Abstract
Background: Different methods have been used to fabricate and measure marginal gap in all-metal crowns, yet a systematic review on this topic has not been conducted. Objective: To review the existing literature regarding the measurement methods employed for the in vitro marginal gap measurement of pre-cemented all-metal single crowns and examine the influence of crown fabrication method on the marginal gap. Materials and Methods: A systematic search was performed from December 2024 backwards across EBSCO Host, Scopus, PubMed, and Web of Science databases following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and predefined eligibility criteria. The quality of included articles was evaluated using the Joanna Briggs Critical Appraisal Checklist. Results: Ten studies, involving 180 crowns, assessed marginal gaps using computerised superimposition (102 µm), scanning electron microscopy (89 µm), profilometry (100 µm), photogrammetry (59 µm), impression replica techniques (124 µm), and direct view microscopy (35 µm). Marginal gaps varied across crowns constructed with cobalt–chromium (97 µm), titanium (56 µm), noble metals (127 µm), and base metal alloys (35 µm). No significant differences (t = 1.06, p = 0.315) were observed between CAD/CAM (103.21 ± 58.56 µm) and lost wax casting method (71.59 ± 43.94 µm) of crown fabrication when analysed using an independent t-test. Conclusions: Cobalt–chromium was the most used material for AMCs, while titanium alloys produced the lowest mean marginal gap per crown. No significant differences in reported marginal gaps were observed between crowns fabricated using lost wax casting and CAD/CAM techniques. However, the limited number of studies, variation in measurement methods, and inconsistency in methodological rigour restricted the generalisability of the findings.
1. Introduction
All-metal crowns (AMCs) provide benefits of strength, durability, and resistance to chipping and fracture. In the aesthetically focussed modern era of advanced technologies and increased use of tooth coloured crown materials, AMCs remain a restorative option often recommended on account of the conservative reduction required in the tooth preparation process [1,2]. While their popularity may be declining, AMCs still provide an important option in restorative dentistry.
The traditional lost wax technique for constructing AMCs is labour-intensive and technique-sensitive [1]. More recently, computer-aided design and computer-aided manufacturing (CAD-CAM) technology have been employed to fabricate AMCs, delivering results comparable to those achieved with traditional methods [2]. Additionally, metal 3D printing has been applied to produce cobalt–chromium alloy AMCs with marginal gap accuracy comparable to AMCs constructed using conventional casting techniques, therefore offering a reliable alternative [3].
The marginal gap is the space between the axial wall of the prepared tooth and the internal surface of the restoration at the margin [4]. The marginal fit describes how precisely the crown conforms to the edge of the tooth. An ideal crown should exhibit a minimal and uniform marginal gap, preventing the accumulation of bacteria or debris, which in turn enhances the restoration’s durability and clinical success. Among aesthetics and fracture resistance, the marginal fit of a restoration is considered the most important factor for the success of crowns [5,6,7]. Precise marginal fit reduces the risk of plaque accumulation and hypersensitivity from microleakage, while suboptimal marginal fit can predispose to periodontal disease, caries, pulpitis, and increased cement exposure to the oral environment [6,7,8]. The factors that influence the marginal fit of a restoration include preparation design, finish line location, restorative material, fabrication method, impression material, and impression technique [9,10,11,12,13,14,15].
Measuring the marginal gap of pre-cemented AMCs is critical to assessing fit and overall quality as the precision of marginal fit directly impacts the longevity and clinical success. The accuracy of the marginal fit significantly influences the durability and clinical success of restorations [16]. Accurate measurement of the marginal gap assists clinicians and dental technicians to evaluate the fabrication process and make necessary modifications.
The numerical value for an acceptable marginal gap has changed over time and differs depending on the type of crown. Traditionally, clinical marginal gaps of up to 120 µm [17] have been considered acceptable, though it was acknowledged that margins greater than 160 µm could potentially be clinically successful [18]. This work was based on in vitro measurements using polyether rubber films of in vivo seated restorations [17]. However, recent research has suggested more stringent acceptable gaps such as ≤100 µmm [19,20], ≤90 µm [21], and ≤75 µm [22]; however, different materials, fabrication methods, and measurement methods have been used [23,24,25]. Despite these findings, there is no consensus on the ideal marginal gap [26].
Marginal gap measurements are usually made at convenient locations and the measurements averaged to infer the overall crown marginal gap [4,27,28]. It has been recommended to make at least 50 measurements per crown to reduce potential errors; however, this was based on calculations of the arithmetic mean and linked to the variation in gaps and desired precision in a small sample size [29]. There is currently no consensus on the ideal number of measurements needed for an accurate evaluation of crown marginal gap [30,31,32].
Methods for measuring marginal gaps can be categorised as two-dimensional (2D) or three-dimensional (3D), and destructive (DE) or non-destructive (ND), and the main measurement methods include direct view microscopy (2D, ND), scanning electron microscopy (3D, ND), and impression replica (2D, ND). There have been conflicting reports comparing the accuracy of scanning electron microscopy with light microscopy in measuring crown marginal gap [33,34]. Despite numerous reviews investigating crown marginal gap assessment and its influencing factors, a thorough comparison of the different measurement methods has not been conducted [15,22,24,26,35,36,37].
The aim of this study was to systematically review the existing literature regarding the measurement methods employed for in vitro marginal gap measurement of pre-cemented all-metal single crowns. Moreover, this study aimed to determine whether variables such as the crown fabrication method influenced the measured marginal gap. It was hypothesised that there would be no significant difference in marginal gaps between crowns fabricated using the traditional lost wax technique and those produced via CAD/CAM.
2. Materials and Methods
This systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). The study protocol was registered with Open Science Framework (https://osf.io/y5xah; accessed on 9 April 2025). The inclusion criteria concentrated on in vitro studies that examined marginal gaps of complete-coverage single AMCs pre-cementation. Eligible studies were required to provide a detailed methodology for gap assessment, including the number of measurements performed. Crown types considered included laboratory-fabricated crowns made of any metal or metal alloy, such as noble metals, base metal alloys, gold alloys, stainless steel, or titanium. Only studies that measured pre-cementation marginal gaps using a consistent method throughout the experiment were included to ensure comparability of results.
The exclusion criteria ruled out in vivo studies involving complete coverage all-ceramic crowns, metal–ceramic crowns, or crowns constructed by layering secondary materials onto cast alloys, as well as crowns evaluated virtually without a physical component. Studies assessing marginal gaps on preformed metal crowns, paediatric crowns, partial crowns, fixed partial dentures, or endocrowns were also excluded. Additionally, studies relying solely on manual visual or tactile estimations of marginal gaps or those focusing solely on internal fit without addressing marginal gaps were deemed ineligible.
Data were collected from the following databases: Scopus®, PubMed.gov, EBSCOHost Dentistry and Oral Sciences Source (DOSS), and Web of Science™ (WoS). Web of Science™ includes multiple indexed databases, such as the Web of Science Core Collection™, Current Contents Connect®, Derwent Innovations Index™, KCI-Korean Journal Database™, MEDLINE®, Russian Science Citation Index™, and SciELO Citation Index™, with translations into English where applicable. Searches were performed from December 2024 backwards, with no restrictions on publication dates. Field-specific filters were applied in Scopus and Web of Knowledge to focus on research related to material sciences in dentistry and healthcare.
The search process was independently conducted by two reviewers (JD and THF), and inter-rater reliability was assessed using the Cohen’s kappa (K) coefficient. The methodology incorporated keyword-based logic grids, Boolean operators, and manual reviews of bibliographies from related publications. Below is an example search query used for EBSCOHost DOSS.
(TI(Fit OR Gap* OR Space OR Distance OR Length* OR Accuracy* OR Precision) OR AB(Fit OR Gap* OR Space OR Distance OR Length* OR Accuracy* OR Precision)) AND (TI(“internal margin*” OR “internal discrepancy*” OR “margin* adaptation*” OR “cervical margin*” OR preparation OR “margin* integrity” OR “margin* opening*” OR “edge gap*” OR “margin* gap*”) OR AB(“internal margin*” OR “internal discrepancy*” OR “margin* adaptation*” OR “cervical margin*” OR preparation OR “margin* integrity” OR “margin* opening*” OR “edge gap*” OR “margin* gap*”)) AND (TI(“Un-cemented” OR “Fixed dental”) OR AB(“Un-cemented” OR “Fixed dental”) OR DE “Dental Crowns”) AND (TI(titanium* OR gold OR alloy OR noble OR metal OR “base metal” OR “Ni-Cr” OR Nickel OR chromium) OR AB(titanium* OR gold OR alloy OR noble OR metal OR “base metal” OR “Ni-Cr” OR Nickel OR chromium)) NOT (TI(PBM OR “Porcelain fused to metal” OR “Porcelain bonded to zirconia” OR “PBZ” OR ceramic OR laminate* OR veneer OR inlay OR onlay OR implant OR monolithic OR Emax OR “Lithium disilicate” OR dentures) OR AB(PBM OR “Porcelain fused to metal” OR “Porcelain bonded to zirconia” OR “PBZ” OR ceramic OR laminate* OR veneer OR inlay OR onlay OR implant OR monolithic OR Emax OR “Lithium disilicate” OR dentures)).
Eligible manuscripts were screened using the Covidence systematic review platform (Covidence.org; Veritas Health Innovations Ltd., Melbourne, Australia), which facilitated automated removal of duplicates and ensured consensus among reviewers. Disagreements were resolved prior to advancing eligible articles for further review, ensuring full agreement on the final selection. To ensure comprehensive coverage, all relevant studies were included for a broad narrative summary. The quality of the included studies was assessed by a prosthodontist (JD) using the Joanna Briggs Institute Critical Appraisal Checklist for Analytical Cross-Sectional Studies. No studies were excluded based solely on quality assessment results.
The following parameters were recorded for analysis: the number of crowns fabricated, crown material, method of crown construction, underlying crown preparation material, tooth form measured, measurement methods used, the number of marginal gap measurements per crown, the reported range of marginal gaps (in µm) across any direction, and the mean marginal gap for AMCs (rounded to the nearest whole number, in µm).
Statistical analyses were performed using SPSS software (version 26; IBM Corp, Armonk, NY, USA). The Shapiro–Wilk test was used to assess normality (p = 0.579). An independent t-test was conducted to compare the overall means of the marginal gaps across fabrication methods, namely, CAD/CAM and lost wax casting. This was followed by a robust equality of means test to evaluate the influence of data distribution on group outcomes.
3. Results
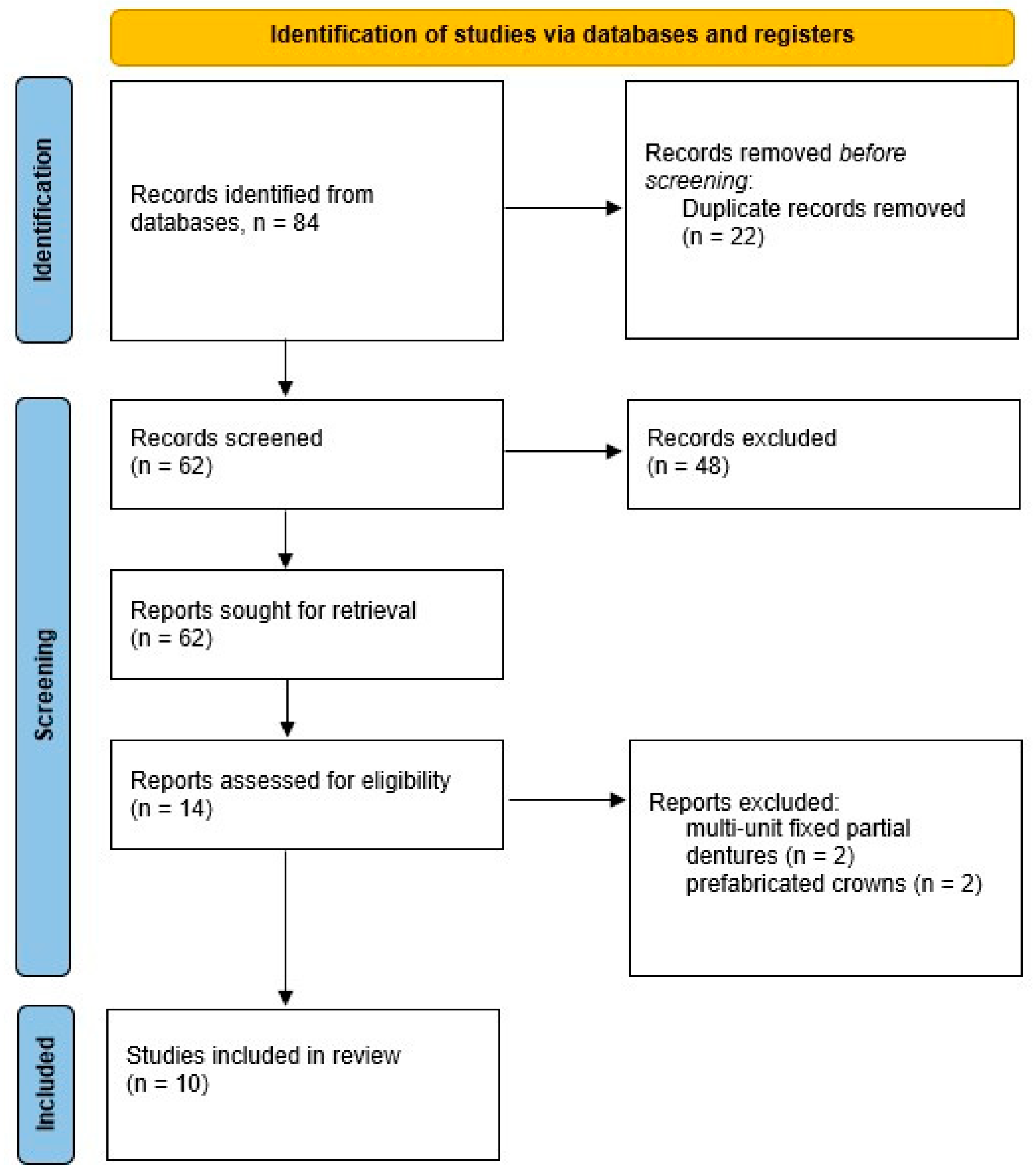
Ten articles were included for appraisal, as outlined in the PRISMA flow diagram (Figure 1), involving the marginal gaps of 180 crowns. Six studies evaluated the marginal gaps of cobalt–chromium alloy crowns (97.17 ± 55.73 µm) [38,39,40,41,42,43], which was the material used in all included studies published within the past 10 years. Earlier studies (prior to 2014) documented assessments of AMCs fabricated with titanium (55.85 ± 30.57 µm) [44,45], noble metals (127 µm) [46], and base metal alloys (35 µm) [47]. Computer-aided design–computer-aided manufacturing (CAD-CAM) was the most used AMC fabrication method, followed by lost wax casting and laser sintering. The findings have been summarised in Table 1. A critical appraisal (Table 2) revealed that five of the ten articles [38,39,40,45,46] did not fully address all of the identified confounding factors that could have influenced the measurement of the marginal gap. An important consideration is the inconsistency in the underlying materials of the dies used to fabricate the crowns, which introduces a significant risk of variation and bias, thereby impacting the overall certainty of the evidence.
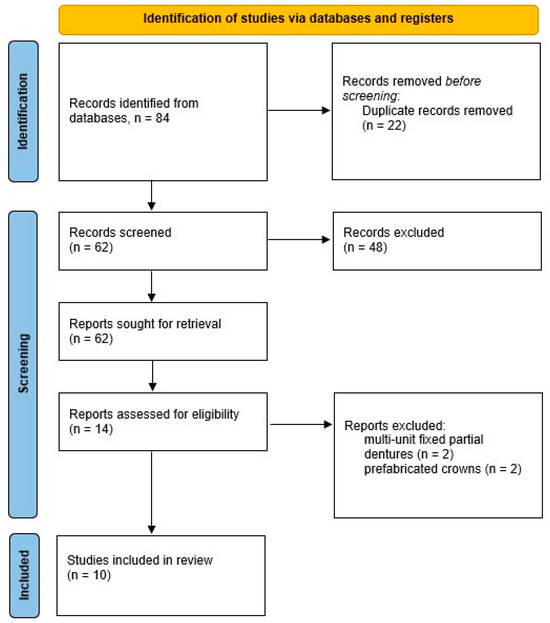
Figure 1.
PRISMA flowchart showing search results.

Table 1.
Marginal gap assessment for all-metal crowns.
Table 2.
Critical appraisal outcomes.
The most frequently used method for measuring the marginal gap was 3D superimposition, used in four studies; however, seven different measurement methods were used across the ten studies. The measurement methods used to measure marginal gaps (and their resultant mean marginal gap) included computerised superimposition (102 µm), scanning electron microscopy (89 µm), profilometry (100 µm), photogrammetry (59 µm), impression replica techniques (134 µm), and direct view microscopy (35 µm). A statistical comparison across these measurement methods was not feasible due to the limited data and the unequal distribution of measurements across the methods applied.
Assuming the accuracy of these measurement methods and materials used for crown fabrication was comparable [18], variations in the traditional lost wax technique and CAD/CAM in AMC fabrication were analysed (Table 3). Levene’s test for equality of variance was not significant (F = 0.381, p = 0.551).
Table 3.
Comparison between lost wax casting and CAD/CAM for all-metal crown fabrication.
The number of marginal gap measurement points made per crown was not reported in all studies. The most documented underlying abutment tooth used for AMC fabrication was an acrylic tooth, and the most frequently used tooth form was a maxillary molar, used in five studies.
4. Discussion
This systematic review found that only ten studies reported on the in vitro marginal gap measurement of pre-cemented single AMCs. Clinical significance is underpinned by in vivo research, and with the lack of in vitro studies, clinicians and researchers are directed to lower levels of evidence that may not have scientific and clinical rigour. With AMCs still holding clinical significance, the robustness of research in this area requires development and standardisation to develop reliable guidelines for clinical practice.
The various measurement methods have certain limitations that could have influenced the results [18,37]. The most frequently used method for measuring the marginal gap of pre-cemented AMCs was 3D superimposition. This method involves overlapping 3D scans and measures volume rather than points; therefore, marginal gap measurement requires 2D sections of the 3D analysis to measure points [48]. Three-dimensional superimposition offers the benefits of convenience, practicality, and repeatability but requires specialised and costly equipment.
The direct-view microscopy method is susceptible to errors due to the selection of measurement points and the differentiation between materials. It also relies on magnification and is restricted to in vitro use, which may not fully replicate clinical conditions. Additionally, the magnification process can introduce inaccuracies if the measurement points are not precisely chosen or if there is difficulty distinguishing between different materials. The impression replica method, while useful, may encounter difficulties in pinpointing the location of crown margins. This tool can also suffer from tearing of the elastomeric film, which can lead to inaccuracies. Errors in sectioning the impression can further contribute to overestimated measurements, as the process may not capture the true dimensions of the marginal gap. While profilometry is non-destructive, it necessitates accurate repositioning to avoid discrepancies. Any slight misalignment during repositioning can result in discrepancies, affecting the reliability of the measurements. The large range of different measurement methods used across the included studies indicates a lack of standardisation in method selection, likely dictated by availability and cost.
In addition to these tool-specific limitations, frequent confounding factors included the uneven distribution of samples among groups and the variability in measurement tools, each with its own limitations, as previously mentioned [18]. Moreover, inconsistencies in specimen preparation, differences in cement space, and variations in alloy composition introduced biases. The absence of standardised protocols across studies further complicated result comparisons, potentially impacting the accuracy and reliability of the findings. These confounding factors underscore the necessity for more rigorous and standardised methodologies in future research. Establishing consistent protocols for sample preparation and measurement methods across research teams could greatly improve the comparability and reliability of the results. Additionally, addressing uneven sample distribution through better study designs and larger sample sizes would lead to more robust and generalisable findings.
Seven [28,38,39,40,41,45,47] of the ten included studies reported mean marginal gaps within the generally recognised clinically acceptable limit of 120 µm [17]. The study by Mai et al. [42] seemingly represents an outlier (reporting a mean marginal gap of 200 µm) and the Ferrari et al. [46] study did not fully address all identified confounding factors. The accuracy of different measurement methods has not been compared, and a statistical analysis was not possible in this study due to the limited data, which impedes meaningful comparison across the included studies. Consequently, clinicians and researchers must rely on individual study findings to assess marginal gaps against established standards [17], clinical guidelines that suggest <80 µm is difficult to detect [22], or personal preferences [31]. Despite smaller gaps being preferable, some studies indicate that bonding materials to tooth surfaces may reduce the importance of the marginal gap [37]. The optimal marginal gap for AMCs, and indeed for crowns in general, remains uncertain.
The average number of crowns evaluated in each study was 16, which falls below the suggested 50 measurements previously recommended [29]. Without explicit justification in the included research, it appears convenience was the primary factor in determining the sample size, rather than scientific rationale. A critical aspect of further research should focus on establishing an appropriate number of samples and measurements per sample, instead of simply citing previous studies to justify methodological choices.
The most used AMC material was a cobalt–chromium alloy, which was the only material used in the five included studies published in the past 10 years. Congruently, CAD/CAM was the most used method of AMC fabrication. This represents a change to the traditional AMC fabrication philosophy that used the lost wax technique with precious or semi-precious alloys. The fabrication process using CAD/CAM milling can be either additive or subtractive, which helps to eliminate the issues of porosity and imperfections typically associated with casting techniques [11,12]. However, there are multiple CAD/CAM design and milling unit variables that can influence the marginal gap, such as cement space settings [49]. Nevertheless, within the limitations of this study, the method of fabrication did not influence the marginal gap of the AMCs, based on the assumption that the accuracy of the measurement methods was comparable. It is difficult to provide a scientific rationale for the lack of difference in the AMC marginal gap across the different fabrication methods considering the data distribution. The large range of experimental variables (materials, fabrication methods, measurement methods, and number of measurements) used in the included studies reduced the statistical analysis meaning; therefore, this observation should be observed with some caution.
The current study focused on the in vitro measurement of pre-cemented AMCs. The statistical analysis was constrained by experimental variables, crown construction techniques, and variations in measurement methods, which resulted in significant mean variations offset by large standard deviations. Although in vitro analysis provided a controlled environment for assessing marginal gaps, it could not account for factors such as preparation design and clinically used impression materials, highlighting a limitation of in vitro studies on crown marginal gaps. Evaluating the finish line location was deemed superfluous as the classification of supra- or sub-gingival margins holds little relevance in an in vitro context. This limitation highlights the need for future research to standardise the marginal gap measurement methods and protocols to ensure accuracy, regardless of the measurement methods used. Future studies should also aim to transition from in vitro to in vivo measurements to better reflect clinical conditions. Standardising these methods will help achieve more reliable and consistent results, ultimately improving the clinical success and longevity of AMCs. By addressing these limitations, researchers can enhance the understanding of marginal gaps and their impact on AMCs. This study provides a reference point for future research.
5. Conclusions
The most frequently used method for measuring the marginal gaps of pre-cemented all-metal crowns was 3D superimposition, used in four of the ten included studies; however, seven different measurement methods were used across the ten studies. The most prevalent all-metal crown fabrication method was CAD/CAM using a cobalt–chromium alloy, reported in all five of the included studies published in the past 10 years. Within the studies included in this systematic review, the crown fabrication method did not influence the marginal gap of all-metal crowns.
Author Contributions
J.D., conceptualisation, data curation, funding acquisition, investigation, methodology, project administration, resources, supervision, validation, visualisation, writing—original draft, and writing—review and editing; T.H.F., data curation, formal analysis, funding acquisition, investigation, methodology, resources, software, validation, visualisation, writing—original draft, and writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by the University of Adelaide Paul Kwok Lee Bequest (350-75134777) and the University of Adelaide Early Grant Development Scheme (340-13133234).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Quante, K.; Ludwig, K.; Kern, M. Marginal and internal fit of metal-ceramic crowns fabricated with a new laser melting technology. Dent. Mater. 2008, 24, 1311–1315. [Google Scholar] [CrossRef]
- Yang, J.; Li, H. Accuracy of CAD-CAM milling versus conventional lost-wax casting for single metal copings: A systematic review and meta-analysis. J. Prosthet. Dent. 2022, 132, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.; Hong, M.-H.; Lee, H.; Lee, C.-H.; Hong, M.; Lee, J.; Lee, D.-H. Reliability of metal 3D printing with respect to the marginal fit of fixed dental prostheses: A systematic review and meta-analysis. Materials 2020, 13, 4781. [Google Scholar] [CrossRef]
- Holmes, J.R.; Bayne, S.C.; Holland, G.A.; Sulik, W.D. Considerations in measurement of marginal fit. J. Prosthet. Dent. 1989, 62, 405–408. [Google Scholar] [CrossRef]
- Alqahtani, F. Marginal fit of all-ceramic crowns fabricated using two extraoral CAD/CAM systems in comparison with the conventional technique. Clin. Cosmet. Investig. Dent. 2017, 9, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Nonaka, M.; Maruyama, T. In vitro fitting accuracy of copy-milled alumina cores and all-ceramic crowns. Int. J. Prosthodont. 2000, 13, 189. [Google Scholar] [PubMed]
- Contrepois, M.; Soenen, A.; Bartala, M.; Laviole, O. Marginal adaptation of ceramic crowns: A systematic review. J. Prosthet. Dent. 2013, 110, 447–454. [Google Scholar] [CrossRef]
- Souza, R.O.A.; Özcan, M.; Pavanelli, C.A.; Buso, L.; Lombardo, G.H.L.; Michida, S.M.A.; Mesquita, A.M.M.; Bottino, M.A. Marginal and internal discrepancies related to margin design of ceramic crowns fabricated by a CAD/CAM system. J. Prosthodont. Implant. Esthet. Reconstr. Dent. 2012, 21, 94–100. [Google Scholar] [CrossRef]
- Shah, N.; Badwaik, P.; Sheth, V.H.; Bhatnagar, V.; Bhanushali, N.; Patil, P. Effect of different finish line preparations on the marginal and internal adaptation of cobalt-chromium metal alloy copings fabricated by using CAD-CAM technology: A systematic review and meta-analysis. J. Prosthet. Dent. 2022, 127, 716–728. [Google Scholar] [CrossRef]
- Li, J.; Chen, C.; Liao, J.; Liu, L.; Ye, X.; Lin, S.; Ye, J. Bond strengths of porcelain to cobalt-chromium alloys made by casting, milling, and selective laser melting. J. Prosthet. Dent. 2017, 118, 69–75. [Google Scholar] [CrossRef]
- Usta Kutlu, İ.; Hayran, Y. Influence of various fabrication techniques and porcelain firing on the accuracy of metal-ceramic crowns. BMC Oral Health 2024, 24, 845. [Google Scholar] [CrossRef] [PubMed]
- Kocaağaoğlu, H.; Albayrak, H.; Kilinc, H.I.; Gümüs, H.Ö. Effect of repeated ceramic firings on the marginal and internal adaptation of metal-ceramic restorations fabricated with different CAD-CAM technologies. J. Prosthet. Dent. 2017, 118, 672–677. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Chen, Y.; Cheng, H.; Sawase, T. Finish-line designs for ceramic crowns: A systematic review and meta-analysis. J. Prosthet. Dent. 2019, 122, 22–30. [Google Scholar] [CrossRef]
- Asavapanumas, C.; Leevailoj, C. The influence of finish line curvature on the marginal gap width of ceramic copings. J. Prosthet. Dent. 2013, 109, 227–233. [Google Scholar] [CrossRef]
- Tsirogiannis, P.; Reissmann, D.R.; Heydecke, G. Evaluation of the marginal fit of single-unit, complete-coverage ceramic restorations fabricated after digital and conventional impressions: A systematic review and meta-analysis. J. Prosthet. Dent. 2016, 116, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Haralur, S.B.; Ghaseb, G.A.A.L.; Alqahtani, N.A.; Alqahtani, B. Comparison of microleakage between different restorative materials to restore marginal gap at crown margin. PeerJ 2021, 9, e10823. [Google Scholar] [CrossRef]
- McLean, J.W.; von Fraunhofer, J.A. The estimation of cement film thickness by an in vivo technique. Br. Dent. J. 1971, 131, 107–111. [Google Scholar] [CrossRef]
- Dudley, J.; Farook, T.H. Marginal gap measurement of ceramic single crowns before cementation: A systematic review. J. Prosthet. Dent. 2025. [Google Scholar] [CrossRef]
- Davis, D.R. Comparison of fit of two types of all-ceramic crowns. J. Prosthet. Dent. 1988, 59, 12–16. [Google Scholar] [CrossRef]
- Reich, S.; Gozdowski, S.; Trentzsch, L.; Frankenberger, R.; Lohbauer, U.J. Marginal fit of heat-pressed vs. CAD/CAM processed all-ceramic onlays using a milling unit prototype. Oper. Dent. 2008, 33, 644–650. [Google Scholar] [CrossRef]
- Memari, Y.; Mohajerfar, M.; Armin, A.; Kamalian, F.; Rezayani, V.; Beyabanaki, E. Marginal adaptation of CAD/CAM all-ceramic crowns made by different impression methods: A literature review. J. Prosthodont. 2019, 28, e536–e544. [Google Scholar] [CrossRef]
- Hung, S.H.; Hung, K.-S.; Eick, J.D.; Chappell, R.P. Marginal fit of porcelain-fused-to-metal and two types of ceramic crown. J. Prosthet. Dent. 1990, 63, 26–31. [Google Scholar] [CrossRef]
- Vojdani, M.A.; Torabi, K.A.; Farjood, E.B.; Khaledi, A.A.R. Comparison the marginal and internal fit of metal copings cast from wax patterns fabricated by CAD/CAM and conventional wax up techniques. J. Dent. 2013, 14, 118. [Google Scholar]
- Nawafleh, N.A.; Mack, F.; Evans, J.; Mackay, J.; Hatamleh, M.M. Accuracy and reliability of methods to measure marginal adaptation of crowns and FDPs: A literature review. J. Prosthodont. 2013, 22, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Paul, N.; Swamy, K.R.; Dhakshaini, M.R.; Sowmya, S.; Ravi, M.B. Marginal and internal fit evaluation of conventional metal-ceramic versus zirconia CAD/CAM crowns. J. Clin. Exp. Dent. 2020, 12, e31. [Google Scholar] [CrossRef] [PubMed]
- Sanches, I.B.; Metzker, T.C.; Kappler, R.; Oliveira, M.V.; Carvalho, A.O.; Lima, E.M. Marginal adaptation of CAD-CAM and heat-pressed lithium disilicate crowns: A systematic review and meta-analysis. J. Prosthet. Dent. 2023, 129, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Su, S.; Dudley, J. The marginal gaps of lithium disilicate crowns constructed by different scanner and milling unit combinations. Aust. Dent. J. 2022, 67, 125–131. [Google Scholar] [CrossRef]
- Tan, K.; Dudley, J. The marginal gaps of sequentially milled lithium disilicate crowns using two different milling units. Aust. Dent. J. 2022, 67, 239–248. [Google Scholar] [CrossRef]
- Groten, M.; Axmann, D.; Pröbster, L.; Weber, H. Determination of the minimum number of marginal gap measurements required for practical in vitro testing. J. Prosthet. Dent. 2000, 83, 40–49. [Google Scholar] [CrossRef]
- Matta, R.E.; Schmitt, J.; Wichmann, M.; Holst, S. Circumferential fit assessment of CAD/CAM single crowns—A pilot investigation on a new virtual analytical protocol. Quintessence Int. 2012, 43, 801. [Google Scholar]
- Dudley, J.; Xu, J. The influence of different cement spaces on the marginal gap of lithium disilicate crowns constructed by two scanner and milling unit combinations. Aust. Dent. J. 2024, 69, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Kwong, B.; Dudley, J. A comparison of the marginal gaps of lithium disilicate crowns fabricated by two different intraoral scanners. Aust. Dent. J. 2020, 65, 150–157. [Google Scholar] [CrossRef]
- Groten, M.; Girthofer, S.; Pröbster, L. Marginal fit consistency of copy-milled all-ceramic crowns during fabrication by light and scanning electron microscopic analysis in vitro. J. Oral Rehabil. 1997, 24, 871–881. [Google Scholar] [CrossRef] [PubMed]
- Schmalz, G.; Federlin, M.; Reich, E. Effect of dimension of luting space and luting composite on marginal adaptation of a class II ceramic inlay. J. Prosthet. Dent. 1995, 73, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Hasanzade, M.; Aminikhah, M.; Afrashtehfar, K.I.; Alikhasi, M. Marginal and internal adaptation of single crowns and fixed dental prostheses by using digital and conventional workflows: A systematic review and meta-analysis. J. Prosthet. Dent. 2021, 126, 360–368. [Google Scholar] [CrossRef]
- Kandavalli, S.R.; Kandavalli, S.R.; Ruban, R.S.; Lo, C.H.; Kumar, R.; Elshalakany, A.B.; Pruncu, C.I. A conceptual analysis on ceramic materials used for dental practices: Manufacturing techniques and microstructure. ECS J. Solid State Sci. Technol. 2022, 11, 053005. [Google Scholar] [CrossRef]
- Van den Breemer, C.R.G.; Gresnigt, M.M.M.; Cune, M.S. Cementation of glass-ceramic posterior restorations: A systematic review. BioMed Res. Int. 2015, 2015, 148954. [Google Scholar] [CrossRef] [PubMed]
- Berger, L.; Adler, W.; Katharina Kreuzer, M.M.; Wichmann, M.; Matta, R.E. Comparison of digital and conventional impressions based on the 3D fit of crowns. Int. J. Prosthodont. 2022, 35, 801–808. [Google Scholar] [CrossRef]
- Gholamrezaei, K.; Vafaee, F.; Afkari, B.F.; Firouz, F.; Seif, M. Fit of cobalt-chromium copings fabricated by the selective laser melting technology and casting method: A comparative evaluation using a profilometer. Dent. Res. J. (Isfahan) 2020, 17, 200–207. [Google Scholar]
- Chang, H.-S.; Peng, Y.-T.; Hung, W.-L.; Hsu, M.-L. Evaluation of marginal adaptation of CoCrMo metal crowns fabricated by traditional method and computer-aided technologies. J. Dent. Sci. 2019, 14, 288–294. [Google Scholar] [CrossRef]
- Dahl, B.E.; Dahl, J.E.; Rønold, H.J. Digital evaluation of marginal and internal fit of single-crown fixed dental prostheses. Eur. J. Oral Sci. 2018, 126, 512–517. [Google Scholar] [CrossRef] [PubMed]
- Mai, H.N.; Lee, K.E.; Lee, K.B.; Jeong, S.M.; Lee, S.J.; Lee, C.H.; An, S.Y.; Lee, D.H. Verification of a computer-aided replica technique for evaluating prosthesis adaptation using statistical agreement analysis. J. Adv. Prosthodont. 2017, 9, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Chou, W.-T.; Chuang, C.-C.; Wang, Y.-B.; Chiu, H.-C. Comparison of the internal fit of metal crowns fabricated by traditional casting, computer numerical control milling, and three-dimensional printing. PLoS ONE 2021, 16, e0257158. [Google Scholar] [CrossRef]
- Tan, P.L.; Gratton, D.G.; Diaz-Arnold, A.M.; Holmes, D.C. An in vitro comparison of vertical marginal gaps of CAD/CAM titanium and conventional cast restorations. J. Prosthodont. 2008, 17, 378–383. [Google Scholar] [CrossRef]
- Besimo, C.; Jeger, C.; Guggenheim, R. Marginal adaptation of titanium frameworks produced by CAD/CAM techniques. Int. J. Prosthodont. 1997, 10, 541–546. [Google Scholar] [PubMed]
- Ferrari, M.; Mason, P.N.; Poli, L.; Di Dente, M. Marginal Adaptation of Crowns: A Scanning Electron Microscopic Investigation. Int. J. Periodontics Restor. Dent. 1994, 14, 272–279. [Google Scholar]
- White, S.N.; Kipnis, V. The three-dimensional effects of adjustment and cementation on crown seating. Int. J. Prosthodont. 1993, 6, 248–254. [Google Scholar]
- Park, J.Y.; Bae, S.Y.; Lee, J.J.; Kim, J.H.; Kim, H.Y.; Kim, W.C. Evaluation of the marginal and internal gaps of three different dental prostheses: Comparison of the silicone replica technique and three-dimensional superimposition analysis. J. Adv. Prosthodont. 2017, 9, 159–169. [Google Scholar] [CrossRef]
- Zhang, Y.; Dudley, J. The influence of different cement spaces on the marginal gap of CAD/CAM all-ceramic crowns. Aust. Dent. J. 2019, 64, 167–174. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).