

Fracture Resistance of Repaired 5Y-PSZ Zirconia Crowns after Endodontic Access

 , and
, and 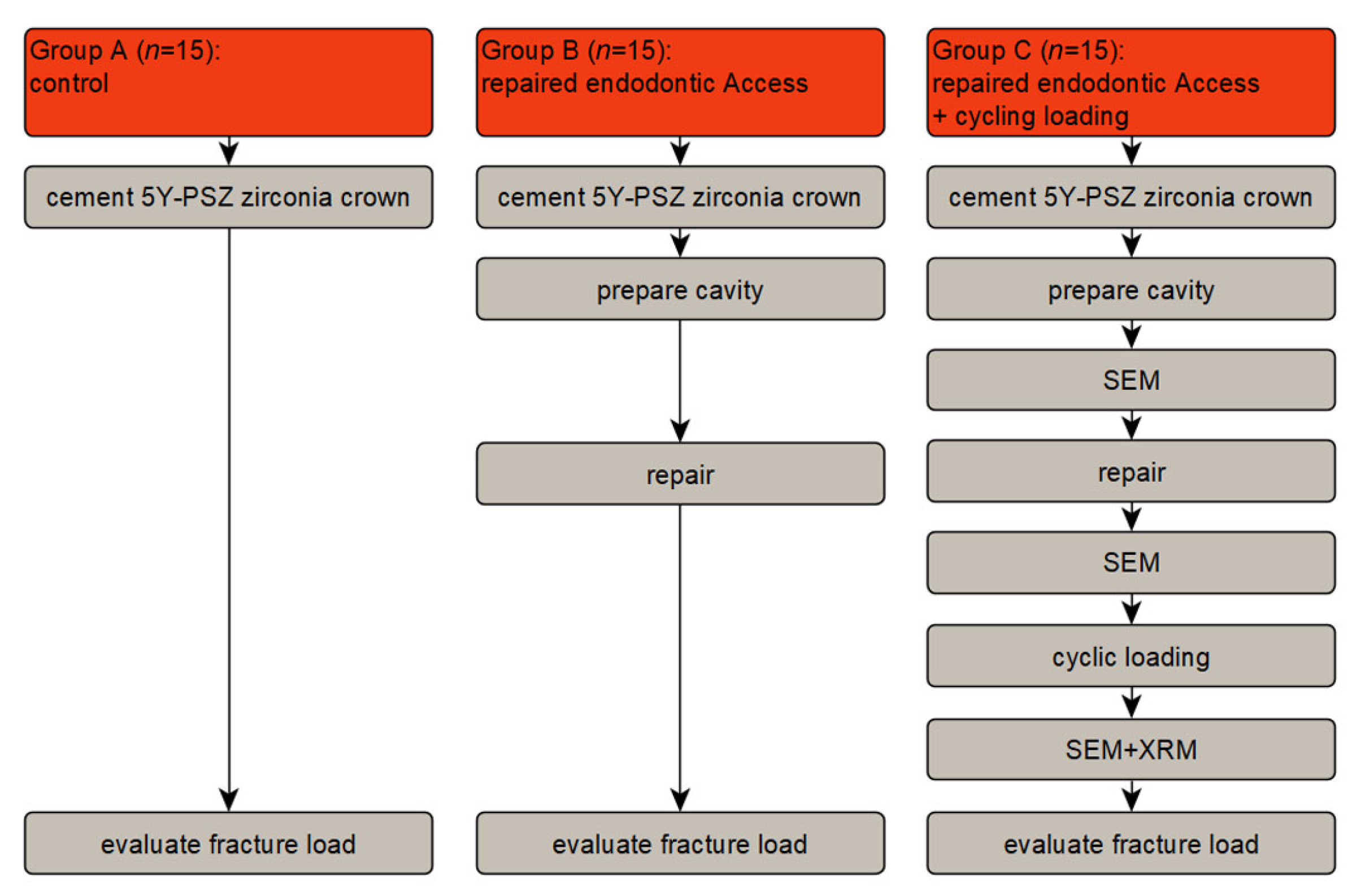{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
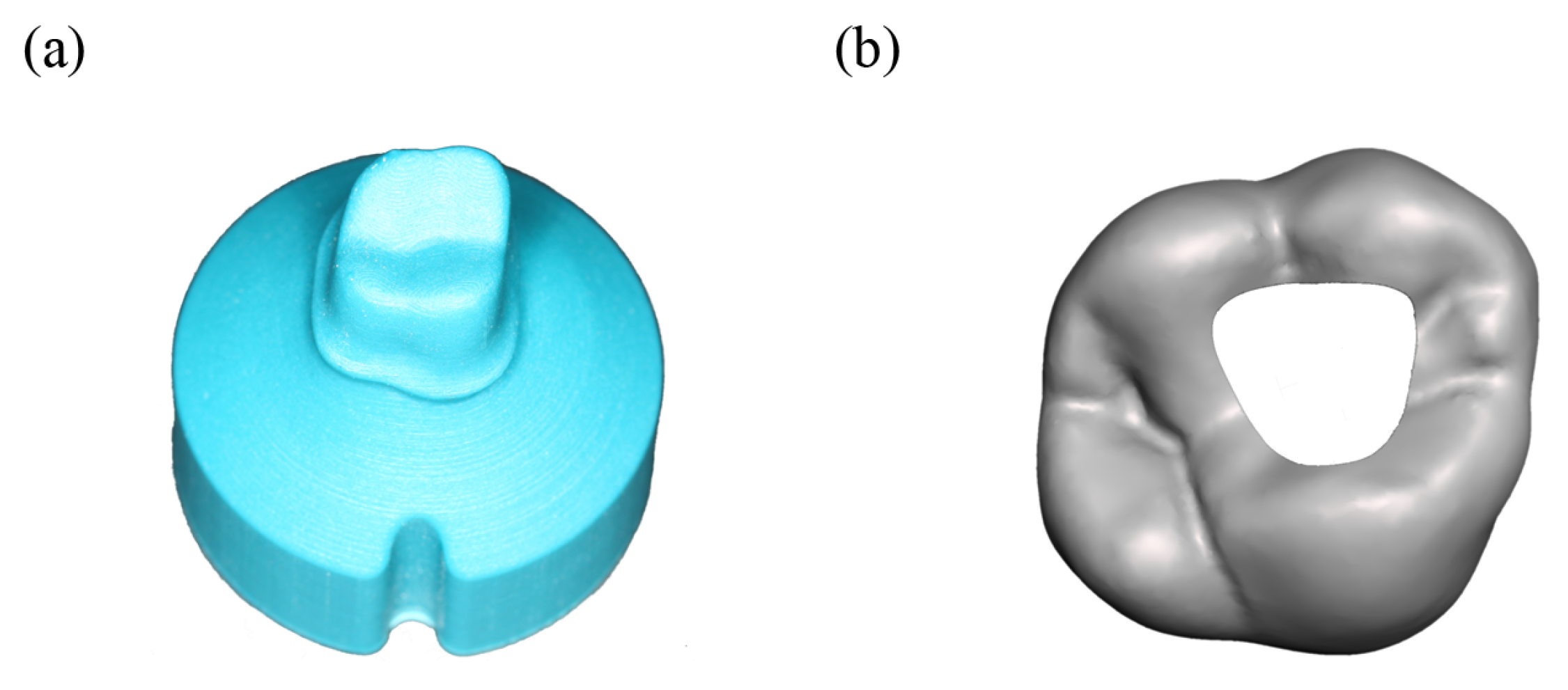
2.1. Specimen Preparation
2.1.1. Abutment Teeth
2.1.2. Crown Production
2.1.3. Crown Cementation
2.1.4. Cavity for Endodontic Access
2.1.5. Repairing the Crown and Polishing
2.2. Thermomechanical Testing
2.3. Fracture Test
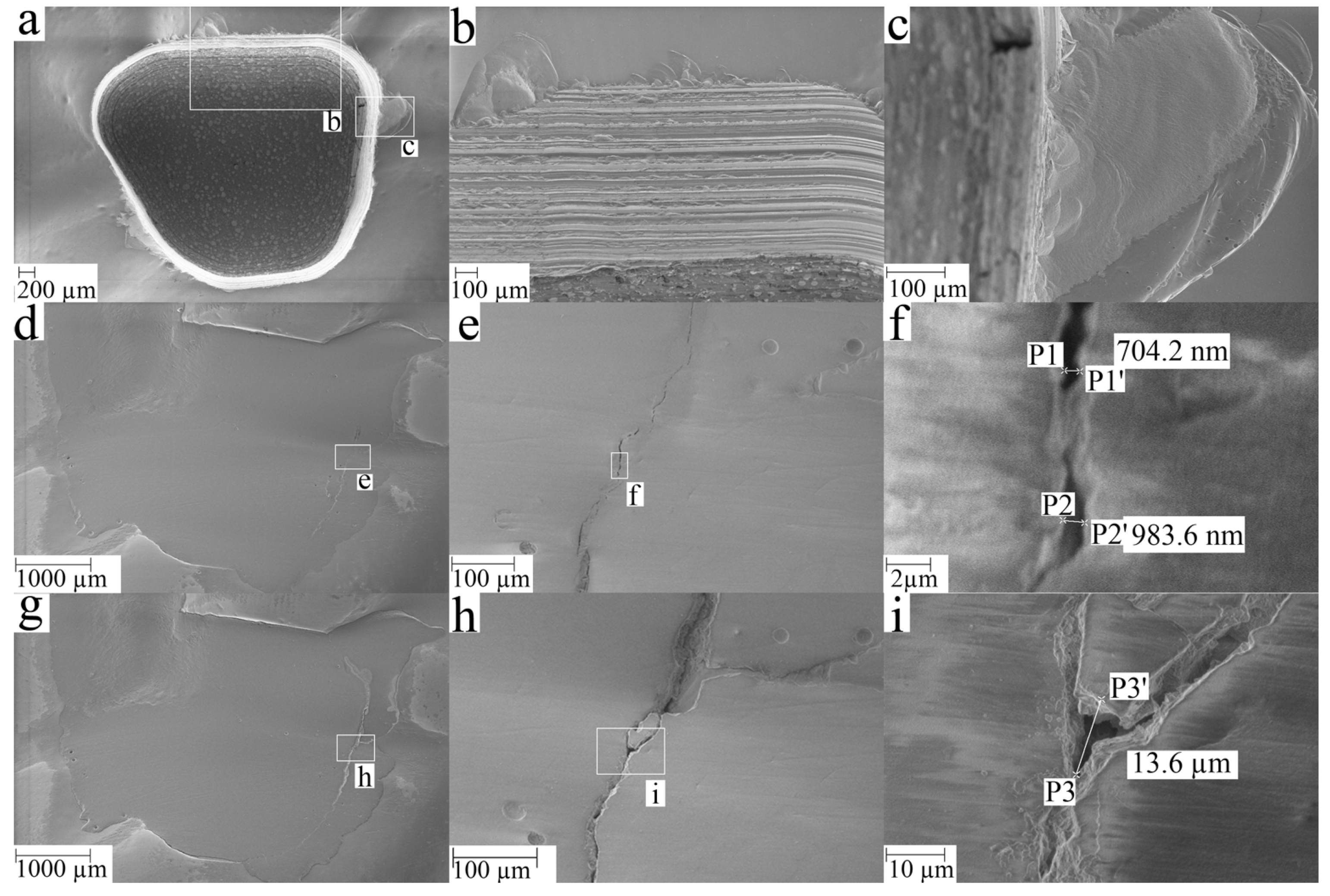
2.4. Scanning Electron Microscopy (SEM)
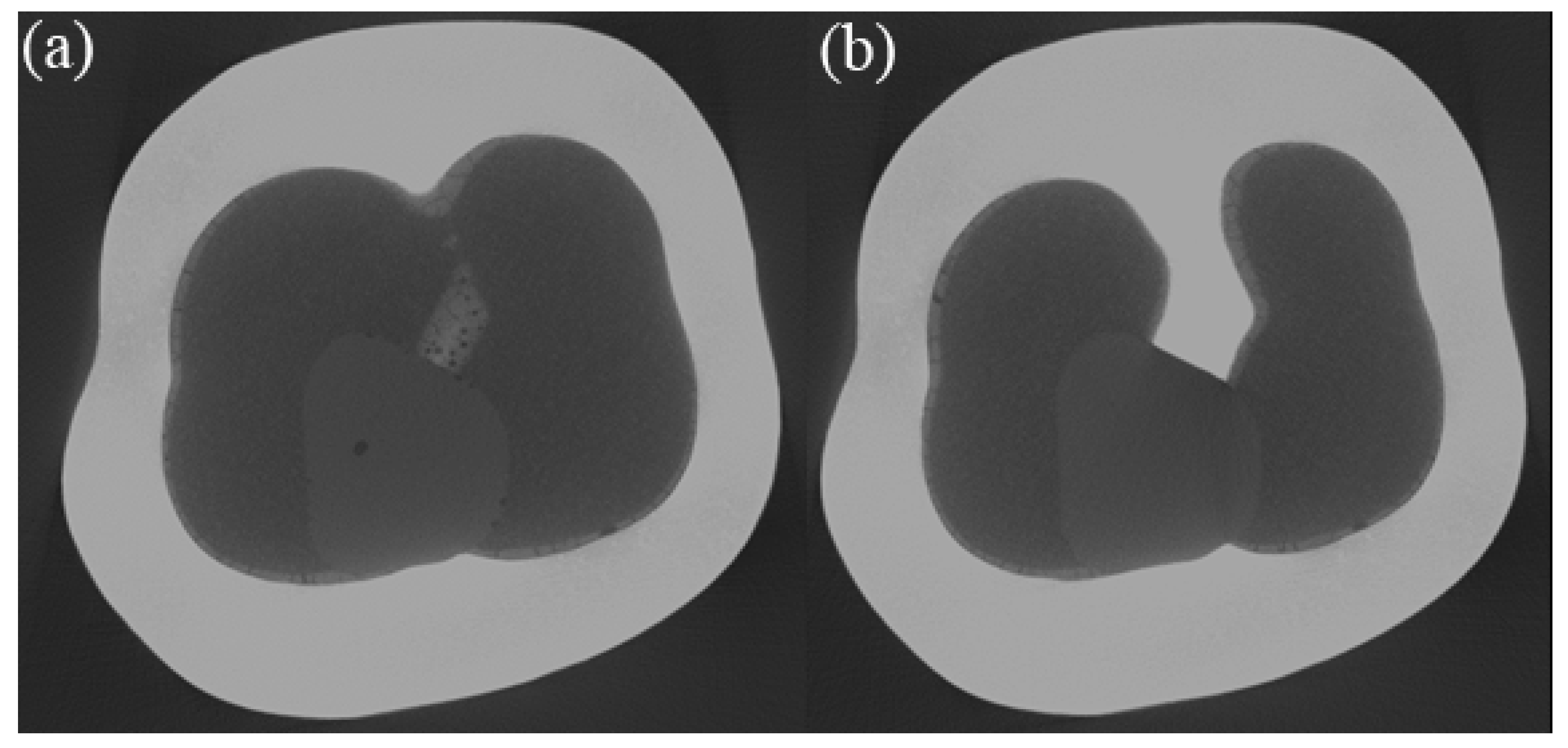
2.5. X-ray Microscopy (XRM)
2.6. Statistical Analysis
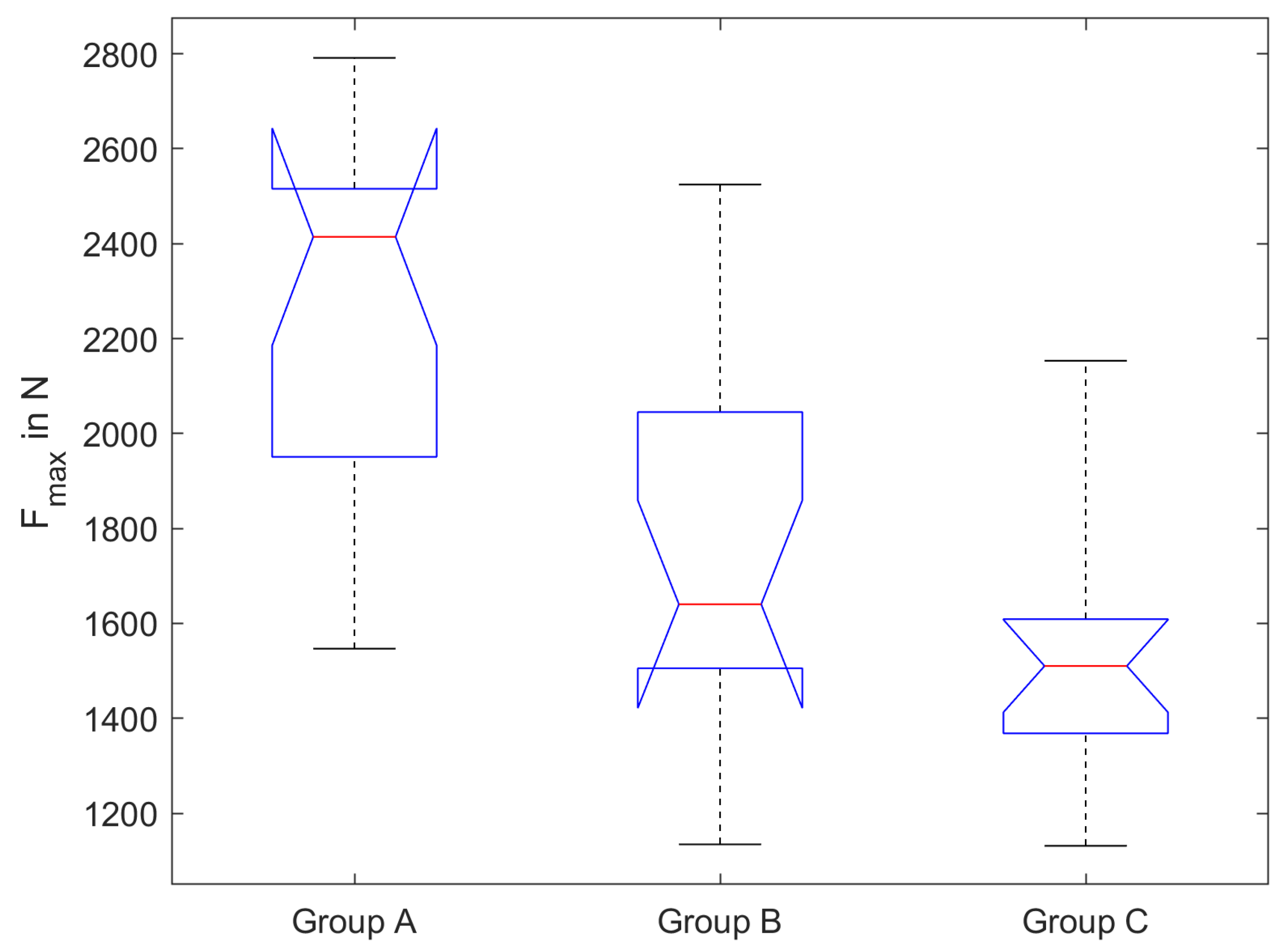
3. Results
4. Discussion
5. Conclusions
- Trepanned and composite repaired 5Y-PSZ crowns show lower fracture loads than 5Y-PSZ crowns without trepanation.
- The fracture load of trepanned and repaired crowns after thermomechanical ageing representing about 2 years of function appears reasonably high (>1100 N).
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Denry, I.; Kelly, J.R. State of the art of zirconia for dental applications. Dent. Mater. 2008, 24, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Kelly, P.M.; Rose, L.F. The martensitic transformation in ceramics—Its role in transformation toughening. Prog. Mater. Sci. 2002, 47, 463–557. [Google Scholar] [CrossRef]
- Miyazaki, T.; Nakamura, T.; Matsumura, H.; Ban, S.; Kobayashi, T. Current status of zirconia restoration. J. Prosthodont. Res. 2013, 57, 236–261. [Google Scholar] [CrossRef] [PubMed]
- Stawarczyk, B.; Keul, C.; Eichberger, M.; Figge, D.; Edelhoff, D.; Lümkemann, N. Three generations of zirconia: From veneered to monolithic. Part I. Quintessence Int. 2017, 48, 369–380. [Google Scholar] [PubMed]
- Worpenberg, C.; Stiesch, M.; Eisenburger, M.; Breidenstein, B.; Busemann, S.; Greuling, A. The effect of surface treatments on the adhesive bond in all-ceramic dental crowns using four-point bending and dynamic loading tests. J. Mech. Behav. Biomed. Mater. 2023, 139, 105686. [Google Scholar] [CrossRef]
- Swain, M.V. Unstable cracking (chipping) of veneering porcelain on all-ceramic dental crowns and fixed partial dentures. Acta Biomater. 2009, 5, 1668–1677. [Google Scholar] [CrossRef]
- Schmitter, M.; Mueller, D.; Rues, S. Chipping behaviour of all-ceramic crowns with zirconia framework and CAD/CAM manufactured veneer. J. Dent. 2012, 40, 154–162. [Google Scholar] [CrossRef]
- Zhang, Y.; Lawn, B.R. Novel zirconia materials in dentistry. J. Dent. Res. 2018, 97, 140–147. [Google Scholar] [CrossRef]
- Lynch, C.D.; Hale, R.; Chestnutt, I.G.; Wilson, N. Reasons for placement and replacement of crowns in general dental practice. Br. Dent. J. 2018, 225, 229–234. [Google Scholar] [CrossRef]
- Uzgur, R.; Uzgur, Z.; Colak, H.; Ercan, E.; Dalli, M.; Özcan, M. A Cross-Sectional Survey on Reasons for Initial Placement and Replacement of Single Crowns. Eur. J. Prosthodont. Restor. Dent. 2017, 25, 42–48. [Google Scholar] [CrossRef]
- Wiegand, A.; Kanzow, P. Effect of Repairing Endodontic Access Cavities on Survival of Single Crowns and Retainer Restorations. J. Endod. 2020, 46, 376–382. [Google Scholar] [CrossRef]
- Blatz, M.B.; Sadan, A.; Martin, J.; Lang, B. In vitro evaluation of shear bond strengths of resin to densely-sintered high-purity zirconium-oxide ceramic after long-term storage and thermal cycling. J. Prosthet. Dent. 2004, 91, 356–362. [Google Scholar] [CrossRef]
- Kern, M.; Wegner, S.M. Bonding to zirconia ceramic: Adhesion methods and their durability. Dent. Mater. 1998, 14, 64–71. [Google Scholar] [CrossRef]
- Wegner, S.M.; Gerdes, W.; Kern, M. Effect of different artificial aging conditions on ceramic-composite bond strength. Int. J. Prosthodont. 2002, 15, 267–272. [Google Scholar]
- Wolfart, M.; Lehmann, F.; Wolfart, S.; Kern, M. Durability of the resin bond strength to zirconia ceramic after using different surface conditioning methods. Dent. Mater. 2007, 23, 45–50. [Google Scholar] [CrossRef]
- Cristoforides, P.; Amaral, R.; May, L.G.; Bottino, M.A.; Valandro, L.F. Composite resin to yttria stabilized tetragonal zirconia polycrystal bonding: Comparison of repair methods. Oper. Dent. 2012, 37, 263–271. [Google Scholar] [CrossRef]
- Oyagüe, R.C.; Monticelli, F.; Toledano, M.; Osorio, E.; Ferrari, M.; Osorio, R. Effect of water aging on microtensile bond strength of dual-cured resin cements to pre-treated sintered zirconium-oxide ceramics. Dent. Mater. 2009, 25, 392–399. [Google Scholar] [CrossRef]
- Xible, A.A.; de Jesus Tavarez, R.R.; de Araujo, C.d.R.P.; Bonachela, W.C. Effect of silica coating and silanization on flexural and composite-resin bond strengths of zirconia posts: An in vitro study. J. Prosthet. Dent. 2006, 95, 224–229. [Google Scholar] [CrossRef]
- Inokoshi, M.; Poitevin, A.; De Munck, J.; Minakuchi, S.; Van Meerbeek, B. Bonding effectiveness to different chemically pre-treated dental zirconia. Clin. Oral Investig. 2014, 18, 1803–1812. [Google Scholar] [CrossRef]
- Begand, S.; Spintzyk, S.; Geis-Gerstorfer, J.; Bourauel, C.; Keilig, L.; Lohbauer, U.; Worpenberg, C.; Greuling, A.; Adjiski, R.; Jandt, K.D. Fracture toughness of 3Y-TZP ceramic measured by the Chevron-Notch Beam method: A round-robin study. Dent. Mater. 2022, 38, 1128–1139. [Google Scholar] [CrossRef]
- Heydecke, G.; Butz, F.; Hussein, A.; Strub, J.R. Fracture strength after dynamic loading of endodontically treated teeth restored with different post-and-core systems. J. Prosthet. Dent. 2002, 87, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Beschnidt, S.M.; Strub, J.R. Evaluation of the marginal accuracy of different all-ceramic crown systems after simulation in the artificial mouth. J. Oral Rehabil. 1999, 26, 582–593. [Google Scholar] [CrossRef] [PubMed]
- Greuling, A.; Matthies, A.; Eisenburger, M. Fracture load of 4-unit interim fixed partial dentures using 3D-printed and traditionally manufactured materials. J. Prosthet. Dent. 2023, in press. [CrossRef] [PubMed]
- Strub, J.R.; Beschnidt, S.M. Fracture strength of 5 different all-ceramic crown systems. Int. J. Prosthodont. 1998, 11, 602–609. [Google Scholar] [PubMed]
- Gu, X.H.; Kern, M. Marginal discrepancies and leakage of all-ceramic crowns: Influence of luting agents and aging conditions. Int. J. Prosthodont. 2003, 16, 109–116. [Google Scholar]
- Bates, J.; Stafford, G.; Harrison, A. Masticatory function—A review of the literature: III. Masticatory performance and efficiency. J. Oral Rehabil. 1976, 3, 57–67. [Google Scholar] [CrossRef]
- Helkimo, E.; Carlsson, G.E.; Helkimo, M. Bite force and state of dentition. Acta Odontol. Scand. 1977, 35, 297–303. [Google Scholar] [CrossRef]
- Van der Bilt, A. Assessment of mastication with implications for oral rehabilitation: A review. J. Oral Rehabil. 2011, 38, 754–780. [Google Scholar] [CrossRef]
- Haraldson, T.; Karlsson, U.; Carlsson, G.E. Bite force and oral function in complete denture wearers. J. Oral Rehabil. 1979, 6, 41–48. [Google Scholar] [CrossRef]
- Schindler, H.J.; Stengel, E.; Spiess, W.E.L. Feedback control during mastication of solid food textures—A clinical-experimental study. J. Prosthet. Dent. 1998, 80, 330–336. [Google Scholar] [CrossRef]
- Kulyk, V.; Duriagina, Z.; Vasyliv, B.; Vavrukh, V.; Kovbasiuk, T.; Holovchuk, M. Effects of yttria content and sintering temperature on the microstructure and tendency to brittle fracture of yttria-stabilized zirconia. Arch. Mater. Sci. Eng. 2021, 109, 65–79. [Google Scholar] [CrossRef]
- Spintzyk, S.; Geis-Gerstorfer, J.; Bourauel, C.; Keilig, L.; Lohbauer, U.; Brune, A.; Greuling, A.; Arnold, C.; Rues, S.; Adjiski, R. Biaxial flexural strength of zirconia: A round robin test with 12 laboratories. Dent. Mater. 2021, 37, 284–295. [Google Scholar] [CrossRef]
- Kern, M.; Barloi, A.; Yang, B. Surface conditioning influences zirconia ceramic bonding. J. Dent. Res. 2009, 88, 817–822. [Google Scholar] [CrossRef]
- Garcia, I.M.; Soto-Montero, J.; Collares, F.M.; Giannini, M. Bonding of Resin Cements to Ultra-Translucent Zirconia After Aging for 24 Hours and 1 Year. Int. J. Prosthodont. 2022, 35, 460–468. [Google Scholar] [CrossRef]
- DeLong, R.; Sakaguchi, R.; Douglas, W.H.; Pintado, M. The wear of dental amalgam in an artificial mouth: A clinical correlation. Dent. Mater. 1985, 1, 238–242. [Google Scholar] [CrossRef]
- Aboushelib, M.N. Simulation of cumulative damage associated with long term cyclic loading using a multi-level strain accommodating loading protocol. Dent. Mater. 2013, 29, 252–258. [Google Scholar] [CrossRef]
- Scioscia, A.; Helfers, A.; Soliman, S.; Krastl, G.; Zitzmann, N. Performance of monolithic and veneered zirconia crowns after endodontic treatment and different repair strategies. Oper. Dent. 2018, 43, 170–179. [Google Scholar] [CrossRef]
- Grobecker-Karl, T.; Christian, M.; Karl, M. Effect of endodontic access cavity preparation on monolithic and ceramic veneered zirconia restorations. Quintessence Int. 2016, 47, 725–729. [Google Scholar] [CrossRef]
- Schubert, J.; Kirkpatrick, T.; Roberts, H. The effect of endodontic access preparation on the failure load resistance of a 3Y-TZP monolithic zirconia crown. Aust. Endod. J. 2022, 48, 138–143. [Google Scholar] [CrossRef]
- Mallya, J.; DuVall, N.; Brewster, J.; Roberts, H. Endodontic access effect on full contour zirconia and lithium disilicate failure resistance. Oper. Dent. 2020, 45, 276–285. [Google Scholar] [CrossRef]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Greuling, A.; Wiemken, M.; Kahra, C.; Maier, H.J.; Eisenburger, M. Fracture Resistance of Repaired 5Y-PSZ Zirconia Crowns after Endodontic Access. Dent. J. 2023, 11, 76. https://doi.org/10.3390/dj11030076
Greuling A, Wiemken M, Kahra C, Maier HJ, Eisenburger M. Fracture Resistance of Repaired 5Y-PSZ Zirconia Crowns after Endodontic Access. Dentistry Journal. 2023; 11(3):76. https://doi.org/10.3390/dj11030076
Chicago/Turabian StyleGreuling, Andreas, Mira Wiemken, Christoph Kahra, Hans Jürgen Maier, and Michael Eisenburger. 2023. "Fracture Resistance of Repaired 5Y-PSZ Zirconia Crowns after Endodontic Access" Dentistry Journal 11, no. 3: 76. https://doi.org/10.3390/dj11030076
APA StyleGreuling, A., Wiemken, M., Kahra, C., Maier, H. J., & Eisenburger, M. (2023). Fracture Resistance of Repaired 5Y-PSZ Zirconia Crowns after Endodontic Access. Dentistry Journal, 11(3), 76. https://doi.org/10.3390/dj11030076