
New Direct Oral Anticoagulants (DOAC) and Their Use Today

Abstract
:1. Background
2. Nomenclature of Oral Anticoagulants
3. Pharmacokinetic Profiles of DOAC
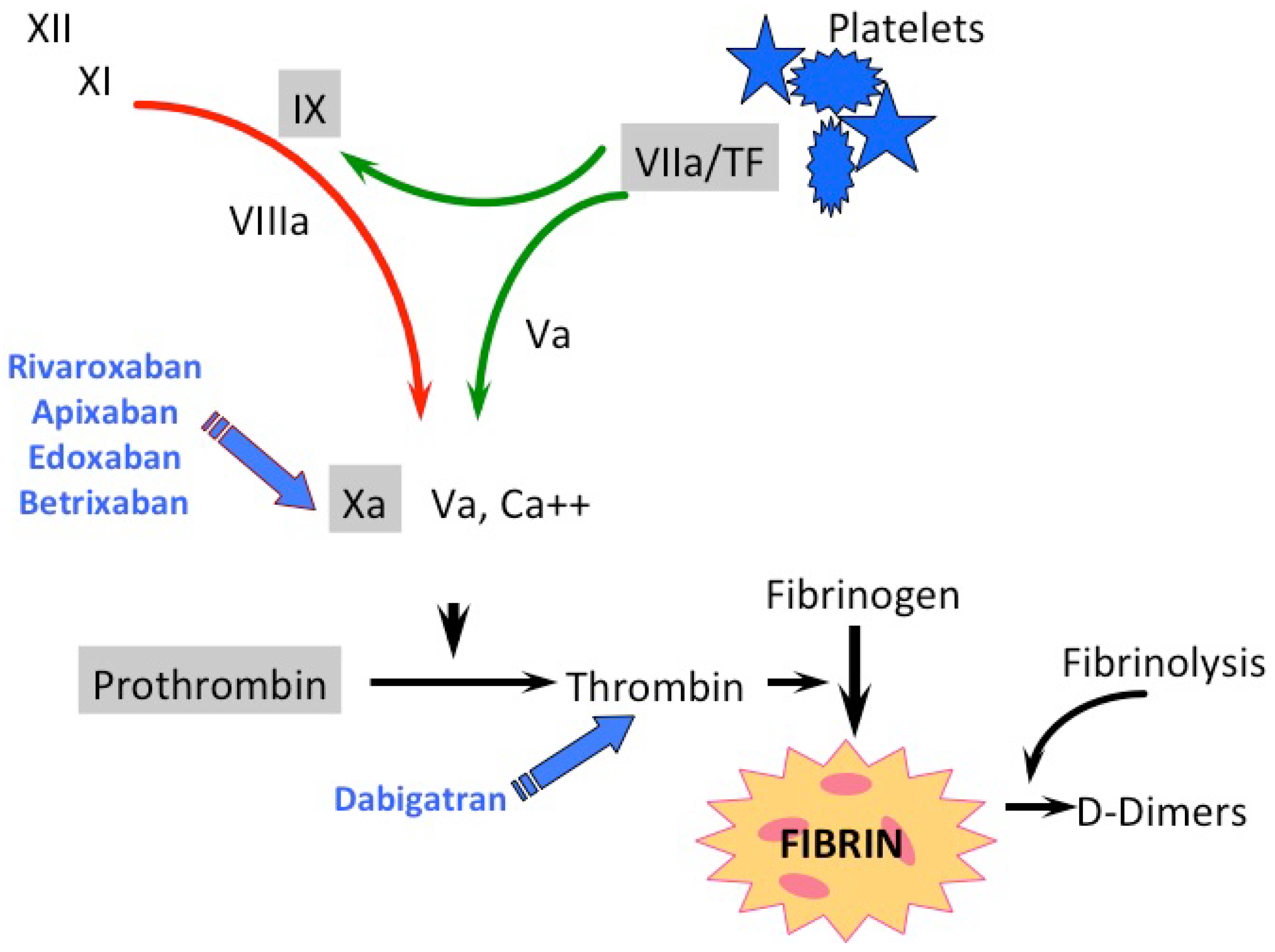
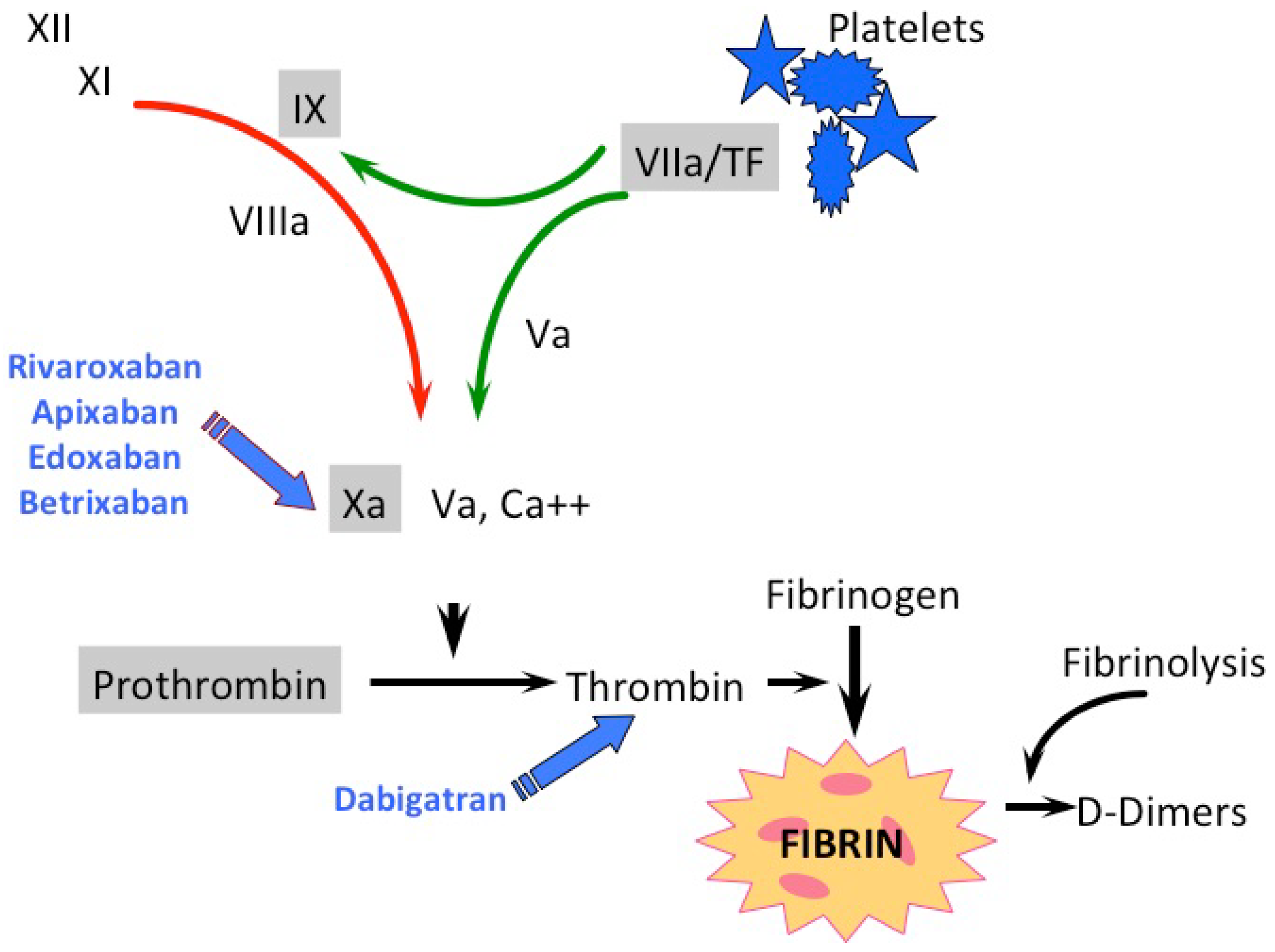
3.1. Direct Oral Factor IIa-Inhibitor
3.2. Direct Oral Factor Xa-Inhibitors
4. Indications
5. Relevant Drug-Drug Interactions and Criteria for Dose Reduction
5.1. Dabigatran
5.2. Rivaroxaban
5.3. Apixaban
5.4. Edoxaban
6. Is Adherence Still a Problem?
7. Monitoring of DOACs
8. Interferences, Effect or Lack of Effect on Routine Coagulation Tests
9. Managing the Risk of Periprocedural and Spontaneous Bleeding with DOACs
10. Management of Unexpected Bleeding
11. How to Switch between Anticoagulants
12. DOAC in Cancer Patients with Thrombosis
13. Perspectives
Author Contributions
Conflicts of Interest
Abbreviations
| ACS | acute coronary syndrome |
| AF | atrial fibrillation |
| APTT | activated partial thromboplastin time |
| ASA | acetylsalicylic acid |
| AUC | area under the plasma concentration-time curve |
| BID | twice daily |
| CKD | chronic kidney disease |
| CrCl | creatinine clearance |
| ECT | Ecarin clotting time |
| FIIa | activated factor II |
| FXa | activated factor X |
| DOAC | direct oral anticoagulant |
| DVT | deep vein thrombosis |
| HIT | Heparin-induce thrombocytopenia |
| LMWH | low molecular weight heparin |
| NVAF | non-valvular atrial fibrillation |
| OD | once daily |
| 4fPCC | four factor prothrombin complex concentrate |
| PE | pulmonary embolism |
| PT | prothrombin time |
| rFVIIa | recombinant factor VIIa |
| SEE | systemic embolic event |
| t ½ | half life |
| TSOAC | target specific oral anticoagulant =DOAC= NOAC |
| TT | Thrombin time |
| UFH | unfractionated heparin |
| VKA | Vitamin K Antagonist |
| VTE | venous thrombotic event |
References
- Haas, S. GARFIELD-AF–First data on healthcare of patients with atrial fibrillation in Germany. Dtsch. Med. Wochenschr. 2015, 140, S13–S14. [Google Scholar] [PubMed]
- Barnes, G.D.; Ageno, W.; Ansell, J.; Kaatz, S. Recommendation on the nomenclature for oral anticoagulants: Communication from the SSC of the ISTH. J. Thromb. Haemost 2015, 13, 1154–1156. [Google Scholar] [CrossRef] [PubMed]
- Weitz, J.I. Factor Xa and thrombin as targets for new oral anticoagulants. Thromb. Res. 2011, 127, S5–S12. [Google Scholar] [CrossRef]
- Perzborn, E.; Heitmeier, S.; Laux, V. Effects of Rivaroxaban on Platelet Activation and Platelet-Coagulation Pathway Interaction: In Vitro and In Vivo Studies. J. Cardiovasc. Pharmacol. Ther. 2015, 20, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Raghavan, N.; Frost, C.E.; Yu, Z.; He, K.; Zhang, H.; Humphreys, W.G.; Pinto, D.; Chen, S.; Bonacorsi, S.; Wong, P.C.; et al. Apixaban metabolism and pharmacokinetics after oral administration to humans. Drug Metab. Dispos. 2009, 37, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Frost, C.E.; Song, Y.; Shenker, A.; Wang, J.; Barrett, Y.C.; Schuster, A.; Harris, S.I.; LaCreta, F. Effects of age and sex on the single-dose pharmacokinetics and pharmacodynamics of apixaban. Clin. Pharmacokinet. 2015, 54, 651–662. [Google Scholar] [CrossRef] [PubMed]
- Bounameaux, H.; Camm, A.J. Edoxaban: An update on the new oral direct factor Xa inhibitor. Drugs 2014, 74, 1209–1231. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.H.; Rushton-Smith, S.K.; Goldhaber, S.Z.; Fitzmaurice, D.A.; Mantovani, L.G.; Goto, S.; Haas, S.; Bassand, J.-P.; Camm, A.J.; Ambrosio, G.; et al. Does sex affect anticoagulant use for stroke prevention in nonvalvular atrial fibrillation? The prospective global anticoagulant registry in the FIELD-Atrial Fibrillation. Circ. Cardiovasc. Qual. Outcomes 2015, 8, S12–S20. [Google Scholar] [CrossRef] [PubMed]
- Newby, L.K.; LaPointe, N.M.A.; Chen, A.Y.; Kramer, J.M.; Hammill, B.G.; DeLong, E.R.; Muhlbaier, L.H.; Califf, R.M. Long-term adherence to evidence-based secondary prevention therapies in coronary artery disease. Circulation 2006, 113, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Platt, A.B.; Localio, A.R.; Brensinger, C.M.; Cruess, D.G.; Christie, J.D.; Gross, R.; Parker, C.S.; Price, M.; Metlay, J.P.; Cohen, A.; et al. Risk factors for nonadherence to warfarin: Results from the IN-RANGE study. Pharmacoepidemiol. Drug Saf. 2008, 17, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Scridon, A.; Constantin Serban, R. Laboratory monitoring–A turning point in the use of new oral anticoagulants. Ther. Drug Monit. 2016, 38, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Mueck, W.; Schwers, S.; Stampfuss, J. Rivaroxaban and other novel oral anticoagulants: Pharmacokinetics in healthy subjects, specific patient populations and relevance of coagulation monitoring. Thromb. J. 2013, 11, 10. [Google Scholar] [CrossRef] [PubMed]
- Chin, P.K.L.; Wright, D.F.B.; Zhang, M.; Wallace, M.C.; Roberts, R.L.; Patterson, D.M.; Jensen, B.P.; Barclay, M.L.; Begg, E.J. Correlation between trough plasma dabigatran concentrations and estimates of glomerular filtration rate based on creatinine and cystatin C. Drugs R D 2014, 14, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Tsakiris, D.A. Direct oral anticoagulants—Interference with laboratory tests and mechanism of action. Semin. Hematol. 2014, 51, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Van Ryn, J.; Stangier, J.; Haertter, S.; Liesenfeld, K.-H.; Wienen, W.; Feuring, M.; Clemens, A. Dabigatran etexilate—A novel, reversible, oral direct thrombin inhibitor: Interpretation of coagulation assays and reversal of anticoagulant activity. Thromb. Haemost 2010, 103, 1116–1127. [Google Scholar] [CrossRef] [PubMed]
- Shahjouei, S.; Tsivgoulis, G.; Bavarsad Shahripour, R.; Jones, G.M.; Alexandrov, A.V.; Zand, R. Safety of intravenous thrombolysis among stroke patients taking new oral anticoagulants-case series and systematic review of reported cases. J. Stroke Cerebrovasc. Dis. 2015, 24, 2685–2693. [Google Scholar] [CrossRef] [PubMed]
- Schulman, S.; Crowther, M.A. How I treat with anticoagulants in 2012: New and old anticoagulants, and when and how to switch. Blood 2012, 119, 3016–3023. [Google Scholar] [CrossRef] [PubMed]
- Gogarten, W.; Vandermeulen, E.; Van Aken, H.; Kozek, S.; Llau, J.V.; Samama, C.M. Regional anaesthesia and antithrombotic agents: Recommendations of the european society of anaesthesiology. Eur. J. Anaesthesiol. 2010, 27, 999–1015. [Google Scholar] [CrossRef] [PubMed]
- Sie, P.; Samama, C.M.; Godier, A.; Rosencher, N.; Steib, A.; Llau, J.V.; Van der Linden, P.; Pernod, G.; Lecompte, T.; Gouin-Thibault, I.; et al. Surgery and invasive procedures in patients on long-term treatment with direct oral anticoagulants: Thrombin or factor-Xa inhibitors. Recommendations of the Working Group on Perioperative Haemostasis and the French Study Group on Thrombosis and Haemostasi. Arch. Cardiovasc. Dis. 2011, 104, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Stangier, J.; Feuring, M. Using the HEMOCLOT direct thrombin inhibitor assay to determine plasma concentrations of dabigatran. Blood Coagul. Fibrinolysis 2012, 23, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Douketis, J.D.; Wang, G.; Chan, N.; Eikelboom, J.W.; Syed, S.; Barty, R.; Moffat, K.A.; Spencer, F.A.; Blostein, M.; Schulman, S. Effect of standardized perioperative dabigatran interruption on the residual anticoagulation effect at the time of surgery or procedure. J. Thromb. Haemost 2016, 14, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Pollack, C.V.J.; Reilly, P.A.; Eikelboom, J.; Glund, S.; Verhamme, P.; Bernstein, R.A.; Dubiel, R.; Huisman, M.V.; Hylek, E.M.; Kamphuisen, P.W.; et al. Idarucizumab for Dabigatran Reversal. N. Engl. J. Med. 2015, 373, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Ghadimi, K.; Dombrowski, K.E.; Levy, J.H.; Welsby, I.J. Andexanet Alfa for the Reversal of Factor Xa inhibitor related Anticoagulation. Expert Rev. Hematol. 2016, 9, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Greinacher, A.; Thiele, T.; Selleng, K. Reversal of anticoagulants: An overview of current developments. Thromb. Haemost 2015, 113, 931–942. [Google Scholar] [CrossRef] [PubMed]
- Das, A.; Liu, D. Novel antidotes for target specific oral anticoagulants. Exp. Hematol. Oncol. 2015, 4, 25. [Google Scholar] [CrossRef] [PubMed]
- Barco, S.; Whitney Cheung, Y.; Coppens, M.; Hutten, B.A.; Meijers, J.C.M.; Middeldorp, S. In vivo reversal of the anticoagulant effect of rivaroxaban with four-factor prothrombin complex concentrate. Br. J. Haematol. 2016, 172, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Dibu, J.R.; Weimer, J.M.; Ahrens, C.; Manno, E.; Frontera, J.A. The Role of FEIBA in Reversing Novel Oral Anticoagulants in Intracerebral Hemorrhage. Neurocrit. Care 2015, in press. [Google Scholar]
- Dzik, W.H. Reversal of oral factor Xa inhibitors by prothrombin complex concentrates: A re-appraisal. J. Thromb. Haemost 2015, 13 (Suppl. 1), S187–S194. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Eikelboom, J.; Oldgren, J.; Parekh, A.; Pogue, J.; Reilly, P.A.; Themeles, E.; Varrone, J.; et al. Dabigatran versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Granger, C.B.; Alexander, J.H.; McMurray, J.J.V.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Avezum, A.; et al. Apixaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef] [PubMed]
- Camm, A.J.; Lip, G.Y.H.; De Caterina, R.; Savelieva, I.; Atar, D.; Hohnloser, S.H.; Hindricks, G.; Kirchhof, P. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: An update of the 2010 ESC Guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association. Eur. Heart J. 2012, 33, 2719–2747. [Google Scholar] [CrossRef] [PubMed]
- Heidbuchel, H.; Verhamme, P.; Alings, M.; Antz, M.; Diener, H.-C.; Hacke, W.; Oldgren, J.; Sinnaeve, P.; Camm, A.J.; Kirchhof, P. Updated European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist anticoagulants in patients with non-valvular atrial fibrillation. Europace 2015, 17, 1467–1507. [Google Scholar] [CrossRef] [PubMed]
- Prins, M.H.; Lensing, A.W.; Bauersachs, R.; van Bellen, B.; Bounameaux, H.; Brighton, T.A.; Cohen, A.T.; Davidson, B.L.; Decousus, H.; Raskob, G.E.; et al. Oral rivaroxaban versus standard therapy for the treatment of symptomatic venous thromboembolism: A pooled analysis of the EINSTEIN-DVT and PE randomized studies. Thromb. J. 2013, 11, 21. [Google Scholar] [CrossRef] [PubMed]
- Schulman, S.; Kearon, C.; Kakkar, A.K.; Mismetti, P.; Schellong, S.; Eriksson, H.; Baanstra, D.; Schnee, J.; Goldhaber, S.Z. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N. Engl. J. Med. 2009, 361, 2342–2352. [Google Scholar] [CrossRef] [PubMed]
- Larsen, T.B.; Nielsen, P.B.; Skjoth, F.; Rasmussen, L.H.; Lip, G.Y.H. Non-vitamin K antagonist oral anticoagulants and the treatment of venous thromboembolism in cancer patients: A semi systematic review and meta-analysis of safety and efficacy outcomes. PLoS ONE 2014, 9, e114445. [Google Scholar] [CrossRef] [PubMed]
- Lyman, G.H.; Bohlke, K.; Khorana, A.A.; Kuderer, N.M.; Lee, A.Y.; Arcelus, J.I.; Balaban, E.P.; Clarke, J.M.; Flowers, C.R.; Francis, C.W.; et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: American society of clinical oncology clinical practice guideline update 2014. J. Clin. Oncol. 2015, 33, 654–656. [Google Scholar] [CrossRef] [PubMed]
- Kuderer, N.M.; Lyman, G.H. Guidelines for treatment and prevention of venous thromboembolism among patients with cancer. Thromb. Res. 2014, 133, S122–S127. [Google Scholar] [CrossRef]
- Chan, N.C.; Bhagirath, V.; Eikelboom, J.W. Profile of betrixaban and its potential in the prevention and treatment of venous thromboembolism. Vasc. Health Risk Manag. 2015, 11, 343–351. [Google Scholar] [PubMed]
- Gomez-Outes, A.; Suarez-Gea, M.L.; Lecumberri, R.; Rocha, E.; Pozo-Hernandez, C.; Vargas-Castrillon, E. New parenteral anticoagulants in development. Ther. Adv. Cardiovasc. Dis. 2011, 5, 33–59. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| DOAC | Rivaroxaban | Edoxaban | Apixaban | Dabigatran |
|---|---|---|---|---|
| Xarelto ® | Lixiana ® | Eliquis ® | Pradaxa ® | |
| Target | FXa | FXa | FXa | FIIa |
| t ½ | 7–13 h | 10–14 h | 8–15 h | 12–17 h |
| Cmax | 2–4 h | 2–4 h | 2–4 h | 1–2 h |
| Renal clearance | 33% active 33% inactive | 50% | 25% | 80% |
| Bioavailability | 80% | 62% | 50% | 6% |
| Dosing scheme | OD | OD | BID | BID |
| Interaction | CYP3A4, CYP2J2, P-gp | P-gp | CYP3A4 P-gp | P-gp |
| Interference with food | Increases AUC to 39% | None | None | Prolongs Cmax to 2 h |
| Antidote | Andexanet alfa | Andexanet alfa | Andexanet alfa | Idarucizumab |
| Allowed in pregnancy | No | No | No | No |
| Induces HIT II | No | No | No | No |
| DOAC | Dosing Schedule | Total Trough (ng/mL) Median (P10-P90) | Total Peak (ng/mL) Median (P10-P90) | Anti-Xa Maximum (IU/mL) | Anti-Xa Minimum (IU/mL); (Median) |
|---|---|---|---|---|---|
| Dabigatran | 110 mg BID | 66 (28–155) | 133 (52–275) | ||
| 150 mg BID | 93 (40–215) | 184 (74–383) | |||
| Rivaroxaban | 15 mg BID | 57 (20–140) | 229 (180–320) | ||
| 20 mg OD | 25.6 (5.93–86.9) | 255 (189–419) | |||
| Apixaban | 2.5 mg BID | 1.3 (0.67–2.4) | 0.84 (0.37–1.8) | ||
| 5 mg BID | 2.55 (1.36–4.79) | 1.54 (0.61–3.43) | |||
| Edoxaban | 30 mg OD | 2.1 | 0.35 (0.21–0.57) | ||
| 60 mg OD | 3.8 | 0.64 (0.37–1.12) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwarb, H.; Tsakiris, D.A. New Direct Oral Anticoagulants (DOAC) and Their Use Today. Dent. J. 2016, 4, 5. https://doi.org/10.3390/dj4010005
Schwarb H, Tsakiris DA. New Direct Oral Anticoagulants (DOAC) and Their Use Today. Dentistry Journal. 2016; 4(1):5. https://doi.org/10.3390/dj4010005
Chicago/Turabian StyleSchwarb, Heike, and Dimitrios A. Tsakiris. 2016. "New Direct Oral Anticoagulants (DOAC) and Their Use Today" Dentistry Journal 4, no. 1: 5. https://doi.org/10.3390/dj4010005
APA StyleSchwarb, H., & Tsakiris, D. A. (2016). New Direct Oral Anticoagulants (DOAC) and Their Use Today. Dentistry Journal, 4(1), 5. https://doi.org/10.3390/dj4010005