
Drugs Prescribed for Asthma and Their Adverse Effects on Dental Health

 ,
,  and
and 
Abstract

1. Introduction
2. Materials and Methods
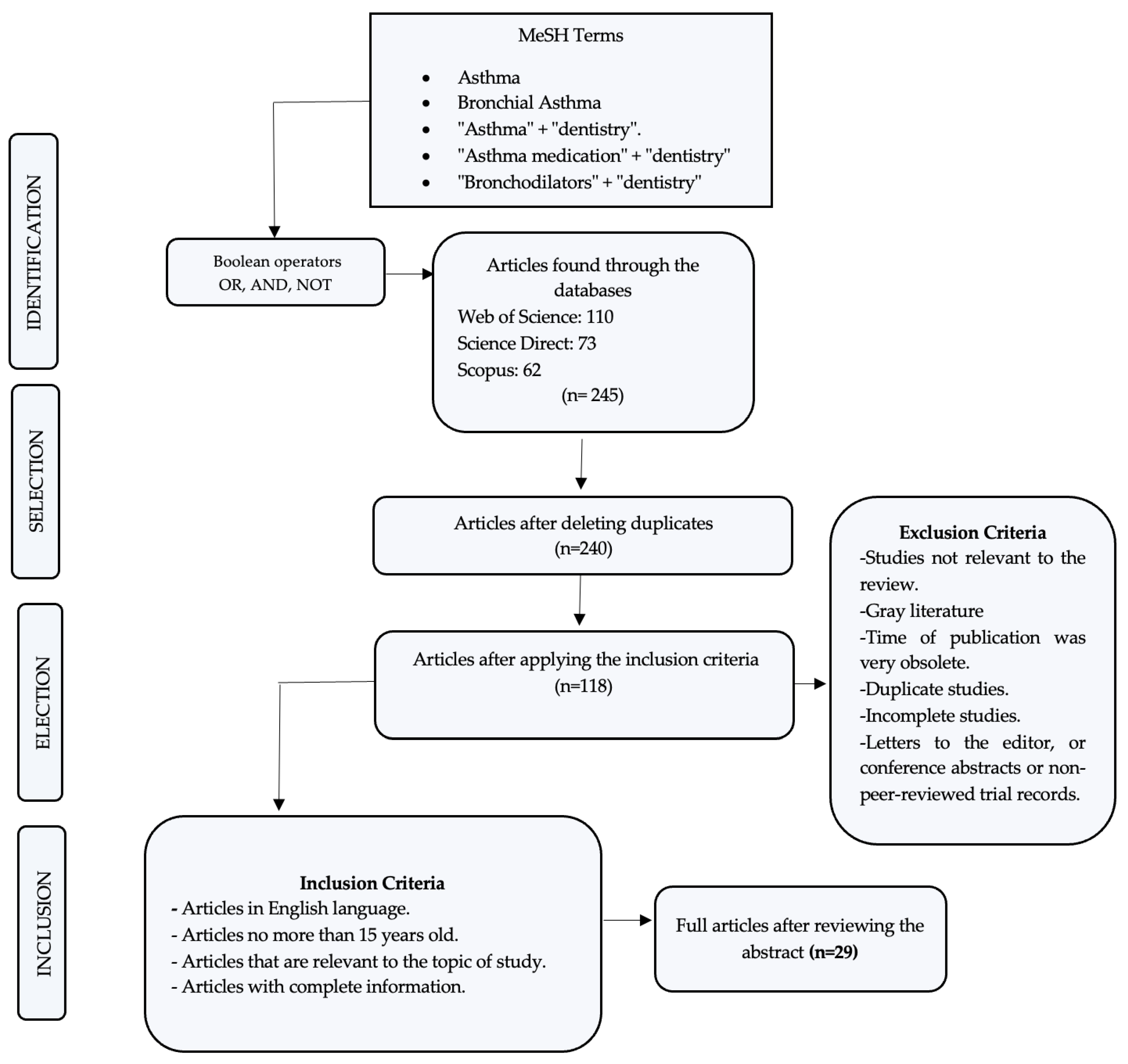
2.1. Bibliographic Search
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Data Analysis
3. Results
3.1. Effects on Dental Health
3.1.1. Asthma and Dental Caries
3.1.2. Asthma and Oral Candidiasis
3.1.3. Asthma and Periodontal Disease
3.1.4. Asthma and Dental Erosion
4. Discussion
4.1. Perspectives
4.2. Strengths
4.3. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| GINA | Global Initiative for Asthma |
| NAEPP | National Asthma Education and Prevention Program |
| BTS | British Thoracic Society |
| WHO | World Health Organization |
| ICS | Inhaled corticosteroids |
| LABA | Long-acting β2-adrenergic agonists |
| SABA | Short-acting β2-adrenergic agonists |
| MDI | Pressurized metered-dose inhaler |
| DPI | Dry power inhaler |
| SIg-A | Secreted immunoglobulin A |
| IgA | Immunoglobulin A |
| DMTF | Decayed, Missing, and Filled Teeth index |
| PFT | Pulmonary function tests |
| OH: SALSA | Health Oral San Antonio Longitudinal Study of Aging |
| LS | Lumbar spine |
| FN | Femoral neck |
| DEXA | Dual energy X-ray absorptiometry |
| BMD | Bone mineral density |
| PPD | Probing depth |
| CAL | Clinical attachment level. |
| START | Steroids as regular therapy. |
| GOHAI | General Oral Health Assessment Index. |
References
- Boonpiyathad, T.; Sözener, Z.C.; Satitsuksanoa, P.; Akdis, C.A. Immunologic Mechanisms in Asthma. Semin. Immunol. 2019, 46, 101333. [Google Scholar] [CrossRef]
- Gani, F.; Caminati, M.; Bellavia, F.; Baroso, A.; Faccioni, P.; Pancera, P.; Batani, V.; Senna, G. Oral Health in Asthmatic Patients: A Review: Asthma and Its Therapy May Impact on Oral Health. Clin. Mol. Allergy 2020, 18, 22. [Google Scholar] [CrossRef]
- Quirt, J.; Hildebrand, K.J.; Mazza, J.; Noya, F.; Kim, H. Asthma. Allergy Asthma Clin. Immunol. 2018, 14, 1–16. [Google Scholar] [CrossRef]
- O’Byrne, P.; Fabbri, L.M.; Pavord, I.D.; Papi, A.; Petruzzelli, S.; Lange, P. Asthma Progression and Mortality: The Role of Inhaled Corticosteroids. Eur. Respir. J. 2019, 54, 1900491. [Google Scholar] [CrossRef]
- Dharmage, S.C.; Perret, J.L.; Custovic, A. Epidemiology of Asthma in Children and Adults. Front. Pediatr. 2019, 7, 246. [Google Scholar] [CrossRef]
- Kudo, M.; Ishigatsubo, Y.; Aoki, I. Pathology of Asthma. Front. Microbiol. 2013, 4, 1–16. [Google Scholar] [CrossRef]
- Stern, J.; Pier, J.; Litonjua, A.A. Asthma Epidemiology and Risk Factors. Semin. Immunopathol. 2020, 42, 5–15. [Google Scholar] [CrossRef]
- Shah, R.; Newcomb, D.C. Sex Bias in Asthma Prevalence and Pathogenesis. Front. Immunol. 2018, 9, 2997. [Google Scholar] [CrossRef]
- Rehman, A.; Amin, F.; Sadeeqa, S. Prevalence of Asthma and Its Management: A Review. J. Pak. Med. Assoc. 2018, 68, 1823–1827. [Google Scholar]
- Global Strategy for Asthma Management and Prevention. 2021. Available online: https://ginasthma.org/wp-content/uploads/2021/05/GINA-Main-Report-2021-V2-WMS.pdf (accessed on 11 April 2023).
- Bostantzoglou, C.; Delimpoura, V.; Samitas, K.; Zervas, E.; Kanniess, F.; Gaga, M. Clinical Asthma Phenotypes in the Real World: Opportunities and Challenges. Breathe 2015, 11, 186–193. [Google Scholar] [CrossRef]
- Alahmadi, T.S.; Banjari, M.A.; Alharbi, A.S. The Prevalence of Childhood Asthma in Saudi Arabia. Int. J. Pediatr. Adolesc. Med. 2019, 6, 74–77. [Google Scholar] [CrossRef]
- Kamga, A.; Rochefort-Morel, C.; Le Guen, Y.; Ouksel, H.; Pipet, A.; Leroyer, C. Asthma and Smoking: A Review. Respir. Med. Res. 2022, 82, 100916. [Google Scholar] [CrossRef]
- Holloway, J.W.; Yang, I.A.; Holgate, S.T. Genetics of Allergic Disease. J. Allergy Clin. Immunol. 2010, 125, S81–S94. [Google Scholar] [CrossRef]
- Ranjbar, M.; Whetstone, C.E.; Omer, H.; Power, L.; Cusack, R.P.; Gauvreau, G.M. The Genetic Factors of the Airway Epithelium Associated with the Pathology of Asthma. Genes 2022, 13, 1870. [Google Scholar] [CrossRef]
- Ober, C.; Yao, T.C. The Genetics of Asthma and Allergic Disease: A 21st Century Perspective. Immunol. Rev. 2011, 242, 10–30. [Google Scholar] [CrossRef]
- Mims, J.W. Asthma: Definitions and Pathophysiology. Int. Forum Allergy Rhinol. 2015, 5, S2–S6. [Google Scholar] [CrossRef]
- Castillo, J.R.; Peters, S.P.; Busse, W.W. Asthma Exacerbations: Pathogenesis, Prevention, and Treatment. J. Allergy Clin. Immunol. Pract. 2017, 5, 918–927. [Google Scholar] [CrossRef]
- Alaki, S.M.; Ashiry, E.A.A.; Bakry, N.S.; Baghlaf, K.K.; Bagher, S.M. The Effects of Asthma and Asthma Medication on Dental Caries and Salivary Characteristics in Children. Oral Health Prev. Dent. 2013, 11, 113–120. [Google Scholar] [CrossRef]
- Nunes, C.; Pereira, A.M.; Morais-Almeida, M. Asthma Costs and Social Impact. Asthma Res. Pract. 2017, 3, 1. [Google Scholar] [CrossRef]
- dos Santos, C.C.O.; Bellini-Pereira, S.A.; Medina, M.C.G.; Normando, D. Allergies/Asthma and Root Resorption: A Systematic Review. Prog. Orthod. 2021, 22, 8. [Google Scholar] [CrossRef]
- Wu, F.; Liu, J. Asthma Medication Increases Dental Caries among Children in Taiwan: An Analysis Using the National Health Insurance Research Database. J. Dent. Sci. 2019, 14, 413–418. [Google Scholar] [CrossRef]
- GINA Report, Global Strategy for Asthma Management and Prevention. Available online: https://ginasthma.org/gina-reports/ (accessed on 22 May 2022).
- National Asthma Education and Prevention Program Coordinating Committee (NAEPPCC)|NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/science/national-asthma-education-and-prevention-program-naepp (accessed on 23 May 2022).
- Sin, D.D.; Man, J.; Sharpe, H.; Gan, W.Q.; Man, S.F.P. Pharmacological Management to Reduce Exacerbations in Adults with Asthma: A Systematic Review and Meta-Analysis. J. Am. Med. Assoc. 2004, 292, 367–376. [Google Scholar] [CrossRef]
- Lommatzsch, M.; Virchow, J.C. Severe Asthma. Dtsch. Arztebl. Int. 2014, 111, 847–855. [Google Scholar] [CrossRef]
- Arafa, A.; Aldahlawi, S.; Fathi, A. Assessment of the Oral Health Status of Asthmatic Children. Eur. J. Dent. 2017, 11, 357–363. [Google Scholar] [CrossRef]
- Orellana-Alpala, C.; Pacheco-Quito, E.-M.; Calle-Prado, D.; Cuenca-León, K. Knowledge Level Regarding the Prescription of Antibiotics within the Dentistry Field. Arch. Venez. Farmacol. Ter. 2022, 41, 665–670. [Google Scholar] [CrossRef]
- Velez-León, E.M.; Vargas, K.L.; Cuenca-León, K.; Acurio-Vargas, C.; Zumba, A.; Pacheco-Quito, E.M. Ambulatory Sedation for Dental Procedures-Case of Cuenca, Ecuador. Children 2022, 9, 1618. [Google Scholar] [CrossRef]
- Brigic, A.; Kobaslija, S.; Zukanovic, A. Cariogenic Potential of Inhaled Antiasthmatic Drugs. Med. Arch. 2015, 69, 247–250. [Google Scholar] [CrossRef]
- Brigic, A.; Kobaslija, S.; Zukanovic, A. Antiasthmatic Inhaled Medications as Favoring Factors for Increased Concentration of Streptococcus Mutans. Mater. Socio Med. 2015, 27, 237. [Google Scholar] [CrossRef]
- Botelho, M.P.J.; MacIel, S.M.; Cerci Neto, A.; Dezan, C.C.; Fernandes, K.B.P.; De Andrade, F.B. Cariogenic Microorganisms and Oral Conditions in Asthmatic Children. Caries Res. 2011, 45, 386–392. [Google Scholar] [CrossRef]
- Ersin, N.K.; Gülen, F.; Eronat, N.; Cogulu, D.; Demir, E.; Tanaç, R.; Aydemir, Ş. Oral and Dental Manifestations of Young Asthmatics Related to Medication, Severity and Duration of Condition. Pediatr. Int. 2006, 48, 549–554. [Google Scholar] [CrossRef]
- Stensson, M.; Wendt, L.K.; Koch, G.; Oldaeus, G.; Ramberg, P.; Birkhed, D. Oral Health in Young Adults with Long-Term, Controlled Asthma. Acta Odontol. Scand. 2011, 69, 158–164. [Google Scholar] [CrossRef]
- Doğan, M.; Şahiner, Ü.M.; Ataç, A.S.; Ballıkaya, E.; Soyer, Ö.U.; Şekerel, B.E. Oral Health Status of Asthmatic Children Using Inhaled Corticosteroids. Turk. J. Pediatr. 2021, 63, 77–85. [Google Scholar] [CrossRef]
- Thomas, M.S.; Parolia, A.; Kundabala, M.; Vikram, M. Asthma and Oral Health: A Review. Aust. Dent. J. 2010, 55, 128–133. [Google Scholar] [CrossRef]
- Świątkowska-Bury, M.; Zawadzka-Krajewska, A.; Kulus, M.; Olczak-Kowalczyk, D. The Effect of the Type of Inhaled Anti-Asthmatic Therapy on the Properties of Saliva in Children—A Phantom Study. J. Stomatol. 2021, 74, 22–27. [Google Scholar] [CrossRef]
- Dawes, C.; Wong, D.T.W. Role of Saliva and Salivary Diagnostics in the Advancement of Oral Health. J. Dent. Res. 2019, 98, 133–141. [Google Scholar] [CrossRef]
- Rezende, G.; dos Santos, N.M.L.; Stein, C.; Hilgert, J.B.; Faustino-Silva, D.D. Asthma and Oral Changes in Children: Associated Factors in a Community of Southern Brazil. Int. J. Paediatr. Dent. 2019, 29, 456–463. [Google Scholar] [CrossRef]
- Sivasithamparam, K.; Young, W.G.; Jirattanasopa, V.; Priest, J.; Khan, F.; Harbrow, D.; Daley, T.J. Dental Erosion in Asthma: A Case-Control Study from South East Queensland. Aust. Dent. J. 2002, 47, 298–303. [Google Scholar] [CrossRef]
- Dugmore, C.R.; Rock, W.P. A Multifactorial Analysis of Factors Associated with Dental Erosion. Br. Dent. J. 2004, 196, 283–286. [Google Scholar] [CrossRef]
- Huchon, G.; Magnussen, H.; Chuchalin, A.; Dymek, L.; Gonod, F.B.; Bousquet, J. Lung Function and Asthma Control with Beclomethasone and Formoterol in a Single Inhaler. Respir. Med. 2009, 103, 41–49. [Google Scholar] [CrossRef]
- Boskabady, M.; Nematollahi, H.; Boskabady, M.H. Effect of Inhaled Medication and Inhalation Technique on Dental Caries in Asthmatic Patients. Iran. Red Crescent Med. J. 2012, 14, 816–821. [Google Scholar] [CrossRef]
- Ehsani, S.; Moin, M.; Meighani, G.; Pourhashemi, S.J.; Khayatpisheh, H.; Yarahmadi, N. Oral Health Status in Preschool Asthmatic Children in Iran. Iran J. Allergy Asthma Immunol. 2013, 12, 254–261. [Google Scholar] [PubMed]
- Godara, N.; Khullar, M.; Godara, R.; Singh, V. Evaluation of Cariogenic Potential of Dry Powder Inhalers: A Case-Control Study. Lung India 2013, 30, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Prasanthi, B.; Kannan, N.; Patil, R. Effect of Diuretics on Salivary Flow, Composition and Oral Health Status: A Clinico-Biochemical Study. Ann. Med. Health Sci. Res. 2014, 4, 549. [Google Scholar] [CrossRef]
- Monadi, M.; Javadian, Y.; Cheraghi, M.; Heidari, B.; Amiri, M. Impact of Treatment with Inhaled Corticosteroids on Bone Mineral Density of Patients with Asthma: Related with Age. Osteoporos. Int. 2015, 26, 2013–2018. [Google Scholar] [CrossRef] [PubMed]
- Reddel, H.K.; Busse, W.W.; Pedersen, S.; Tan, W.C.; Chen, Y.Z.; Jorup, C.; Lythgoe, D.; O’Byrne, P.M. Should Recommendations about Starting Inhaled Corticosteroid Treatment for Mild Asthma Be Based on Symptom Frequency: A Post-Hoc Efficacy Analysis of the START Study. Lancet 2017, 389, 157–166. [Google Scholar] [CrossRef]
- Rodríguez, F.; Duran, A.; Muñoz, Z.; Palomera, E.; Serra-Prat, M.; Boixeda, R.; Vicente, V.; Almirall, J. Oral Health and Risk of Pneumonia in Asthmatic Pacients with Inhaled Treatment. Med. Clin. 2018, 150, 455–459. [Google Scholar] [CrossRef]
- Ashuja, R.B.; Nandini, D.B.; Vidyasagar, B.; Ashwini, R.; Donoghue, M.; Madhushankari, G.S. Oral Carriage of Cariogenic Bacteria and Candida Albicans in Asthmatic Adults before and after Anti-Asthma Medication: A Longitudinal Study. J. Oral Maxillofac. Pathol. 2018, 22, 144–145. [Google Scholar] [CrossRef]
- Hu, L.; He, C.; Zhao, C.; Chen, X.; Hua, H.; Yan, Z. Characterization of Oral Candidiasis and the Candida Species Profile in Patients with Oral Mucosal Diseases. Microb. Pathog. 2019, 134, 103575. [Google Scholar] [CrossRef]
- Hassanpour, K.; Tehrani, H.; Goudarzian, M.; Beihaghi, S.; Ebrahimi, M.; Amiri, P. Comparison of the Frequency of Dental Caries in Asthmatic Children under Treatment with Inhaled Corticosteroids and Healthy Children in Sabzevar in 2017–2018. Electron. J. Gen. Med. 2019, 16, em119. [Google Scholar] [CrossRef]
- Khassawneh, B.; Alhabashneh, R.; Ibrahim, F. The Association between Bronchial Asthma and Periodontitis: A Case-Control Study in Jordan. J. Asthma. 2019, 56, 404–410. [Google Scholar] [CrossRef]
- Chumpitaz-Cerrate, V.; A Bellido-Meza, J.; Chávez-Rimache, L.; Rodríguez-Vargas, C. Impact of Inhaler Use on Dental Caries in Asthma Pediatrics Patients: A Case-Control Study. Arch. Argent. Pediatr. 2020, 118, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Bairappan, S.; Puranik, M.P.; Sowmya, K.R. Impact of Asthma and Its Medication on Salivary Characteristics and Oral Health in Adolescents: A Cross-Sectional Comparative Study. Spec. Care Dent. 2020, 40, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Brasil-Oliveira, R.; Cruz, Á.A.; Souza-Machado, A.; Pinheiro, G.P.; Inácio, D.D.S.; Sarmento, V.A.; Lins-Kusterer, L. Oral Health-Related Quality of Life in Individuals with Severe Asthma. J. Bras. Pneumol. 2021, 47, e20200117. [Google Scholar] [CrossRef] [PubMed]
- Akiki, Z.; Saadeh, D.; Farah, R.; Hallit, S.; Sacre, H.; Hosseini, H.; Salameh, P. Asthma Prevalence and Associated Factors among Lebanese Adults: The First National Survey. BMC Pulm. Med. 2021, 21, 162. [Google Scholar] [CrossRef] [PubMed]
- Slob, E.M.A.; Richards, L.B.; Vijverberg, S.J.H.; Longo, C.; Koppelman, G.H.; Pijnenburg, M.W.H.; Bel, E.H.D.; Neerincx, A.H.; Herrera Luis, E.; Perez-Garcia, J.; et al. Genome-Wide Association Studies of Exacerbations in Children Using Long-Acting Beta2-Agonists. Pediatr. Allergy Immunol. 2021, 32, 1197–1207. [Google Scholar] [CrossRef]
- Abidullah, M.; Sanober, A.; Kumar, S.; Gaddikeri, K.; Soorneedi, N.; Fatema, R.; Ahmed, S.M. Salivary Candida Albicans in Asthmatic Patients Taking Anti-Asthmatic Medication. J. Med. Life 2022, 15, 1110. [Google Scholar] [CrossRef]
- Postma, D.S.; Kerstjens, H.A.M.; Ten Hacken, N.H.T. Inhaled Corticosteroids and Long-Acting Beta-Agonists in Adult Asthma: A Winning Combination in All? Naunyn Schmiedebergs Arch. Pharmacol. 2008, 378, 203215, Erratum in Naunyn Schmiedebergs Arch. Pharmacol. 2009, 380, 97. [Google Scholar] [CrossRef]
- Jeminiwa, R.; Hohmann, L.; Qian, J.; Garza, K.; Hansen, R.; Fox, B.I. Impact of EHealth on Medication Adherence among Patients with Asthma: A Systematic Review and Meta-Analysis. Respir. Med. 2019, 149, 59–68. [Google Scholar] [CrossRef]
- Adams, N.P.; Jones, P.W. The Dose-Response Characteristics of Inhaled Corticosteroids When Used to Treat Asthma: An Overview of Cochrane Systematic Reviews. Respir. Med. 2006, 100, 1297–1306. [Google Scholar] [CrossRef]
- Pandya, D.; Puttanna, A.; Balagopal, V. Systemic Effects of Inhaled Corticosteroids: An Overview. Open Respir. Med. J. 2015, 8, 59–65. [Google Scholar] [CrossRef]
- Reddel, H.K.; Taylor, D.R.; Bateman, E.D.; Boulet, L.P.; Boushey, H.A.; Busse, W.W.; Casale, T.B.; Chanez, P.; Enright, P.L.; Gibson, P.G.; et al. An Official American Thoracic Society/European Respiratory Society Statement: Asthma Control and Exacerbations—Standardizing Endpoints for Clinical Asthma Trials and Clinical Practice. Am. J. Respir. Crit. Care Med. 2009, 180, 59–99. [Google Scholar] [CrossRef] [PubMed]
- Laube, B.L.; Janssens, H.M.; De Jongh, F.H.C.; Devadason, S.G.; Dhand, R.; Diot, P.; Everard, M.L.; Horvath, I.; Navalesi, P.; Voshaar, T.; et al. What the Pulmonary Specialist Should Know about the New Inhalation Therapies. Eur. Respir. J. 2011, 37, 1308–1331. [Google Scholar] [CrossRef] [PubMed]
- Muchão, F.P.; Da Silva Filho, L.V.R.F. Advances in Inhalation Therapy in Pediatrics. J. Pediatr. 2010, 86, 367–376. [Google Scholar] [CrossRef]
- Cheng, Y.S. Mechanisms of Pharmaceutical Aerosol Deposition in the Respiratory Tract. AAPS PharmSciTech 2014, 15, 630–640. [Google Scholar] [CrossRef] [PubMed]
- Dal Negro, R.W. Dry Powder Inhalers and the Right Things to Remember: A Concept Review. Multidiscip. Respir. Med. 2015, 10, 13. [Google Scholar] [CrossRef]
- Haughney, J.; Price, D.; Barnes, N.C.; Virchow, J.C.; Roche, N.; Chrystyn, H. Choosing Inhaler Devices for People with Asthma: Current Knowledge and Outstanding Research Needs. Respir. Med. 2010, 104, 1237–1245. [Google Scholar] [CrossRef]
- Choi, H.; Bae, K.H.; Lee, J.W. Association between Age at Asthma Diagnosis and Tooth Loss. Acta Odontol. Scand. 2018, 76, 466–472. [Google Scholar] [CrossRef]
- Patel, S.J.; Teach, S.J. Asthma. Pediatr. Rev. 2019, 40, 549–565. [Google Scholar] [CrossRef]
- Zahran, H.S.; Bailey, C.M.; Qin, X.; Johnson, C. Long-Term Control Medication Use and Asthma Control Status among Children and Adults with Asthma. J. Asthma 2017, 54, 1065–1072. [Google Scholar] [CrossRef]
- Elyassi Gorji, N.; Nasiri, P.; Malekzadeh Shafaroudi, A.; Moosazadeh, M. Comparison of Dental Caries (DMFT and DMFS Indices) between Asthmatic Patients and Control Group in Iran: A Meta-Analysis. Asthma Res. Pract. 2021, 7, 2. [Google Scholar] [CrossRef]
- Alshammari, F.R.; Alamri, H.; Aljohani, M.; Sabbah, W.; O’Malley, L.; Glenny, A.M. Dental Caries in Saudi Arabia: A Systematic Review. J. Taibah. Univ. Med. Sci. 2021, 16, 643–656. [Google Scholar] [CrossRef] [PubMed]
- Vélez-León, E.M.; Albaladejo-Martínez, A.; Cuenca-León, K.; Encalada-Verdugo, L.; Armas-Vega, A.; Melo, M. Caries Experience and Treatment Needs in Urban and Rural Environments in School-Age Children from Three Provinces of Ecuador: A Cross-Sectional Study. Dent. J. 2022, 10, 185. [Google Scholar] [CrossRef] [PubMed]
- Vélez-León, E.; Albaladejo, A.; Cuenca-León, K.; Jiménez-Romero, M.; Armas-Vega, A.; Melo, M. Prevalence of Caries According to the ICDAS II in Children from 6 and 12 Years of Age from Southern Ecuadorian Regions. Int. J. Environ. Res. Public Health 2022, 19, 7266. [Google Scholar] [CrossRef]
- Stensson, M.; Wendt, L.K.; Koch, G.; Oldaeus, G.; Lingström, P.; Birkhed, D. Caries Prevalence, Caries-Related Factors and Plaque PH in Adolescents with Long-Term Asthma. Caries Res. 2011, 44, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Vélez-León, E.; Albaladejo-Martínez, A.; Pacheco-Quito, E.-M.; Armas-Vega, A.; Delgado-Gaete, A.; Pesántez-Ochoa, D.; Melo, M. Developmental Enamel Defects in Children from the Southern Region of Ecuador. Children 2022, 9, 1755. [Google Scholar] [CrossRef] [PubMed]
- Bozejac, B.V.; Stojšin, I.; Đurić, M.; Zvezdin, B.; Brkanić, T.; Budišin, E.; Vukoje, K.; Sečen, N. Impact of Inhalation Therapy on the Incidence of Carious Lesions in Patients with Asthma and COPD. J. Appl. Oral Sci. 2017, 25, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Hatipoğlu, Ö.; Pertek Hatipoğlu, F. Association between Asthma and Caries-Related Salivary Factors: A Meta-Analysis. J. Asthma 2022, 59, 38–53. [Google Scholar] [CrossRef]
- Cherkasov, S.V.; Popova, L.Y.; Vivtanenko, T.V.; Demina, R.R.; Khlopko, Y.A.; Balkin, A.S.; Plotnikov, A.O. Oral Microbiomes in Children with Asthma and Dental Caries. Oral Dis. 2019, 25, 898–910. [Google Scholar] [CrossRef]
- Azarpazhooh, A.; Leake, J.L. Systematic Review of the Association Between Respiratory Diseases and Oral Health. J. Periodontol. 2006, 77, 1465–1482. [Google Scholar] [CrossRef]
- Maupomé, G.; Shulman, J.D.; Medina-Soils, C.E.; Ladeinde, O. Is There a Relationship between Asthma and Dental Caries?: A Critical Review of the Literature. J. Am. Dent. Assoc. 2010, 141, 1061–1074. [Google Scholar] [CrossRef]
- Shah, P.D.; Badner, V.M.; Rastogi, D.; Moss, K.L. Association between Asthma and Dental Caries in US (United States) Adult Population. J. Asthma 2021, 58, 1329–1336. [Google Scholar] [CrossRef] [PubMed]
- Shashikiran, N.D.; Reddy, V.V.S.; Krishnam Raju, P. Effect of Antiasthmatic Medication on Dental Disease: Dental Caries and Periodontal Disease. J. Indian Soc. Pedod. Prev. Dent. 2007, 25, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Steinbacher, D.M.; Glick, M. The Dental Patient with Asthma: An Update and Oral Health Considerations. J. Am. Dent. Assoc. 2001, 132, 1229–1239. [Google Scholar] [CrossRef] [PubMed]
- Al-Haddad, K.A.; Al-dossary, O.A.E.; Al-Shamahy, H.A. Prevalence and Associated Factors of Oral Non-Candida Albicans Candida Carriage in Denture Wearers in Sana’a City—Yemen. Univers. J. Pharm. Res. 2018, 3, 69–73. [Google Scholar] [CrossRef]
- Pour, A.H.; Salari, S.; Nejad Almani, P.G. Oropharyngeal Candidiasis in HIV/AIDS Patients and Non-HIV Subjects in the Southeast of Iran. Curr. Med. Mycol. 2018, 4, 1–6. [Google Scholar] [CrossRef]
- GÜMRÜ, B.; AKKİTAP, M.P. Oral Candidiasis as a Local Adverse Effect of Inhaled Corticosteroids: What the Dental Practitioner Should Know. Black Sea J. Health Sci. 2021, 5, 107–115. [Google Scholar] [CrossRef]
- Vila, T.; Sultan, A.S.; Montelongo-Jauregui, D.; Jabra-Rizk, M.A. Oral Candidiasis: A Disease of Opportunity. J. Fungi 2020, 6, 15. [Google Scholar] [CrossRef]
- Sharma, S.; Gaur, P.; Gupta, S.; Kant, S. Impact of Asthma on Oral Health: A Review. Int. J. Recent. Sci. Res. 2018, 9, 26512–26514. [Google Scholar]
- Lemmetyinen, R.; Karjalainen, J.; But, A.; Renkonen, R.; Pekkanen, J.; Haukka, J.; Toppila-Salmi, S. Diseases with Oral Manifestations among Adult Asthmatics in Finland: A Population-Based Matched Cohort Study. BMJ Open 2021, 11, e053133. [Google Scholar] [CrossRef]
- Cuenca-León, K.; Pacheco-Quito, E.M.; Granda-Granda, Y.; Vélez-León, E.; Zarzuelo-Castañeda, A. Phytotherapy: A Solution to Decrease Antifungal Resistance in the Dental Field. Biomolecules 2022, 12, 789. [Google Scholar] [CrossRef]
- Ferreira, M.K.M.; Ferreira, R.d.O.; Castro, M.M.L.; Magno, M.B.; Almeida, A.P.C.P.S.C.; Fagundes, N.C.F.; Maia, L.C.; Lima, R.R. Is There an Association between Asthma and Periodontal Disease among Adults? Systematic Review and Meta-Analysis. Life Sci. 2019, 223, 74–87. [Google Scholar] [CrossRef] [PubMed]
- Gomes-Filho, I.S.; da Cruz, S.S.; Trindade, S.C.; Passos-Soares, J.d.S.; Carvalho-Filho, P.C.; Figueiredo, A.C.M.G.; Lyrio, A.O.; Hintz, A.M.; Pereira, M.G.; Scannapieco, F. Periodontitis and Respiratory Diseases: A Systematic Review with Meta-Analysis. Oral Dis. 2020, 26, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Yaghobee, S.; Paknejad, M.; Khorsand, A. Association between Asthma and Periodontal Disease. Front. Dent. (J. Dent. Tehran Univ. Med. Sci.) 2018, 5, 47–51. [Google Scholar]
- Moraschini, V.; de Albuquerque Calasans-Maia, J.; Calasans-Maia, M.D. Association Between Asthma and Periodontal Disease: A Systematic Review and Meta-Analysis. J. Periodontol. 2017, 89, 440–455. [Google Scholar] [CrossRef]
- Rivera, R.; Andriankaja, O.M.; Perez, C.M.; Joshipura, K. Relationship between Periodontal Disease and Asthma among Overweight/Obese Adults. J. Clin. Periodontol. 2016, 43, 566–571. [Google Scholar] [CrossRef]
- Gomes-Filho, I.S.; Soledade-Marques, K.R.; Seixas da Cruz, S.; de Santana Passos-Soares, J.; Trindade, S.C.; Souza-Machado, A.; Fischer Rubira-Bullen, I.R.; de Moraes Marcílio Cerqueira, E.; Barreto, M.L.; Costa de Santana, T.; et al. Does Periodontal Infection Have an Effect on Severe Asthma in Adults? J. Periodontol. 2014, 85, e179–e187. [Google Scholar] [CrossRef] [PubMed]
- Candeo, L.C.; Rigonato-Oliveira, N.C.; Brito, A.A.; Marcos, R.L.; França, C.M.; Fernandes, K.P.S.; Mesquita-Ferrari, R.A.; Bussadori, S.K.; Vieira, R.P.; Lino-Dos-Santos-Franco, A.; et al. Effects of Periodontitis on the Development of Asthma: The Role of Photodynamic Therapy. PLoS ONE 2017, 12, e0187945. [Google Scholar] [CrossRef] [PubMed]
- Shen, T.-C.; Chang, P.-Y.; Lin, C.-L.; Wei, C.-C.; Tu, C.-Y.; Hsia, T.-C.; Shih, C.-M.; Hsu, W.-H.; Sung, F.-C.; Kao, C.-H. Risk of Periodontal Disease in Patients with Asthma: A Nationwide Population-Based Retrospective Cohort Study. J. Periodontol. 2017, 88, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Mappangara, S.; Basir, I.; Oktawati, S.; Adam, M.; Achmad, H. Periodontal Disease Associated with Corticosteroid in Asthma Patients-A Systematic Review. Int. J. Appl. Pharm. 2019, 11, 68–70. [Google Scholar] [CrossRef]
- Taji, S.; Seow, W.K. A Literature Review of Dental Erosion in Children. Aust. Dent. J. 2010, 55, 358–367. [Google Scholar] [CrossRef]
- Manuel, S.T.; Kundabaka, M.; Shetty, N.; Parolia, A. Asthma and Dental Erosion. Kathmandu Univ. Med. J. 2008, 6, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; Pandit, I.K.; Srivastava, N.; Gugnani, N. Dental Erosion in Children. J. Oral Health Comm. Dent. 2009, 3, 56–61. [Google Scholar]
- Lussi, A.; Jaeggi, T. Dental Erosion in Children. Monogr. Oral Sci. 2006, 20, 140–151. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Type of Study | Author/Year | Objetives | Drugs | Study Design | Main Findings | References |
|---|---|---|---|---|---|---|
| Case—control | Sivasithamparam et al./2002 | To determine the incidence of dental erosion in asthmatic and non-asthmatic patients. | Salbutamol | Subjects were examined by recording tooth wear patterns. | There was a higher incidence of dental hypersensitivity, xerostomia, salivary gland abnormalities, gastric discomfort, and self-induced vomiting in asthmatic patients compared to the control group. | [40] |
| Retrospective study | Dugmore et al./2004 | To analyze the relationship of possible etiological factors for the presence of dental erosion. | Terbuline Salbutamol | The erosion index used was based on the 1993 Children’s Dental Health Survey. | At 12 years, significant positive associations were found between the experience of erosion and decay (odds ratio [OR] = 1.48), drinking fruit juice (OR = 1.42) or soft drinks (OR = 1.59–2.52, depending on quantity and frequency). | [41] |
| Case—control | Ersin et al./2006 | To investigate the dental caries risk of asthmatics in relation to dental plaque indices, salivary flow rate, pH and buffering capacity, saliva composition, and salivary levels of Streptococcus mutans compared to healthy subjects. | Inhaled corticosteroids B2 agonists Leukotrienes | The World Health Organization criteria were used for dental examinations and the Silness and Löe plaque index was used for plaque indices. | Children in the asthmatic group aged 6 to 10 years had a significantly higher prevalence of dental caries compared to the control group of the same age. | [33] |
| Randomized clinical trial | Huchon et al./2009 | To evaluate lung function and asthma control with beclomethasone and formoterol in a single inhaler. | Beclamoentasone/formoterol inhaled | Patients received extrafine fixed combination treatment of beclomethasone dipropionate 200 mg/formoterol 12 mg twice daily, or beclomethasone dipropionate and formoterol. | The combination of beclomethasone dipropionate/formoterol through a single inhaler or through separate inhalers improved morning lung function. | [42] |
| Case—control | Botello et al./2011 | To evaluate the dental caries risk of asthmatic patients based on the levels of Streptococcus mutans and lactobacillus in saliva samples, as well as the index of oral hygiene and dental caries. | Beclomethasone Budesonide Ciclesonide Fluticasone propionate Mometasone furoate | Parents were interviewed about factors related to oral health. WHO criteria for dental examinations were used. | No differences were observed between the asthma and control groups for the prevalence of dental caries in children aged 3 to 6 years and 7 to 10 years, except for severe cases in the younger group. | [32] |
| Cross-sectional study | Stensson et al./2011 | To study oral health in young adults with long-term controlled asthma. | Salmeterol/Fluctisona Formoterol/budenoside | A clinical examination was performed to determine the prevalences of dental caries, erosions, gingival inflammation, cervicular fluid, and presence of periodontal pockets and the rate of plaque formation. | The asthmatic participant group had more gingivitis (p = 0.01) and a lower stimulated salivary secretion rate than the controls (p = 0.01). Asthmatics also had a somewhat lower initial pH value, although not statistically significant. | [34] |
| Case—control | Boskabady et al./2012 | To examine the relationship between type of inhaled medication, duration of use, dosage, technique of inhaler use, and severity and duration of disease on dental caries in asthmatic patients. | Corticosteroids β2-adrenergic receptor agonists | In asthmatic patients, the type, dose, duration of medication, technique of inhaler use, and severity and duration of the disease were recorded. Dental health status, including DMFT index, was examined. In addition, pulmonary function tests (PFTs) were performed for both groups. | All dental cavity rates in the asthmatic group were higher than those of the controls. There was no significant correlation between dental cavity rates and disease duration, PFT values; medication dose or inhaler use technique. | [43] |
| Case—control | Ehsani et al./2013 | To investigate oral health indices in healthy children and children with mild to moderate asthma. | Salbutamol Inhaled corticosteroids Fluctisone Beclomentasone Systemic corticosteroids Antihistamines Theophylline | Dental plaque, gingival inflammation, mouth breathing and dental caries were assessed by a trained examiner according to the World Health Organization criteria. | The results indicated no significant differences between the children with asthma and those without asthma regarding (decayed, missing, filled, teeth) dmft index (mean of 3.34 in asthmatic children and 3.0 in the control group). | [44] |
| Case—control | Godara et al./2013 | To examine the potential link between dental caries and the specific use of dust inhalers in patients with bronchial asthma. | B2 agonists Inhaled corticosteroids | A clinical examination performed, which included the DMFT index to assess the presence of dental caries. | Asthmatic subjects exhibited a higher incidence of dental caries compared to the control group, but the difference was not statistically significant. | [45] |
| Case—control | Alaki et al./2013 | To investigate the prevalence and severity of dental caries in children with a history of asthma. | Inhaled corticosteroids β2-agonist inhalers Anti-asthma 2 agonist inhalers and antihistamines combined with corticosteroids | Interviews and questionnaires were completed by the parents of the children involved and dental examinations were performed. Stimulated salivary samples were collected to determine salivary flow rate, buffering capacity, and salivary levels of Streptoccocus mutans and Lactobacillus. | No significant differences were found in the DMFT index or community periodontal index scores between cases and controls. | [19] |
| Case—control | Prasanthi et al./2014 | Evaluation of the effect of diuretics on oral health status with respect to pH, buffering, total protein content, various ion concentrations, and oral mucosal lesions. | Agonists of β2-adrenergic receptors. | Unstimulated and stimulated saliva was collected for further evaluation. Dental caries and periodontal status were measured using the DMFT index and Russell’s periodontal index, respectively. | Prevalence was found for dental caries (p < 0.01), periodontal status (p < 0.001), and mucosal lesions (p < 0.01). | [46] |
| Case—control | Monadi et al./2015 | To investigate the effect of inhaled corticosteroids on bone mineral density. | Inhaled corticosteroids | Bone mineral density in the lumbar spine (LS) and femoral neck (FN) was measured by dual energy X-ray absorptiometry (DEXA). | Compared to controls, bone mineral density decreased only in patients < 50 years in both spine (11.3%, p = 0.013) and hip (8.8%, p = 0.044), while in patients ≥ 50 years, BMD did not decrease significantly. | [47] |
| Retrospective-prospective study | Brigic et al./2015 | Cariogenic potential of inhaled anti-asthmatics | Inhaled anti-asthmatics | 200 patients, aged 7 to 14 years, divided into two groups: the control group (n1 = 100) was made up of healthy children and the experimental group was made up of children suffering from asthma (n2 = 100). In both groups of respondents, the following were found inthe DMFT index: the plaque index value and the hygienic-dietary habits by means of the questionnaire. | The subjects in the control group had a significantly higher DMFT index than the subjects in the experimental group (p = 0.004). It is determined that there are no significant differences in plaque index values (p > 0.05). | [31] |
| Retrospective-prospective study | Brigic et al./2015 | Asthma/dental caries | Inhaled anti-asthmatics | The study sample consisted of 200 patients, aged from 7–14 years, divided into two groups: the control group (n1 = 100) consisted of healthy children and the experimental group consisted of children suffering from asthma (n2 = 100). In both groups of respondents, the following were determined in the DMFT index: plaque index value and hygienic-dietary habits using the questionnaire. | The results of this research have once again confirmed that the dental caries is a disease with multifactorial etiology in which mutual relationships and interactions between numerous etiological factors contribute even more to the complexity to estimate the of cavity risk problem. | [30] |
| Randomized clinical trial | Reddel et al./2017 | To analyze the benefits of initiation of inhaled corticosteroid therapy for mild asthma on symptom frequency. | Inhaled corticosteroids | Study of treatment with inhaled steroids as regular therapy (START) of 3 years, conducted in 32 countries, with clinical visits every 3 months. | Of 7138 patients (n = 3577 budesonide; n = 3561 placebo), the initial frequency of symptoms was 0 to 1 days per week for 2184 (31%) participants, more than 1 and less than or equal to 2 days of symptoms per week for 1914 (27%) participants, and more than 2 days with symptoms per week for 3040 (43%) participants. | [48] |
| Case—control | Arafa et al./2017 | To evaluate oral health status and salivary composition in a group of children with bronchial asthma. | Inhaled corticosteroids β2-agonist inhalers | The children were clinically examined to assess their dental cavity experience, dental erosion status, and gingival status. | The results of this study revealed that asthmatic children presented a significantly higher mean DMFT index, dental erosion status, and gingival status compared to the control groups. | [27] |
| Case—control | Rodríguez et al./2018 | To determine whether oral health is a risk factor for community-acquired pneumonia in asthmatic patients undergoing inhaled therapy. | Inhaled anti-asthmatics | The main study factor was the general oral health assessment index (GOHAI) score. | Bivariate analysis shows a statistically significant association of community-acquired pneumonia with a GOHAI ≤ 57 points (poor oral health) (OR 1.69). | [49] |
| Case—control | Ashuja et al./2018 | To evaluate and compare Streptococcus mutans (SM) and plaque lactobacilli and C. albicans counts in saliva samples from asthmatic adults with controls during the course of medication longitudinally. | Budesonide Methylprednisolone Formoterol | Samples were collected from twenty newly diagnosed asthmatic adults and twenty controls for estimation of microbial counts at baseline and at three and six months after initiation of medication. | Asthmatics at baseline had higher microbial counts than controls, but the difference was not statistically significant. | [50] |
| Cohort | Wu et al./2019 | Asthma/caries | Inhaled corticosteroids Bronchodilator agents: short or long-acting b2 agonists | Investigating the correlation between asthma medications and dental caries among children in Taiwan. | The prevalence of caries in children without asthma was 85.2% and that of children with asthma was 90.0%, children who received asthma medication have a higher prevalence of dental caries and a higher rate of severe caries than children without asthma. | [22] |
| Cross-sectional study | Rezende et al./2019 | To evaluate caries, erosion, and enamel defects in children with and without asthma. | Salbutamol | The assessment consisted of an oral examination and a structured interview with the children’s parents/guardians. | Of 112 asthmatic children, 63 (51.2%) had dental caries and 25 (53.2%) had enamel defects. In the adjusted analysis, dental caries and salbutamol use were associated (PR = 1.32, 95% CI = 1.01–1.72). | [39] |
| Retrospective study | Hu et al./2019 | To assess the characterization of oral candidiasis and the species profiles in such patients. | Corticosteroids, vasoconstrictors, and antihistamines | Over a period of four consecutive years, patients with oral mucosal diseases were screened for oral candidiasis through a combination of clinical presentation and laboratory findings. | In total, 9769 (6.09%) of the 160,357 patients examined were diagnosed as having oral candidiasis on the basis of both clinical manifestations and laboratory tests. | [51] |
| Case—control | Hassanpour et al./2019 | To determine and compare the frequency of dental caries among asthmatic children, with asthmatic children who inhaled corticosteroid treatment and healthy children. | Inhaled corticosteroids | An examination for the diagnosis of dental caries was performed using the DMF index. | The mean DMF index score in each of the subscales of decayed teeth (D/d), missing teeth (P/p), and filled teeth (O/o), was higher in asthmatic children compared to healthy children (p < 0.05). | [52] |
| Case—control | Khassawneh et al./2019 | To study the association between bronchial asthma (BA) and periodontitis. | Oral corticosteroids and inhaled corticosteroids | AB cases were diagnosed by a physician and subjects had been prescribed anti-asthma medications for ≥12 months. Periodontitis was defined as the presence of ≥4 teeth with ≥1 site with probing depth (PPD) ≥ 4 mm and clinical attachment level (CAL) ≥ 3 mm. | Periodontitis was present in 52 (40.0%) patients with AB and 26 (20.0%) in the control group, p < 0.005. | [53] |
| Case—control | Chumpitaz-Cerrate, et al./2020 | To determine the prevalence of dental caries in pediatric asthmatic patients using inhaled drugs. | Budesonide/salbutamol or fluticasone/salmeterol | A medical examination was performed to determine the type, timing, and frequency of treatment and an oral examination to establish the prevalence of dental caries and the decayed, missing, and filled tooth DMFT index. | The prevalence of dental caries was 34.2% in the control group and 28.3% in the case group (p = 0.094). In relation to the rate of dental caries, the DMFT index in the control group was 4.73 ± 0.32 and in the case group 3.98 ± 0.31 (p = 0.08). | [54] |
| Cross-sectional comparative study | Bairappan et al./2020 | To assess and compare the salivary characteristics and oral health, and to evaluate the impact of asthma and its medication on dental caries among adolescents with and without asthma. | Short-acting beta-agonists, systemic corticosteroids, and anticholinergic drugs | Study was conducted among 50 asthmatic and 50 nonasthmatic adolescents aged 12–15 years. Salivary samples were collected to determine the flow rate, pH, buffering capacity, and Streptococcus mutans and Lactobacilli counts. Oral health assessment was performed using WHO 2013 proforma. | Asthmatic participants had a significantly higher mean number of teeth with dental caries, gingival bleeding, and dental erosion than nonasthmatics (p < 0.05). The prevalence of fluorosis, traumatic dental injuries, and oral mucosal lesions in asthmatics were 34.0%, 38.0%, and 28.0%, respectively. Statistically significant difference was found in the flow rate, pH, buffering capacity, S. mutans and Lactobacilli counts, and decayed, missing, filled teeth (DMFT) index between asthmatic and nonasthmatic participants. | [55] |
| Cross-sectional study | Brasil-Oliveira et al./2021 | To assess oral health-related quality of life (OHRQoL) among individuals with severe asthma, comparing it with that observed among persons with mild to moderate asthma and persons without asthma. | Inhaled corticosteroids | The index of decayed, missing, and filled teeth (DMFT index) was calculated, as well as the periodontal screening and recording index, and salivary flow was determined. | Periodontitis and reduced salivary flow were more common in patients with severe asthma compared to the group of participants with mild to moderate asthma and no asthma. | [56] |
| Cross-sectional study | Akiki et al./2021 | To assess the prevalence of physician-diagnosed asthma and current asthma, and its determinants. | Inhaled corticosteroids, and antihistamines | The questionnaire used collected information on asthma, respiratory symptoms, and risk factors. | The prevalence of physician-diagnosed asthma was 6.7% (95% CI 5–8.7%) and that of current asthma was 5% (95% CI 3.6–6.9%). | [57] |
| Meta analysis | Slob, et al./2021 | To evaluate whether genetic variations were associated with exacerbations in children treated with beta2-agonists from a global consortium. | Long-acting beta2-agonist | To analyze the genome-wide association performed in 1425 children and young adults with asthma (age 6–21 years) withregular use of beta2-agonists. | Genome-wide association results were analyzed for a total of 82,996 common single nucleotide polymorphisms (SNPs, MAF ≥ 1%) with high imputation quality. Eight independent variants were suggestively (p-value threshold ≤ 5 × 10–6) associated with exacerbations despite beta2-agonist use. | [58] |
| Prospective study | Abidullah et al./2022 | This study aimed to estimate salivary Candida Albicans in asthmatic patients taking anti-asthmatics medication. | Anti-asthmatic medicine in doses of 100, 250, or 500 mg | The research comprised a total of 100 individuals, 50 of whom were asthmatics, and 50 healthy controls who were age and sex-matched to the asthmatics. | 32 people had candida growth and 18 individuals did not have any candidal development at all. Eighteen people were in the 400 CFU/mL group, and 32 individuals were in the 401 CFU/mL group, respectively. It was 0.000 in the 400 colony forming unit/milliliter group, and 27,200 in the 401 CFU/mL group, with 0.00 being the median. There was a notable difference between study and control groups in terms of colony forming unit per milliliter (p = 0.000). | [59] |
| Group | Type of Medication | Drugs | Mechanisms of Action | Indications | Adverse Effects | Reference |
|---|---|---|---|---|---|---|
| β2 Beta-adress beta agonists inhalation bronchodilators | Short-acting β2-adrenergic agonists (SABA) | Terbutaline Fenoterol Salbutamol Albuterol | Relaxes smooth muscles, activates b2 adrenergic receptors in the lungs, bronchodilation. Duration of 2 to 3 min after administration. | Indicated for the rapid relief and prevention of bronchospasms caused by physical exercise. | Oropharyngeal deposition by pharmaceutical inhalers: 60–70%. Decreased buffering capacity of saliva. Increased cariogenic bacterial load in children. Dental erosion, candidiasis, gingivitis. Acid oral pH favoring the production of cariogenic bacteria. Alteration of salivary composition. Susceptibility to dental caries. | [43,45,67,68,71,72,73] |
| Long-acting β2-adrenergic agonists (LABAs) | Indacaterol, Salmeterol, Formoterol Olodaterol Vilanterol Arfomoterol | Duration about 12 h. | ||||
| Anticholinergics | Bronchodilators | Ipratropium Bromide | Antimuscarinic agent, decrease in smooth muscle contractility resulting in bronchodilatation. | Moderate to severe exacerbations (emergencies). Transient pupil dilation and blurred vision. | Dry mouth, intestinal constipation, blurred vision, aggravation of glaucoma. | |
| Corticosteroids | Intermediate and long duration | Prednisone Dexamentasone Blecomethasone Methylprednisolone | Anti-inflammatory; reverses B2 receptor down-regulation. | Reduces inflammatory symptoms indicated for the treatment of moderate to severe exacerbations. | Oropharyngeal deposition by pharmaceutical inhalers: 60–70%. Decreased buffering capacity of saliva. Increased cariogenic bacterial load in children. Dental erosion, candidiasis, gingivitis. Acid oral pH favoring the production of cariogenic bacteria. Alteration of salivary composition. Susceptibility to dental caries. | |
| Inhaled | Ciclesonide Fluticasone Fluorosone propionate Fluticasone propionate Mumetasone fluorosideBudesonide | They inhibit migration, activation of inflammatory cells and secretion of proinflammatory substances. | ||||
| Antihistamines, Anti H1 Antihistamines, H1 Receptor Antagonists | Ketotifen Diphenhydramine | They stabilize membranes and block the release of mediators, reducing epithelial damage. | Restricted corticosteroid use, moderate exacerbations in children. | Central nervous system depression or paradoxical CNS stimulation, dry mouth, dizziness and convulsions. | ||
| Chromoglycate | Sodium chromoglycate | Reduction of bronchial hyperresponsiveness, anti-inflammation. | Preventive treatment, exercise-induced bronchospasm. | Mild pharyngeal irritation, transient cough and bronchospasm may occur. | ||
| Teofilina | Theophylline | Bronchodilator for systemic use, relaxing the smooth muscles of the bronchial tree and pulmonary vessels. | Preventing and treating wheezing, shortness of breath, and chest tightness. | Symptoms and signs of central nervous system and cardiovascular system stimulation, at high doses. Nausea, gastroesophageal reflux, vomiting, headache, insomnia, nervousness, tachycardia, tremor, in rare doses. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pacheco-Quito, E.-M.; Jaramillo, J.; Sarmiento-Ordoñez, J.; Cuenca-León, K. Drugs Prescribed for Asthma and Their Adverse Effects on Dental Health. Dent. J. 2023, 11, 113. https://doi.org/10.3390/dj11050113
Pacheco-Quito E-M, Jaramillo J, Sarmiento-Ordoñez J, Cuenca-León K. Drugs Prescribed for Asthma and Their Adverse Effects on Dental Health. Dentistry Journal. 2023; 11(5):113. https://doi.org/10.3390/dj11050113
Chicago/Turabian StylePacheco-Quito, Edisson-Mauricio, Jessica Jaramillo, Jéssica Sarmiento-Ordoñez, and Katherine Cuenca-León. 2023. "Drugs Prescribed for Asthma and Their Adverse Effects on Dental Health" Dentistry Journal 11, no. 5: 113. https://doi.org/10.3390/dj11050113
APA StylePacheco-Quito, E.-M., Jaramillo, J., Sarmiento-Ordoñez, J., & Cuenca-León, K. (2023). Drugs Prescribed for Asthma and Their Adverse Effects on Dental Health. Dentistry Journal, 11(5), 113. https://doi.org/10.3390/dj11050113