accelerated tooth movement was achieved using adjunctive HFA treatment with aligner therapy.
- Use of an HFA device allowed 66% faster aligner exchanges than control.
- HFA subjects required significantly fewer aligners to complete treatment than controls.
- HFA subjects required significantly fewer refinements than control subjects.
Conflicts of Interest
References
- Woodhouse, N.; DiBiase, A.; Johnson, N.; Slipper, C.; Grant, J.; Alsaleh, M.; Donaldson, A.; Cobourne, M. Supplemental Vibrational Force during Orthodontic Alignment: A Randomized Trial. J. Dent. Res. 2015, 94, 682–689. [Google Scholar] [CrossRef] [PubMed]
- Alikhani, M.; Khoo, E.; Alyami, M.; Raptis, M.; Salgueiro, J.; Oliveira, S.; Boskey, A.; Teixeira, C. Osteogenic Effect of High-frequency Acceleration on Alveolar Bone. J. Dent. Res. 2012, 91, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Yadav, S.; Dobie, T.; Assefnia, A.; Gupta, H.; Kalajzic, Z.; Nanda, R. Effect of low-frequency mechanical vibration on orthodontic tooth movement. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 440–449. [Google Scholar] [CrossRef] [PubMed]
- Leethanakul, C.; Suamphan, S.; Jitpukdeebodintra, S.; Thongudomporn, U.; Charoemratrote, C. Vibratory stimulation increases interleukin-1 beta secretion during orthodontic tooth movement. Angle Orthod. 2015, 86, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Hsu, H.; Li, X.; Xian, C. Effects of Frequency and Acceleration Amplitude on Osteoblast Mechanical Vibration Responses: A Finite Element Study. BioMed Res. Int. 2016, 2016, 2735091. [Google Scholar] [CrossRef] [PubMed]
- Brezniak, N. The Clear Plastic Appliance. Angle Orthod. 2008, 78, 381–382. [Google Scholar] [CrossRef]
- Fujiyama, K.; Honjo, T.; Suzuki, M.; Matsuoka, S.; Deguchi, T. Analysis of pain level in cases treated with Invisalign aligner: Comparison with fixed edgewise appliance therapy. Prog. Orthod. 2014, 15, 64. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, L.; Arreghini, A.; Ramina, F.; Huanca Ghislanzoni, L.; Siciliani, G. Predictability of orthodontic movement with orthodontic aligners: A retrospective study. Prog. Orthod. 2017, 18, 35. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Oh, H.; Chambers, D.W.; Baumrind, S.; Xu, T. Validity of the American Board of Orthodontics Discrepancy Index and the Peer Assessment Rating Index for comprehensive evaluation of malocclusion severity. Orthod. Craniofac. Res. 2017, 20, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Jyothikiran, H.; Shanthara, J.R.; Subbiah, P.; Thomas, M. Craniofacial imaging in orthodontics—Past present and future. Int. J. Orthod. 2014, 25, 21–26. [Google Scholar]
- Nahas, A.Z.; Samara, S.A.; Rastegar-Lari, T.A. Decrowding of lower anterior segment with and without photobiomodulation: A single center, randomized clinical trial. Lasers Med. Sci. 2017, 32, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Johansson, K.; Lundström, F. Orthodontic treatment efficiency with self-ligating and conventional edgewise twin brackets: A prospective randomized clinical trial. Angle Orthod. 2012, 82, 929–934. [Google Scholar] [CrossRef] [PubMed]
- Bakathir, M.A.; Hassan, A.H.; Bahammam, M.A. Piezocision as an adjunct to orthodontic treatment of unilateral posterior crossbite. Saudi Med. J. 2017, 38, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Sfondrini, M.F.; Xheka, E.; Scribante, A.; Gandini, P.; Sfondrini, G. Reconditioning of self-ligating brackets. Angle Orthod. 2012, 82, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Hassan, A.H.; AlGhamdi, A.T.; Al-Fraidi, A.A.; Al-Hubail, A.; Hajrassy, M.K. Unilateral cross bite treated by corticotomy-assisted expansion: Two case reports. Head Face Med. 2010, 6, 6. [Google Scholar] [CrossRef] [PubMed]
- Brignardello-Petersen, R. Low-quality evidence suggesting benefits of vibration on distalization of canines during orthodontic treatment. J. Am. Dent. Assoc. 2018, 149, e89. [Google Scholar] [CrossRef] [PubMed]
- Alikhani, M.; Alansari, S.; Hamidaddin, M.A.; Sangsuwon, C.; Alyami, B.; Thirumoorthy, S.N.; Oliveira, S.M.; Nervina, J.M.; Teixeira, C.C. Vibration paradox in orthodontics: Anabolic and catabolic effects. PLoS ONE 2018, 13, e0196540. [Google Scholar] [CrossRef] [PubMed]
- Parrish, L.; Roberts, W.; Maupome, G.; Stewart, K.; Bandy, R.; Kula, K. The relationship between the ABO discrepancy index and treatment duration in a graduate orthodontic clinic. Angle Orthod. 2011, 81, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Boyd, R.; Miller, R.; Vlaskalic, V. The Invisalign System in Adult Orthodontics—Mild Crowding and Space Closure Cases. J. Clin. Orthod. 2000, 34, 203–212. [Google Scholar]
- Garrett, J. Effect of Reducing the Incremental Distance of Tooth Movement per Aligner While Maintaining the Overall Rate of Movement on Self-Reported Discomfort in Invisalign Patients. Ph.D. Thesis, Saint Louis University, St. Louis, MO, USA, 2012. [Google Scholar]
- Simon, M.; Keilig, L.; Schwarze, J.; Jung, B.; Bourauel, C. Treatment outcome and efficacy of an aligner technique—Regarding incisor torque, premolar derotation and molar distalization. BMC Oral Health 2014, 14, 68. [Google Scholar] [CrossRef] [PubMed]
- English, J.D.; Akyalcin, S.; Peltomaki, T.; Litschel, K. Mosby’s Orthodontic Review; Elsevier Health Sciences: Amsterdam, The Netherlands, 2014; pp. 157–159. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| (a) Age 14-45 (Male or Female) at initial visit. | (a) Subjects with caries present at time of treatment. |
| (b) Class I. | (b) Chronic NSAID, or steroid therapy. |
| (c) Crowding mild to moderate (3–5 mm). | (c) Bisphosphonate Therapy. |
| (d) Completed aligner series with Smarttrack aligner material. | (d) Pregnancy. |
| (e) Post treatment digital Vivera retainer scan. |
| Clinical Measures | Aligner | Aligner + HFA | p Value |
|---|---|---|---|
| Baseline ABO Discrepancy Index | 16.13 | 12.25 | 0.536 |
| SD | 14.32 | 9.63 | |
| Baseline Crowding—Upper | 0.95 mm | 0.74 mm | 0.412 |
| SD | 4.45 mm | 3.47 mm | |
| Baseline Crowding—Lower | 0.6 mm | 1.86 mm | 0.332 |
| SD | 2.24 mm | 2.76 mm | |
| Number of Aligners Prescribed Initially | 29.38 | 25.63 | 0.224 |
| SD | 6.00 | 5.78 | |
| Estimated Treatment Duration in Weeks | 58.75 | 51.25 | 0.224 |
| SD | 12.0 | 11.56 | |
| Aligner Exchange Rate Prescribed (days) | 14 | 14 | 1.0 |
| SD | 0 | 0 | |
| Aligner Exchange Rate Actual (days) | 14 | 4.75 | 0.001 |
| SD | 0 | 0.70 | |
| Number of Aligners Required to complete | 45 | 25.63 | 0.001 |
| SD | 10.18 | 5.78 | |
| Actual Treatment Duration in Weeks | 96.75 | 19.25 | 0.005 |
| SD | 18.76 | 3.88 | |
| Case Refinements | 7 | 0 | 0.0001 |
| % | 87.5 | 0 |
© 2018 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shipley, T.S. Effects of High Frequency Acceleration Device on Aligner Treatment—A Pilot Study. Dent. J. 2018, 6, 32. https://doi.org/10.3390/dj6030032
Shipley TS. Effects of High Frequency Acceleration Device on Aligner Treatment—A Pilot Study. Dentistry Journal. 2018; 6(3):32. https://doi.org/10.3390/dj6030032
Chicago/Turabian StyleShipley, Thomas S. 2018. "Effects of High Frequency Acceleration Device on Aligner Treatment—A Pilot Study" Dentistry Journal 6, no. 3: 32. https://doi.org/10.3390/dj6030032
APA StyleShipley, T. S. (2018). Effects of High Frequency Acceleration Device on Aligner Treatment—A Pilot Study. Dentistry Journal, 6(3), 32. https://doi.org/10.3390/dj6030032