
An Evaluation of the Accuracy of Digital Models—An In Vitro Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Sample Selection
2.2. Scanning Procedures
2.3. Tooth Preparation
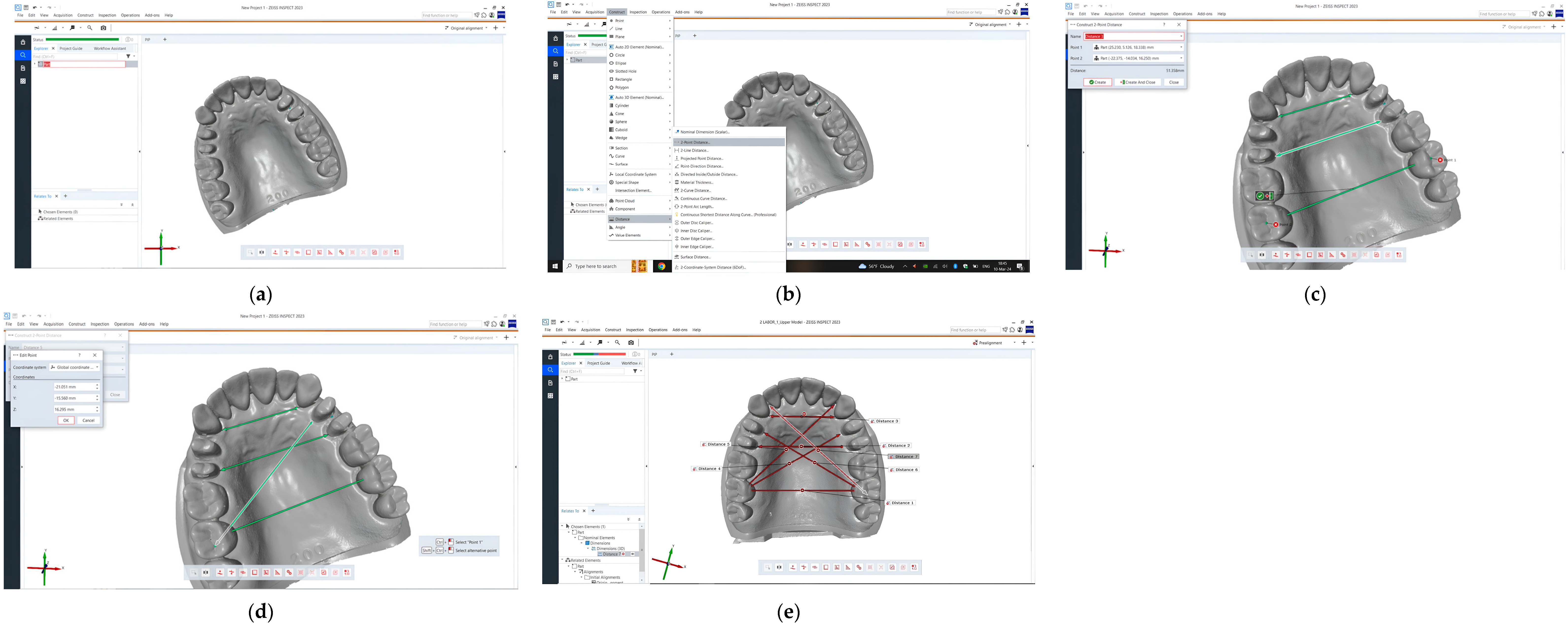
2.4. Measurements/STL Files Comparison
- A1, B1, a1, b1: in the central fossa of the molars 17, 27, 47, 37;
- A2, B2, a2, b2: in the distal fossa of the molars 17, 27, 47, 37;
- C, D, c, d: at the tip of the artificial interdental papillae in the interdental spaces 12–13, 22–23, 42–43, 32–33;
- R1, R2, R3, L1, L2, L3, r1, r2, r3, l1, l2, l3: on the artificial gingiva at the maximum convexity of the oral cervical contour of the teeth 13, 14, 15, 23, 24, 25/43, 44, 45, 33, 34, 35;
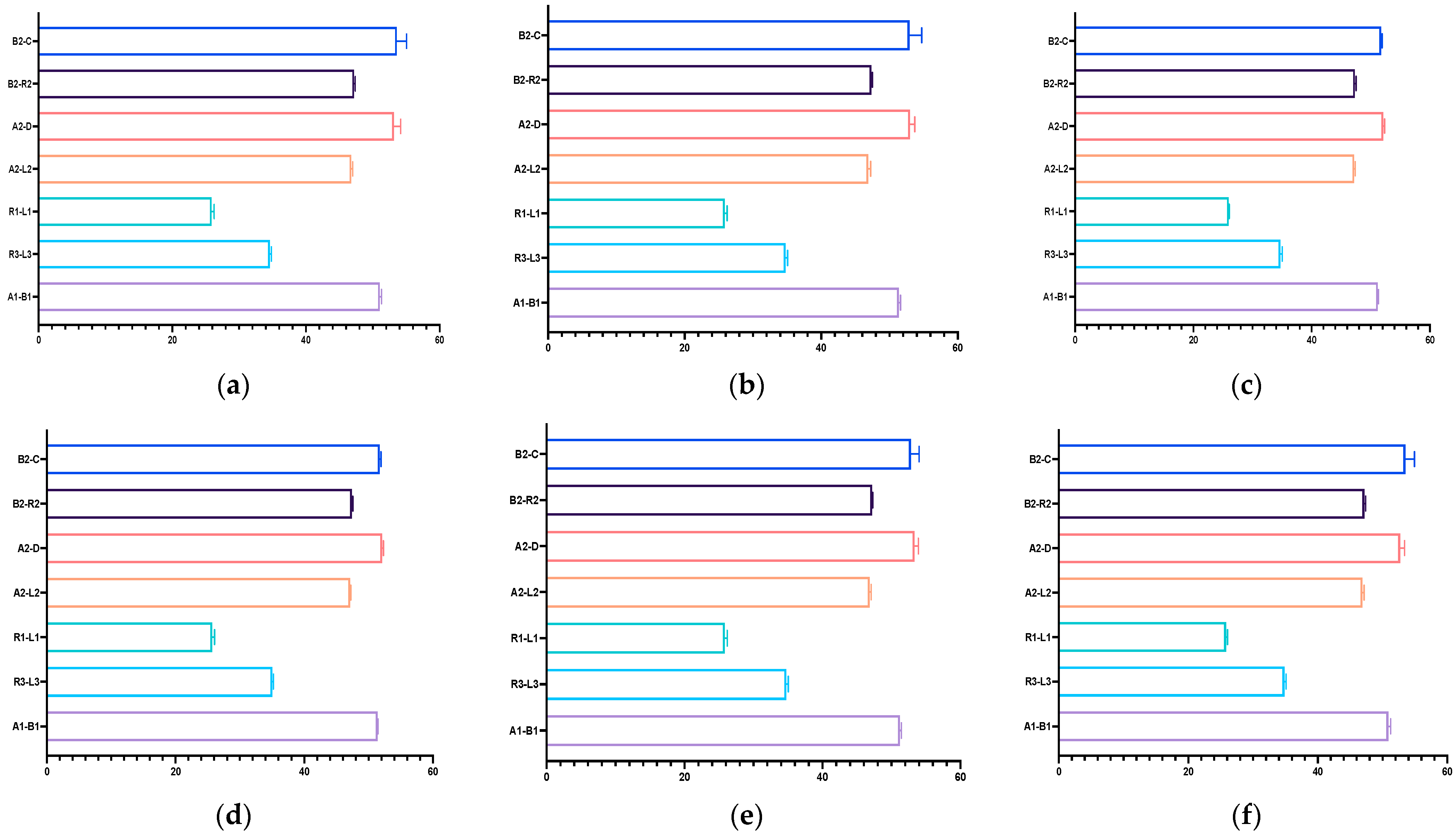
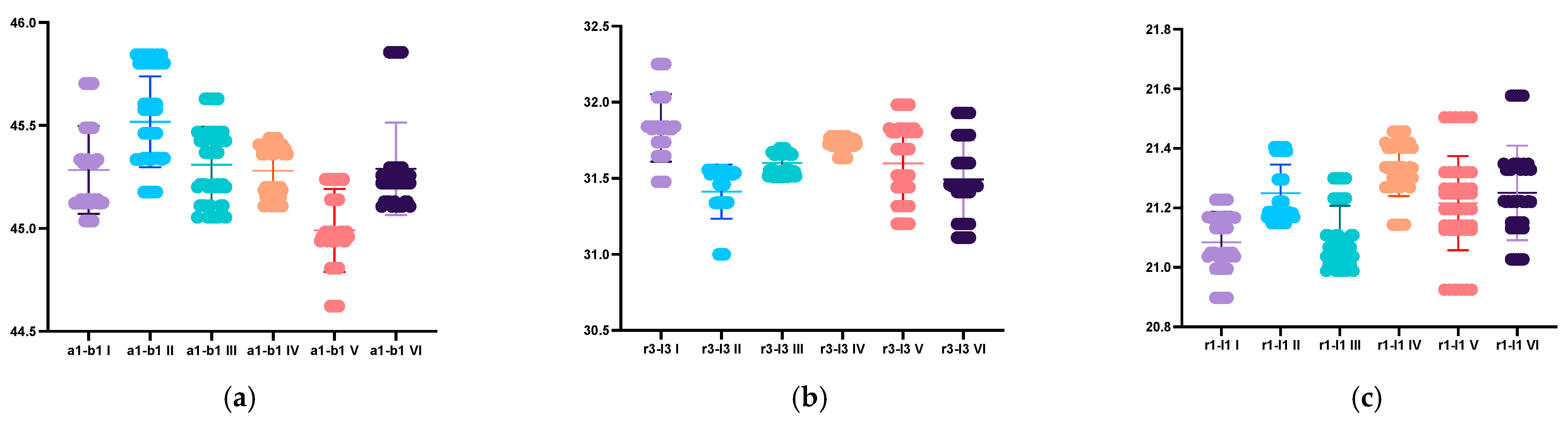
- To obtain the values in the transversal plane, the following distances were measured: R1-L1, R3-L3, A1-B1, r1-l1, r3-l3, a1-b1;
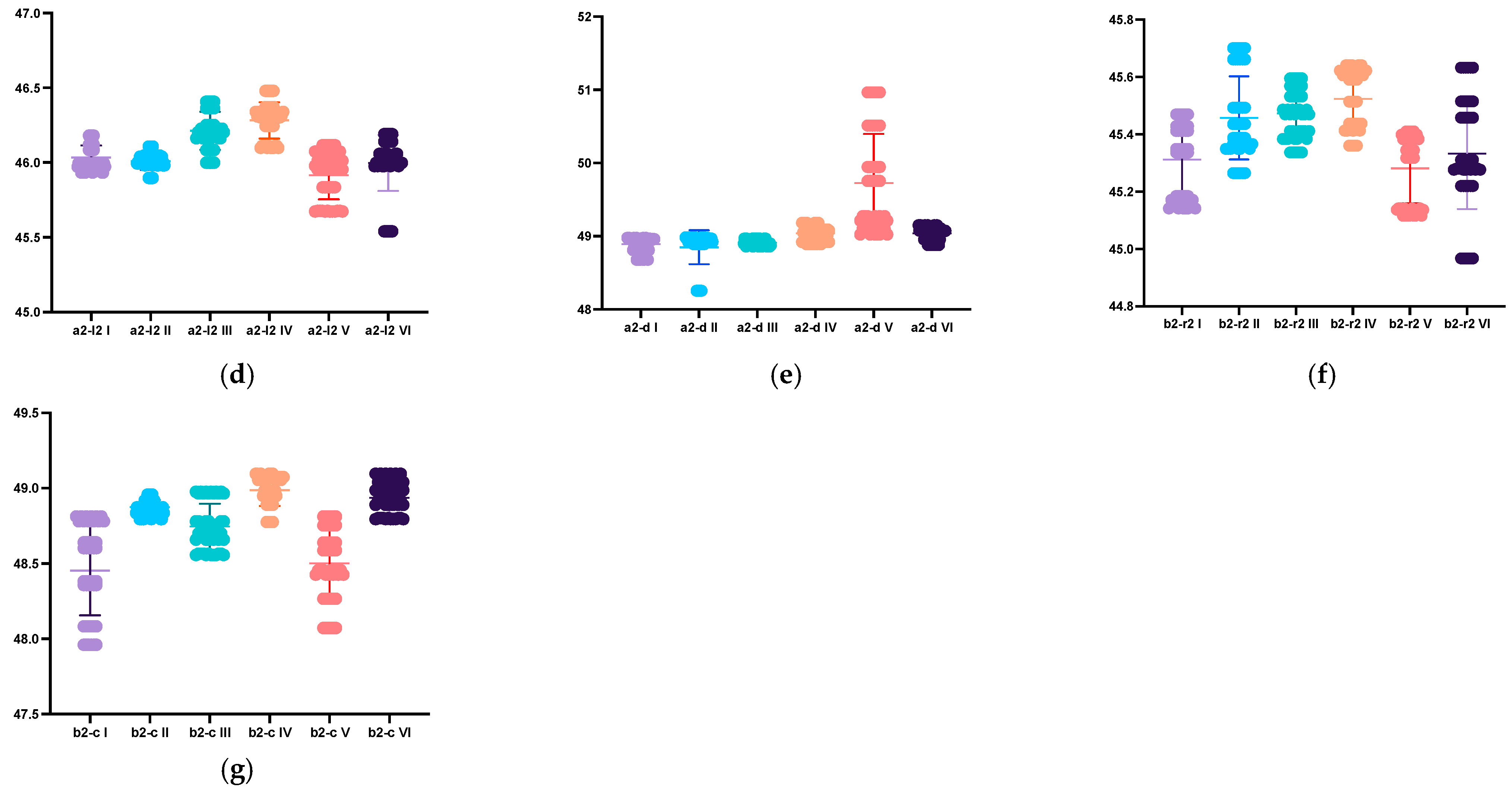
- To obtain the values in the sagittal plane, the following distances were measured: A2-D, A2-L2, B2-C, B2-R2, a2-d, a2-l2, b2-c, b2-r2.
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
- The accuracy of the scans can be influenced by the number of prepared teeth and their position on the dental arches. Distortions may occur on dental arches with multiple preparations, as in our study in the case of the lower arch.
- The digital models are distorted in full-arch scans, with the level of distortion being related to the scanning distance from the starting point.
- The manufacturer’s recommended scanning path may not always yield the most accurate results for intraoral scanners. Scientific research should guide the selection of the appropriate scanning path for each scanner, as was the case with the intraoral scanners used during this research.
- Self-calibrating systems may reduce accuracy; therefore, regular calibration is essential for obtaining realistic parameters during the scanning process.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Minimum (min) | Median (M) | Maximum (Max) | Mean (m) | Std. Deviation (SD) | Lower 95% CI of Mean | Upper 95% CI of Mean | ||
|---|---|---|---|---|---|---|---|---|
| VV np | A1-B1 | 50.74 | 51.02 | 51.45 | 51.04 | 0.2634 | 50.97 | 51.12 |
| R3-L3 | 34.25 | 34.6 | 34.96 | 34.58 | 0.2556 | 34.51 | 34.66 | |
| R1-L1 | 25.35 | 25.94 | 26.39 | 25.89 | 0.3727 | 25.78 | 26 | |
| A2-L2 | 46.4 | 46.81 | 47.06 | 46.77 | 0.2199 | 46.7 | 46.83 | |
| A2-D | 51.5 | 53.25 | 54.48 | 53.16 | 1.006 | 52.86 | 53.45 | |
| B2-R2 | 46.86 | 47.23 | 47.46 | 47.2 | 0.1805 | 47.14 | 47.25 | |
| B2-C | 50.57 | 54.03 | 55.11 | 53.59 | 1.472 | 53.16 | 54.02 | |
| VV p | A1-B1 | 50.97 | 51.25 | 51.81 | 51.37 | 0.2579 | 51.29 | 51.44 |
| R3-L3 | 34.26 | 34.86 | 35.1 | 34.77 | 0.3017 | 34.69 | 34.86 | |
| R1-L1 | 25.35 | 25.86 | 26.49 | 25.86 | 0.3473 | 25.76 | 25.96 | |
| A2-L2 | 46.38 | 46.9 | 47.4 | 46.9 | 0.3367 | 46.8 | 47 | |
| A2-D | 51.6 | 53.09 | 53.94 | 53.01 | 0.7064 | 52.8 | 53.21 | |
| B2-R2 | 47.1 | 47.3 | 47.68 | 47.34 | 0.1644 | 47.29 | 47.38 | |
| B2-C | 50.6 | 52.07 | 55.58 | 52.93 | 1.775 | 52.42 | 53.45 | |
| NOT np | A1-B1 | 50.99 | 51.15 | 51.45 | 51.17 | 0.1382 | 51.13 | 51.21 |
| R3-L3 | 33.87 | 34.8 | 35.01 | 34.68 | 0.3528 | 34.58 | 34.79 | |
| R1-L1 | 25.86 | 26.01 | 26.08 | 25.98 | 0.0884 | 25.95 | 26 | |
| A2-L2 | 46.85 | 47.17 | 47.47 | 47.19 | 0.1811 | 47.14 | 47.24 | |
| A2-D | 51.77 | 52.06 | 52.61 | 52.08 | 0.2538 | 52.01 | 52.15 | |
| B2-R2 | 47.03 | 47.27 | 47.73 | 47.31 | 0.2218 | 47.24 | 47.37 | |
| B2-C | 51.46 | 51.78 | 52.01 | 51.73 | 0.1892 | 51.67 | 51.78 | |
| NOT p | A1-B1 | 51.23 | 51.38 | 51.53 | 51.38 | 0.0886 | 51.36 | 51.41 |
| R3-L3 | 34.75 | 35.01 | 35.3 | 35.04 | 0.175 | 34.99 | 35.09 | |
| R1-L1 | 25.14 | 25.81 | 26.14 | 25.73 | 0.3412 | 25.63 | 25.83 | |
| A2-L2 | 46.97 | 47.11 | 47.28 | 47.13 | 0.1045 | 47.1 | 47.16 | |
| A2-D | 51.83 | 52.09 | 52.43 | 52.12 | 0.2016 | 52.06 | 52.18 | |
| B2-R2 | 47.22 | 47.44 | 47.65 | 47.43 | 0.1529 | 47.38 | 47.47 | |
| B2-C | 51.38 | 51.74 | 51.98 | 51.72 | 0.2035 | 51.66 | 51.78 | |
| IOS np | A1-B1 | 50.99 | 51.21 | 51.57 | 51.23 | 0.1996 | 51.17 | 51.29 |
| R3-L3 | 34.32 | 34.8 | 35.05 | 34.76 | 0.2783 | 34.68 | 34.84 | |
| R1-L1 | 24.96 | 25.9 | 26.19 | 25.84 | 0.3567 | 25.74 | 25.94 | |
| A2-L2 | 46.55 | 46.84 | 47.15 | 46.85 | 0.2018 | 46.79 | 46.91 | |
| A2-D | 52.58 | 53.26 | 54.23 | 53.35 | 0.5459 | 53.19 | 53.51 | |
| B2-R2 | 47.08 | 47.22 | 47.3 | 47.21 | 0.0666 | 47.19 | 47.23 | |
| B2-C | 51.51 | 52.45 | 55.2 | 52.82 | 1.202 | 52.47 | 53.17 | |
| IOS p | A1-B1 | 50.39 | 51.01 | 51.29 | 50.9 | 0.3403 | 50.8 | 51 |
| R3-L3 | 34.41 | 34.9 | 35.15 | 34.85 | 0.2473 | 34.78 | 34.93 | |
| R1-L1 | 25.43 | 25.78 | 26.21 | 25.83 | 0.2474 | 25.75 | 25.9 | |
| A2-L2 | 46.59 | 46.85 | 47.28 | 46.9 | 0.26 | 46.82 | 46.97 | |
| A2-D | 51.48 | 52.75 | 53.69 | 52.71 | 0.6907 | 52.51 | 52.91 | |
| B2-R2 | 46.84 | 47.29 | 47.37 | 47.17 | 0.2051 | 47.11 | 47.23 | |
| B2-C | 51.25 | 54.25 | 54.84 | 53.51 | 1.418 | 53.1 | 53.93 |
| Minimum (min) | Median (M) | Maximum (Max) | Mean (m) | Std. Deviation (SD) | Lower 95% CI of Mean | Upper 95% CI of Mean | ||
|---|---|---|---|---|---|---|---|---|
| VV np | a1-b1 | 45.04 | 45.23 | 45.7 | 45.28 | 0.213 | 45.22 | 45.35 |
| r3-l3 | 31.48 | 31.83 | 32.25 | 31.83 | 0.2219 | 31.77 | 31.9 | |
| r1-l1 | 20.9 | 21.09 | 21.23 | 21.08 | 0.1029 | 21.05 | 21.11 | |
| a2-l2 | 45.93 | 45.99 | 46.18 | 46.03 | 0.0808 | 46.01 | 46.06 | |
| a2-d | 48.68 | 48.95 | 48.98 | 48.89 | 0.1014 | 48.86 | 48.92 | |
| b2-r2 | 45.14 | 45.34 | 45.47 | 45.31 | 0.1214 | 45.28 | 45.35 | |
| b2-c | 47.96 | 48.49 | 48.81 | 48.45 | 0.2963 | 48.37 | 48.54 | |
| VV p | a1-b1 | 45.18 | 45.52 | 45.84 | 45.52 | 0.221 | 45.45 | 45.58 |
| r3-l3 | 31 | 31.49 | 31.56 | 31.41 | 0.1778 | 31.36 | 31.46 | |
| r1-l1 | 21.15 | 21.2 | 21.4 | 21.25 | 0.096 | 21.22 | 21.28 | |
| a2-l2 | 45.9 | 46 | 46.11 | 46.01 | 0.0572 | 45.99 | 46.03 | |
| a2-d | 48.25 | 48.92 | 48.98 | 48.85 | 0.23 | 48.78 | 48.92 | |
| b2-r2 | 45.27 | 45.41 | 45.7 | 45.46 | 0.1451 | 45.42 | 45.5 | |
| b2-c | 48.8 | 48.87 | 48.96 | 48.87 | 0.0469 | 48.86 | 48.89 | |
| NOT np | a1-b1 | 45.05 | 45.29 | 45.63 | 45.31 | 0.1857 | 45.25 | 45.36 |
| r3-l3 | 31.51 | 31.6 | 31.7 | 31.6 | 0.0736 | 31.58 | 31.62 | |
| r1-l1 | 20.99 | 21.08 | 21.3 | 21.1 | 0.1029 | 21.07 | 21.13 | |
| a2-l2 | 46 | 46.22 | 46.41 | 46.21 | 0.1274 | 46.18 | 46.25 | |
| a2-d | 48.86 | 48.9 | 48.97 | 48.91 | 0.04 | 48.9 | 48.92 | |
| b2-r2 | 45.34 | 45.48 | 45.6 | 45.47 | 0.0858 | 45.45 | 45.5 | |
| b2-c | 48.56 | 48.73 | 48.98 | 48.75 | 0.152 | 48.7 | 48.79 | |
| NOT p | a1-b1 | 45.11 | 45.28 | 45.44 | 45.28 | 0.1233 | 45.24 | 45.32 |
| r3-l3 | 31.63 | 31.74 | 31.78 | 31.73 | 0.0443 | 31.71 | 31.74 | |
| r1-l1 | 21.14 | 21.34 | 21.46 | 21.33 | 0.0937 | 21.31 | 21.36 | |
| a2-l2 | 46.1 | 46.31 | 46.48 | 46.28 | 0.1217 | 46.25 | 46.32 | |
| a2-d | 48.89 | 49.06 | 49.18 | 49.04 | 0.0894 | 49.01 | 49.06 | |
| b2-r2 | 45.36 | 45.55 | 45.64 | 45.52 | 0.1016 | 45.49 | 45.55 | |
| b2-c | 48.78 | 49.02 | 49.1 | 48.99 | 0.1053 | 48.96 | 49.02 | |
| IOS np | a1-b1 | 44.62 | 44.97 | 45.24 | 44.99 | 0.2016 | 44.93 | 45.05 |
| r3-l3 | 31.2 | 31.61 | 31.98 | 31.6 | 0.2575 | 31.52 | 31.67 | |
| r1-l1 | 20.93 | 21.22 | 21.5 | 21.22 | 0.1582 | 21.17 | 21.26 | |
| a2-l2 | 45.67 | 45.97 | 46.12 | 45.92 | 0.1609 | 45.87 | 45.96 | |
| a2-d | 49.02 | 49.51 | 50.97 | 49.72 | 0.6737 | 49.53 | 49.92 | |
| b2-r2 | 45.12 | 45.33 | 45.41 | 45.28 | 0.1205 | 45.25 | 45.32 | |
| b2-c | 48.07 | 48.52 | 48.81 | 48.5 | 0.2353 | 48.43 | 48.57 | |
| IOS p | a1-b1 | 45.11 | 45.23 | 45.86 | 45.29 | 0.2243 | 45.22 | 45.35 |
| r3-l3 | 31.11 | 31.45 | 31.93 | 31.49 | 0.26 | 31.42 | 31.57 | |
| r1-l1 | 21.03 | 21.22 | 21.58 | 21.25 | 0.159 | 21.2 | 21.3 | |
| a2-l2 | 45.54 | 46.04 | 46.19 | 46 | 0.1874 | 45.94 | 46.05 | |
| a2-d | 48.88 | 49.07 | 49.15 | 49.03 | 0.0848 | 49.01 | 49.06 | |
| b2-r2 | 44.97 | 45.3 | 45.63 | 45.33 | 0.193 | 45.28 | 45.39 | |
| b2-c | 48.8 | 48.94 | 49.1 | 48.94 | 0.1011 | 48.91 | 48.97 |
Appendix B
| VV np | VV p | NOT np | NOT p | IOS np | IOS p | ||
|---|---|---|---|---|---|---|---|
| VV np | A1-B1 | - | <0.0001 | ns | <0.0001 | 0.0404 | ns |
| R3-L3 | - | 0.0029 | ns | <0.0001 | 0.0129 | <0.0001 | |
| R1-L1 | - | ns | ns | ns | ns | ns | |
| A2-L2 | - | ns | <0.0001 | <0.0001 | ns | ns | |
| A2-D | - | ns | <0.0001 | <0.0001 | ns | ns | |
| B2-R2 | - | 0.011 | ns | 0.011 | ns | ns | |
| B2-C | - | <0.0001 | <0.0001 | ns | ns | ||
| VV p | A1-B1 | <0.0001 | - | 0.0031 | ns | ns | <0.0001 |
| R3-L3 | 0.0029 | - | ns | 0.0003 | ns | ns | |
| R1-L1 | ns | - | ns | ns | ns | ns | |
| A2-L2 | ns | - | <0.0001 | 0.0006 | ns | ns | |
| A2-D | ns | - | <0.0001 | <0.0001 | ns | ns | |
| B2-R2 | 0.011 | - | ns | ns | 0.028 | 0.028 | |
| B2-C | ns | - | <0.0001 | <0.0001 | ns | ns | |
| NOT np | A1-B1 | ns | 0.0031 | - | <0.0001 | ns | ns |
| R3-L3 | ns | ns | - | <0.0001 | ns | ns | |
| R1-L1 | ns | ns | - | 0.0019 | ns | ns | |
| A2-L2 | <0.0001 | <0.0001 | - | ns | <0.0001 | <0.0001 | |
| A2-D | <0.0001 | <0.0001 | - | ns | <0.0001 | 0.0002 | |
| B2-R2 | ns | ns | - | ns | 0.016 | ns | |
| B2-C | <0.0001 | <0.0001 | - | ns | <0.0001 | <0.0001 | |
| NOT p | A1-B1 | <0.0001 | ns | <0.0001 | - | 0.0014 | <0.0001 |
| R3-L3 | <0.0001 | 0.0003 | <0.0001 | - | <0.0001 | 0.0259 | |
| R1-L1 | ns | ns | 0.0019 | - | ns | ns | |
| A2-L2 | <0.0001 | <0.0001 | ns | - | <0.0001 | 0.0004 | |
| A2-D | <0.0001 | <0.0001 | ns | - | <0.0001 | 0.0007 | |
| B2-R2 | 0.011 | ns | ns | - | <0.0001 | ns | |
| B2-C | <0.0001 | <0.0001 | ns | - | <0.0001 | <0.0001 | |
| IOS np | A1-B1 | 0.0404 | ns | ns | 0.0014 | - | 0.0001 |
| R3-L3 | 0.0129 | ns | ns | <0.0001 | - | ns | |
| R1-L1 | ns | ns | ns | ns | - | ns | |
| A2-L2 | ns | ns | <0.0001 | <0.0001 | - | ns | |
| A2-D | ns | ns | <0.0001 | <0.0001 | - | 0.0022 | |
| B2-R2 | ns | 0.028 | 0.016 | <0.0001 | - | ns | |
| B2-C | ns | ns | <0.0001 | <0.0001 | - | ns | |
| IOS p | A1-B1 | ns | <0.0001 | ns | <0.0001 | 0.0001 | - |
| R3-L3 | <0.0001 | ns | ns | <0.0001 | ns | - | |
| R1-L1 | ns | ns | ns | ns | ns | - | |
| A2-L2 | ns | ns | <0.0001 | 0.0004 | ns | - | |
| A2-D | ns | 0.0002 | 0.0007 | ns | 0.0022 | - | |
| B2-R2 | ns | <0.0001 | ns | ns | ns | - | |
| B2-C | ns | ns | <0.0001 | <0.0001 | ns | - |
| VV np | VV p | NOT np | NOT p | IOS np | IOS p | ||
|---|---|---|---|---|---|---|---|
| VV np | a1-b1 | - | <0.0001 | ns | ns | <0.0001 | |
| r3-l3 | - | <0.0001 | <0.0001 | ns | <0.0001 | <0.0001 | |
| r1-l1 | - | <0.0001 | ns | <0.0001 | 0.0003 | <0.0001 | |
| a2-l2 | - | ns | <0.0001 | <0.0001 | ns | ns | |
| a2-d | - | ns | ns | <0.0001 | <0.0001 | <0.0001 | |
| b2-r2 | - | <0.0001 | <0.0001 | <0.0001 | ns | ns | |
| b2-c | - | <0.0001 | 0.0062 | <0.0001 | ns | 0.0062 | |
| VV p | a1-b1 | <0.0001 | - | 0.003 | <0.0001 | <0.0001 | <0.0001 |
| r3-l3 | <0.0001 | - | 0.0062 | <0.0001 | 0.0013 | ns | |
| r1-l1 | <0.0001 | - | <0.0001 | ns | ns | ns | |
| a2-l2 | ns | - | <0.0001 | <0.0001 | ns | ns | |
| a2-d | ns | - | ns | <0.0001 | <0.0001 | <0.0001 | |
| b2-r2 | <0.0001 | - | ns | ns | <0.0001 | 0.0177 | |
| b2-c | <0.0001 | - | 0.0233 | 0.0206 | <0.0001 | ns | |
| NOT np | a1-b1 | ns | 0.003 | - | ns | <0.0001 | ns |
| r3-l3 | <0.0001 | 0.0062 | - | 0.0037 | ns | ns | |
| r1-l1 | ns | <0.0001 | - | <0.0001 | 0.0013 | <0.0001 | |
| a2-l2 | <0.0001 | <0.0001 | - | ns | <0.0001 | <0.0001 | |
| a2-d | ns | ns | - | <0.0001 | <0.0001 | <0.0001 | |
| b2-r2 | <0.0001 | ns | - | ns | <0.0001 | 0.0003 | |
| b2-c | 0.0062 | 0.0233 | - | <0.0001 | 0.0068 | <0.0001 | |
| NOT p | a1-b1 | ns | <0.0001 | ns | - | <0.0001 | ns |
| r3-l3 | ns | <0.0001 | 0.0037 | - | 0.0164 | <0.0001 | |
| r1-l1 | <0.0001 | ns | <0.0001 | - | 0.0003 | 0.0074 | |
| a2-l2 | <0.0001 | <0.0001 | ns | - | <0.0001 | <0.0001 | |
| a2-d | <0.0001 | <0.0001 | <0.0001 | - | <0.0001 | ns | |
| b2-r2 | <0.0001 | ns | ns | - | <0.0001 | <0.0001 | |
| b2-c | <0.0001 | 0.0206 | <0.0001 | - | <0.0001 | ns | |
| IOS np | a1-b1 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | - | <0.0001 |
| r3-l3 | <0.0001 | 0.0013 | ns | 0.0164 | - | ns | |
| r1-l1 | 0.0003 | ns | 0.0013 | 0.0003 | - | ns | |
| a2-l2 | ns | ns | <0.0001 | <0.0001 | - | ns | |
| a2-d | <0.0001 | <0.0001 | <0.0001 | <0.0001 | - | <0.0001 | |
| b2-r2 | ns | <0.0001 | <0.0001 | <0.0001 | - | ||
| b2-c | ns | <0.0001 | 0.0068 | <0.0001 | - | <0.0001 | |
| IOS p | a1-b1 | ns | <0.0001 | ns | ns | <0.0001 | - |
| r3-l3 | <0.0001 | ns | ns | <0.0001 | ns | - | |
| r1-l1 | <0.0001 | ns | <0.0001 | 0.0074 | ns | - | |
| a2-l2 | ns | ns | <0.0001 | <0.0001 | ns | - | |
| a2-d | <0.0001 | <0.0001 | <0.0001 | ns | <0.0001 | - | |
| b2-r2 | ns | 0.0177 | 0.0003 | <0.0001 | ns | - | |
| b2-c | 0.0062 | ns | <0.0001 | ns | <0.0001 | - |
References
- Mhatre, S.; Gholap, P.; Kakade, P.; Srichand, R.; Joshi, M. Evolution of intraoral scanners in dentistry: An overview. Eur. Chem. Bull. 2023, 12, 4267–4276. [Google Scholar]
- Ahmed, S.; Hawsah, A.; Rustom, R.; Alamri, A.; Althomairy, S.; Alenezi, M.; Shaker, S.; Al-Rawsaa, F.; Althumairy, A.; Alteraigi, A. Digital Impressions Versus Conventional Impres-sions in Prosthodontics: A Systematic Review. Cureus 2024, 16, e51537. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cappare, P.; Sannino, G.; Minoli, M.; Montemezzi, P.; Ferrini, F. Conventional versus Digital Impressions for Full Arch Screw-Retained Maxillary Rehabilitations: A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2019, 16, 829. [Google Scholar] [CrossRef] [PubMed]
- Ben-Izhack, G.; Rosner, O.; Zenziper, E.; Nissan, J.; Hosary, R.; Lugassy, D.; Shely, A. Comparison between Conventional and Digital Impres-sions for Determining Axes and Distances of Three Implants in Straight and Curved Lines: An In Vitro Study. J. Clin. Med. 2024, 13, 2352. [Google Scholar] [CrossRef] [PubMed]
- Farhan, F.A.; Sahib, A.J.; Fatalla, A.A. Comparison of the accuracy of intraoral digital impression system and conventional impression techniques for multiple implants in the full-arch edentulous mandible. J. Clin. Exp. Dent. 2021, 13, e487–e492. [Google Scholar] [CrossRef]
- Nedelcu, R.; Olsson, P.; Nyström, I.; Rydén, J.; Thor, A. Accuracy and precision of 3 intraoral scanners and accuracy of conventional impressions: A novel in vivo analysis method. J. Dent. 2018, 69, 110–118. [Google Scholar] [CrossRef]
- Oh, H.-S.; Lim, Y.-J.; Kim, B.; Kim, M.-J.; Kwon, H.-B.; Baek, Y.-W. Influence of Scanning-Aid Materials on the Accuracy and Time Efficiency of Intraoral Scanners for Full-Arch Digital Scanning: An In Vitro Study. Materials 2021, 14, 2340. [Google Scholar] [CrossRef]
- Ender, A.; Zimmermann, M.; Attin, T.; Mehl, A. In vivo precision of conventional and digital methods for obtaining quadrant dental impressions. Clin. Oral Investig. 2016, 20, 1495–1504. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.; Klussmann, L.; Wöstmann, B.; Schlenz, M.A. Accuracy of Digital and Conventional Full-Arch Impressions in Patients: An Update. J. Clin. Med. 2020, 9, 688. [Google Scholar] [CrossRef]
- Ender, A.; Mehl, A. Accuracy in dental medicine, a new way to measure trueness and precision. J. Vis. Exp. 2014, 29, 51374. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rudolph, H.; Salmen, H.; Moldan, M.; Kuhn, K.; Sichwardt, V.; Wöstmann, B.; Luthardt, R.G. Accuracy of intraoral and extraoral digital data acquisition for dental restorations. J. Appl. Oral Sci. 2016, 24, 85–94. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ender, A.; Mehl, A. Influence of scanning strategies on the accuracy of digital intraoral scanning systems. Int. J. Comput. Dent. 2013, 16, 11–21. [Google Scholar] [PubMed]
- Kim, J.H.; Kim, K.B.; Kim, S.H.; Kim, W.C.; Kim, H.Y.; Kim, J.H. Quantitative evaluation of common errors in digital impression obtained by using an LED blue light in-office CAD/CAM system. Quintessence Int. 2015, 46, 401–407. [Google Scholar] [PubMed]
- Logozzo, S.; Zanetti, E.; Franceschini, G.; Kilpela, A.; Mäkynen, A. Recent advances in dental optics–Part I: 3D intraoral scanners for restorative dentistry. Opt. Lasers Eng. 2014, 54, 203–221. [Google Scholar] [CrossRef]
- Sfondrini, M.F.; Gandini, P.; Malfatto, M.; Di Corato, F.; Trovati, F.; Scribante, A. Computerized Casts for Orthodontic Purpose Using Powder-Free Intraoral Scanners: Accuracy, Execution Time, and Patient Feedback. BioMed Res. Int. 2018, 2018, 4103232. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jánosi, K.M.; Cerghizan, D.; Mártha, K.I.; Elekes, É.; Szakács, B.; Elekes, Z.; Kovács, A.; Szász, A.; Mureșan, I.; Hănțoiu, L.G. Evaluation of Intraoral Full-Arch Scan versus Conventional Preliminary Impression. J. Clin. Med. 2023, 12, 5508. [Google Scholar] [CrossRef]
- Cicciù, M.; Fiorillo, L.; D’Amico, C.; Gambino, D.; Amantia, E.M.; Laino, L.; Crimi, S.; Campagna, P.; Bianchi, A.; Herford, A.S.; et al. 3D Digital Impression Systems Compared with Tradi-tional Techniques in Dentistry: A Recent Data Systematic Review. Materials 2020, 13, 1982. [Google Scholar] [CrossRef]
- Resende, C.C.D.; Barbosa, T.A.Q.; Moura, G.F.; Tavares, L.D.N.; Rizzante, F.A.P.; George, F.M.; Neves, F.D.D.; Mendonça, G. Influence of operator experience, scanner type, and scan size on 3D scans. J. Prosthet. Dent. 2021, 125, 294–299. [Google Scholar] [CrossRef]
- Bosniac, P.; Rehmann, P.; Wöstmann, B. Comparison of an indirect impression scanning system and two direct intraoral scanning systems in vivo. Clin. Oral Investig. 2019, 23, 2421–2427.125. [Google Scholar] [CrossRef] [PubMed]
- Memari, Y.; Mohajerfar, M.; Armin, A.; Kamalian, F.; Rezayani, V.; Beyabanaki, E. Marginal Adaptation of CAD/CAM All-Ceramic Crowns Made by Different Impression Methods: A Literature Review. J. Prosthodont. 2019, 28, e536–e544. [Google Scholar] [CrossRef]
- Jeong, I.D.; Lee, J.J.; Jeon, J.H.; Kim, J.H.; Kim, H.Y.; Kim, W.C. Accuracy of complete-arch model using an intraoral video scanner: An in vitro study. J. Prosthet. Dent. 2016, 115, 755–759. [Google Scholar] [CrossRef] [PubMed]
- Nedelcu, R.G.; Persson, A.S. Scanning accuracy and precision in 4 intraoral scanners: An in vitro comparison based on 3-dimensional analysis. J. Prosthet. Dent. 2014, 112, 1461–1471. [Google Scholar] [CrossRef] [PubMed]
- Goracci, C.; Franchi, L.; Vichi, A.; Ferrari, M. Accuracy, reliability, and efficiency of intraoral scanners for full-arch impressions: A systematic review of the clinical evidence. Eur. J. Orthod. 2016, 38, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Khraishi, H.; Duane, B. Evidence for use of intraoral scanners under clinical conditions for obtaining full-arch digital impressions is insufficient. Evid. Based Dent. 2017, 18, 24–25. [Google Scholar] [CrossRef]
- Kurz, M.; Attin, T.; Mehl, A. Influence of material surface on the scanning error of a powder-free 3D measuring system. Clin. Oral Investig. 2015, 19, 2035–2043. [Google Scholar] [CrossRef]
- Atieh, M.A.; Ritter, A.V.; Ko, C.C.; Duqum, I. Accuracy evaluation of intraoral optical impres-sions: A clinical study using a reference appliance. J. Prosthet. Dent. 2017, 118, 400–405. [Google Scholar] [CrossRef]
- Kuhr, F.; Schmidt, A.; Rehmann, P.; Wöstmann, B. A new method for assessing the accuracy of full arch impressions in patients. J. Dent. 2016, 55, 68–74. [Google Scholar] [CrossRef]
- Keul, C.; Güth, J.F. Accuracy of full-arch digital impressions: An in vitro and in vivo comparison. Clin. Oral Investig. 2020, 24, 735–745. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Lee, J.S.; Choo, H.H.; Hwang, H.S.; Lee, K.M. Reproducibility of an intraoral scanner: A comparison between in-vivo and ex-vivo scans. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, L.; Marques, T.; Karasan, D.; Fehmer, V.; Sailer, I.; Correia, A.; Gomez-Polo, M. Influence of Implant Scanbody Material and Intraoral Scanner on the Accuracy of Complete-Arch Digital Implant Impressions. Int. J. Prosthodont. 2023, 36, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, L.; Marques, T.; Karasan, D.; Fehmer, V.; Sailer, I.; Correia, A.; Gómez-Polo, M. Effect of Splinting Scan Bodies on the Trueness of Complete Arch Digital Implant Scans with 5 Different Intraoral Scanners. J. Prosthet. Dent. 2024, 132, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Müller, P.; Ender, A.; Joda, T.; Katsoulis, J. Impact of digital intraoral scan strategies on the impression accuracy using the TRIOS Pod scanner. Quintessence Int. 2016, 47, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Park, G.H.; Son, K.; Lee, K.B. Feasibility of using an intraoral scanner for a complete-arch digital scan. J. Prosthet. Dent. 2019, 121, 803–810. [Google Scholar] [CrossRef]
- Ender, A.; Attin, T.; Mehl, A. In vivo precision of conventional and digital methods of obtaining complete-arch dental impressions. J. Prosthet. Dent. 2016, 115, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Fukazawa, S.; Odaira, C.; Kondo, H. Investigation of accuracy and reproducibility of abutment position by intraoral scan-ners. J. Prosthodont. Res. 2017, 61, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Carbajal Mejía, J.B.; Wakabayashi, K.; Nakamu-ra, T.; Yatani, H. Influence of abutment tooth geometry on the accuracy of conventional and digital methods of obtaining dental impressions. J. Prosthet. Dent. 2017, 118, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Medina-Sotomayor, P.; Pascual-Moscardo, A.; Camps, A.I. Accuracy of 4 digital scanning systems on prepared teeth digitally isolated from a complete dental arch. J. Prosthet. Dent. 2019, 121, 811–820. [Google Scholar] [CrossRef] [PubMed]
- Kernen, F.; Schlager, S.; Seidel Alvarez, V.; Mehrhof, J.; Vach, K.; Kohal, R.; Nelson, K.; Flügge, T. Accuracy of intraoral scans: An in vivo study of different scanning devices. J. Prosthet. Dent. 2022, 128, 1303–1309. [Google Scholar] [CrossRef]
- Sason, G.K.; Mistry, G.; Tabassum, R.; Shetty, O. A comparative evaluation of intraoral and extraoral digital impressions: An in vivo study. J. Indian Prosthodont. Soc. 2018, 18, 108–116. [Google Scholar] [CrossRef]
- Güth, J.F.; Edelhoff, D.; Schweiger, J.; Keul, C. A New Method for the Evaluation of the Accuracy of Full-Arch Digital Impressions in Vitro. Clin. Oral Investig. 2016, 20, 1487–1494. [Google Scholar] [CrossRef]
- Revilla-León, M.; Jiang, P.; Sadeghpour, M.; Piedra-Cascón, W.; Zandinejad, A.; Özcan, M.; Krishnamurthy, V.R. Intraoral digital scans-Part 1: Influence of ambient scanning light conditions on the accuracy (trueness and precision) of different intraoral scanners. J. Prosthet. Dent. 2020, 124, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Blanco, D.; Fernández, P.; Cuesta, E.; Suárez, C.M. Influence of ambient light on the quality of laser digitized surfaces. In Proceedings of the World Congress on Engineering, London, UK, 2–4 July 2008; Volume 1, pp. 32–37. [Google Scholar]
- Arakida, T.; Kanazawa, M.; Iwaki, M.; Suzuki, T.; Minakuchi, S. Evaluating the influence of ambient light on scanning trueness, precision, and time of intra oral scanner. J. Prosthodont. Res. 2018, 62, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.Y.; Esguerra, R.J.; Chia, V.A.P.; Tan, Y.H.; Tan, K.B.C. Three-dimensional accuracy of digital static interocclusal registration by three intraoral scanner systems. J. Prosthodont. 2018, 27, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Subramanian, S.G.; Att, W.; Krishnamurthy, V.R. Analysis of different illuminance of the room lighting condition on the accuracy (trueness and precision) of an intraoral scanner. J. Prosthodont. 2021, 30, 157–162. [Google Scholar] [CrossRef]
- Kang, B.H.; Son, K.; Lee, K.B. Accuracy of five intraoral scanners and two laboratory scanners for a complete arch: A comparative in-vitro study. Appl. Sci. 2020, 10, 74. [Google Scholar] [CrossRef]
- Rehmann, P.; Sichwardt, V.; Wöstmann, B. Intraoral Scanning Systems: Need for Maintenance. Int. J. Prosthodont. 2017, 30, 27–29. [Google Scholar] [CrossRef] [PubMed]
- Schimmel, M.; Akino, N.; Srinivasan, M.; Wittneben, J.G.; Yilmaz, B.; Abou-Ayash, S. Accuracy of intraoral scanning in completely and partially edentulous maxillary and mandibular jaws: An in vitro analysis. Clin. Oral Investig. 2021, 25, 1839–1847. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Alfaraj, A.; Khanlar, L.N.; Lin, W.S.; Zandinejad, A. Exploring the impact of the extent of the partially edentulous area on the accuracy of two intraoral scanners. J. Prosthet. Dent. 2024, 131, 163.e1–163.e8. [Google Scholar] [CrossRef]




| Discrepancy | Theoretical Mean | p Value | ||||||
|---|---|---|---|---|---|---|---|---|
| VV np | VV p | NOT np | NOT p | IOS np | IOS p | |||
| A1-B1 | 0.3075 | 0.5445 | 0.4465 | 0.671 | 0.5045 | 0.2975 | 50.71 | <0.0001 |
| R3-L3 | 0.9015 | 1.164 | 1.103 | 1.313 | 1.103 | 1.199 | 33.7 | |
| R1-L1 | 1.245 | 1.158 | 1.315 | 1.108 | 1.201 | 1.084 | 24.7 | |
| A2-L2 | 0.265 | 0.3665 | 0.631 | 0.576 | 0.360 | 0.3105 | 46.54 | |
| A2-D | 2.490 | 2.330 | 1.308 | 1.334 | 2.504 | 1.994 | 50.76 | |
| B2-R2 | 0.6945 | 0.7630 | 0.7295 | 0.898 | 0.685 | 0.752 | 46.54 | |
| B2-C | 3.278 | 1.316 | 1.023 | 0.979 | 1.691 | 3.941 | 50.76 | |
| Discrepancy | Theoretical Mean | p Value | ||||||
|---|---|---|---|---|---|---|---|---|
| VV np | VV p | NOT np | NOT p | IOS np | IOS p | |||
| a1-b1 | 0.049 | 0.339 | 0.111 | 0.0995 | −0.209 | 0.046 | 45.18 | <0.05 |
| r3-l3 | 1.375 | 1.036 | 1.147 | 1.280 | 1.148 | 0.9965 | 30.46 | |
| r1-l1 | 0.4901 | 0.6031 | 0.4821 | 0.7351 | 0.6216 | 0.6211 | 20.60 | |
| a2-l2 | 1.199 | 1.204 | 1.420 | 1.511 | 1.171 | 1.241 | 44.80 | |
| a2-d | 0.4915 | 0.4555 | 0.437 | 0.5965 | 1.051 | 0.604 | 58.46 | |
| b2-r2 | 0.5465 | 0.616 | 0.682 | 0.7565 | 0.5355 | 0.4955 | 44.80 | |
| b2-c | 0.0295 ns | 0.409 | 0.267 | 0.5565 | 0.059 ns | 0.4795 | 58.46 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jánosi, K.M.; Cerghizan, D.; Bai, E.E.; Mureșan, I.É.; Kovács, A.; Szász, A.; Hulpe, A.; Markovics, E.R.; Mártha, K.I.; Pop, S.I. An Evaluation of the Accuracy of Digital Models—An In Vitro Study. Dent. J. 2024, 12, 313. https://doi.org/10.3390/dj12100313
Jánosi KM, Cerghizan D, Bai EE, Mureșan IÉ, Kovács A, Szász A, Hulpe A, Markovics ER, Mártha KI, Pop SI. An Evaluation of the Accuracy of Digital Models—An In Vitro Study. Dentistry Journal. 2024; 12(10):313. https://doi.org/10.3390/dj12100313
Chicago/Turabian StyleJánosi, Kinga Mária, Diana Cerghizan, Eszter Elza Bai, Izabella Éva Mureșan, Alpár Kovács, Andrea Szász, Adrian Hulpe, Emese Rita Markovics, Krisztina Ildikó Mártha, and Silvia Izabella Pop. 2024. "An Evaluation of the Accuracy of Digital Models—An In Vitro Study" Dentistry Journal 12, no. 10: 313. https://doi.org/10.3390/dj12100313
APA StyleJánosi, K. M., Cerghizan, D., Bai, E. E., Mureșan, I. É., Kovács, A., Szász, A., Hulpe, A., Markovics, E. R., Mártha, K. I., & Pop, S. I. (2024). An Evaluation of the Accuracy of Digital Models—An In Vitro Study. Dentistry Journal, 12(10), 313. https://doi.org/10.3390/dj12100313