Proposal of a New Therapeutic Classification in Gingival Smiles Focused on Treatment with Semi-Permanent Infiltrations

 ,
,  ,
, 

Abstract
1. Introduction
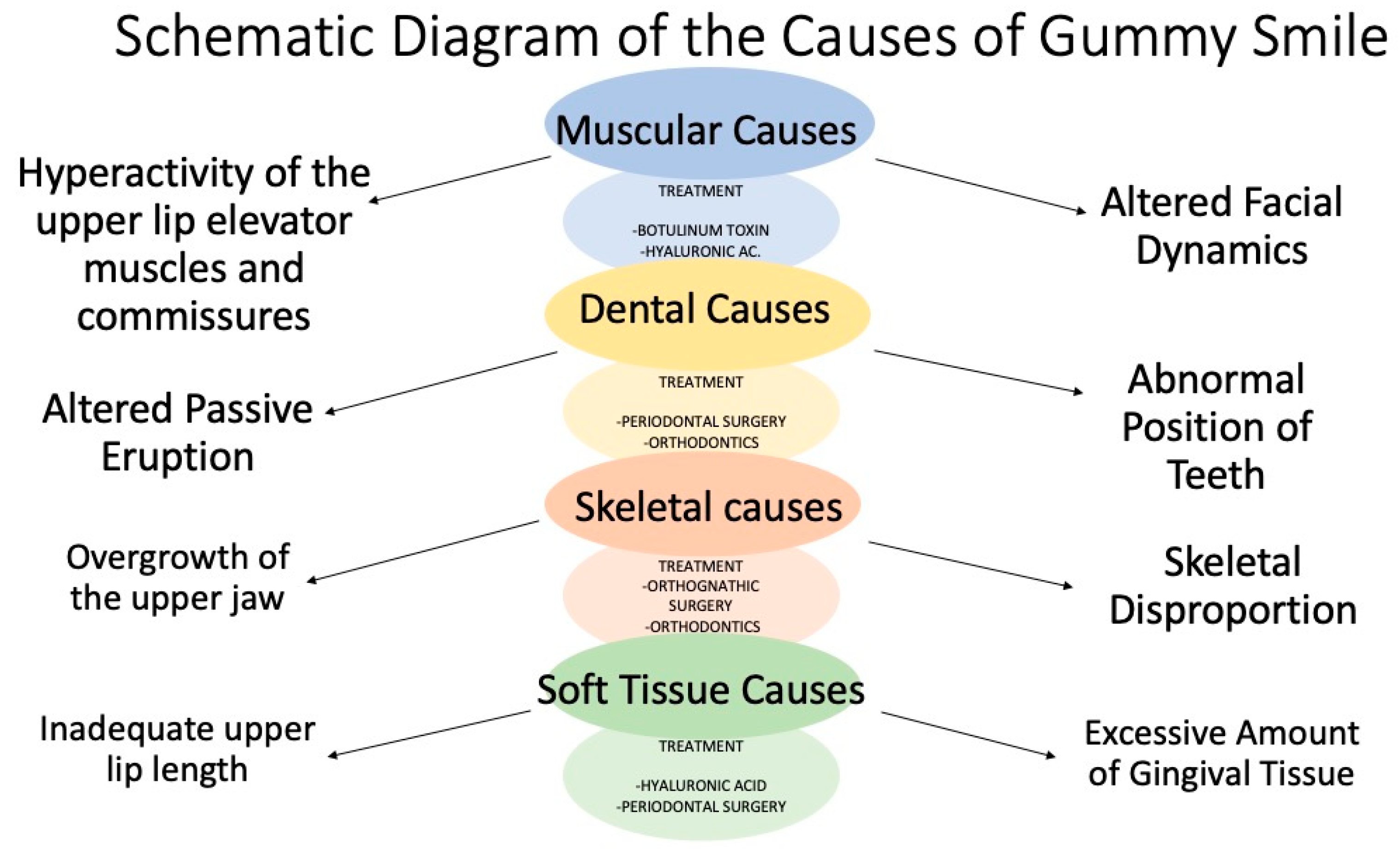
2. Etiology
3. Classifications
4. Proposed Classification of the Gingival Smile with a Focus on Semi-Permanent Infiltration Treatment
- Type 1.—Upper lip vermilion red refinement.
- Type 2.—Loss or lack of bone and fat volume.
- a.
- Upper jaw.
- b.
- Piriform fossa.
- c.
- Chin.
- Type 3.—Muscle hypermobility.
- a.
- Lift muscle of the upper lip and wing of the nose (LLSAN).
- b.
- Levator labii superioris muscle (LLS).
- c.
- Nasal septal depressor muscle (myrtiformis).
- d.
- Zygomaticus major (ZM) and zygomaticus minor (Zm) muscles.
- Type 1.—Upper lip vermilion red refinement
- Type 2.—Loss or lack of bone and fat volume
- a.
- Upper jaw: lack of bony projection and fat volume of the medial and nasolabial compartment.
- b.
- Piriform fossa: lack of bony projection in the canine fossa.
- c.
- Chin: Lack of bony projection and fatty volume of the mentonian compartment.
- Type 3.—Muscle hypermobility
- a.
- LLSAN: this subcategory focuses on the action of the levator labii superioris and ala nasalis (LLSAN) muscles in the excessive elevation of the lips during smiling, which can result in increased gum exposure.
- b.
- Levator labii superioris (LLS) muscle: similar to above, but also involves the levator labii superioris (LLS).
- c.
- Nasal septal depressor muscle (myrtiformis): here, we consider the influence of the nasal septum or myrtiformis muscle and the levator muscles of the upper lip and ala of the nose, together with the orbicularis on the mobility of the lips, tip of the nose, and gingival exposure.
- d.
- Zygomaticus major (ZM) and zygomaticus minor (Zm) muscles: we explored how traction of the zygomaticus muscles can contribute to a wide gingival smile by exposing the premolars, including the molars.
5. Application of the Proposed Classification to the Therapeutic Field
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mazzuco, R.; Hexsel, D. Gummy smile and botulinum toxin: A new approach based on the gingival exposure area. J. Am. Acad. Dermatol. 2010, 63, 1042–1051. [Google Scholar] [CrossRef] [PubMed]
- Coppola, G.; Christopoulou, I.; Gkantidis, N.; Verna, C.; Pandis, N.; Kanavakis, G. The effect of orthodontic treatment on smile attractiveness: A systematic review. Prog. Orthod. 2023, 24, 4. [Google Scholar] [CrossRef]
- Rubin, L.R. The anatomy of a smile: Its importance in treating facial paralysis. Plast. Reconstr. Surg. 1974, 53, 384–387. [Google Scholar] [CrossRef]
- Huang, S.H.; Huang, Y.H.; Lin, Y.N.; Lee, S.S.; Chou, C.K.; Lin, T.Y.; Takahashi, H.; Kuo, Y.-R.; Lai, C.-S.; Lin, S.-D.; et al. Micro-autologous fat transplantation for treating a gummy smile. Aesthetic Surg. J. 2018, 38, 925–937. [Google Scholar] [CrossRef]
- Polo, M. Commentary on: Micro-Autologous Fat Transplantation for Treating a Gummy Smile. Aesthetic Surg. J. 2018, 38, 938–940. [Google Scholar] [CrossRef] [PubMed]
- Passia, N.; Blatz, M.; Strub, J.R. Is the smile line a valid parameter for esthetic evaluation? A systematic literature review. Eur. J. Esthet. Dent. 2011, 6, 314–327. [Google Scholar]
- Beall, A.E. Can a new smile make you look more intelligent and successful? Dent. Clin. N. Am. 2007, 51, 289–297. [Google Scholar] [CrossRef]
- Peck, S.; Peck, L. The gingival smile line. Angle Orthod. 1992, 62, 91–100. [Google Scholar] [PubMed]
- Wu, J.C.; Gu, Y.J.; McGrath, C.; Wong, R.W. Patients’ perception of anterior gingival display and aesthetics in smile analysis. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 633–639. [Google Scholar]
- Snider, C.C.; Amalfi, A.N.; Hutchinson, L.E.; Sommer, N.Z. New Insights into the Anatomy of the Midface Musculature and its Implications on the Nasolabial Fold. Aesthetic Plast. Surg. 2017, 41, 1083–1090. [Google Scholar] [CrossRef]
- Hwang, W.S.; Hur, M.S.; Hu, K.S.; Song, W.-C.; Koh, K.-S.; Baik, H.-S.; Kim, S.-T.; Kim, H.-J.; Lee, K.-J. Surface anatomy of the lip elevator muscles for treating gummy smile using botulinum toxin. Angle Orthod. 2009, 79, 70–77. [Google Scholar] [CrossRef] [PubMed]
- London, J.A.; Botero, P. Smile analysis and esthetic preferences: A systematic review. J. Prosthet. Dent. 2012, 108, 255–261. [Google Scholar]
- Venugopal, A.; Manzano, P.; Ahmed, F.; Vaid, N.R.; Bowman, S.J. Gummy Smiles: Etiologies, Diagnoses & Formulating a Clinically Effective Treatment Protocol. Semin. Orthod. 2024. [Google Scholar] [CrossRef]
- Tjan, A.H.; Miller, G.D.; The, J.G. Some esthetic factors in a smile. J. Prosthet. Dent. 1984, 51, 24–28. [Google Scholar] [CrossRef]
- Rubin, L.R.; Mishriki, Y.; Lee, G. Anatomy of the nasolabial fold: The keystone of the smiling mechanism. Plast. Reconstr. Surg. 1989, 83, 1–10. [Google Scholar] [CrossRef]
- De Maio, M. Myomodulation with injectable fillers: An innovative approach to addressing facial muscle movement. Aesthetic Plast. Surg. 2018, 42, 798–814. [Google Scholar] [CrossRef]
- Micheli-Pellegrini, V. About muscle insertions in man (Proposal for a new nomenclature of striated muscle). Acta Otorhinolaryngol. Ital. 2011, 31, 167–176. [Google Scholar]
- Von Arx, T.; Nakashima, M.J.; Lozanoff, S. The face—A musculoskeletal perspective. A literature review. Swiss Dent. J. 2018, 128, 678–688. [Google Scholar] [CrossRef] [PubMed]
- Dym, H.; Pierre, R. II Diagnosis and Treatment Approaches to a “Gummy Smile”. Dent. Clin. N. Am. 2020, 64, 341–349. [Google Scholar] [CrossRef]
- Nourah, D. Digital Smile Makeover: A Multidisciplinary Team Approach. Eur. J. Dent. 2023, 17, 1349–1355. [Google Scholar] [CrossRef]
- Sharif, H.; Aghayan, S. New Approaches for Gummy Smile Treatment: A Review. J. Res. Dent. Maxillofac. Sci. 2022, 8, 154. [Google Scholar] [CrossRef]
- Mercado, A.M.; Rosso, K. Update on diagnosing and treating gingival excess. Rev. ADM 2021, 78, 292–301. [Google Scholar]
- Monaco, A.; Streni, O.; Marci, M.C.; Sabetti, L.; Gatto, R. Clinical classification of gummy smile. Minerva Stomatol. 2004, 53, 53–59. [Google Scholar]
- Patel, D.; Megtha, F.; Trivedi, R.; Thakkar, S.; Suthar, J. Botulinum toxin and gummy smile-a review. IOSR J. Dent. Med. Sci. 2013, 4, 01–05. [Google Scholar] [CrossRef]
- Wu, H.; Lin, J.; Zhou, L.; Bai, D. Classification and craniofacial features of gummy smile in adolescents. J. Craniofac Surg. 2010, 21, 1474–1479. [Google Scholar] [CrossRef]
- Garber, D.A.; Salama, M.A. The aesthetic smile: Diagnosis and treatment. Periodontology 2000 1996, 11, 18–28. [Google Scholar] [CrossRef]
- Sarver, D.M.; Ackerman, M.B. Dynamic smile visualization and quantification: Part Evolution of the concept and dynamic records for smile capture. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 4–12. [Google Scholar] [CrossRef]
- Pavone, A.F.; Paganelli, C.; Di Taranto, S.; Fiorillo, L.; Lanza, A. Classification and management of gummy smiles: A real need in modern society. J. Craniofac Surg. 2019, 30, 691–694. [Google Scholar]
- Tatakis, D.N.; Paramitha, V.; Lu, W.E.; Guo, X. Upper lip characteristics and associated excessive gingival display etiologies in adults: Race and sex differences. J. Periodontol. 2024, 95, 74–83. [Google Scholar] [CrossRef]
- Oliveira, M.T.; Molina, G.O.; Furtado, A.; Ghizoni, J.S.; Pereira, J.R. Gummy smile: A contemporary and multidisciplinary overview. Dent. Hypotheses 2013, 4, 55–60. [Google Scholar]
- Robbins, J.W.; Mazzuco, R.; Farouk, K. The multidisciplinary management of gummy smile. Compend. Contin. Educ. Dent. 2005, 26, 340–352. [Google Scholar]
- Hur, M.S.; Hu, K.S.; Park, J.T.; Youn, K.H.; Kim, H.J. New anatomical insight of the levator labii superioris alaeque nasi and the transverse part of the nasalis. Surg. Radiol. Anat. 2010, 32, 753–756. [Google Scholar] [CrossRef] [PubMed]
- Hur, M.S.; Youn, K.H.; Hu, K.S.; Song, W.C.; Koh, K.S.; Fontaine, C.; Kim, H.J. New anatomic considerations on the levator labii superioris related to the nasal ala. J. Craniofacial Surg. 2010, 21, 258–260. [Google Scholar] [CrossRef] [PubMed]
- Olszewski, R.; Liu, Y.; Duprez, T.; Xu, T.M.; Reychler, H. Three-dimensional appearance of the lips muscles with three-dimensional isotropic MRI: In vivo study. Int. J. Comput. Assist. Radiol. Surg. 2009, 4, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Al Mashhrawi, Y.M.; AlNojaidi, T.F.; Alkhaldi, R.A.; Alshami, N.S.; Alhadlaq, A.S. Awareness and Knowledge of the Adverse Effects of Dermal Fillers Among the Saudi Population: A Cross-Sectional Study. Cureus 2023, 15, e40322. [Google Scholar] [CrossRef]
- Kyriazidis, I.; Spyropoulou, G.A.; Zambacos, G.; Tagka, A.; Rakhorst, H.A.; Gasteratos, K.; Berner, J.E.; Mandrekas, A. Adverse Events Associated with Hyaluronic Acid Filler Injection for Non-surgical Facial Aesthetics: A Systematic Review of High Level of Evidence Studies. Aesthetic Plast. Surg. 2024, 48, 719–741. [Google Scholar] [CrossRef]
- Nishikawa, A.; Aikawa, Y.; Kono, T. Current Status of Early Complications Caused by Hyaluronic Acid Fillers: Insights From a Descriptive, Observational Study of 41,775 Cases. Aesthetic Surg. J. 2023, 43, 893–904. [Google Scholar] [CrossRef]
- Rahman, E.; Philipp-Dormston, W.G.; Webb, W.R.; Rao, P.; Sayed, K.; Sharif AQ, M.O.; Yu, N.; Ioannidis, S.; Tam, E.; Rahman, Z.; et al. “Filler-Associated Acute Stroke Syndrome”: Classification, Predictive Modelling of Hyaluronidase Efficacy, and Updated Case Review on Neurological and Visual Complications. Aesthetic Plast. Surg. 2024. [Google Scholar] [CrossRef]
- Vega López, P.; Tejero García, P.; López-Pitalúa, J.A.; Pinto, H. Side effects after hyaluronic acid facial injection in adults during COVID-19 pandemic. J. Cosmet. Dermatol. 2023, 22, 1714–1719. [Google Scholar] [CrossRef]
- Farronato, M.; Cenzato, N.; Crispino, R.; Tartaglia, F.C.; Biagi, R.; Baldini, B.; Maspero, C. Divergence between CBCT and Optical Scans for Soft Tissue Analysis and Cephalometry in Facial Imaging: A cross-sectional study on healthy adults. Int. Orthod. 2024, 22, 100845. [Google Scholar] [CrossRef]
- Tatis, D.F.; Medina, C.X.; Delgado, D.; Agudelo, F.I.; Wallis, L.S.; Chica García, K.; Fernández Osorio, A. Correlation between the analysis of the dentoalveolar square and the photometric clinical diagnosis of smile. Int. J. Comput. Dent. 2022, 25, 125–132. [Google Scholar] [CrossRef]
- Özsoy, Ö.; Özsoy, U.; Yıldırım, Y.; Alkan, E.; Yılmaz, B.; Güllü, S.E. Correlation of 3D Morphometric Changes, Kinematics, and Muscle Activity During Smile. Laryngoscope 2024, 134, 3112–3119. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Classification Group | Authors | Factors Studied | Proposed Treatment | Main Conclusions |
|---|---|---|---|---|
| Muscular and Dento-Gingival Anatomy | Mazzuco [1], Mercado and Rosso [22], Monaco [23], Patel [24], Hao Wu [25] | Area and muscles of gingival exposure (Mazzuco): analyzes the amount and location of visible gingiva during the smile, identifying specific muscles such as the levator labii superioris and nasolabial (LLSAN) that contribute to different types of gingival smile. Esthetics, etiopathogenesis, and muscle functionality (Mercado and Rosso): they evaluate how smile appearance affects esthetic perception and underlying causes such as dental position and facial muscle activity. Dento-gingival and structural relationships (Monaco): this section considers altered passive eruption, upper lip length, and facial typology, which influence the smile’s appearance. Muscle mobility and control of gingival exposure (Patel): This section focuses on excessive muscle contraction and its impact on tooth and gingival exposure. It examines muscle mobility to classify the gingival smile. Detailed craniofacial variables (Hao Wu): uses precise measurements such as ANB, Pog-NP, and other facial dimensions to classify and better understand the craniofacial characteristics associated with different gingival smiles. | Botulinum Toxin: applied to reduce the hyperactivity of specific muscles involved in the gummy smile. Hyaluronic Acid: improves the support and projection of the maxilla and balance the muscular forces. Surgery and Orthodontics: in cases where the dentofacial structure requires it, orthognathic surgeries or orthodontic treatments can correct misalignments or structural problems. | Improved classification and treatment of the gingival smile based on specific anatomy and muscle functionality. |
| Esthetics and Facial Function | Garber and Salama [26], Saber and Ackerman [27], London and Botero [12] | Severity of gingival exposure, incisal-labial relationship (Garber and Salama): measures the amount of visible gingiva and the relationship between the incisal edge of the teeth and the upper lip at rest to classify the severity of gingival exposure. Facial harmony and lip movement (Saber and Ackerman): analyze how the lips move during smiling and their interaction with the teeth to determine the impact on overall facial esthetics. Physiological, anatomical, and functional characteristics (London and Botero): they evaluate facial symmetry, lips, gingiva, teeth, and smile dimensions. | Orthognathic and Periodontal Surgery: a more radical modification of the facial or gingival structure is needed for severe cases. Orthodontics and prosthodontics: less invasive treatments that seek to improve facial harmony and muscular functionality, including using orthodontic devices and dental esthetic techniques. | Emphasis on the importance of esthetics and facial functionality in treating the gingival smile, with proposals for personalized intervention. |
| Complex Customized Evaluations | Pavone [28], Tatakis [29], Oliveira [30] | Dental and periodontal analysis, individual characteristics (Pavone, Tatakis): this includes a detailed examination of the three-dimensional position of the teeth and clinical attachment levels. Subjective and objective evaluations of the smile (Tomas Oliveira): combines personal perception of the patient with objective measurements such as the shape and position of the teeth. Etiology of gingival excess and lip characteristics (Tatakis): focus on upper lip mobility and altered passive eruption. | Orthodontics and surgery for specific conditions. Personalized planning and multidisciplinary treatments to address specific causes identified in the evaluations. | A detailed and personalized evaluation of each patient leads to more effective and targeted treatments, recognizing the diversity of causes of the gummy smile. |
| Classification | Subcategory | Description | Evaluation Criteria | Treatment |
|---|---|---|---|---|
| 1. Upper Lip Vermilion Red Refinement | To evaluate lip tissue thinning and orbicularis muscle inversion during smiling. | - Objective measurement of gingival exposure by photographic and video analysis. - Clinical evaluation of vermilion red thickness. | - Application of hyaluronic acid using standardized microinjection techniques to restore the volume and proportion of vermilion red. - Continuous evaluation of results through photographic and clinical analysis. | |
| 2. Bone and Fat Volume | 2.1. Upper jaw | Identify loss or lack of volume in key areas. | Evaluation of bone projection and fat volume by 3D imaging and volumetric analysis. Patients usually have a flat midcheek. | - Bone and fat volume replacement using hyaluronic acid in specific areas (maxilla, piriform fossa, chin) both in periosteum with a 27 G needle and with a 25 G cannula in deep dermis. - Use of 3D imaging such as MRI and ultrasound to guide treatment delivery and adjustment. |
| 2.2. Piriform fossa | Analysis of the bony projection with computed tomography and clinical measurements. With the naked eye we can observe a subsidence or shadow in the area. | - Bone and fat volume replacement using hyaluronic acid in specific areas (maxilla, piriform fossa, chin) both in periosteum with a 27 G needle and with a 25 G cannula in deep dermis. - Use of 3D imaging such as MRI and ultrasound to guide treatment delivery and adjustment. | ||
| 2.3. Chi | Evaluation of fat and bone volume by MRI and clinical analysis. We will analyze with the Ricketts plane. | - Bone and fat volume replacement using hyaluronic acid in specific areas (maxilla, piriform fossa, chin) both in periosteum with a 27 G needle and with a 25 G cannula in deep dermis. - Use of 3D imaging such as MRI and ultrasound to guide treatment delivery and adjustment. | ||
| 3. Muscle Hypermobility and Muscle Function. | 3.1. Muscles elevating muscles of the upper lip and wing of the nose (LLSAN) | Analyze the excessive elevation of the upper lip. | -Electromyography evaluation. - Analysis of muscle dynamics during smiling. | - Myomodulation with hyaluronic acid and injection techniques in the affected areas. - Assessment of muscle response by electromyography and adjustments as needed. |
| 3.2. Levator labii superioris muscle (LLS) | To evaluate the contribution of the upper lip elevator to gingival exposure. | - Clinical examination. - Electromyography to measure muscle activity. | - Targeted myomodulation through injections to control upper lip levator muscle activity, adjusting gingival exposure. | |
| 3.3. Nasal septal depressor muscle (myrtiformis). | To analyze the influence of the nasal septal depressor muscle on gingival exposure. | - Clinical evaluation. - Analysis of the dynamics during smiling. | - Myomodulation treatment to adjust nasal septal depressor muscle activity, evaluating results and modifying as needed. | |
| 3.4. Zygomaticus major (ZM) and zygomaticus minor (Zm) muscles | To examine how zygomatic muscle traction contributes to the gingival smile. | - Measurement of muscle activity. - Analysis of facial dynamics. | - Comprehensive management of the muscular activity of the zygomatic muscles using myomodulation techniques and possible surgical interventions if necessary to optimize the gingival smile. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angulo-Manzaneque, G.; Baus-Domínguez, M.; Ruiz-de-León, G.; Serrera-Figallo, M.-Á.; Aguilera, F.S.; Torres-Lagares, D. Proposal of a New Therapeutic Classification in Gingival Smiles Focused on Treatment with Semi-Permanent Infiltrations. Dent. J. 2024, 12, 319. https://doi.org/10.3390/dj12100319
Angulo-Manzaneque G, Baus-Domínguez M, Ruiz-de-León G, Serrera-Figallo M-Á, Aguilera FS, Torres-Lagares D. Proposal of a New Therapeutic Classification in Gingival Smiles Focused on Treatment with Semi-Permanent Infiltrations. Dentistry Journal. 2024; 12(10):319. https://doi.org/10.3390/dj12100319
Chicago/Turabian StyleAngulo-Manzaneque, Gema, María Baus-Domínguez, Gonzalo Ruiz-de-León, María-Ángeles Serrera-Figallo, Fátima S. Aguilera, and Daniel Torres-Lagares. 2024. "Proposal of a New Therapeutic Classification in Gingival Smiles Focused on Treatment with Semi-Permanent Infiltrations" Dentistry Journal 12, no. 10: 319. https://doi.org/10.3390/dj12100319
APA StyleAngulo-Manzaneque, G., Baus-Domínguez, M., Ruiz-de-León, G., Serrera-Figallo, M.-Á., Aguilera, F. S., & Torres-Lagares, D. (2024). Proposal of a New Therapeutic Classification in Gingival Smiles Focused on Treatment with Semi-Permanent Infiltrations. Dentistry Journal, 12(10), 319. https://doi.org/10.3390/dj12100319