
Pilot Study of a New Mandibular Advancement Device

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Device
2.3. Study Design
3. Results
Efficacy of the OrthoApnea NOA® Device
4. Discussion
Limitations and Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.M.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pépin, J.L.; et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [Green Version]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. American Academy of Sleep Medicine. Rules for scoring respiratory events in sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [PubMed] [Green Version]
- Ramar, K.; Dort, L.C.; Katz, S.G.; Lettieri, C.J.; Harrod, C.G.; Thomas, S.M.; Chervin, R.D. Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy: An Update for 2015. J. Dent. Sleep Med. 2015, 11, 773–827. [Google Scholar] [CrossRef]
- Vanderveken, O.M.; Devolder, A.; Marklund, M.; Boudewyns, A.N.; Braem, M.; Okkerse, W.; Verbraecken, J.A.; Franklin, K.; De Backer, W.A.; Van de Heyning, P. Comparison of a Custom-made and a Thermoplastic Oral Appliance for the Treatment of Mild Sleep Apnea. Am. J. Respir. Crit. Care Med. 2008, 178, 197–202. [Google Scholar] [CrossRef]
- Sharples, L.; Glover, M.; Clutterbuck-James, A.; Bennett, M.; Jordan, J.; Chadwick, R.; Pittman, M.; East, C.; Cameron, M.; Davies, M.; et al. Clinical effectiveness and cost-effectiveness results from the randomised controlled Trial of Oral Mandibular Advancement Devices for Obstructive sleep apnoea-hypopnoea (TOMADO) and long-term economic analysis of oral devices and continuous positive airway pressure. Health Technol. Assess. 2014, 18, 1–296. [Google Scholar]
- Pépin, J.L.; Raymond, N.; Lacaze, O.; Aisenberg, N.; Forcioli, J.; Bonte, E.; Bourdin, A.; Launois, S.; Tamisier, R.; Molinari, N. Heat-moulded versus custom-made mandibular advancement devices for obstructive sleep apnoea: A randomised non-inferiority trial. Thorax 2019, 74, 667–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Randerath, W.J.; Verbraecken, J.; Andreas, S.; Bettega, G.; Boudewyns, A.; Hamans, E.; Jalbert, F.; Paoli, J.R.; Sanner, B.; Smith, I.; et al. European Respiratory Society task force on non-CPAP therapies in sleep apnoea. Non-CPAP therapies in obstructive sleep apnoea. Eur. Respir. J. 2011, 37, 1000–1028. [Google Scholar] [CrossRef] [Green Version]
- Ahrens, A.; McGrath, C.; Hägg, U. Subjective efficacy of oral appliance design features in the management of obstructive sleep apnea: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 559–576. [Google Scholar] [CrossRef]
- Levrini, L.; Sacchi, F.; Milano, F.; Polimeni, A.; Cozza, P.; Bernkopf, E.; Segù, M. Italian recommendations on dental support in the treatment of adult obstructive sleep apnea syndrome (OSAS). Ann. di Stomatol. 2015, 6, 81–86. [Google Scholar] [CrossRef]
- Skeie, M.S.; Frid, P.; Mustafa, M.; Aßmus, J.; Rosén, A. DC/TMD Examiner Protocol: Longitudinal Evaluation on Interexaminer Reliability. Pain Res. Manag. 2018, 2018, 7474608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kazemeini, E.; de Beeck, S.O.; Vroegop, A.; Van Loo, D.; Willemen, M.; Verbraecken, J.; Braem, M.J.; Vanderveken, O.M.; Dieltjens, M. A pilot study on comparison of subjective titration versus remotely controlled mandibular positioning during polysomnography and drug-induced sleep endoscopy, to determine the effective protrusive position for mandibular advancement device therapy. Sleep Breath. 2022, 1–9. [Google Scholar] [CrossRef]
- Jaiswal, M.; Srivastava, G.N.; Pratap, C.B.; Sharma, V.K.; Chaturvedi, T. Effect of Oral Appliance for Snoring and Obstructive Sleep Apnea. Int. J. Orthod. (Milwaukee Wis.) 2015, 26, 67–71. [Google Scholar]
- Segù, M.; Cosi, A.; Santagostini, A.; Scribante, A. Efficacy of a Trial Oral Appliance in OSAS Management: A New Protocol to Recognize Responder/Nonresponder Patients. Int. J. Dent. 2021, 2021, 8811700. [Google Scholar] [CrossRef]
- Punjabi, N.M. The epidemiology of adult obstructive sleep apnea. Proc. Am. Thorac. Soc. 2008, 5, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Young, T.; Palta, M.; Dempsey, J.; Skatrud, J.; Weber, S.; Badr, S. The occurrence of sleep-disordered breathing among middle-aged adults. N. Engl. J. Med. 1993, 328, 1230–1235. [Google Scholar] [CrossRef] [Green Version]
- Hoekema, A.; Stegenga, B.; Wijkstra, P.J.; van der Hoeven, J.H.; Meinesz, A.F.; de Bont, L.G. Obstructive sleep apnea therapy. J. Dent. Res. 2008, 87, 882–887. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Long, H.; Jian, F.; Lin, J.; Zhu, J.; Gao, M.; Lai, W. The effectiveness of oral appliances for obstructive sleep apnea syndrome: A meta-analysis. J. Dent. 2015, 43, 1394–1402. [Google Scholar] [CrossRef]
- Iftikhar, I.H.; Bittencourt, L.; Youngstedt, S.D.; Ayas, N.; Cistulli, P.; Schwab, R.; Durkin, M.W.; Magalang, U.J. Comparative efficacy of CPAP, MADs, exercise-training, and dietary weight loss for sleep apnea: A network meta-analysis. Sleep Med. 2017, 30, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Attali, V.; Chaumereuil, C.; Arnulf, I.; Golmard, J.-L.; Tordjman, F.; Morin, L.; Goudot, P.; Similowski, T.; Collet, J.-M. Predictors of long-term effectiveness to mandibular repositioning device treatment in obstructive sleep apnea patients after 1000 days. Sleep Med. 2016, 27–28, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Uniken Venema, J.A.M.; Doff, M.H.J.; Joffe-Sokolova, D.; Wijkstra, P.J.; van der Hoeven, J.H.; Stegenga, B.; Hoekema, A. Long-term obstructive sleep apnea therapy: A 10-year follow-up of mandibular advancement device and continuous positive airway pressure. J. Clin. Sleep Med. 2020, 16, 353–359. [Google Scholar] [CrossRef]
- Marklund, M.; Verbraecken, J.; Randerath, W. Non-CPAP therapies in obstructive sleep apnoea: Mandibular advancement device therapy. Eur. Respir. J. 2011, 39, 1241–1247. [Google Scholar] [CrossRef] [Green Version]
- Silva Gomes Ribeiro, C.V.; Ribeiro-Sobrinho, D.; Muñoz Lora, V.R.M.; Morais Dornelas Bezerra, L.; Del Bel Cury, A.A. Association between mandibular advancement device therapy and reduction of excessive daytime sleepiness due to obstructive sleep apnoea. J. Oral Rehabil. 2019, 46, 1031–1035. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, K.A.; Ono, T.; Lowe, A.A.; Keenan, S.P.; Fleetham, J.A. A randomized crossover study of an oral appliance vs nasal-continuous positive airway pressure in the treatment of mild-moderate obstructive sleep apnea. Chest 1996, 109, 1269–1275. [Google Scholar] [CrossRef] [Green Version]
- Durán-Cantolla, J.; Alkhraisat, M.; Martínez-Null, C.; Aguirre, J.J.; Guinea, E.R.; Anitua, E. Frequency of Obstructive Sleep Apnea Syndrome in Dental Patients with Tooth Wear. J. Clin. Sleep Med. 2015, 11, 445–450. [Google Scholar] [CrossRef]
- Milano, F.; Mondini, S.; Billi, M.; Gobbi, R.; Gracco, A.; Sorrenti, G. The impact of a multidisciplinary approach on response rate of mandibular advancing device therapy in patients with obstructive sleep apnoea syndrome. Acta Otorhinolaryngol. Ital. 2013, 33, 337–342. [Google Scholar]
- Schwartz, M.; Acosta, L.; Hung, Y.-L.; Padilla, M.; Enciso, R. Effects of CPAP and mandibular advancement device treatment in obstructive sleep apnea patients: A systematic review and meta-analysis. Sleep Breath. 2017, 22, 555–568. [Google Scholar] [CrossRef]
- Rotty, M.-C.; Suehs, C.M.; Mallet, J.-P.; Martinez, C.; Borel, J.-C.; Rabec, C.; Bertelli, F.; Bourdin, A.; Molinari, N.; Jaffuel, D. Mask side-effects in long-term CPAP-patients impact adherence and sleepiness: The InterfaceVent real-life study. Respir. Res. 2021, 22, 17. [Google Scholar] [CrossRef]
- Baratta, F.; Pastori, D.; Bucci, T.; Fabiani, M.; Fabiani, V.; Brunori, M.; Loffredo, L.; Lillo, R.; Pannitteri, G.; Angelico, F.; et al. Long-term prediction of adherence to continuous positive air pressure therapy for the treatment of moderate/severe obstructive sleep apnea syndrome. Sleep Med. 2017, 43, 66–70. [Google Scholar] [CrossRef] [PubMed]
- García-Campos, E.; Labra, A.; Galicia-Polo, L.; Sánchez-Narváez, F.; Haro, R.; Jiménez, U.; Poblano, A. Decrease of respiratory events in patients with obstructive sleep apnea-hypopnea syndrome using a mandibular advancement device assessed with split night polysomnography. Sleep Sci. 2016, 9, 221–224. [Google Scholar] [CrossRef] [Green Version]
- Dieltjens, M.; Vanderveken, O.M.; Van de Heyning, P.H.; Braem, M.J. Current opinions and clinical practice in the titration of oral appliances in the treatment of sleep-disordered breathing. Sleep Med. Rev. 2012, 16, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Sharples, L.D.; Clutterbuck-James, A.L.; Glover, M.J.; Bennett, M.S.; Chadwick, R.; Pittman, M.A.; Quinnell, T.G. Meta-analysis of randomised controlled trials of oral mandibular advancement devices and continuous positive airway pressure for obstructive sleep apnoea-hypopnoea. Sleep Med. Rev. 2016, 27, 108–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Sanjuán, P.; Arrieta, J.J.; Sanabria, J.; Alcaraz, M.; Bosco, G.; Pérez-Martín, N.; Pérez, A.; Carrasco-Llatas, M.; Moreno-Hay, I.; Ríos-Lago, M.; et al. Optimizing Mandibular Advancement Maneuvers during Sleep Endoscopy with a Titratable Positioner: DISE-SAM Protocol. J. Clin. Med. 2022, 11, 658. [Google Scholar] [CrossRef]
- Sato, K.; Nakajima, T. Review of systematic reviews on mandibular advancement oral appliance for obstructive sleep apnea: The importance of long-term follow-up. Jpn. Dent. Sci. Rev. 2019, 56, 32–37. [Google Scholar] [CrossRef] [PubMed]
- De Almeida, F.R.; Lowe, A.A.; Otsuka, R.; Fastlicht, S.; Farbood, M.; Tsuiki, S. Long-term sequellae of oral appliance therapy in obstructive sleep apnea patients: Part 2. Study-model analysis. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, K.A.; Cartwright, R.; Rogers, R.; Schmidt-Nowara, W. Oral Appliances for Snoring and Obstructive Sleep Apnea: A Review. Sleep 2006, 29, 244–262. [Google Scholar] [CrossRef] [Green Version]
- De Britto Teixeira, A.O.; Abi-Ramia, L.B.; de Oliveira Almeida, M.A. Treatment of obstructive sleep apnea with oral appliances. Prog. Orthod. 2013, 14, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scherr, S.C.; Almeida, F.R.; Bennett, K.M.; Dort, L.C.; Essick, G.K.; Katz, S.G.; McLornan, P.M.; Phillips, K.S.; Rogers, R.R.; Sheats, R.D.; et al. Definition of an effective oral appliance for the treatment of obstructive sleep apnea and snoring: A report of the American Academy of Dental Sleep Medicine. J. Dent. Sleep Med. 2014, 1, 39–50. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Number of patients | 8 |
| Males | 3 |
| Females | 5 |
| Age, mean ± SD | 56.25 ± 9.75 |
| OSAS severity, number of patients | |
| Mild (5 ≥ AHI < 15) | 4 |
| oderate (15 ≥ AHI < 30) | 1 |
| Severe (AHI ≥ 30) | 3 |
| AHI | 21.33 ± 14.79 |
| Supine AHI | 35.64 ± 12.80 |
| ODI | 17.51 ± 13.5 |
| SpO2 < 90% | 7.82 ± 17.08 |
| MeanSpO2% | 93.45 ± 1.86 |
| T0 | T1 | p | |
|---|---|---|---|
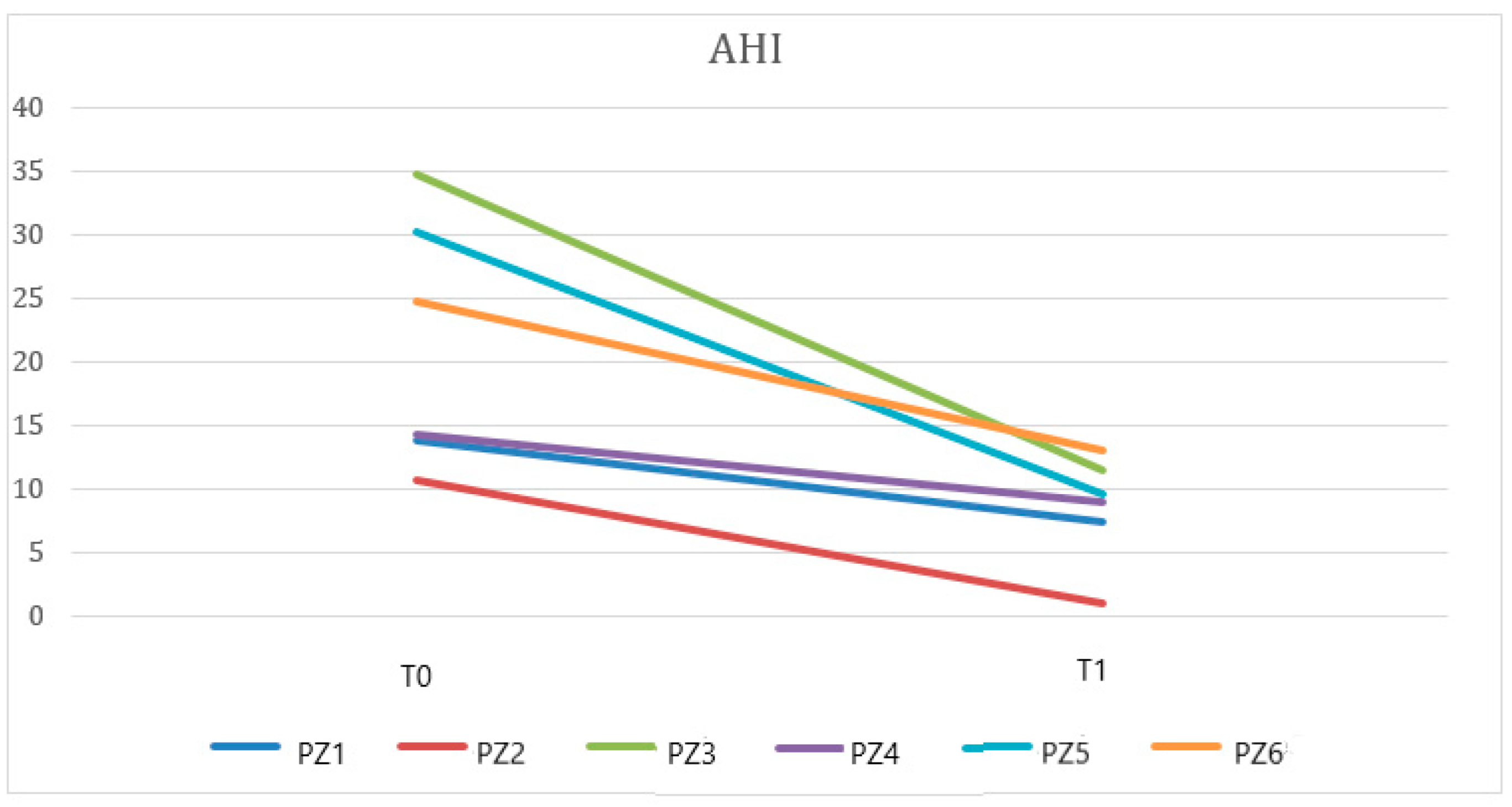
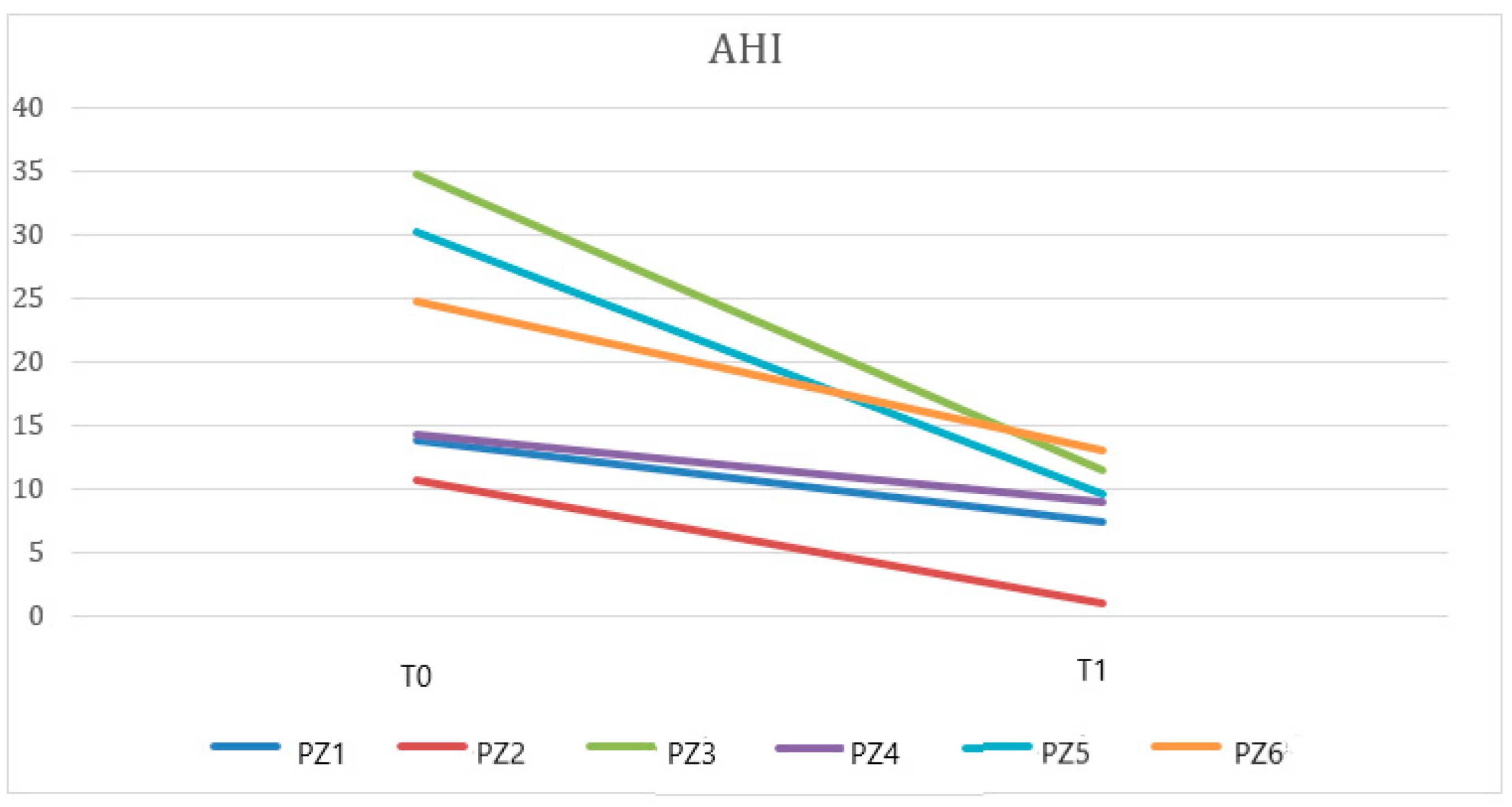
| AHI | 21.33 ± 9.75 | 8.6 ± 4.21 | 0.008 |
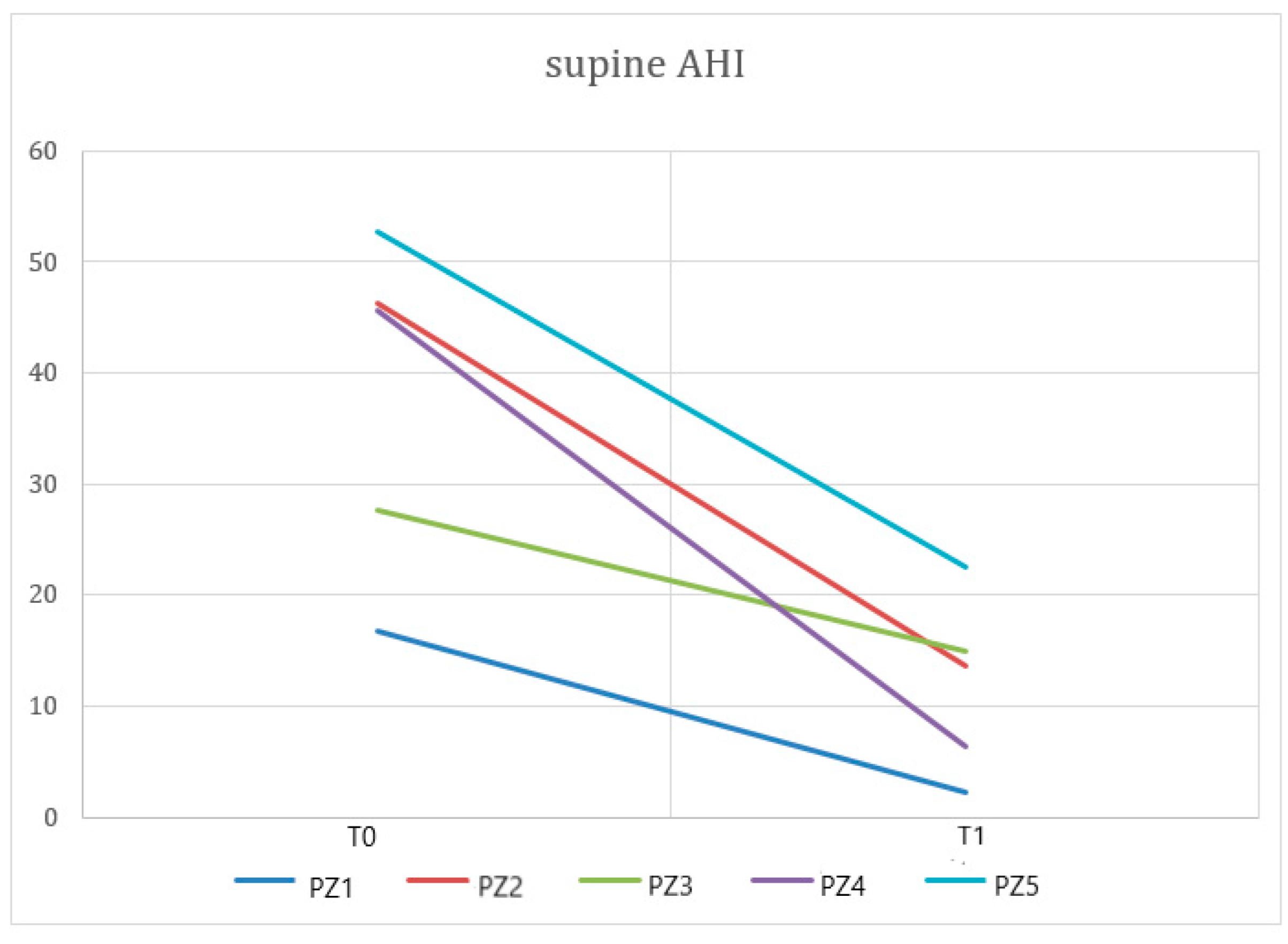
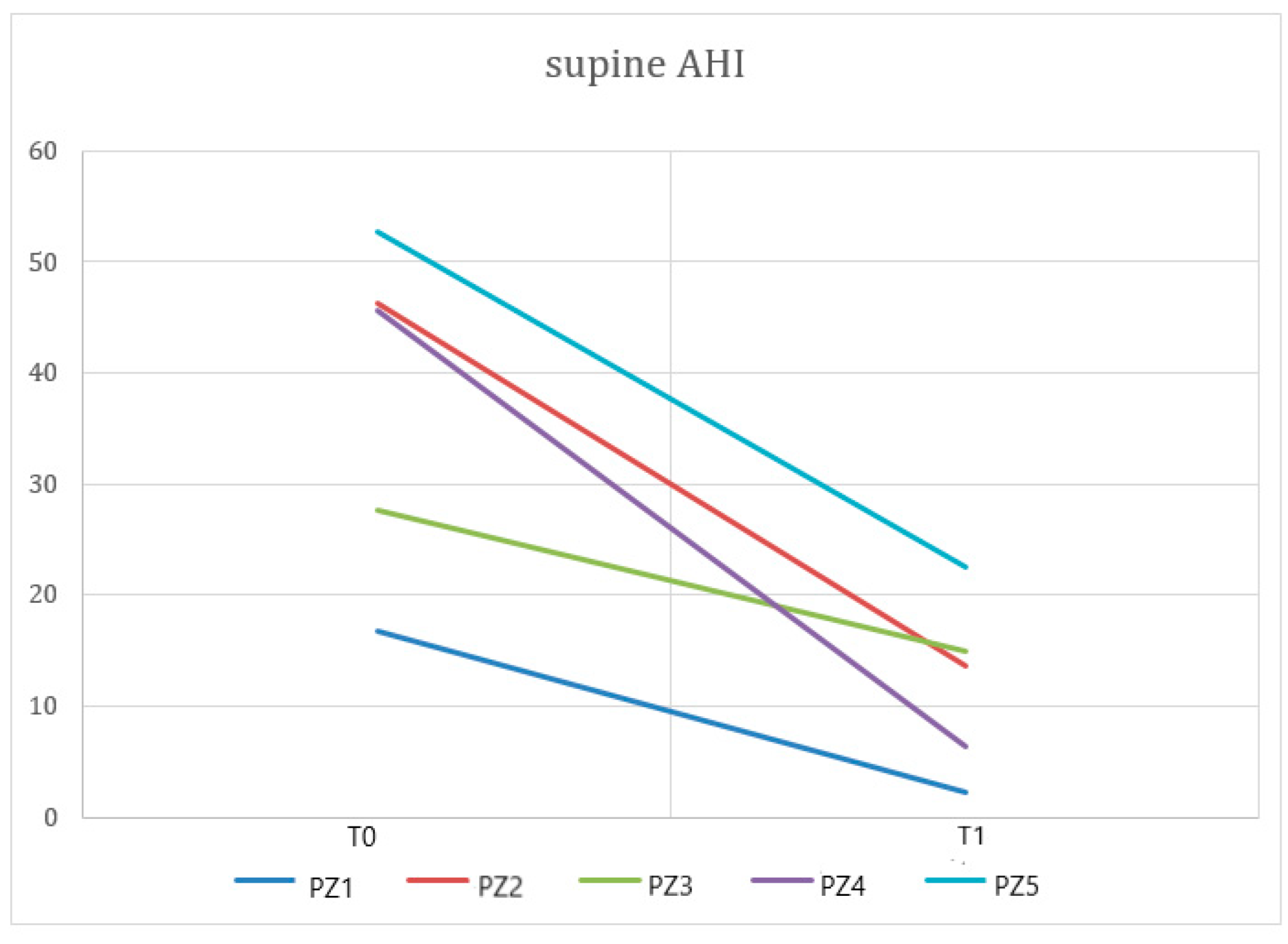
| Supine AHI | 35.64 ± 12.80 | 11.21 ± 7.26 | 0.002 |
| ODI | 17.51 ± 13.5 | 8.81 ± 4.59 | 0.07 |
| SpO2 < 90% | 7.82 ± 17.08 | 0.66 ± 1.43 | 0.17 |
| MeanSpO2 | 93.45 ± 1.86 | 93.66 ± 1.03 | 0.82 |
| Patients | Changes in AHI T0–T1 | Changes in Supine AHI T0–T1 |
|---|---|---|
| 1 | −46% | −75% |
| 2 | −91% | −86% |
| 3 | −67% | −17% |
| 4 | −37% | −46% |
| 5 | −68% | −86% |
| 6 | −47% | −57% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Segù, M.; Campagnoli, G.; Di Blasio, M.; Santagostini, A.; Pollis, M.; Levrini, L. Pilot Study of a New Mandibular Advancement Device. Dent. J. 2022, 10, 99. https://doi.org/10.3390/dj10060099
Segù M, Campagnoli G, Di Blasio M, Santagostini A, Pollis M, Levrini L. Pilot Study of a New Mandibular Advancement Device. Dentistry Journal. 2022; 10(6):99. https://doi.org/10.3390/dj10060099
Chicago/Turabian StyleSegù, Marzia, Giovanna Campagnoli, Marco Di Blasio, Antonio Santagostini, Matteo Pollis, and Luca Levrini. 2022. "Pilot Study of a New Mandibular Advancement Device" Dentistry Journal 10, no. 6: 99. https://doi.org/10.3390/dj10060099
APA StyleSegù, M., Campagnoli, G., Di Blasio, M., Santagostini, A., Pollis, M., & Levrini, L. (2022). Pilot Study of a New Mandibular Advancement Device. Dentistry Journal, 10(6), 99. https://doi.org/10.3390/dj10060099