
Clinical Factors on Dental Implant Fractures: A Systematic Review

 ,
,  ,
,  ,
, 

Abstract
1. Introduction
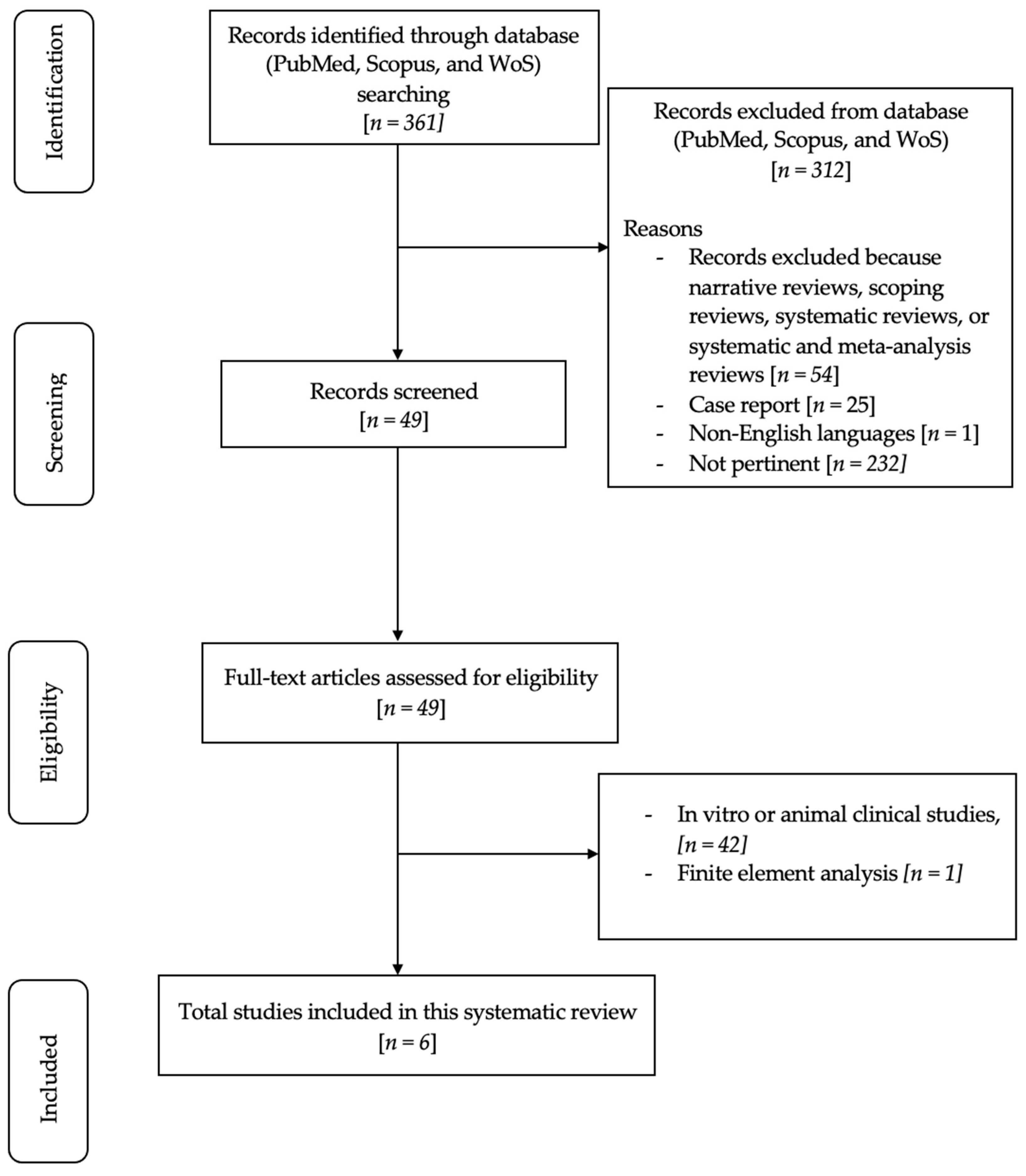
2. Materials and Methods
2.1. Focused Question
2.2. Eligibility Criteria
2.3. Search Strategy
2.4. Research
2.5. Data Extraction
2.6. Quality Assessment of Included Studies
3. Results
- Implant Characteristics: Diameter, Length, Design, Material, Cervical Feature, Microthread, Platform Switching, Connection Type;
- Patient Demographics: Age, Biological Sex;
- Surgical and Prosthetic Variables: Position in Jaw, Bone Characteristics, Timing;
- Prosthesis Characteristics: Type of Prosthesis, Type of Retention, Material of Prosthesis;
- Biomechanical and Functional Factors: Alignment, Jaw Relation, Functional Duration, Marginal Bone Loss, GBR, Screw Loosening, Screw Fracture, Fractured Implant Bodies;
- Clinical and Procedural Variables: Type of Abutment, Type of Implant-Abutment Connection, Healing Type, Opposing Tooth Type;
- Complications and Maintenance: Loosening and Fracture of Abutment Screws, Fractured Implant Bodies, Time of Onset of Complication.
Risk of Bias
4. Discussion
4.1. Implant Diameter and Structural Resistance Correlation
4.2. Implant Position and Impact on IF Incidence
4.3. Influence of Implant Design and Material on Fracture Risk
4.4. Impact of Prosthesis Type on Dental Implant Fractures
4.5. Biomechanical Overload as a Significant Factor in Dental Implant Fractures
4.6. Crucial Role of Implant-Abutment Connection in Dental Implant Performance
4.7. Peri-Implant Bone Loss and Regeneration Procedures
4.8. Biological Sex, Surgical Expertise, and Other Parameters
4.9. Limitations and Future Studies
4.10. Result Summary Table
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CSR | Cumulative Survival Rate |
| FDPs | Fixed Dental Prostheses |
| FEA | Finite Element Analysis |
| GBR | Guided Bone Regeneration |
| IF | Implant Fracture |
| ISQ | Implant Stability Quotient (ISQ) |
| MeSH | Medical Subject Headings |
| NHLBI | National Heart, Lung, and Blood Institute |
| PCC | Population–Concept–Context |
| RCTs | Randomized Controlled Trials |
| ROBINS-I | Risk Of Bias in Non-Randomized Studies of Interventions |
| SEM | Scanning Electron Microscopic |
| WoS | Web of Science |
References
- Lini, F.; Poli, P.P.; Beretta, M.; Cortinovis, I.; Maiorana, C. Long-term retrospective observational cohort study on the survival rate of stepped screw titanium implants followed up to 20 years. Int. J. Oral Maxillofac. Implants. 2019, 34, 999–1006. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Persson, G.R.; Pirih, F.Q.; Camargo, P.M. Peri-implant health, peri-implant mucositis, and peri-implantitis: Case definitions and diagnostic considerations. J. Clin. Periodontol. 2018, 45, S278–S285. [Google Scholar] [CrossRef] [PubMed]
- Poli, P.P.; de Miranda, F.V.; Polo, T.O.B.; Santiago Júnior, J.F.; Lima Neto, T.J.; Rios, B.R.; Assunção, W.G.; Ervolino, E.; Maiorana, C.; Faverani, L.P. Titanium Allergy Caused by Dental Implants: A Systematic Literature Review and Case Report. Materials 2021, 14, 5239. [Google Scholar] [CrossRef] [PubMed]
- Tey, V.H.S.; Phillips, R.; Tan, K. Five-year retrospective study on success, survival and incidence of complications of single crowns supported by dental implants. Clin. Oral Implants Res. 2017, 28, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Jin, S.Y.; Kim, S.G.; Oh, J.S.; You, J.S.; Jeong, M.A. Incidence and management of fractured dental implants: Case reports. Implant Dent. 2017, 26, 802–806. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, M.; Meyer, S.; Mombelli, A.; Muller, F. Dental implants in the elderly population: A systematic review and meta-analysis. Clin. Oral Implants Res. 2017, 28, 920–930. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.R.; Kisch, J.; Albrektsson, T.; Wennerberg, A. Bruxism and dental implant failures: A multilevel mixed effects parametric survival analysis approach. J. Oral Rehabil. 2016, 43, 813–823. [Google Scholar] [CrossRef] [PubMed]
- Verma, A.; Singh, S.V.; Arya, D.; Shivakumar, S.; Chand, P. Mechanical failures of dental implants and supported prostheses: A systematic review. J. Oral Biol. Craniofac. Res. 2023, 13, 306–314. [Google Scholar] [CrossRef]
- Nayana, P.; Nayak, S.S.; Chatterjee, A.; Sivaraman, K.; Srikanth, G.; Singh, C. Retrieval of Fractured Implant Abutment Screws: A Narrative Review. J. Int. Soc. Prev. Community Dent. 2022, 12, 287–294. [Google Scholar]
- Attard, L.; Lee, V.; Le, J.; Lowe, C.; Singh, V.; Zhao, J.; Sharma, D. Mechanical Factors Implicated in Zirconia Implant Fracture Placed within the Anterior Region-A Systematic Review. Dent. J. 2022, 10, 22. [Google Scholar] [CrossRef]
- Aromataris, E.; Munn, Z. JBI Manual for Evidence Synthesis. 2020. Available online: https://synthesismanual.jbi.global (accessed on 12 January 2024).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- National Heart, Lung, and Blood Institute. Study Quality Assessment Tool. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 12 January 2024).
- Bufalá Pérez, M.; Zubizarreta-Macho, Á.; Borrajo Sánchez, J.; Hernández Rodríguez, J.; Alonso Pérez-Barquero, J.; Riad Deglow, E.; Hernández Montero, S. Removal capability, implant-abutment connection damage and thermal effect using ultrasonic and drilling techniques for the extraction of fractured abutment screws: An in vitro study. BMC Oral Health 2022, 221, 603. [Google Scholar] [CrossRef] [PubMed]
- Gehrke, S.A.; Dedavid, B.A.; Prados-Frutos, J.C. Effects of different switched or not-switched implant and abutment platform designs and marginal bone loss on fracture strength: An in vitro study. J. Prosthet. Dent. 2022, 128, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Khorshidparast, S.; Akhlaghi, P.; Rouhi, G.; Barikani, H. Measurement of bone damage caused by quasi-static compressive loading-unloading to explore dental implants stability: Simultaneous use of in-vitro tests, μ-CT images, and digital volume correlation. J. Mech. Behav. Biomed. Mater. 2023, 138, 105566. [Google Scholar] [CrossRef] [PubMed]
- Leitão-Almeida, B.; Camps-Font, O.; Correia, A.; Mir-Mari, J.; Figueiredo, R.; Valmaseda-Castellón, E. Effect of crown to implant ratio and implantoplasty on the fracture resistance of narrow dental implants with marginal bone loss: An in vitro study. BMC Oral Health 2020, 20, 329. [Google Scholar] [CrossRef] [PubMed]
- Jorio, I.C.; Stawarczyk, B.; Attin, T.; Schmidlin, P.R.; Sahrmann, P. Reduced fracture load of dental implants after implantoplasty with different instrumentation sequences. An in vitro study. Clin. Oral Implants Res. 2021, 32, 881–892. [Google Scholar] [CrossRef] [PubMed]
- Aramburú, J.S.; Gehrke, S.A.; Dedavid, B.A.; Treichel, T.L.E.; Pippi, N.L. Correlation of Fracture Resistance of Dental Implants and Bite Force in Dogs described in the literature: An In VitroStudy. J. Vet. Dent. 2021, 38, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Bordin, D.; Bergamo, E.T.P.; Fardin, V.P.; Coelho, P.G.; Bonfante, E.A. Fracture strength and probability of survival of narrow and extra-narrow dental implants after fatigue testing: In vitro and in silico analysis. J. Mech. Behav. Biomed. Mater. 2021, 71, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Ko, K.H.; Park, C.J.; Cho, L.R.; Huh, Y.H. Connector design effects on the in vitro fracture resistance of 3-unit monolithic prostheses produced from 4 CAD-CAM materials. J. Prosthet. Dent. 2022, 128, 1319.e1–1319.e10. [Google Scholar] [CrossRef]
- Streckbein, P.; Wilbrand, J.F.; Kähling, C.; Pons-Kühnemann, J.; Rehmann, P.; Wöstmann, B.; Howaldt, H.P.; Möhlhenrich, S.C. Evaluation of the surface damage of dental implants caused by different surgical protocols: An in vitro study. Int. J. Oral Maxillofac. Surg. 2019, 48, 971–981. [Google Scholar] [CrossRef]
- Burkhardt, F.; Spies, B.C.; Riemer, L.; Adolfsson, E.; Doerken, S.; Kohal, R.J. Fracture resistance and crystal phase transformation of a one- and a two-piece zirconia implant with and without simultaneous loading and aging-An in vitro study. Clin. Oral Implants Res. 2021, 32, 1288–1298. [Google Scholar] [CrossRef] [PubMed]
- Gehrke, S.A.; Bonachela, W.C.; Lopes Moreno, J.M.; Orlato Rossetti, P.H.; Cortellari, G.C.; Dedavid, B.A.; Calvo-Guirado, J.L. Zirconium Oxide Three-Unit Fixed Partial Denture Frameworks Supported by Dental Implants in Acceptable and Reduced Interocclusal Space Possibilities: Pilot In Vitro Fracture Strength and Fractographic Analyses. Int. J. Oral Maxillofac. Implants 2019, 34, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Agustín-Panadero, R.; Baixauli-López, M.; Gómez-Polo, M.; Cabanes-Gumbau, G.; Senent-Vicente, G.; Roig-Vanaclocha, A. In vitro comparison of the efficacy of two fractured implant-prosthesis screw extraction methods: Conventional versus mechanical. J. Prosthet. Dent. 2020, 124, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Leitão-Almeida, B.; Camps-Font, O.; Correia, A.; Mir-Mari, J.; Figueiredo, R.; Valmaseda-Castellón, E. Effect of bone loss on the fracture resistance of narrow dental implants after implantoplasty. An in vitro study. Med. Oral Patol. Oral Cir. Bucal. 2021, 26, e611–e618. [Google Scholar] [CrossRef] [PubMed]
- Bauer, R.; Zacher, J.; Strasser, T.; Rosentritt, M. In vitro performance and fracture resistance of interim conventional or CAD-CAM implant-supported screw- or cement-retained anterior fixed partial dentures. J. Prosthet. Dent. 2021, 126, 575–580. [Google Scholar] [CrossRef]
- Foong, J.K.; Judge, R.B.; Palamara, J.E.; Swain, M.V. Fracture resistance of titanium and zirconia abutments: An in vitro study. J. Prosthet. Dent. 2013, 109, 304–312. [Google Scholar] [CrossRef] [PubMed]
- El-Mahdy, M.; Aboelfadl, A.; Ahmed, F.; El-Banna, A.; Wahsh, M. Strain gauge analysis and fracture resistance of implant-supported PEKK hybrid abutments restored with two crown materials: An in vitro study. Dent. Med. Probl. 2023, 60, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Kono, K.; Kurihara, D.; Suzuki, Y.; Ohkubo, C. In vitro assessment of mandibular single/two implant-retained overdentures using stress-breaking attachments. Implant. Dent. 2014, 23, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Asl, H.G.; Alsaran, A. In vitro comparison of commercial and ultrafine-grained titanium osteosynthesis miniplates used on mandibular fractures. Dent. Med. Probl. 2020, 57, 351–358. [Google Scholar] [PubMed]
- Emam, M.; Arafa, A.M. Stress distribution and fracture resistance of green reprocessed polyetheretherketone (PEEK) single implant crown restorations compared to unreprocessed PEEK and Zirconia: An in-vitro study. BMC Oral Health 2023, 23, 275. [Google Scholar] [CrossRef]
- Igarashi, K.; Afrashtehfar, K.I.; Schimmel, M.; Gazzaz, A.; Brägger, U. Performance of a repair service set for the retrieval of fractured abutment screws: A pilot in vitro study. Int. J. Oral Maxillofac. Implants 2019, 34, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Freitas, D.Q.; Vasconcelos, T.V.; Noujeim, M. Diagnosis of vertical root fracture in teeth close and distant to implant: An in vitro study to assess the influence of artifacts produced in cone beam computed tomography. Clin. Oral Investig. 2019, 23, 1263–1270. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Z.; Nakano, T.; Chen, Y.; Watanabe, S.; Matsuoka, T.; Ishigaki, S. Implant deformation and implant-abutment fracture resistance after standardized artificial aging: An in vitro study. Clin. Implant. Dent. Relat. Res. 2023, 25, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Vult von Steyern, P.; Kokubo, Y.; Nilner, K. Use of abutment-teeth vs. dental implants to support all-ceramic fixed partial dentures: An in-vitro study on fracture strength. Swed. Dent. J. 2005, 29, 53–60. [Google Scholar] [PubMed]
- Gehrke, S.A.; Souza Dos Santos Vianna, M.; Dedavid, B.A. Influence of bone insertion level of the implant on the fracture strength of different connection designs: An in vitro study. Clin. Oral Investig. 2014, 18, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Chong, K.K.; Palamara, J.; Wong, R.H.; Judge, R.B. Fracture force of cantilevered zirconia frameworks: An in vitro study. J. Prosthet. Dent. 2014, 112, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Kohal, R.J.; Wolkewitz, M.; Tsakona, A. The effects of cyclic loading and preparation on the fracture strength of zirconium-dioxide implants: An in vitro investigation. Clin. Oral Implants Res. 2011, 22, 808–814. [Google Scholar] [CrossRef] [PubMed]
- Bein, L.; Rauch, A.; Schmidt, M.; Rosentritt, M. In vitro fatigue and fracture testing of temporary materials from different manufacturing processes in implant-supported anterior crowns. Clin. Oral Investig. 2023, 27, 4215–4224. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Cai, P.; Zhuo, Y.; Lin, L.; Zheng, Z. Effect of abutment design on fracture resistance of resin-matrix ceramic crowns for dental implant restoration: An in vitro study. BMC Oral Health 2023, 23, 410. [Google Scholar] [CrossRef]
- Rues, S.; Kappel, S.; Ruckes, D.; Rammelsberg, P.; Zenthöfer, A. Resistance to Fracture in Fixed Dental Prostheses Over Cemented and Screw-Retained Implant-Supported Zirconia Cantilevers in the Anterior Region: An In Vitro Study. Int. J. Oral Maxillofac. Implants 2020, 35, 521–529. [Google Scholar] [CrossRef]
- Katsavochristou, A.; Sierraalta, M.; Saglik, B.; Koumoulis, D.; George, F.; Razzoog, M. Implant Angulation Effect on the Fracture Resistance of Monolithic Zirconia Custom Abutments: An In Vitro Study. J. Prosthodont. 2020, 29, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Vahnström, M.; Johansson, P.H.; Svanborg, P.; Stenport, V.F. Comparison of porcelain veneer fracture in implant-supported fixed full-arch prostheses with a framework of either titanium, cobalt-chromium, or zirconia: An in vitro study. Clin. Exp. Dent. 2022, 8, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Sailer, I.; Sailer, T.; Stawarczyk, B.; Jung, R.E.; Hämmerle, C.H. In vitro study of the influence of the type of connection on the fracture load of zirconia abutments with internal and external implant-abutment connections. Int. J. Oral Maxillofac. Implants 2009, 24, 850–858. [Google Scholar] [PubMed]
- Schmitter, M.; Rammelsberg, P.; Lenz, J.; Scheuber, S.; Schweizerhof, K.; Rues, S. Teeth restored using fiber-reinforced posts: In vitro fracture tests and finite element analysis. Acta Biomater. 2010, 6, 3747–3754. [Google Scholar] [CrossRef] [PubMed]
- Ghodsi, S.; Tanous, M.; Hajimahmoudi, M.; Mahgoli, H. Effect of aging on fracture resistance and torque loss of restorations supported by zirconia and polyetheretherketone abutments: An in vitro study. J. Prosthet. Dent. 2021, 125, 501.e1–501.e6. [Google Scholar] [CrossRef] [PubMed]
- Gehrke, S.A. Importance of Crown Height Ratios in Dental Implants on the Fracture Strength of Different Connection Designs: An In Vitro Study. Clin. Implant Dent. Relat. Res. 2015, 17, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Giner, S.; Bartolomé, J.F.; Gomez-Cogolludo, P.; Castellote, C.; Pradíes, G. Fatigue fracture resistance of titanium and chairside CAD-CAM zirconia implant abutments supporting zirconia crowns: An in vitro comparative and finite element analysis study. J. Prosthet. Dent. 2021, 125, 503.e1–503.e9. [Google Scholar] [CrossRef]
- Wilmes, B.; Panayotidis, A.; Drescher, D. Fracture resistance of orthodontic mini-implants: A biomechanical in vitro study. Eur. J. Orthod. 2011, 33, 396–401. [Google Scholar] [CrossRef]
- Att, W.; Kurun, S.; Gerds, T.; Strub, J.R. Fracture resistance of single-tooth implant-supported all-ceramic restorations: An in vitro study. J. Prosthet. Dent. 2006, 95, 111–116. [Google Scholar] [CrossRef]
- Moorthy, A.; Aljudaibi, S.; Donnelly-Swift, E.; Polyzois, I.; Grufferty, B. An in vitro evaluation of 2 methods for retrieving fractured abutment screw fragments from the intaglio of 4 different implant systems. J. Prosthet. Dent. 2022, 131, 282–290. [Google Scholar] [CrossRef]
- Coppedê, A.R.; Bersani, E.; de Mattos, M.D.G.C.; Rodrigues, R.C.; Sartori, I.A.; Ribeiro, R.F. Fracture resistance of the implant-abutment connection in implants with internal hex and internal conical connections under oblique compressive loading: An in vitro study. Int. J. Prosthodont. 2009, 22, 283–286. [Google Scholar] [PubMed]
- Patankar, A.; Kheur, M.; Kheur, S.; Lakha, T.; Burhanpurwala, M. Fracture Resistance of Implant Abutments Following Abutment Alterations by Milling the Margins: An In Vitro Study. J. Oral Implantol. 2016, 42, 464–468. [Google Scholar] [CrossRef] [PubMed]
- Bhagat, J.A.; Naganathan, V.; Krishnan, L.; Raj, D.; Prakash, R. Development of a new V-shaped implant with locking plates and screws for mandibular fracture fixation: An in vitro study using finite element analysis. Br. J. Oral Maxillofac. Surg. 2019, 57, 805–807. [Google Scholar] [CrossRef] [PubMed]
- Takeshita, K.; Toia, M.; Jinno, Y.; Sumi, T.; Takahashi, T.; Halldin, A.; Jimbo, R. Implant Vertical Fractures Provoked by Laboratory Procedures: A Finite Element Analysis Inspired from Clinical Cases. Implant. Dent. 2016, 25, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Gahlert, M.; Burtscher, D.; Grunert, I.; Kniha, H.; Steinhauser, E. Failure analysis of fractured dental zirconia implants. Clin. Oral Implants Res. 2012, 23, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Cha, H.S.; Kim, Y.S.; Jeon, J.H.; Lee, J.H. Cumulative survival rate and complication rates of single-tooth implant; focused on the coronal fracture of fixture in the internal connection implant. J. Oral Rehabil. 2013, 40, 595–602. [Google Scholar] [CrossRef]
- Tabrizi, R.; Behnia, H.; Taherian, S.; Hesami, N. What Are the Incidence and Factors Associated With Implant Fracture? J. Oral Maxillofac. Surg. 2017, 75, 1866–1872. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, Y.T.; Jeong, S.N.; Kim, N.H.; Lee, D.W. Incidence and pattern of implant fractures: A long-term follow-up multicenter study. Clin. Implant Dent. Relat. Res. 2018, 20, 463–469. [Google Scholar] [CrossRef]
- Stoichkov, B.; Kirov, D. Analysis of the causes of dental implant fracture: A retrospective clinical study. Quintessence Int. 2018, 49, 279–286. [Google Scholar]
- Lee, D.W.; Kim, N.H.; Lee, Y.; Oh, Y.A.; Lee, J.H.; You, H.K. Implant fracture failure rate and potential associated risk indicators: An up to 12-year retrospective study of implants in 5,124 patients. Clin. Oral Implants Res. 2019, 30, 206–217. [Google Scholar] [CrossRef]
- Gonçalves, G.S.Y.; de Magalhães, K.M.F.; Rocha, E.P.; Dos Santos, P.H.; Assunção, W.G. Oral health-related quality of life and satisfaction in edentulous patients rehabilitated with implant-supported full dentures all-on-four concept: A systematic review. Clin. Oral Investig. 2022, 26, 83–94. [Google Scholar] [CrossRef] [PubMed]
- Sailer, I.; Karasan, D.; Todorovic, A.; Ligoutsikou, M.; Pjetursson, B.E. Prosthetic failures in dental implant therapy. Periodontol. 2000 2022, 88, 130–144. [Google Scholar] [CrossRef] [PubMed]
- Gealh, W.C.; Mazzo, V.; Barbi, F.; Camarini, E.T. Osseointegrated implant fracture: Causes and treatment. J. Oral Implantol. 2011, 37, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Geng, J.; Jones, D.; Xu, W. Comparison of the fracture resistance of dental implants with different abutment taper angles. Mater. Sci. Eng. C Mater Biol. Appl. 2016, 63, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Stavropoulos, A.; Bertl, K.; Eren, S.; Gotfredsen, K. Mechanical and biological complications after implantoplasty-A systematic review. Clin. Oral Implants Res. 2019, 30, 833–848. [Google Scholar] [CrossRef] [PubMed]
- Costa-Berenguer, X.; García-García, M.; Sánchez-Torres, A.; Sanz-Alonso, M.; Figueiredo, R.; Valmaseda-Castellón, E. Effect of implantoplasty on fracture resistance and surface roughness of standard diameter dental implants. Clin. Oral Implants Res. 2018, 29, 46–54. [Google Scholar] [CrossRef]
- Camps-Font, O.; González-Barnadas, A.; Mir-Mari, J.; Figueiredo, R.; Gay-Escoda, C.; Valmaseda-Castellón, E. Fracture resistance after implantoplasty in three implant-abutment connection designs. Med. Oral Patol. Oral Cir. Bucal. 2020, 25, e691–e699. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Higgins, J.P.T.; Elbers, R.G.; Reeves, B.C.; The Development Group for ROBINS-I. Risk of Bias in Non-Randomized Studies of Interventions (ROBINS-I): Detailed Guidance, Updated 12 October 2016. Available online: http://www.riskofbias.info (accessed on 12 January 2024).

{kind=link}
|
|
|
|
| References (Authors, Year and Publication Country) | No. of Patients and Women (%) | Mean Age ± SD and/or Range (Years) | Inclusion and Exclusion Criteria | No. of Fixtures and Jaw Implant Position (%) | No. of Fractures and Jaw Implant Position (%) |
|---|---|---|---|---|---|
| Gahlert et al., 2012 Germany [57] | 79; N.R. | N.R. | Inclusion criteria: N.R. Exclusion criteria: N.R. | 170 N.R. | 13 Maxilla, 11 (84.62%) Mandible, 2 (15.38%) |
| Cha et al., 2013 South Korea [58] | 120; 63 (52.5%) | 47 (18.8–81.1) | Inclusion criteria: N.R. Exclusion criteria: N.R. | 136 Maxilla, 70 (51.5%) Mandible, 66 (48.5%) | 11 Maxilla, 3 (27.27%) Mandible, 8 (72.73%) |
| Tabrizi et al., 2017 Iran [59] | 6051; N.R. | N.R. | Inclusion criteria: missing teeth and dental implant treatment Exclusion criteria: dental implant fracture due to trauma | 18,700 N.R. | 37 Maxilla, 12 (32.43%) Mandible, 25 (67.57%) |
| Lee et al., 2018 South Korea [60] | 8501; 663 (7.80%) | 62.5 (27–81) | Inclusion criteria: N.R. Exclusion criteria: failure of initial and early osseointegration | 19,087 Maxilla, 8528 (44.7%) Mandible, 10,559 (56.3%) | 92 (only 70 analyzed) Maxilla, 32 (45.7%) Mandible, 38 (54.3%) |
| Stoichkov et al., 2018 Bulgaria [61] | 101; 46 (45.5%) | N.R. | Inclusion criteria: N.R. Exclusion criteria: N.R. | 218 Maxilla, 94 (43.12%) Mandible, 124 (56.88%) | 5 Maxilla, 2 (40.00%) Mandible, 3 (60.00%) |
| Lee et al., 2019 South Korea [62] | 5124; 554 (10.81%) | 63.15 ± 9.10 | Inclusion criteria: N.R. Exclusion criteria: inaccurate chart recordings, external or one-piece connection systems, supported removable prostheses, failure of initial or early osseointegration | 19,006 Maxilla, 9722 (51.15%) Mandible, 9284 (48.85%) | 174 Maxilla, 88 (50.57%) Mandible, 86 (49.43%) |
| Authors and Year of Publication | Study Design and Aim | Sample Analysis | Type of Implant | Predictive Variables | Results |
|---|---|---|---|---|---|
| Gahlert et al., 2012 [57] | A 36.75 ± 5.34-month retrospective cohort study with no control group aimed to evaluate the failure mechanism of 13 fractured dental zirconia implants by clinical, macroscopic, and scanning electron microscopic (SEM) methods. | Macroscopic, Light microscopy, SEM analysis. | Z-Look3 one-piece zirconia implants 3.25, 4, and 5 mm. | Diameter, implant position, implant alignment, jaw relation, time to failure. | Fracture incidence was approximately 10%; 12 of the 13 fractured implants had a diameter of 3.25 mm. All fractures occurred due to mechanical overloading (bending loads). Direction of crack propagation was always from the palatal position, lingual towards buccal. Macroscopic and light microscopic examinations offered no evidence that fracture of the implants occurred due to machining marks that might have been created for the connection of crowns or frameworks after implantation. SEM examinations confirmed that all fractures occurred due to singular bending overload (so-called forced rupture). |
| Cha et al., 2013 [58] | A 5-year retrospective cohort study with no control group aimed to evaluate the long-term cumulative survival rate (CSR) and complication rates of a 4.0 mm-diameter internal connection implant (MicrothreadTM OsseospeedTM) installed for single-tooth restoration. | Survival rates, complications. | MicroThread Osseospeed Astra Tech, 4.0-mm-diameter internal connection implant. | Implant position, biological sex, fixture length, timing of implant placement, type of healing, type of opposing tooth, type of abutment type of prosthesis retention material of prosthesis, most distal position. | The occurrence of complications was significantly related to implant position. The complication survival rates of the whole arch and the molar region were 91.9% and 87.6%, respectively, after 5 years of loading. Hence, the failure rate of the molar region was 12.4%. The CSR of the molar region was significantly lesser than that of the anterior and premolar regions (p = 0.037). |
| Tabrizi et al., 2017 [59] | A 14-year retrospective cohort study with no control group aimed to estimate the incidence of implant fractures and identify factors associated with fracture. | Survival rates, complications. | Not specified. | Demographic characteristics (age, biological sex), anatomy (location of implants), physical characteristic of implants (cylindrical or tapered, size, and shape), type of implant-abutment connection, type of prosthesis (single crown or multiple implants with fixed prosthesis or cantilever prosthesis), and type of retention (screw-retained or cement-retained prosthesis). | Tapered implants and screw-retained implants increased the HR in implant fracture. The incidence of implant fracture was higher in the molars and premolars than in the anterior of the jaws. Implant fracture occurred sooner in cantilevers, screw-retained crowns, and tapered fixtures. No difference was found among the four implant-abutment connections. A cantilever prosthesis significantly increases stress in the implant prosthesis, and this may lead to implant fracture due to fatigue. |
| Lee et al., 2018 [60] | A 9-year retrospective cohort study with no control group aimed to investigate the incidence of implant fractures (IF) and long-term follow-up of patients with multicenter collaboration to classify patterns of fracture and to evaluate related clinical factors. | Survival rates, complications. | Astra Tech [Osseo-Speed, Mannheim, Germany], BioHorizons [Maestro, Birmingham, USA], Bio-TIS [Spider, Seoul, Korea], Camlog Biotechnologies [Root-Line, Wimsheim, Germany], Damool Science [Damool, Daegu, Korea], Dentis [OneQ/Cleanant, Daegu, Korea], Osstem [GS/TS, Seoul, Korea], Nobel Biocare [Replace, Göteborg, Sweden], and Zimmer [TSV, Carls- bad, USA]. Materials that were 3.0–6.0 mm in diameter (narrow [<3.75 mm], standard [3.75–5.0 mm], wide [>5.0 mm]) and 9.0–13.0 mm in length (standard [9.0–13.0] and long [>13 mm]) were used for implant surgery. | Patient variables (sex and age) and implant variables (implant system, diameter, length, position in the jaw, placement location, prosthesis type, marginal bone loss, functional duration, guided bone regeneration [GBR], screw loosening, and screw fracture). | Fractures were observed in a total of nine different implant systems, with an incidence of 0.4%. Most stress caused by biomechanical overloading is focused on the cervical area. No difference in diameters (small diameters were only placed in anterior zones) was found between mandible and maxilla. Peri-implantitis-induced marginal and vertical bone loss and structural weakness of the specific designs were major factors in IF. |
| Stoichkov et al., 2018 [61] | A 3–10-year retrospective cohort study with no control group aimed to analyze the possible causative factors contributing to implant body fracture. | Survival rates, complications. | TBR Connect, Periosave-M, and Z1-M (TBR Implants Group), Ankylos (Dentsply Implants), and Straumann Bone Level Implants (Institut Straumann) 3.2 to 6 mm. | Available bone volume, location of the dental implants and their inclinations (mesiodistal and buccolingual), type of prosthetic restorations (i.e., single crowns, splinted crowns, implant-supported fixed dental prostheses [FDPs], and tooth-implant-supported FDPs]), presence of cantilever extensions, type of connection between the implant and the abutment, size of the used diameters, degree of crestal resorption, loosening and fracture of the abutment screws, fractured implant bodies, as well as the time of onset of the complication. | Occlusal overload due to bruxism or to inappropriate or inadequate occlusion as single factors or a combination of these factors during the first years after the functional load can cause implant fracture. Fracture of the implant body more frequently occurred with single crowns than with other implant-supported FDPs. |
| Lee et al., 2019 [62] | A 12-year retrospective cohort study with no control group aimed to determining the fracture rate and risk indicator of internal connection implants installed in a single center. | Survival rates, complications. | Internal connection implants. | Age and sex of the patient; length of the fixture, diameter of the fixture, location of the implant, bone graft (presence or absence); fixture material (commercially pure titanium Grade 4 or titanium–aluminum–vanadium (Ti-6Al-4V)); cervical feature (polished or unpolished); type of implant connection (butt joint or conical joint); microthread (presence or absence); and platform switching (presence or absence). Dates for fixture installation, prosthesis delivery, and final visit. | Wide-diameter implants had a lower risk of fracture than narrow or regular-diameter implants; the absence of microthreads or bone grafts led to a higher risk of fracture than the presence of these features; the mandibular anterior area had a lower risk of fracture than other sites. |
| Influencing Factor | Key Findings |
|---|---|
| Implant Diameter |
|
| Implant Position |
|
| Implant Design and Material |
|
| Prosthesis Type |
|
| Biomechanical Overload |
|
| Implant-Abutment Connection |
|
| Peri-implant Bone Loss |
|
| Biological Sex and Expertise |
|
| Other Parameters |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manfredini, M.; Poli, P.P.; Giboli, L.; Beretta, M.; Maiorana, C.; Pellegrini, M. Clinical Factors on Dental Implant Fractures: A Systematic Review. Dent. J. 2024, 12, 200. https://doi.org/10.3390/dj12070200
Manfredini M, Poli PP, Giboli L, Beretta M, Maiorana C, Pellegrini M. Clinical Factors on Dental Implant Fractures: A Systematic Review. Dentistry Journal. 2024; 12(7):200. https://doi.org/10.3390/dj12070200
Chicago/Turabian StyleManfredini, Mattia, Pier Paolo Poli, Luca Giboli, Mario Beretta, Carlo Maiorana, and Matteo Pellegrini. 2024. "Clinical Factors on Dental Implant Fractures: A Systematic Review" Dentistry Journal 12, no. 7: 200. https://doi.org/10.3390/dj12070200
APA StyleManfredini, M., Poli, P. P., Giboli, L., Beretta, M., Maiorana, C., & Pellegrini, M. (2024). Clinical Factors on Dental Implant Fractures: A Systematic Review. Dentistry Journal, 12(7), 200. https://doi.org/10.3390/dj12070200