


Clinical Evaluation of Corrosion Resistance, Ion Release, and Biocompatibility of CoCr Alloy for Metal-Ceramic Restorations Produced by CAD/CAM Technologies

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
Statistics
3. Results
4. Discussion
5. Conclusions
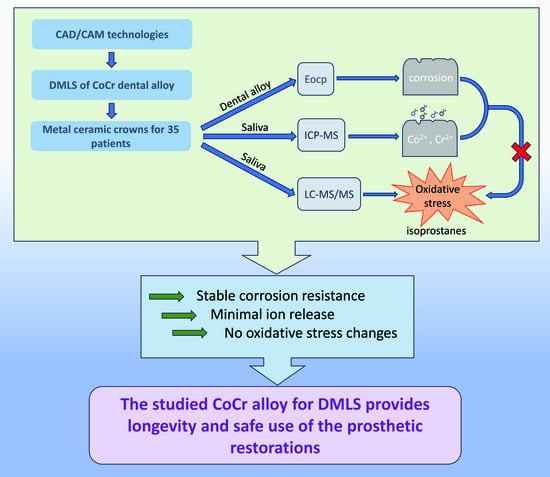
- Co ion emission significantly increases 2 h after intraoral placement.
- Seven days after placement in the oral cavity, the metal ion release from the studied alloy is insignificant compared to the initial metal ion concentration in non-stimulated saliva.
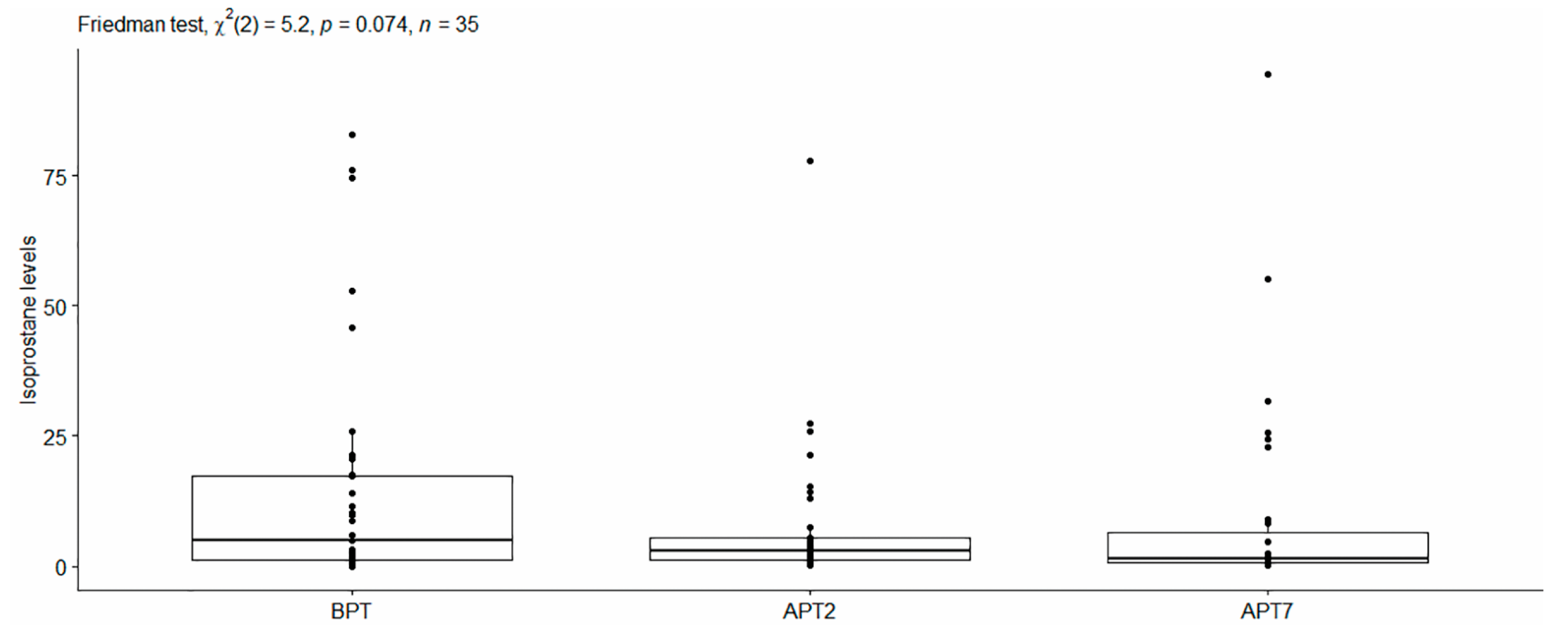
- No correlation exists between the metal ion emission and the concentration of 8-isoPGF2-alpha in non-stimulated saliva.
- Regarding the constant in-time Eocp values, the studied dental alloy has high and stable resistance to corrosion.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alharbi, N.; Wismeijer, D.; Osman, R.B. Additive Manufacturing Techniques in Prosthodontics: Where Do We Currently Stand? A Critical Review. Int. J. Prosthodont. 2017, 30, 474–484. [Google Scholar] [CrossRef] [PubMed]
- Alghazzawi, T.F. Advancements in CAD/CAM technology: Options for practical implementation. J. Prosthodont. Res. 2016, 60, 72–84. [Google Scholar] [CrossRef] [PubMed]
- Takaichi, A.; Suyalatu; Nakamoto, T.; Joko, N.; Nomura, N.; Tsutsumi, Y.; Migita, S.; Doi, H.; Kurosu, S.; Chiba, A.; et al. Microstructures and mechanical properties of Co–29Cr–6Mo alloy fabricated by selective laser melting process for dental applications. J. Mech. Behav. Biomed. Mater. 2013, 21, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.-K.; Kim, S.-K.; Heo, S.-J.; Koak, J.-Y. Mechanical Properties and Metal-Ceramic Bond Strength of Co-Cr Alloy Manufactured by Selective Laser Melting. Materials 2020, 13, 5745. [Google Scholar] [CrossRef]
- Marti, A. Cobalt-base alloys used in bone surgery. Injury 2000, 31 (Suppl. 4), D18–D21. [Google Scholar] [CrossRef]
- Girão, D.D.C.; Béreš, M.; Jardini, A.L.; Filho, R.M.; Silva, C.C.; de Siervo, A.; de Abreu, H.F.G.; Araújo, W.S. An assessment of biomedical CoCrMo alloy fabricated by direct metal laser sintering technique for implant applications. Mater. Sci. Eng. C 2019, 107, 110305. [Google Scholar] [CrossRef]
- Sterzenbach, T.; Helbig, R.; Hannig, C.; Hannig, M. Bioadhesion in the oral cavity and approaches for biofilm management by surface modifications. Clin. Oral Investig. 2020, 24, 4237–4260. [Google Scholar] [CrossRef]
- Tuna, S.H.; Pekmez, N.; Keyf, F.; Canlı, F. The influence of the pure metal components of four different casting alloys on the electrochemical properties of the alloys. Dent. Mater. 2009, 25, 1096–1103. [Google Scholar] [CrossRef]
- Eliaz, N. Corrosion of Metallic Biomaterials: A Review. Materials 2019, 12, 407. [Google Scholar] [CrossRef]
- Procházková, J.; Podzimek, S.; Tomka, M.; Kucerová, H.; Mihaljevic, M.; Hána, K. Metal alloys in the oral cavity as a cause of oral discomfort in sensitive patients. Neuro Endocrinol. Lett. 2006, 27 (Suppl. 1), 53–58. [Google Scholar]
- Lu, C.; Zheng, Y.; Zhong, Q. Corrosion of dental alloys in artificial saliva with Streptococcus mutans. PLoS ONE 2017, 12, e0174440. [Google Scholar] [CrossRef] [PubMed]
- Močnik, P.; Kosec, T.; Kovač, J.; Bizjak, M. The effect of pH, fluoride and tribocorrosion on the surface properties of dental archwires. Mater. Sci. Eng. C 2017, 78, 682–689. [Google Scholar] [CrossRef]
- Faccioni, F.; Franceschetti, P.; Cerpelloni, M.; Fracasso, M.E. In vivo study on metal release from fixed orthodontic appliances and DNA damage in oral mucosa cells. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Xia, G.; Cao, X.-M.; Wang, J.; Xu, B.-Y.; Huang, P.; Chen, Y.; Jiang, Q.-W. Urinary levels of nickel and chromium associated with dental restoration by nickel–chromium based alloys. Int. J. Oral Sci. 2013, 5, 44–48. [Google Scholar] [CrossRef]
- Keegan, G.M.; Learmonth, I.D.; Case, C.P. A systematic comparison of the actual, potential, and theoretical health effects of cobalt and chromium exposures from industry and surgical implants. Crit. Rev. Toxicol. 2008, 38, 645–674. [Google Scholar] [CrossRef]
- Zhou, J.; Paul, A.; Bennani, V.; Thomson, W.M.; Firth, N. New Zealand dental practitioners’ experience of patient allergies to dental alloys used for prosthodontics. N. Z. Dent. J. 2010, 106, 55. [Google Scholar]
- Akbar, M.; Brewer, J.M.; Grant, M.H. Effect of chromium and cobalt ions on primary human lymphocytes in vitro. J Immunotoxicol. 2011, 8, 140–149. [Google Scholar] [CrossRef]
- Yamada, K. Cobalt: Its Role in Health and Disease. Met. Ions Life Sci. 2013, 13, 295–320. [Google Scholar] [CrossRef] [PubMed]
- Permenter, M.G.; Dennis, W.E.; Sutto, T.E.; Jackson, D.A.; Lewis, J.A.; Stallings, J.D. Exposure to Cobalt Causes Transcriptomic and Proteomic Changes in Two Rat Liver Derived Cell Lines. PLoS ONE 2013, 8, e83751. [Google Scholar] [CrossRef]
- Kumagai, S.; Kusaka, Y.; Goto, S. Cobalt Exposure Level and Variability in the Hard Metal Industry of Japan. Am. Ind. Hyg. Assoc. J. 1996, 57, 365–369. [Google Scholar] [CrossRef]
- Li, P.; Ding, D.; Salvi, R.; Roth, J.A. Cobalt-Induced Ototoxicity in Rat Postnatal Cochlear Organotypic Cultures. Neurotox. Res. 2015, 28, 209–221. [Google Scholar] [CrossRef] [PubMed]
- DNEL Chromium. Available online: https://echa.europa.eu/bg/registration-dossier/-/registered-dossier/15551/4/1 (accessed on 6 July 2023).
- Maret, W. Chromium Supplementation in Human Health, Metabolic Syndrome, and Diabetes. Met. Ions Life Sci. 2019, 19, 231–252. [Google Scholar] [CrossRef]
- Pavesi, T.; Moreira, J.C. Mechanisms and individuality in chromium toxicity in humans. J. Appl. Toxicol. 2020, 40, 1183–1197. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-X.; Wu, X.; Bi, R.; Li, L.-X.; Gao, M.; Li, D.; Xie, L.-T. Mechanisms of Cr (VI) toxicity to fish in aquatic environment: A review. Ying Yong Sheng Tai Xue Bao = J. Appl. Ecol. 2015, 26, 3226–3234. [Google Scholar]
- Al Jabbari, Y.S.; Barmpagadaki, X.; Psarris, I.; Zinelis, S. Microstructural, mechanical, ionic release and tarnish resistance characterization of porcelain fused to metal Co-Cr alloys manufactured via casting and three different CAD/CAM techniques. J. Prosthodont. Res. 2019, 63, 150–156. [Google Scholar] [CrossRef]
- Beck, K.A.; Sarantopoulos, D.M.; Kawashima, I.; Berzins, D.W. Elemental Release from CoCr and NiCr Alloys Containing Palladium. J. Prosthodont. 2012, 21, 88–93. [Google Scholar] [CrossRef]
- Denizoğlu, S.; Duymuş, Z.Y.; Akyalçin, Ş. Evaluation of Ion Release from Two Base-Metal Alloys at Various pH Levels. J. Int. Med. Res. 2004, 32, 33–38. [Google Scholar] [CrossRef]
- Garhammer, P.; Hiller, K.-A.; Reitinger, T.; Schmalz, G. Metal content of saliva of patients with and without metal restorations. Clin. Oral Investig. 2004, 8, 238–242. [Google Scholar] [CrossRef]
- Siddharth, R.; Gautam, R.; Chand, P.; Agrawal, K.K.; Singh, R.D.; Singh, B.P. Quantitative analysis of leaching of different metals in human saliva from dental casting alloys: An in vivo study. J. Indian Prosthodont. Soc. 2015, 15, 206–210. [Google Scholar] [CrossRef]
- Singh, D.P.; Sehgal, V.; Pradhan, K.L.; Chandna, A.; Gupta, R. Estimation of nickel and chromium in saliva of patients with fixed orthodontic appliances. World J. Orthod. 2008, 9, 196–202. [Google Scholar]
- Velasco-Ibáñez, R.; Lara-Carrillo, E.; Morales-Luckie, R.A.; Romero-Guzmán, E.T.; Toral-Rizo, V.H.; Ramírez-Cardona, M.; García-Hernández, V.; Medina-Solís, C.E. Evaluation of the release of nickel and titanium under orthodontic treatment. Sci. Rep. 2020, 10, 22280. [Google Scholar] [CrossRef] [PubMed]
- Vaicelyte, A.; Janssen, C.; Le Borgne, M.; Grosgogeat, B. Cobalt–Chromium Dental Alloys: Metal Exposures, Toxicological Risks, CMR Classification, and EU Regulatory Framework. Crystals 2020, 10, 1151. [Google Scholar] [CrossRef]
- Jakubczyk, K.; Dec, K.; Kałduńska, J.; Kawczuga, D.; Kochman, J.; Janda, K. Reactive oxygen species—Sources, functions, oxidative damage. Pol. Merkur. Lekarski. 2020, 48, 124–127. [Google Scholar]
- Yang, S.; Lian, G. ROS and diseases: Role in metabolism and energy supply. Mol. Cell. Biochem. 2019, 467, 1–12. [Google Scholar] [CrossRef]
- Tóthová, L.; Kamodyová, N.; Červenka, T.; Celec, P. Salivary markers of oxidative stress in oral diseases. Front. Cell. Infect. Microbiol. 2015, 5, 73. [Google Scholar] [CrossRef] [PubMed]
- Catalá, A. Lipid peroxidation of membrane phospholipids generates hydroxy-alkenals and oxidized phospholipids active in physiological and/or pathological conditions. Chem. Phys. Lipids 2009, 157, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Gornitsky, M.; Velly, A.M.; Yu, H.; Benarroch, M.; Schipper, H.M. Salivary DNA, lipid, and protein oxidation in nonsmokers with periodontal disease. Free. Radic. Biol. Med. 2009, 46, 914–921. [Google Scholar] [CrossRef]
- Avezov, K.; Reznick, A.Z.; Aizenbud, D. Oxidative stress in the oral cavity: Sources and pathological outcomes. Respir. Physiol. Neurobiol. 2015, 209, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Żukowski, P.; Maciejczyk, M.; Waszkiel, D. Sources of free radicals and oxidative stress in the oral cavity. Arch. Oral Biol. 2018, 92, 8–17. [Google Scholar] [CrossRef]
- Zieniewska, I.; Maciejczyk, M.; Zalewska, A. The Effect of Selected Dental Materials Used in Conservative Dentistry, Endodontics, Surgery, and Orthodontics as Well as during the Periodontal Treatment on the Redox Balance in the Oral Cavity. Int. J. Mol. Sci. 2020, 21, 9684. [Google Scholar] [CrossRef]
- Battaglia, V.; Compagnone, A.; Bandino, A.; Bragadin, M.; Rossi, C.A.; Zanetti, F.; Colombatto, S.; Grillo, M.A.; Toninello, A. Cobalt induces oxidative stress in isolated liver mitochondria responsible for permeability transition and intrinsic apoptosis in hepatocyte primary cultures. Int. J. Biochem. Cell Biol. 2009, 41, 586–594. [Google Scholar] [CrossRef] [PubMed]
- Özcan, S.S.A.; Ceylan, I.; Özcan, E.; Kurt, N.; Dağsuyu, I.M.; Çanakçi, C.F. Evaluation of Oxidative Stress Biomarkers in Patients with Fixed Orthodontic Appliances. Dis. Markers 2014, 2014, 597892. [Google Scholar] [CrossRef]
- Schedle, A.; Samorapoompichit, P.; Rausch-Fan, X.; Franz, A.; Füreder, W.; Sperr, W.; Ellinger, A.; Slavicek, R.; Boltz-Nitulescu, G.; Valent, P. Response of L-929 Fibroblasts, Human Gingival Fibroblasts, and Human Tissue Mast Cells to Various Metal Cations. J. Dent. Res. 1995, 74, 1513–1520. [Google Scholar] [CrossRef] [PubMed]
- Ganbold, B.; Heo, S.-J.; Koak, J.-Y.; Kim, S.-K.; Cho, J. Human Stem Cell Responses and Surface Characteristics of 3D Printing Co-Cr Dental Material. Materials 2019, 12, 3419. [Google Scholar] [CrossRef]
- Tomova, Z.; Tomov, D.; Vlahova, A.; Chaova-Gizdakova, V.; Yoanidu, L.; Svinarov, D. Development and validation of an LC-MS/MS method for determination of 8-iso-prostaglandin F2 alpha in human saliva. J. Med. Biochem. 2022, 41, 466–473. [Google Scholar] [CrossRef]
- EOS SP2 Safety Data Sheet [Internet]. Available online: https://www.infinidentsolutions.com/assets/uploads/service/safety-data-sheets/sds-eos-cobaltchrome-sp2-en.pdf (accessed on 5 June 2023).
- Padrós, R.; Giner-Tarrida, L.; Herrero-Climent, M.; Punset, M.; Gil, F.J. Corrosion Resistance and Ion Release of Dental Prosthesis of CoCr Obtained by CAD-CAM Milling, Casting and Laser Sintering. Metals 2020, 10, 827. [Google Scholar] [CrossRef]
- Barrett, R.D.; Bishara, S.E.; Quinn, J.K. Biodegradation of orthodontic appliances. Part, I. Biodegradation of nickel and chromium in vitro. Am. J. Orthod. Dentofac. Orthop. Off. Publ. Am. Assoc. Orthod. Its Const. Soc. Am. Board. Orthod. 1993, 103, 8–14. [Google Scholar] [CrossRef]
- Amini, F.; Rakhshan, V.; Mesgarzadeh, N. Effects of Long-Term Fixed Orthodontic Treatment on Salivary Nickel and Chromium Levels: A 1-Year Prospective Cohort Study. Biol. Trace Element Res. 2012, 150, 15–20. [Google Scholar] [CrossRef]
- Fors, R.; Persson, M. Nickel in dental plaque and saliva in patients with and without orthodontic appliances. Eur. J. Orthod. 2005, 28, 292–297. [Google Scholar] [CrossRef]
- Kovač, V.; Poljšak, B.; Primožič, J.; Jamnik, P. Are Metal Ions That Make up Orthodontic Alloys Cytotoxic, and Do They Induce Oxidative Stress in a Yeast Cell Model? Int. J. Mol. Sci. 2020, 21, 7993. [Google Scholar] [CrossRef]
- McGinley, E.L.; Moran, G.P.; Fleming, G.J. Biocompatibility effects of indirect exposure of base-metal dental casting alloys to a human-derived three-dimensional oral mucosal model. J. Dent. 2013, 41, 1091–1100. [Google Scholar] [CrossRef] [PubMed]
- Ekuni, D.; Tomofuji, T.; Tamaki, N.; Sanbe, T.; Azuma, T.; Yamanaka, R.; Yamamoto, T.; Watanabe, T. Mechanical stimulation of gingiva reduces plasma 8-OHdG level in rat periodontitis. Arch. Oral Biol. 2008, 53, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Kamodyová, N.; Tóthová, L.; Celec, P. Salivary markers of oxidative stress and antioxidant status: Influence of external factors. Dis. Markers 2013, 34, 313–321. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Element | Wt-% |
|---|---|
| Co | 63.8 |
| Cr | 24.7 |
| Mo | 5.1 |
| W | 5.4 |
| Si | 1 |
| Fe | Max. 0.5 |
| Mn | Max. 0.1 |
| Free of Ni, Be, Cd, and Pb according to ISO 22674 | |
| Variable | n | Min | Max | Median | Mean | sd | |
|---|---|---|---|---|---|---|---|
| BPT | value | 35 | 0 | 82.79 | 4.84 | 15.13 | 23.022 |
| APT2 | value | 35 | 0.11 | 77.93 | 2.85 | 7.543 | 14.171 |
| APT7 | value | 35 | 0.04 | 94.54 | 1.48 | 8.959 | 18.984 |
| Ion | Time | Variable | n | Min | Max | Median | Mean | sd |
|---|---|---|---|---|---|---|---|---|
| Co | BPT | value | 35 | 0.02 | 3.45 | 0.22 | 0.581 | 0.831 |
| APT2 | value | 35 | 0.01 | 6.18 | 0.56 | 0.992 * | 1.276 | |
| APT7 | value | 35 | 0.01 | 4.58 | 0.18 | 0.628 | 1.232 | |
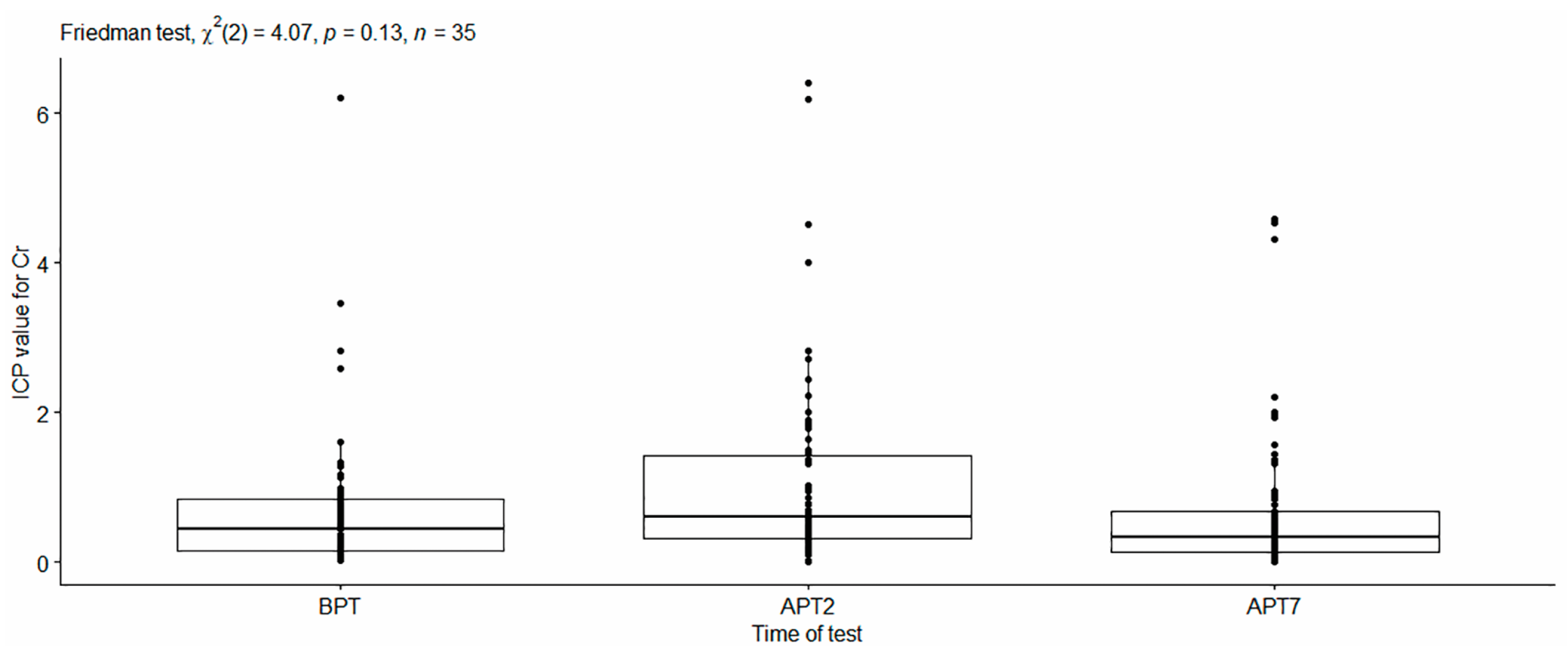
| Cr | BPT | value | 35 | 0.02 | 6.21 | 0.66 | 0.777 | 1.025 |
| APT2 | value | 35 | 0.19 | 6.41 | 0.64 | 1.138 | 1.27 | |
| APT7 | value | 35 | 0.08 | 2.21 | 0.47 | 0.697 | 0.605 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomova, Z.; Vlahova, A.; Zlatev, S.; Stoeva, I.; Tomov, D.; Davcheva, D.; Hadzhigaev, V. Clinical Evaluation of Corrosion Resistance, Ion Release, and Biocompatibility of CoCr Alloy for Metal-Ceramic Restorations Produced by CAD/CAM Technologies. Dent. J. 2023, 11, 166. https://doi.org/10.3390/dj11070166
Tomova Z, Vlahova A, Zlatev S, Stoeva I, Tomov D, Davcheva D, Hadzhigaev V. Clinical Evaluation of Corrosion Resistance, Ion Release, and Biocompatibility of CoCr Alloy for Metal-Ceramic Restorations Produced by CAD/CAM Technologies. Dentistry Journal. 2023; 11(7):166. https://doi.org/10.3390/dj11070166
Chicago/Turabian StyleTomova, Zlatina, Angelina Vlahova, Stefan Zlatev, Ilyana Stoeva, Desislav Tomov, Delyana Davcheva, and Viktor Hadzhigaev. 2023. "Clinical Evaluation of Corrosion Resistance, Ion Release, and Biocompatibility of CoCr Alloy for Metal-Ceramic Restorations Produced by CAD/CAM Technologies" Dentistry Journal 11, no. 7: 166. https://doi.org/10.3390/dj11070166
APA StyleTomova, Z., Vlahova, A., Zlatev, S., Stoeva, I., Tomov, D., Davcheva, D., & Hadzhigaev, V. (2023). Clinical Evaluation of Corrosion Resistance, Ion Release, and Biocompatibility of CoCr Alloy for Metal-Ceramic Restorations Produced by CAD/CAM Technologies. Dentistry Journal, 11(7), 166. https://doi.org/10.3390/dj11070166