
Balancing the Load: How Optimal Forces Shape the Longevity and Stability of Orthodontic Mini-Implants

 ,
,  , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
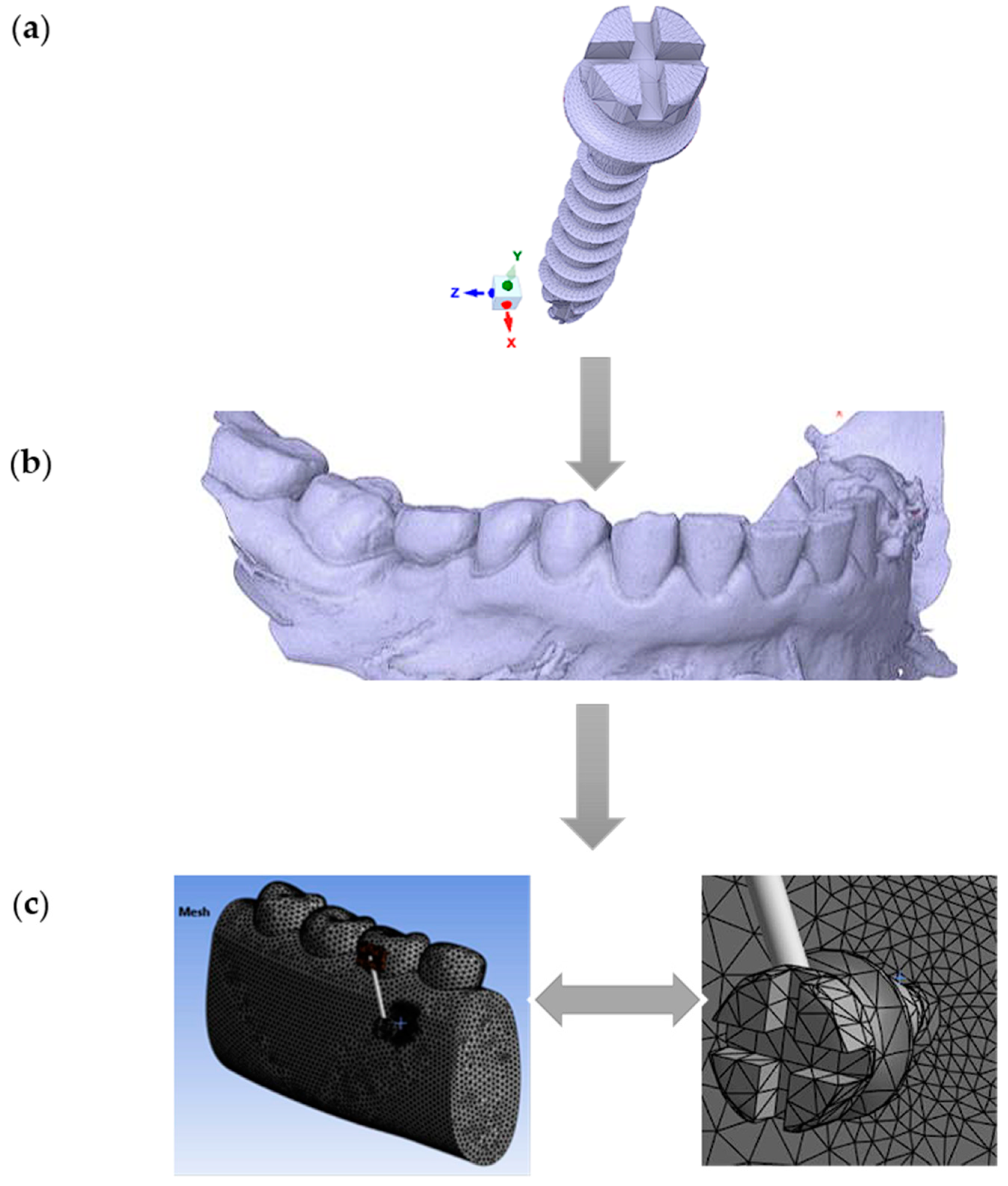
2.1. Geometric Modeling
2.2. Simulation Parameters
2.3. Technical Details of FEA Modeling
- Discretization (nodes/elements): This indicates the number of nodes and elements used in the FEA model. The higher the number of nodes and elements is, the more detailed the geometric representation of the object and its interactions.
- Element: This refers to the type of finite elements used in the model, in this case, 10-node tetrahedrons. These elements are used to discretize the geometry of the object and calculate the structural response.
- Software: This refers to the analysis software used to perform the finite element simulations. In this case, ANSYS is the specified software.
- Material model: This describes the material properties used in the model. The specified model is isotropic, homogeneous, and linear. Thus, the material properties do not vary depending on direction or position. In addition, the material is uniform, and its behavior is linear under load.
- Contact model: This describes how the interactions between different parts of the model are simulated. It mentions the use of nonlinear friction for the interaction between the MI and the bone, as well as linear bonding for other interactions.
- Loading: This specifies the loads applied to the model. The loading is oblique, with values between 2 N and 10 N.
- MI type: This describes the characteristics of the MIs used in the model, including dimensions and thread type.
- Boundary conditions: This specifies the boundary conditions applied to the model. In this case, 100% osseointegration is mentioned, indicating that the MI is fully integrated into the bone and there is no relative movement between them.
3. Results
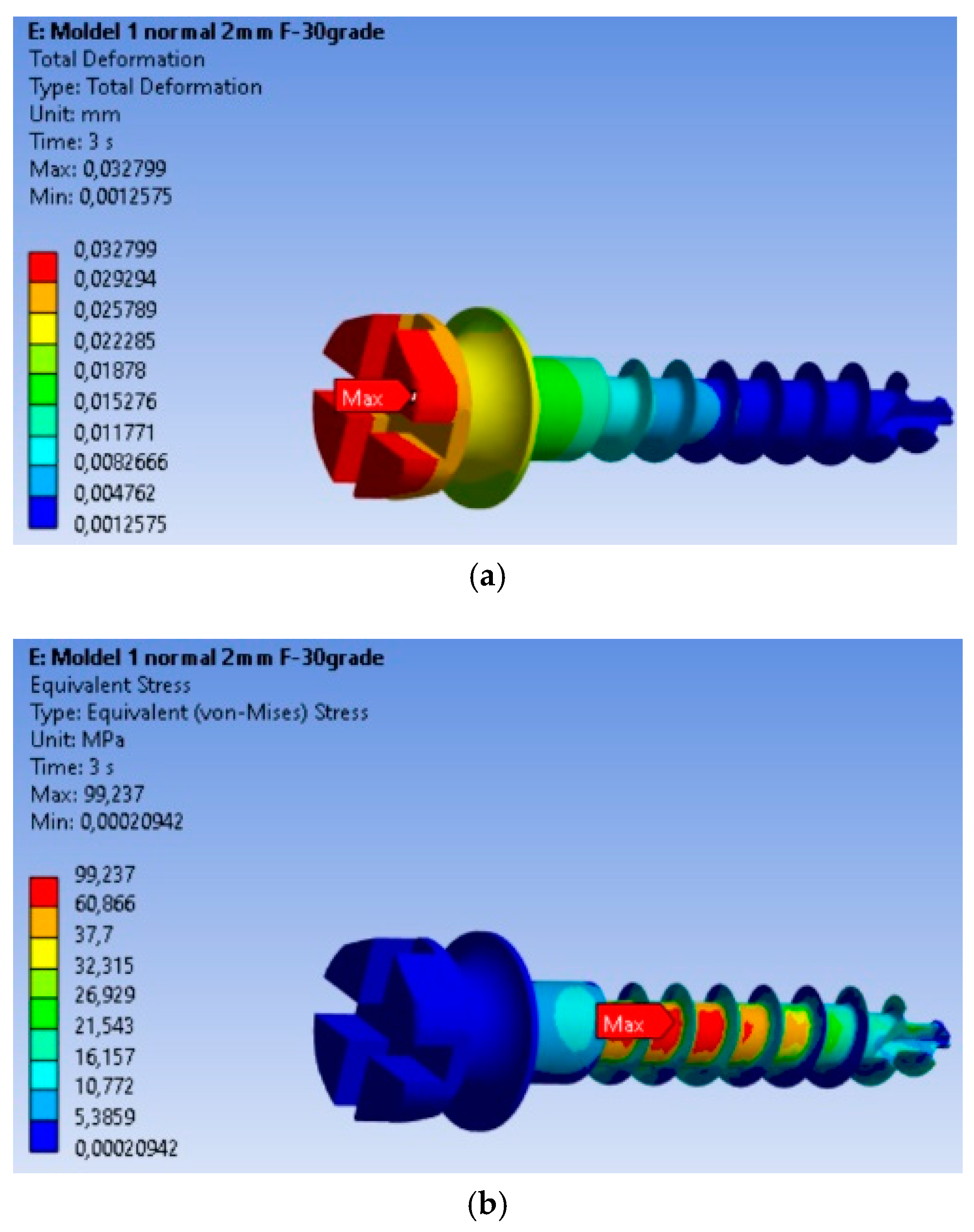
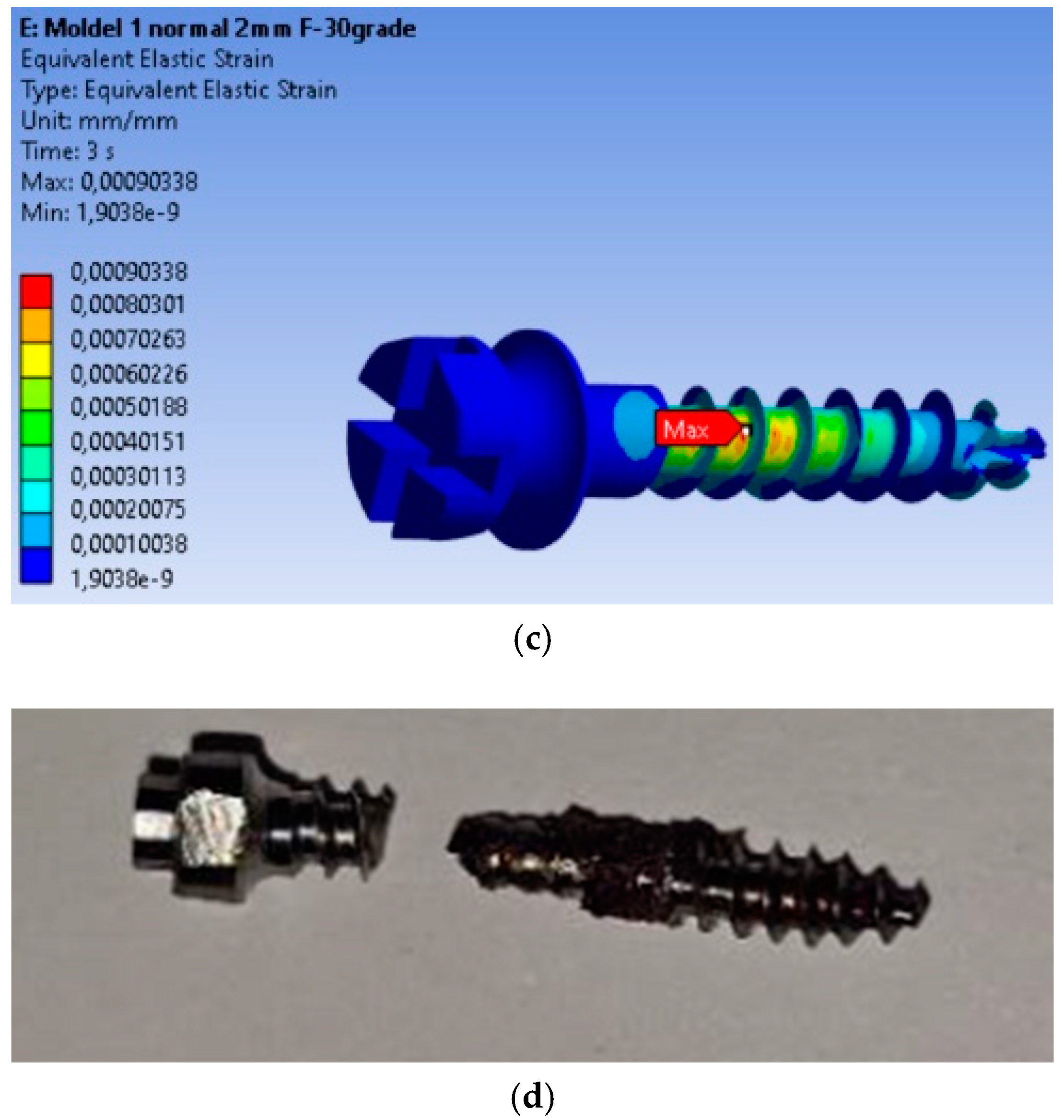
3.1. Determinations: Total Deformations, von Mises Equivalent Stresses, and Equivalent Strains
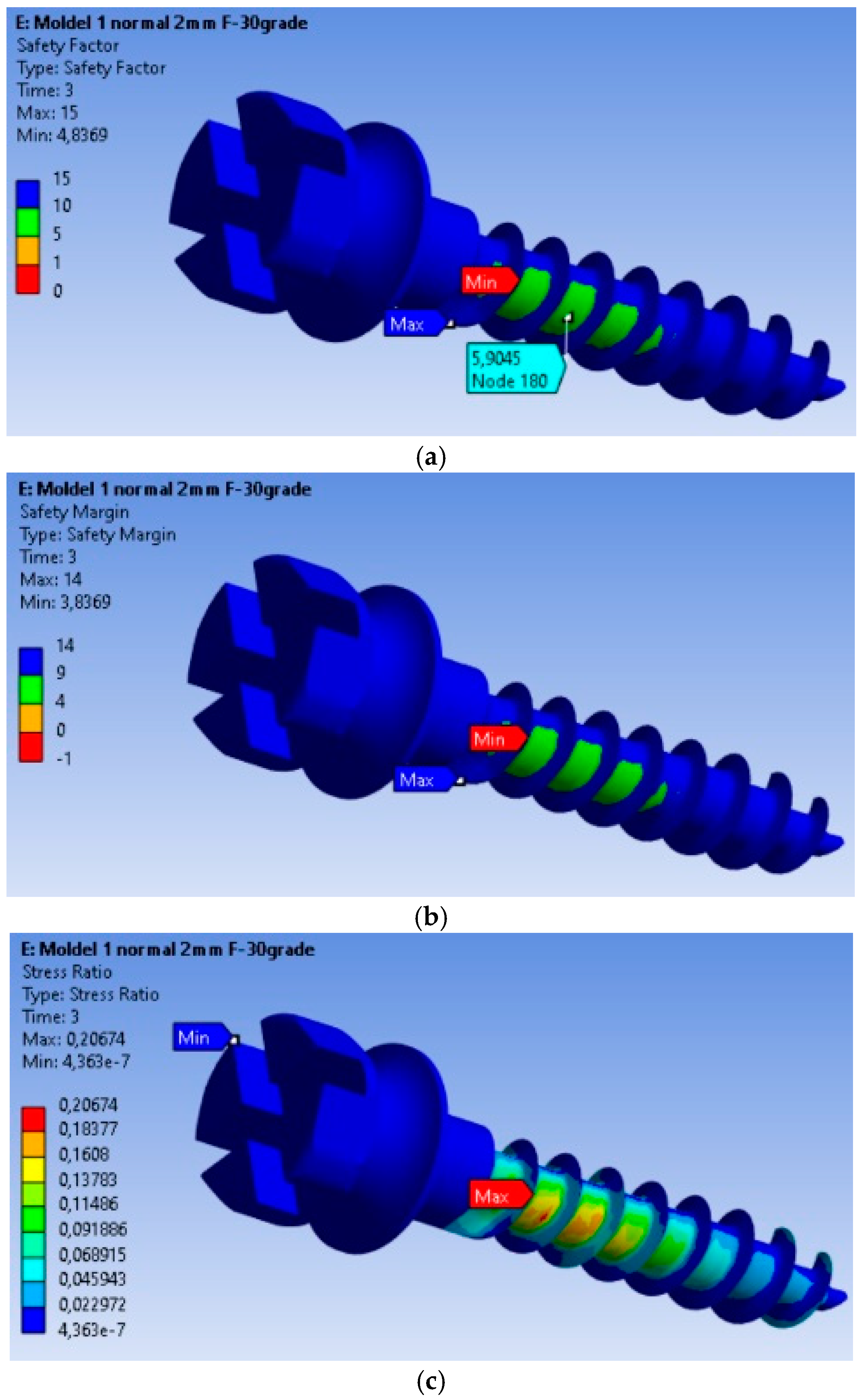
3.2. Safety Analysis of the MI: Safety Factors, Safety Margin, and Stress Ratio
3.3. Fatigue Analysis of the MI Under 2 N Orthodontic Force: Life Expectancy, Safety Factors, and Failure Assessment
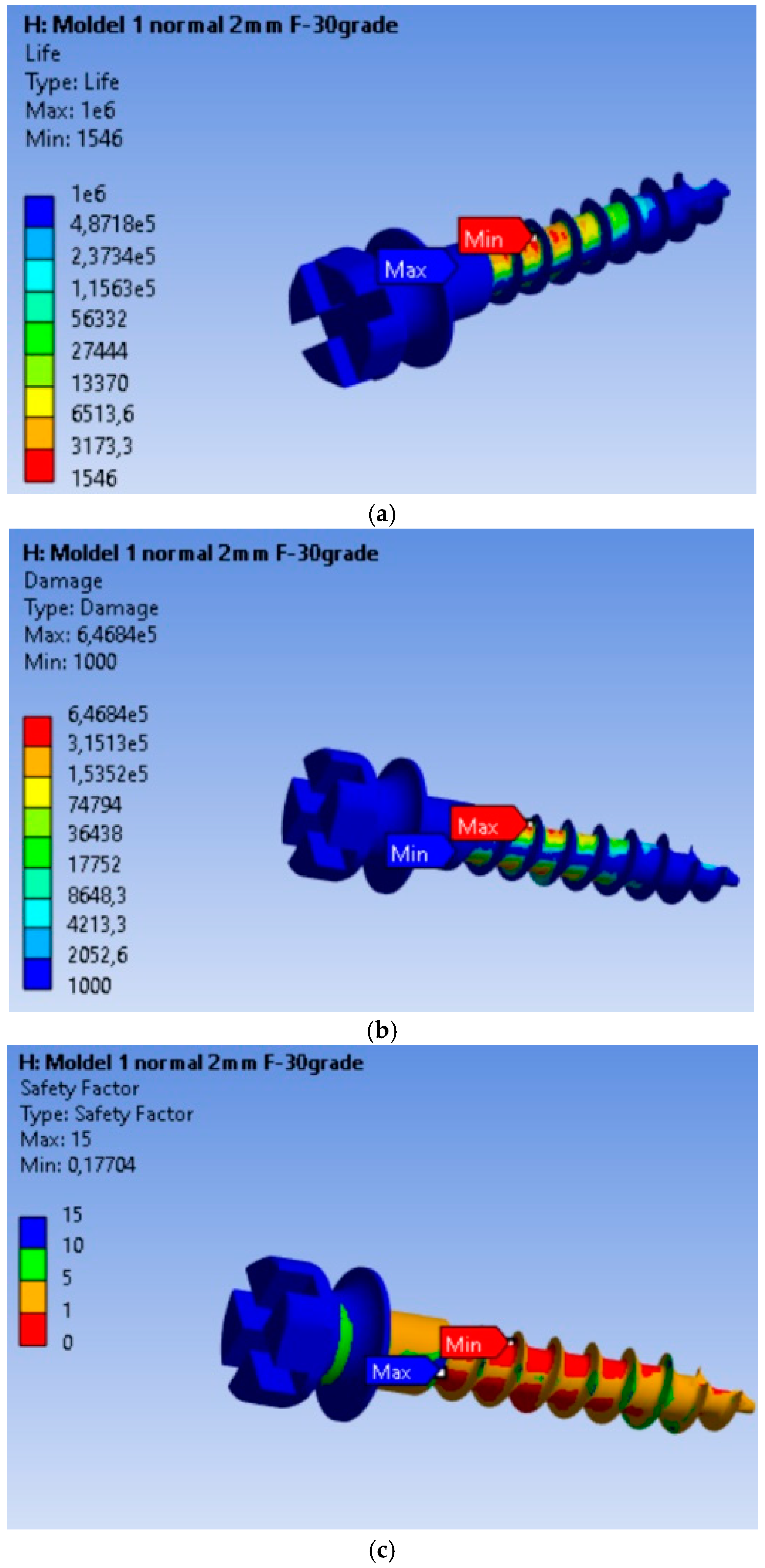
3.4. Fatigue Performance of the MI Under 10 N Orthodontic Force: Life Expectancy, Safety Factors, and Failure Analysis
4. Discussion
4.1. Discussions on Displacement, Stress, Strain, and Safety Factors in Mini-Implants
4.2. Future Research Directions
4.3. Limitations and Future Directions
- (i)
- Use of a single implant length (12 mm): An important aspect of this study is that only MIs with a length of 12 mm were used. Future studies should include a wider range of lengths to better understand the relationship between MI length and mechanical performance;
- (ii)
- Finite models of the bone: The bone modeling was done using linear, elastic, and isotropic mechanical properties. This simplification does not accurately reflect the complex and heterogeneous behavior of real bone, particularly cortical and spongy bone;
- (iii)
- Use of only titanium MIs (Ti6Al4V): As a result, the study does not offer a comparison between the various available materials, such as 316L, which could influence the clinical performance and long-term stability of MIs.
- (iv)
- Ideal insertion and loading conditions: The study assumed that MI insertion was performed under ideal conditions and that complete osseointegration (100%) was achieved. In clinical practice, insertion conditions vary, and osseointegration may not always be complete, which could affect the performance of implants.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malik, F.; Khan, F.; Ali, S.; Rana, F.; Haq, H.; Hussain, M. Factors affecting success and failure of orthodontic mini-implants: A retrospective review. Prof. Med. J. 2023, 30, 285–291. [Google Scholar]
- Ravi, J.; Duraisamy, S.; Rajaram, K.; Kannan, R.; Arumugam, E. Survival rate and stability of surface-treated and non-surface-treated orthodontic mini-implants: A randomized clinical trial. Dent. Press. J. Orthod. 2023, 28, e2321345. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.; Kim, J.; Lee, N.; Kim, Y.; Lee, J.; Kim, T. Analysis of time to failure of orthodontic mini-implants after insertion or loading. J. Korean Assoc. Oral Maxillofac. Surg. Surg. 2015, 41, 240. [Google Scholar] [CrossRef] [PubMed]
- Popa, A.; Dehelean, C.; Călniceanu, H.; Watz, C.; Brad, S.; Sinescu, C.; Szuhanek, C. A custom-made orthodontic mini-implant—Effect of insertion angle and cortical bone thickness on stress distribution with a complex in vitro and in vivo biosafety profile. Materials 2020, 13, 4789. [Google Scholar] [CrossRef]
- Singh, J.; Singh, S.; Gupta, A. Comparative evaluation of primary stability of two different types of orthodontic mini-implants. J. Pharm. Bioallied Sci. 2021, 13, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Dutta, S.; Bhat, J. Orthodontic mini implant and their primary stability: A comparative study. Int. J. Appl. Dent. Sci. 2022, 8, 642–644. [Google Scholar] [CrossRef]
- Arqub, S.A.; Gandhi, V.; Mehta, S.; Palo, L.; Upadhyay, M.; Yadav, S. Survival estimates and risk factors for failure of palatal and buccal mini-implants. Angle Orthod. 2021, 91, 756–763. [Google Scholar] [CrossRef] [PubMed]
- Filipová, D.; Filipi, V.; Kamínek, M. Proclination-induced changes in the labial cortical bone thickness of lower incisors. Bratisl. Med. J. 2019, 120, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Kovuru, V. Factorial analysis of variables affecting bone stress adjacent to mini-implants used for molar distalization by direct anchorage—A finite element study. J. Orthod. Sci. 2023, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Son, E.; Kim, S.; Hong, C.; Chan, V.; Sim, H.; Ji, S.; Chae, H. A study on the morphologic change of palatal alveolar bone shape after intrusion and retraction of maxillary incisors. Sci. Rep. 2020, 10, 14454. [Google Scholar] [CrossRef] [PubMed]
- Thongudomporn, U.; Charoemratrote, C.; Jearapongpakorn, S. Changes of anterior maxillary alveolar bone thickness following incisor proclination and extrusion. Angle Orthod. 2014, 85, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.; Liu, P.; Tseng, Y.; Chou, S.; Wu, C.; Chang, H. Effects of cortical bone thickness and trabecular bone density on primary stability of orthodontic mini-implants. J. Dent. Sci. 2019, 14, 383–388. [Google Scholar] [CrossRef]
- Yu, W.; Tsai, M.; Yu, J.; Huang, H.; Hsu, J. Bone quality affects stability of orthodontic miniscrews. Sci. Rep. 2022, 12, 2849. [Google Scholar] [CrossRef]
- Centeno, A.; Fensterseifer, C.; Chami, V.; Ferreira, E.; Marquezan, M.; Ferrazzo, V. Correlation between cortical bone thickness at mini-implant insertion sites and age of patient. Dent. Press J. Orthod. 2022, 27, e222098. [Google Scholar] [CrossRef] [PubMed]
- Marquezan, M.; Mattos, C.; Sant’Anna, E.; Souza, M.; Maia, L. Does cortical thickness influence the primary stability of miniscrews?:a systematic review and meta-analysis. Angle Orthod. 2014, 84, 1093–1103. [Google Scholar] [CrossRef] [PubMed]
- Hatia, A.; Doldo, T.; Parrini, S.; Chisci, E.; Cipriani, L.; Montagna, L.; Lagana, G.; Guenza, G.; Agosta, E.; Vinjolli, F.; et al. Accuracy and Completeness of ChatGPT-Generated Information on Interceptive Orthodontics: A Multicenter Collaborative Study. J. Clin. Med. 2024, 27, 735. [Google Scholar] [CrossRef] [PubMed]
- Sant’Anna, E.F.; Araújo, M.T.S.; Nojima, L.I.; Cunha, A.C.D.; Silveira, B.L.D.; Marquezan, M. High-intensity laser application in Orthodontics. Dent. Press J. Orthod. 2017, 22, 99–109. [Google Scholar] [CrossRef]
- Weir, T. Clear aligners in orthodontic treatment. Aust. Dent. J. 2017, 62 (Suppl. S1), 58–62. [Google Scholar] [CrossRef] [PubMed]
- Rito-Macedo, F.; Barroso-Oliveira, M.; Paranhos, L.R.; Rodrigues-Brum, J.; Pereira-Lima, I.F.; Gomes-França, F.M.; de Brito-Junior, R.B. Implant insertion angle and depth: Peri-implant bone stress analysis by the finite element method. J. Clin. Exp. Dent. 2021, 10, 1167–1173. [Google Scholar] [CrossRef] [PubMed]
- Panaite, T.; Savin, C.; Olteanu, N.D.; Karvelas, N.; Romanec, C.; Vieriu, R.M.; Balcos, C.; Baltatu, M.S.; Benchea, M.; Achitei, D.; et al. Heat treatment’s vital role: Elevating orthodontic mini-implants for superior performance and longevity—Pilot study. Dent. J. 2024, 12, 103. [Google Scholar] [CrossRef]
- Cozzani, M.; Pasini, M.; Zallio, F.; Ritucci, R.; Mutinelli, S.; Mazzotta, L.; Giuca, M.R.; Piras, V. Comparison of maxillary molar distalization with an implant-supported distal jet and a traditional tooth-supported distal jet appliance. Int. J. Dent. 2014, 10, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Benaissa, A.; Merdji, A.; Bendjaballah, M.Z.; Ngan, P.; Mukdadi, O.M. Stress influence on orthodontic system components under simulated treatment loadings Comput. Methods Programs Biomed. 2020, 10, 195–210. [Google Scholar]
- ASME Elliptical. Available online: https://www.asme.org/ (accessed on 1 June 2024).
- Ghorab, H. Finite element study to evaluate the stress around mini-implant during canine retraction using continuous and interrupted orthodontic forces. Open Access Maced. J. Med. Sci. 2023, 11, 36–43. [Google Scholar] [CrossRef]
- Alrbata, R.; Momani, M.; Al-Tarawneh, A.; Ihyasat, A. Optimal force magnitude loaded to orthodontic microimplants: A finite element analysis. Angle Orthod. 2015, 86, 221–226. [Google Scholar] [CrossRef]
- Nienkemper, M.; Handschel, J.; Drescher, D. Systematic review of mini-implant displacement under orthodontic loading. Int. J. Oral Sci. 2013, 6, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Klein, C.P.; van der Waerden, J. The effect of osseointegration on the mechanical stability of dental implants: A finite element analysis. J. Biomech. 2015, 48, 1–7. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material/Component | Elastic Modulus (MPa) | Poisson’s Ratio | |
|---|---|---|---|
| Bracket | 380,000 | 0.19 | |
| Mini-Implant | 110,000 | 200,000 | 0.3 |
| Tooth | 84,100 | 0.2 | |
| PDL | 68.9 | 0.45 | |
| Cortical bone | 17,000 | 0.3 | |
| Spongy bone | 350 | 0.25 | |
| FEA Parameter | Property |
|---|---|
| Property discretization (nodes/elements) | 356,422/229,672 |
| Element | 10 node tetrahedron |
| Software | ANSYS Workbench 19.2, Canonsburg, PA, USA |
| Material model | Isotropic, homogeneous, linear |
| Contact model | Friction (nonlinear, friction coefficient = 0 between mini-implant and bones), bonded (linear) |
| Loading | Oblique (0.1–10 N) (30°, 45°, 60°) |
| Mini-implant type | Threaded, diameter: 2.0 mm, 12.0 mm length |
| Boundary conditions | 100% osseointegration |
| Parameter | 2 N Force | 10 N Force |
|---|---|---|
| Endurance (operating cycles) | 4.445 × 105 cycles | 1546 cycles (287.48 times lower) |
| Volume of material affected | Small volume of material | Larger volume of material |
| Minimum fatigue safety factor | 0.86863 (located at most stressed node) | 0.17704 (located at most stressed node) |
| Maximum stress concentration | 2250 MPa (2.5× higher than the rest of the material) | 6.468 × 105 MPa (646.8× higher than the rest of the material) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panaite, T.; Savin, C.; Olteanu, N.D.; Romanec, C.L.; Vieriu, R.-M.; Balcos, C.; Chehab, A.; Zetu, I.N. Balancing the Load: How Optimal Forces Shape the Longevity and Stability of Orthodontic Mini-Implants. Dent. J. 2025, 13, 71. https://doi.org/10.3390/dj13020071
Panaite T, Savin C, Olteanu ND, Romanec CL, Vieriu R-M, Balcos C, Chehab A, Zetu IN. Balancing the Load: How Optimal Forces Shape the Longevity and Stability of Orthodontic Mini-Implants. Dentistry Journal. 2025; 13(2):71. https://doi.org/10.3390/dj13020071
Chicago/Turabian StylePanaite, Tinela, Carmen Savin, Nicolae Daniel Olteanu, Cristian Liviu Romanec, Raluca-Maria Vieriu, Carina Balcos, Alice Chehab, and Irina Nicoleta Zetu. 2025. "Balancing the Load: How Optimal Forces Shape the Longevity and Stability of Orthodontic Mini-Implants" Dentistry Journal 13, no. 2: 71. https://doi.org/10.3390/dj13020071
APA StylePanaite, T., Savin, C., Olteanu, N. D., Romanec, C. L., Vieriu, R.-M., Balcos, C., Chehab, A., & Zetu, I. N. (2025). Balancing the Load: How Optimal Forces Shape the Longevity and Stability of Orthodontic Mini-Implants. Dentistry Journal, 13(2), 71. https://doi.org/10.3390/dj13020071