
Three-Dimensional Analysis of Upper and Lower Arches Using Digital Technology: Measurement of the Index of Bolton and Correspondence between Arch Shapesand Orthodontic Arches

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection Criteria
- -
- Caucasian ethnicity;
- -
- Permanent dentition;
- -
- Class I and absence of severe malocclusions;
- -
- Absence of dental extractions or extensive tooth reconstructions;
- -
- Absence of previous maxillo-facial surgery;
- -
- Absence of previous removable or fixed orthodontic treatments;
- -
- Three-dimensional dental casts scanned usingOrtho3shape software.
- -
- Presence of deciduous teeth;
- -
- Teeth with severe rotation;
- -
- Dental agenesis;
- -
- Oligodontia.
2.2. Clinical Procedures
2.3. Statistical Analysis
- -
- Full permanent dentition from right first molar to left first molar in both the upper and lower arches;
- -
- Absence of previous or current orthodontic treatment;
- -
- Absence of severe dental crowding [10].
3. Results
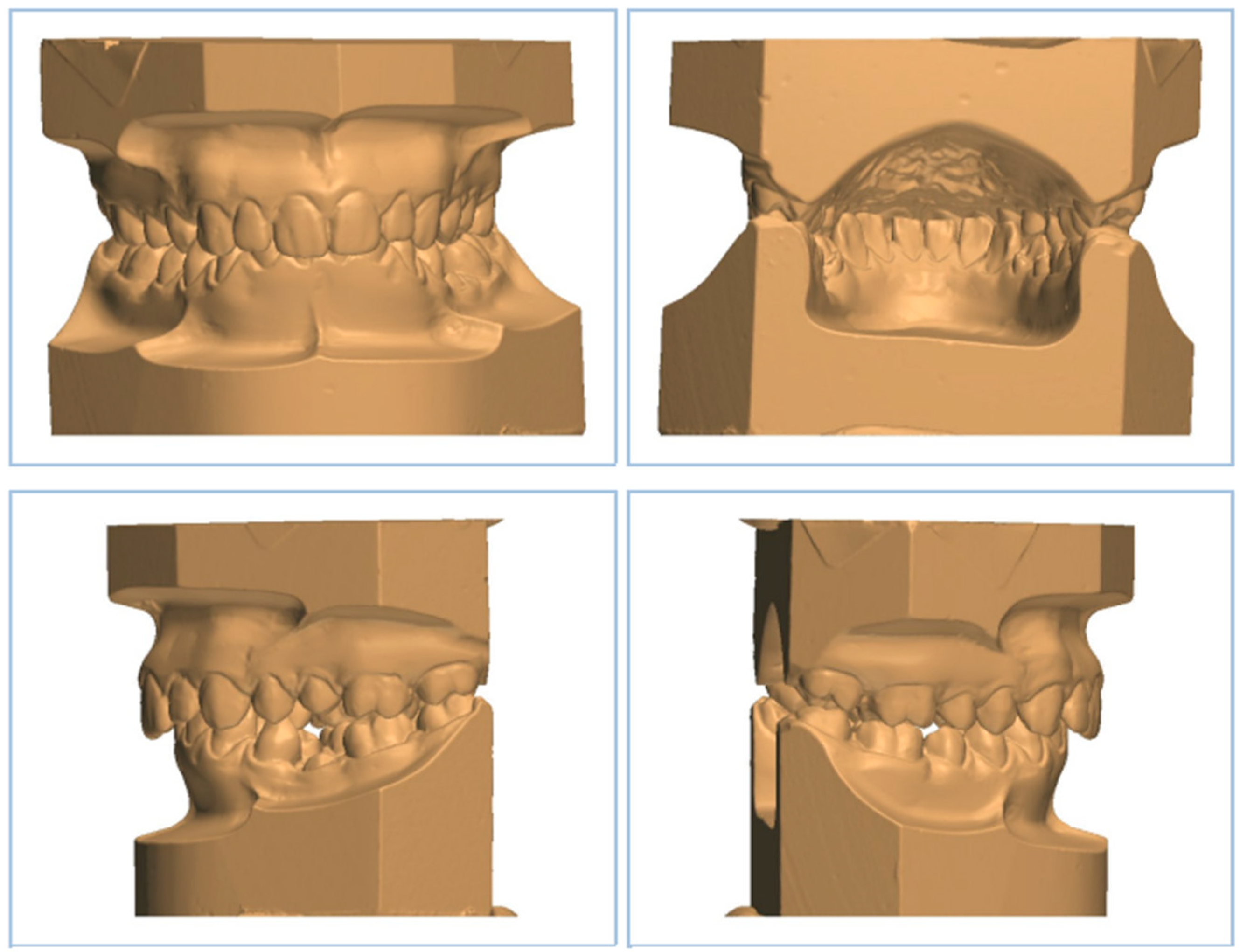
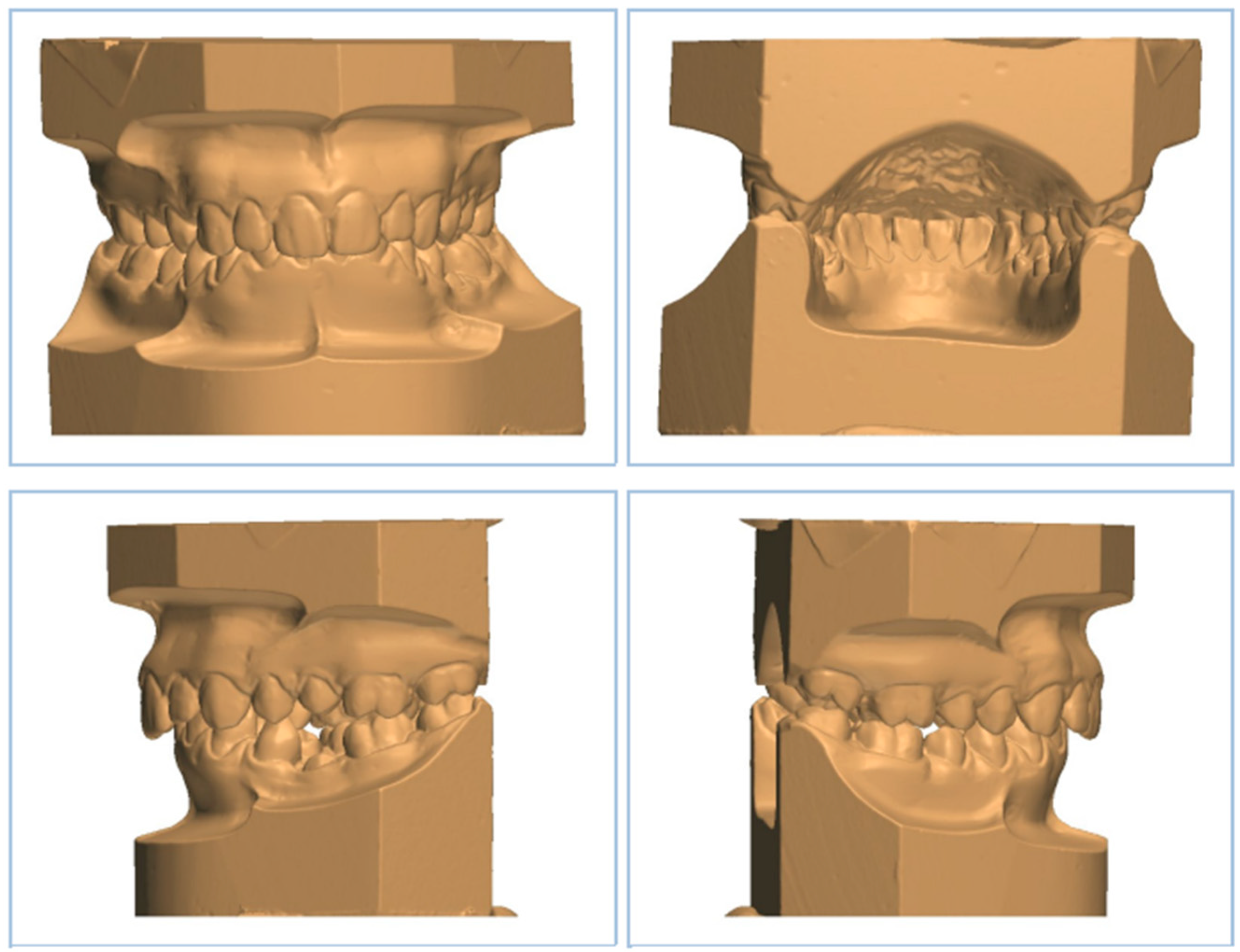
3.1. Digitaldental Casts Analysis
3.2. Bolton Analysis Comparison between Our Study and A. Anand Kumar et al.’s Study [10]
3.3. Comparisonof Anterior and Total Bolton Coefficients between the Two Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ardila, C.M.; Elorza-Durán, A.; Arrubla-Escobar, D. Efficacy of CAD/CAM Technology in Interventions Implemented in Orthodontics: A Scoping Review of Clinical Trials. Biomed. Res. Int. 2022, 2022, 5310555. [Google Scholar] [CrossRef] [PubMed]
- Bosio, J.A.; Rozhitsky, F.; Jiang, S.S.; Mukherjee, P.; Cangialosi, T.J. Comparison of Scanning Times for Different Dental Cast Materials Using an Intraoral Scanner; Rutgers School of Dental Medicine: Newark, NJ, USA, 2017. [Google Scholar]
- Ferreira, J.B.; Christovam, I.O.; Alencar, D.S.; da Motta, A.F.J.; Mattos, C.T.; Cury-Saramago, A. Accuracy and reproducibility of dental measurements on tomographic digital models: A systematic review and meta-analysis. Dentomaxillofac. Radiol. 2017, 46, 20160455. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, L.; Sabbagh, H.; Wichelhaus, A.; Kessler, A. Bracket transfer accuracy with two different three-dimensional printed transfer trays vs silicone transfer trays. Angle Orthod. 2022, 92, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Zheng, Y.; Zhang, Z.; Zhang, Z.; Wu, L.; Liu, J.; Yang, W.; Wang, J. Customized maxillary incisor position relative to dentoskeletal and soft tissue patterns in Chinese women: A retrospective study. Korean J. Orthod. 2022, 52, 150–160. [Google Scholar] [CrossRef] [PubMed]
- Kustrzycka, D.; Marschang, T.; Mikulewicz, M.; Grzebieluch, W. Comparison of the Accuracy of 3D Images Obtained fromDifferent Types of Scanners: A Systematic Review. J. Healthc. Eng. 2020, 2020, 8854204. [Google Scholar] [CrossRef] [PubMed]
- Sabbagh, H.; Heger, S.M.; Stocker, T.; Baumert, U.; Wichelhaus, A.; Hoffmann, L. Accuracy of 3D Tooth Movements in the Fabrication of Manual Setup Models for Aligner Therapy. Materials 2022, 15, 3853. [Google Scholar] [CrossRef] [PubMed]
- Nota, A.; Chegodaeva, A.D.; Ryakhovsky, A.N.; Vykhodtseva, M.A.; Pittari, L.; Tecco, S. One-Stage Virtual Plan of a Complex Orthodontic/Prosthetic Dental Rehabilitation. Int. J. Environ. Res. Public Health 2022, 19, 1474. [Google Scholar] [CrossRef] [PubMed]
- Tartaglia, G.M.; Mapelli, A.; Maspero, C.; Santaniello, T.; Serafin, M.; Farronato, M.; Caprioglio, A. Direct 3D Printing of Clear Orthodontic Aligners: Current State and Future Possibilities. Materials 2021, 14, 1799. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Phillip, A.; Kumar, S.; Rawat, A.; Priya, S.; Kumaran, V. Digital model as an alternative to plaster model in assessment of space analysis. J. Pharm. Bioallied Sci. 2015, 7 (Suppl. S2), S465–S469. [Google Scholar] [CrossRef] [PubMed]
- Moura, W.; Henriques, J.F.C.; Gambardela-Tkacz, C.M.; Cotrin, P.; Garib, D.; Janson, G. Mandibular incisor inclination and gingival recession after treatment with the Jasper Jumper: A 10-year follow-up. Prog. Orthod. 2021, 22, 45. [Google Scholar] [CrossRef] [PubMed]
- De Morais Alves da Cunha, T.; da Silva Barbosa, I.; Palma, K.K. Orthodontic digital workflow: Devices and clinical applications. Dent. Press J. Orthod. 2021, 26, e21spe6. [Google Scholar] [CrossRef] [PubMed]
- Mai, H.-N.; Lee, D.-H. Accuracy of Mobile Device-Compatible 3D Scanners for Facial Digitization: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2020, 22, e22228. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, T.; Marano, G.; Aulakh, R. Five-to-five clear aligner therapy: Predictable orthodontic movement for general dentist to achieve minimally invasive dentistry. BMC Oral Health 2021, 21, 671. [Google Scholar] [CrossRef] [PubMed]
- Pachêco-Pereira, C.; De Luca Canto, G.; Major, P.W.; Flores-Mir, C. Variation of orthodontic treatment decision-making based on dental model type: A systematic review. Angle Orthod. 2015, 85, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Faus-Matoses, I.; Barona, C.G.; Zubizarreta-Macho, Á.; Paredes-Gallardo, V.; Faus-Matoses, V. A Novel Digital Technique for Measuring the Accuracy of an Indirect Bonding Technique Using Fixed Buccal Multibracket Appliances. J. Pers. Med. 2021, 11, 932. [Google Scholar] [CrossRef] [PubMed]
- Jaber, S.T.; Hajeer, M.Y.; Khattab, T.Z.; Mahaini, L. Evaluation of the fused deposition modeling and the digital light processing techniques in terms of dimensional accuracy of printing dental models used for the fabrication of clear aligners. Clin. Exp. Dent. Res. 2021, 7, 591–600. [Google Scholar] [CrossRef] [PubMed]
- Etemad-Shahidi, Y.; Qallandar, O.B.; Evenden, J.; Alifui-Segbaya, F.; Ahmed, K.E. Accuracy of 3-Dimensionally Printed Full-Arch Dental Models: A Systematic Review. J. Clin. Med. 2020, 9, 3357. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, G.; Campobasso, A.; Caldara, G.; Battista, G.; Lo Muzio, E.; Mandelli, G.; Ambrosi, A.; Gastaldi, G. Accuracy of 3-dimensional-printed customized transfer tray using a flash-free adhesive system in digital indirect bonding: An in vivo study. Am. J. Orthod. Dentofac. Orthop. 2023; in press. [Google Scholar]
- Proffit, W.R.; Fields, H.W., Jr.; Larson, B.; Sarver, D.M. Contemporary Orthodontics, 6th ed.; Elsevier: Filadelfia, PA, USA, 2019. [Google Scholar]

{kind=link}
| Upper Arch Analysis | Hypothetical Nickel Titanium Orthodontic Wire Upper Archlength (mm) | Upper Arch Length (mm) |
|---|---|---|
| Maximum Value | 124.33 | 108.07 |
| Minimum Value | 80.03 | 66.47 |
| Mean Value | 103.79 | 92.13 |
| Lower Arch Analysis | Hypothetical Nickel Titanium Orthodontic Wire Lower Archlength(mm) | Lower Arch Length (mm) |
|---|---|---|
| Maximum Value | 109.91 | 107.63 |
| Minimum Value | 75.32 | 68.47 |
| Mean Value | 94.71 | 88.26 |
| Bolton Analysis: Anterior Coefficient | Maxillary Teeth (mm) | Mandibular Teeth (mm) | Bolton Value |
|---|---|---|---|
| Maximum Value | 45.54 | 35.69 | 1.16 |
| Minimum Value | 24.33 | 22.58 | 0.62 |
| Mean Value | 38.16 | 30.10 | 0.79 |
| Bolton Analysis: Total Coefficient | Maxillary Teeth (mm) | Mandibular Teeth (mm) | Bolton Value |
|---|---|---|---|
| Maximum Value | 89.25 | 88.78 | 1.21 |
| Minimum Value | 58.10 | 53.39 | 0.68 |
| Mean Value | 78.99 | 73.77 | 0.94 |
| Mean Value | A. Anand Kumar et al.’s Study | Present Study | p Value |
|---|---|---|---|
| Anterior coefficient | 0.76 | 0.79 | 0.0028 |
| Total coefficient | 0.91 | 0.94 | 0.0009 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pasini, M.; Carli, E.; Giambastiani, F.; Giuca, M.R.; Tripodi, D. Three-Dimensional Analysis of Upper and Lower Arches Using Digital Technology: Measurement of the Index of Bolton and Correspondence between Arch Shapesand Orthodontic Arches. Dent. J. 2023, 11, 188. https://doi.org/10.3390/dj11080188
Pasini M, Carli E, Giambastiani F, Giuca MR, Tripodi D. Three-Dimensional Analysis of Upper and Lower Arches Using Digital Technology: Measurement of the Index of Bolton and Correspondence between Arch Shapesand Orthodontic Arches. Dentistry Journal. 2023; 11(8):188. https://doi.org/10.3390/dj11080188
Chicago/Turabian StylePasini, Marco, Elisabetta Carli, Federico Giambastiani, Maria Rita Giuca, and Domenico Tripodi. 2023. "Three-Dimensional Analysis of Upper and Lower Arches Using Digital Technology: Measurement of the Index of Bolton and Correspondence between Arch Shapesand Orthodontic Arches" Dentistry Journal 11, no. 8: 188. https://doi.org/10.3390/dj11080188
APA StylePasini, M., Carli, E., Giambastiani, F., Giuca, M. R., & Tripodi, D. (2023). Three-Dimensional Analysis of Upper and Lower Arches Using Digital Technology: Measurement of the Index of Bolton and Correspondence between Arch Shapesand Orthodontic Arches. Dentistry Journal, 11(8), 188. https://doi.org/10.3390/dj11080188